Article Text

Abstract
This paper describes the implementation of a clinical pharmacy services in hospitals in Central Norway. Our model for clinical pharmacy services is based on the Integrated Medicines Management (IMM) model originally developed in Northern Ireland, and the Lund IMM (LIMM) developed in the South of Sweden, and adjusted to Norwegian settings. The evaluation process has been completed by conducting projects, mini-audits and surveys.
- Clinical Pharmacy
- Pharmacotherapy
Statistics from Altmetric.com
Introduction
The clinical pharmacy has been defined differently by different organisations.1 The Norwegian Hospital Pharmacy Association defines it as: ‘The use of pharmaceutical competencies, clinical data and other relevant information to achieve correct use of drugs for each individual patient. Clinical pharmacy services are performed in collaboration with the responsible doctor and in some circumstances other health care professionals and the patient.’ This means that in Norway, the term, clinical pharmacy, is mainly used to describe patient-specific services, such as medicines reconciliation, medication review and patient counselling. In secondary care, the clinical pharmacist is usually employed by a hospital pharmacy, but they work as members of the ward team by attending multidisciplinary team meetings and ward rounds. Usually, the Norwegian hospital pharmacists work in different areas within the hospital pharmacy, such as medicines management, dispensary and technical services.
Establishment of clinical pharmacy services
Central Norway Hospital Pharmacy Trust consists of six hospital pharmacies in the cities of Trondheim, Levanger, Namsos, Aalesund, Kristiansund and Molde. We employ about 180 staff members, including 75 pharmacists. The pharmacies serve eight hospitals in the region.
In the past, clinical pharmacy services in Central Norway were not systemised, and the provision and the content of the services were dependent on individual pharmacists. As described earlier in EJHP,2 the introduction of a consistent clinical pharmacy services in Central Norway started when the Integrated Medicines Management (IMM)3 model developed in Northern Ireland, was brought to our attention. In 2009, the hospital pharmacy in Levanger initiated collaboration with Professor Tommy Eriksson and his colleagues in Lund, Sweden. Professor Eriksson and his team have developed the Swedish clinical pharmacy model, Lund IMM (LIMM).4 With assistance from Lund, we started training our hospital pharmacists in clinical skills and use of the model. Later, we also established a good relationship with the IMM team in Northern Ireland, led by Professor James C McElnay and Professor Michael G Scott.
The hospital pharmacies in Central Norway worked dedicatedly over the next few years to meet the needs of the hospitals in our region with regards to drug aspects of patient safety. This resulted in the achievement of funding for nine-and-a-half clinical pharmacist positions from 2011, partly funded by the Regional Health Authority for Central Norway and partly by the Hospital Trusts. From 2013, there is funding for 12 full-time posts, and the clinical pharmacists offer medicines reconciliation on admission and discharge, medication review and patient counselling. The type of services performed depends on the patient group, the ward speciality and local agreements.
Education and training have been, and will be, high priority, and our pharmacists have been encouraged to undertake a postgraduate masters degree in clinical pharmacy at the University of Oslo. So far, 11 pharmacists have completed this study programme. Additionally, we have developed a course in clinical pharmacy and pharmacotherapy at the Norwegian University of Science and Technology (NTNU) that started in 2013. All our clinical pharmacists complete a standardised training programme in the IMM model before being certified fit to carry out clinical pharmacy services.
Furthermore, we have initiated a national collaboration in clinical pharmacy and IMM. All four regional hospital pharmacy trusts, and two private hospital pharmacies, are working together to ensure high quality of the clinical pharmacy services and IMM. Among others, the main tasks for the national collaboration is to make sure the IMM model is maintained with regards to standard operating procedures, and training and certification programmes, and to support the clinical pharmacists in developing knowledge and competencies in clinical pharmacy.
Evaluation of clinical pharmacy services
To show the positive effects of the IMM model in Central Norway, several studies have been completed. Our aim has been to evaluate the services by summarising the results from the different studies completed in 2011 and 2012. Furthermore, we wanted to explore healthcare professionals’ and patients’ experiences with the services.
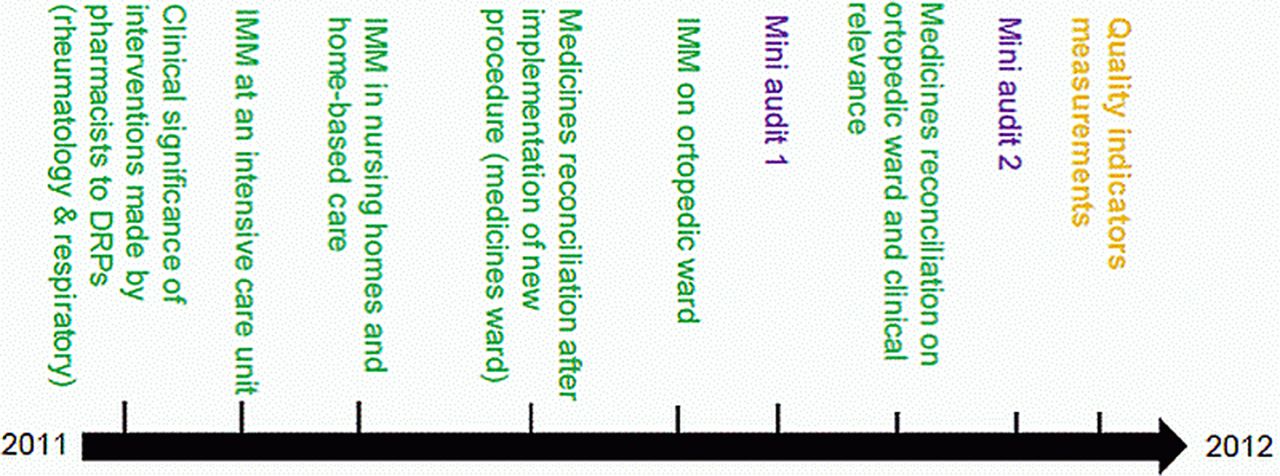
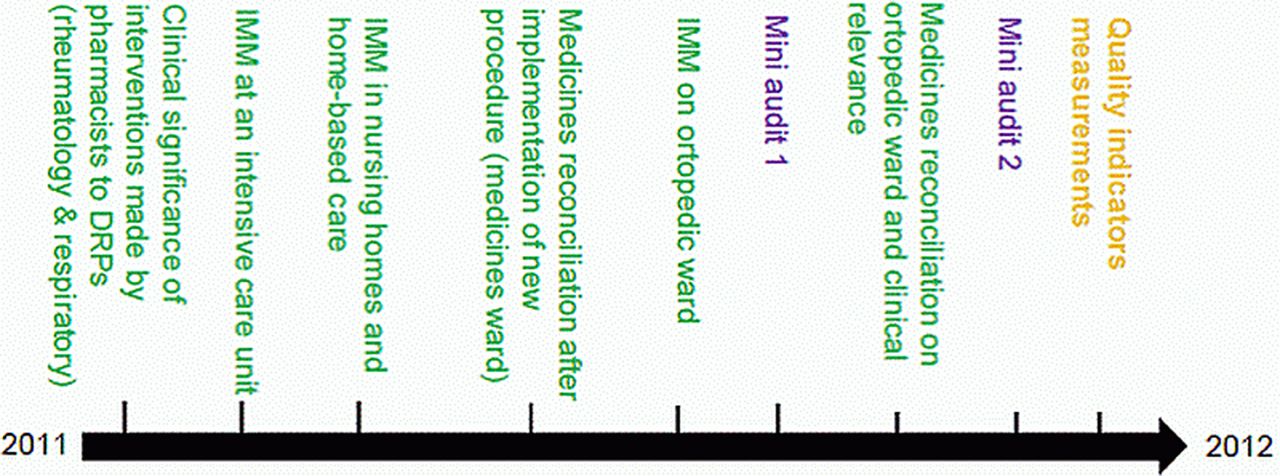
First, the evaluation process included a review of different results obtained through six different research projects, mainly master theses, focusing on medicines reconciliation and/or medication review (figure 1). The projects were set up with slight differences, and involved patients from different specialities, such as rheumatology, respiratory medicine, intensive care and orthopaedics. One study was carried out in primary care, which included patients in nursing homes and patients living in their own home and receiving home care services.5
{kind=link}
Timeline showing the six projects (green coloured) which have studied the Integrated Medicines Management (IMM) model in hospital and primary care, the mini-audits (purple coloured) and measurements of quality indicators (yellow coloured).
Second, two mini-audits were performed to benchmark daily activities, including documentation of discrepancies found in drug histories and drug-related problems (DRP) discovered through medication reviews. Four hospital pharmacies performed the mini audits on different wards, such as orthopaedics, rheumatology, internal medicine and cardiology.
Finally, three different questionnaires were distributed to patients, clinical pharmacists, and doctors and nurses investigating, respectively, patient satisfaction, the clinical pharmacists’ experiences with the IMM model and the attitudes of and usefulness for healthcare professionals.
Results and experiences
Projects
Medicines reconciliation
All together, between 50% and 78% of patients admitted to hospitals had one or more discrepancies in their drug lists. The lowest figure (50%) was seen in orthopaedic patients admitted to hospital due to a fractured neck of femur. The highest figure (78%) was found in patients admitted to the intensive care unit, where a lot of drugs are withheld or stopped at admission, often for a medical reason, however, the documentation was missing. In all projects, we found between one and three discrepancies in each patient's drug history. The main reason for discrepancies was omission of drugs at point of admission.
Medicines reconciliation in the community was performed by comparing the patients’ drug list at the home care services and the general practitioner's (GP) drug lists.5 In some cases, additional information was provided by interviewing the patients. In 55% of the patients receiving home care (ie, community nurses provide the patients with their drugs and help with administration where this is needed), the information about drugs in use was not consistent between the sources of information.
The clinical importance of discrepancies found in drug histories of orthopaedic patients in Trondheim and patients admitted to internal medicine wards in Aalesund were evaluated according to a short-term and a long-term perspective based on a 3-graded scale.6 For the orthopaedic patients, almost 50% of discrepancies could potentially cause moderate to severe harm if not acted upon within a few days. The number increased to nearly 90% if the discrepancies were not corrected at time of discharge and were believed to be carried on in primary care. In Aalesund,7 the numbers were much lower; 20% of the discrepancies had the potential to cause moderate to severe harm in a short-term perspective, and 30% in a long-term perspective. The variation in the results could be due to different patient groups and/or different expert groups assessing the results.
Medication review
The number of drug-related problems (DRPs) per patients varied between different projects and patient populations, the average numbers were: 2.1 for orthopaedic patients, 2.9 for intensive care patients and 3.2 for rheumatology and respiratory care patients. In nursing homes, an average of 2.9 DRPs were identified for each patient compared with 3.2 DRPs for patients living in their own homes receiving home care services.5
Most frequent DRPs were:
-
need for additional therapy
-
inappropriate use of drug(s)
-
unnecessary use of drug(s)/no indication for drug therapy.
Examples of DRPs in hospital could be an elderly patient not prescribed a bisphosphonate after having surgery for a fractured neck of femur (need for additional therapy) but prescribed tramadol for postsurgery pain (inappropriate use of drug).
The most common DRPs in community care were drugs not discontinued after completion of a course (eg, treatment of gastric ulcers with high-dose proton pump inhibitors for much longer than 4 weeks).
For the hospitalised patients, the doctors acknowledged and acted upon the pharmacists’ advice in 50–70% of the cases. In the rest of the cases, the doctors either did not want to alter the treatment or they needed more time to investigate other options.
A multidisciplinary team including pharmacists is not established in community care. During the project period, the pharmacists had meetings with the nursing home doctors and nurses regarding the patients in the nursing home and identified the DRPs, and the doctors accepted the pharmacist's advice to solve DRPs in nearly 70% of the cases.
The GPs are responsible for the drug treatment for patients receiving home care services and community nurses and healthcare workers provide the everyday support. With regards to these patients, only 50% of the discussed DRPs were acted upon by the GPs. This might be because the patients and/or the community nurses were not present when the DRPs were discussed, and needed to be consulted before changing the treatment.5
Clinical significance of the pharmacists’ advice to solve identified DRPs has also been investigated in one of the projects including rheumatology and respiratory care patients. The clinical significance was graded according to Hatoums’ scale8 for intervention grading. The results showed that 85% of the pharmacists’ recommendations were graded to be of clinical importance for the patients (grade ≥3 as per Hatoums’ scale: somewhat significant, significant, very significant, extremely significant).
Drugs involved in DRP
The Anatomic Therapeutic Chemical (ATC) Classification System9 has been used to classify the drugs associated with discrepancies and DRPs. According to our findings, the five most frequent drug groups involved were: A—Alimentary tract and metabolism; B—Blood and blood-forming organs; C—Cardiovascular system; N—Nervous system; R—Respiratory system. This is not unexpected, due to the fact that these groups also represent the most used drugs in Norway.10 Some of the drugs that were most often associated with discrepancies or DRPs were: codeine, oxazepam, metoprolol, acetyl salicylic acid, citalopram, levothyroxine and paracetamol.
Mini-audits
Medicines reconciliation
The patients included in the mini-audits were somewhat similar to the patients included in the studies presented above, that is, orthopaedic, rheumatology, internal medicine and cardiology. Likewise, the results from the mini-audits are also comparable to the results from the projects. On average, we found 2.1 discrepancies per drug history obtained, and between 60% and 70% of the patients had one or more discrepancies in their drug history taken on admission to hospital. The most common discrepancy was due to omission of drug(s).
The groups of drugs which were most often involved in discrepancies were from the ATC groups:9 A, B, C, N and R. Some of the drugs repeatedly involved in discrepancies and highlighted as high-risk drugs were: insulin, warfarin, immunosuppressants, eye drops, β-antagonists and antihypertensives/diuretics.
These results, and the results from the project studies, emphasise the importance of taking a detailed and thorough drug history for all patients. In Norwegian hospitals, there are not enough pharmacists available to offer medicines reconciliation to all patients admitted and discharged from hospital, and we therefore have to look at other solutions to increase patient safety. Medicines reconciliation, as a part of the electronic prescribing system, is one way of increasing the focus on correct drug history taking, documentation and follow-up. Another alternative could be that of having a referral system for patients being prescribed a high number of drugs, or high-risk drugs, to be seen by a pharmacist. A third approach could be to extend the training of doctors and nurses to increase their competencies in drug history taking and medicines reconciliation.
Medication review
We found that up to 80% of the patients could potentially experience, or had experienced, DRPs. The clinical pharmacists found, on average, 2.2 DRPs per patient in the hospital studies. The DRPs were discussed with the responsible doctor, and in some cases with the nurse, if appropriate. The multidisciplinary teamwork was essential for optimising the drug treatment for each patient.
The most common categories of DRPs found were:
-
need for additional therapy
-
inappropriate use of drug(s)
-
drug interactions
-
suboptimal monitoring of drug treatment.
With regards to groups of drugs most often involved in DRPs, the ATC groups9 were: A, B, C, J, M, N and R. Some of the drugs repeatedly involved in DRPs and/or highlighted as high-risk drugs were: antihypertensives, opioids, NSAIDs, statins, antidepressants and benzodiazepines.
As hospital stays get shorter and care is shifted closer to home, some would argue medication review is more useful in community care compared with hospital care. We believe there is a clear need for optimising drug treatment at both levels of care, and the most important challenge is to ensure safe follow-up on drug treatment when changing level of care.
Questionnaires
A questionnaire on the quality of the clinical services was distributed to 421 doctors and nurses on the wards receiving the services. Forty-one per cent replied and nearly three-quarters of the responders were nurses. The doctors and nurses rated the clinical pharmacy services to be very good (5.5 out of 6) with regards to patient benefits and usefulness for healthcare professionals. Fifty-seven per cent rated the services to be of very high value (6 out of 6) for the patients, and 54% rated it to be of very high value for themselves as healthcare professionals. This means that the pharmacists’ contribution to optimising drug therapy is greatly valued, and the doctors and nurses appreciate the pharmacist as a regular member of the multidisciplinary team.
The pharmacists’ contributions to patient safety are recognised by other health personnel. These are some quotations taken from the responses to the question ‘what are the advantages of involving pharmacists in multidisciplinary teams on the wards?’
More resources to perform thorough quality assurance work related to medicines reconciliation; secondarily increased awareness about DRPs; increased competencies among doctors and nurses; change of culture; more correct and appropriate use of drugs both during hospital stay and after discharge.
Consultant, Aalesund Hospital
Improved continuity and better follow up with regards to the use of correct drugs for each patient. My experience is that it's easy to ask the pharmacists and they are committed to each patient.
Nurse, St Olavs Hospital
A second questionnaire was given to the clinical pharmacists for evaluation of their thoughts about contributing to ensure safe use of drugs. The pharmacists rated the services to be of great value for the patients (5.5 out of 6) and for the doctors and nurses (5.1 out of 6). However, it is interesting that the pharmacists believe their contribution to the multidisciplinary team is less than perceived by the doctors and nurses. Still, the pharmacists did express that the clinical pharmacy services were highly valued for optimising and individualising drug therapy, and contributes to patient safety.
The questionnaire also explored the pharmacists’ experiences with the IMM model giving them the opportunity to evaluate the model, and looking at benefits and ways of improvements. The advantages seem to be that the model is systematic and structured and increases the standardisation of the clinical pharmacy services. Ways of improvements are to integrate the pharmacists even closer in the ward teams, and to more effectively use the available electronic tools, such as the electronic patient record and the newly introduced electronic prescribing module, for effective communication.
Finally, a patient satisfaction survey was conducted. The patients also rated the service highly (3.5 on a 4-graded scale). The patients seemed to be very satisfied with the pharmacists’ advice on medicines management and drug administration, and to give information about the specific drugs the patient was taking. The comments from the patients express their positive experience with the clinical pharmacy services:
I feel safer with regards to my drug treatment. (Male, 30–49 years).
High-skilled and updated information. (Male, 50–69 years).
What now?
Our research and quality assurance work is continuous. Since the evaluation process was completed, five more projects have been completed and, additionally, one PhD, one postdoctoral, and other projects are on-going. Our projects are focusing on quantitative and qualitative research. Most of the quantitative studies are descriptive in nature and do not have hard endpoints as outcome measures. One controlled study completed in 2013 in a surgical unit showed that medication reconciliation performed by nurses who received training in medicines reconciliation, significantly reduced the discrepancies in patients’ drug history on admission to hospital. We also have some projects (one on-going and two in the pipeline) designed to evaluate the effect on clinical pharmacy services on clinical outcomes, such as hospital readmission, mortality and survival rate (unpublished data from Aalesund Hospital). The effectiveness of IMM and LIMM have been extensively investigated by others.3 ,4 ,11
The quality of our services may depend on individual competencies of the team members, how the professions work together in the team and across teams, for the patients, imaginary borders in the healthcare system. Applying the IMM model in hospitals is a complex intervention, and the context is very important.12 As explained in the introduction, our clinical pharmacists are not employed by the hospital. The ability to focus on optimising the drug therapy for individual patients therefore depends on how the pharmacists are integrated in the ward team. Thus, we have started to work with qualitative research methods to better understand the context and what is necessary for succeeding in the implementation of IMM. The results from the qualitative studies will, hopefully, become a valuable contribution in our work to optimise our clinical pharmacy services.
Acknowledgments
Many thanks to the ward staff welcoming the pharmacists on the wards and completing the questionnaires. Thanks also to the patients participating in the patient survey. Many thanks to all the pharmacists who have contributed to the data collection and assisting with conducting the questionnaires. A big thank you to everyone who contributed to this article.
Footnotes
-
Collaborators Marit Buajordet, Kristine Lundereng, Kari-Anne Fagervoll, Elizabeth Aa, Anne Marie Gjerde, Eva M. Nor Buset, Kristin Midtdal, Astrid Gilje Hageler.
-
Competing interests None.
-
Provenance and peer review Commissioned; internally peer reviewed.