Article Text

Abstract
Purpose Exercise may be associated with increased health-related quality of life (QoL) in patients with cancer, but it is not prescribed as standard care during or after cancer treatment. We systematically reviewed the methodological quality of, and summarised the evidence from, randomised controlled trials (RCTs). A meta-analysis was performed to examine the effectiveness of exercise in improving the QoL in patients with cancer, during and after medical treatment.
Methods RCTs that met the PICO (Patient Intervention Control Outcome) format were included in this study. 16 RCTs were identified through a search of Embase, Medline (OvidSP) and the Cochrane Library. These trials were reviewed for substantive results and the methodological quality was assessed using the Delphi criteria list.
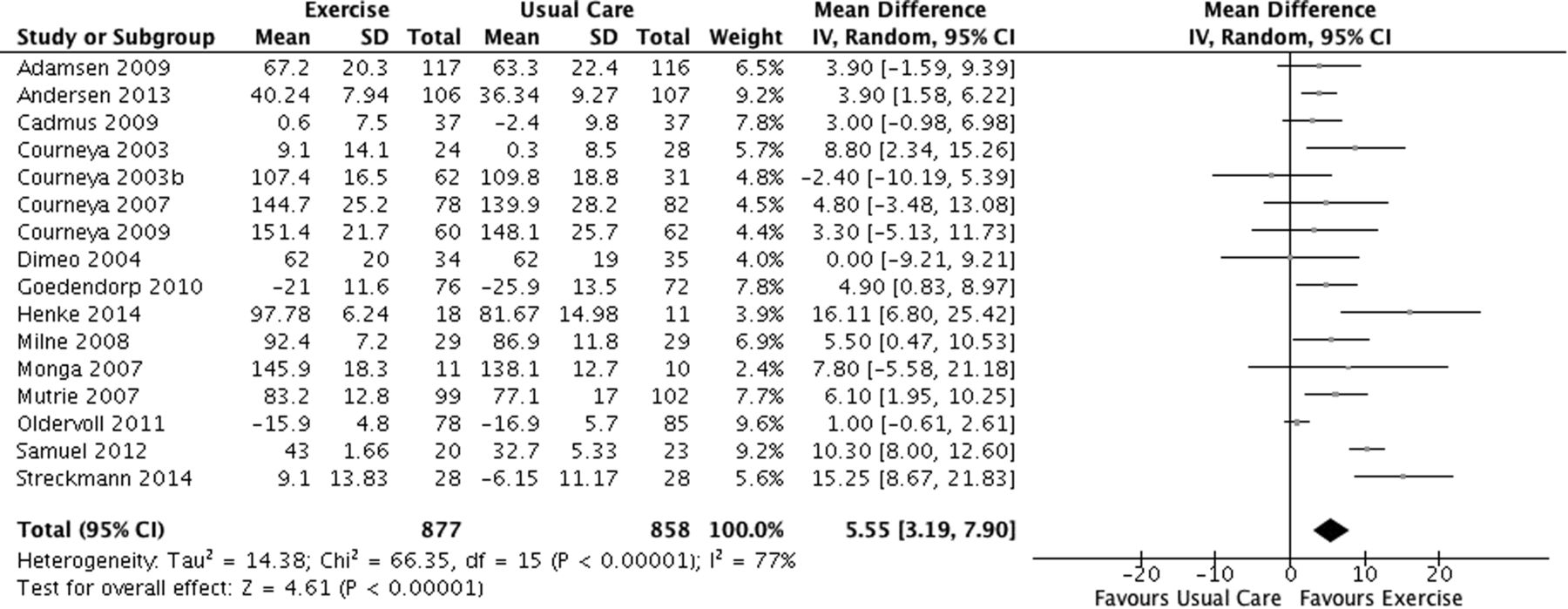
Results Exercise interventions differed widely in content, frequency, duration and intensity. Based on the meta-analysis, exercise improved QoL significantly in patients with cancer as compared to usual care (mean difference 5.55, 95% CI (3.19 to 7.90), p<0.001). Other outcomes closely related to QoL, such as fatigue and physical functioning, also improved.
Conclusions Exercise has a direct positive impact on QoL in patients with cancer, during and following medical intervention. Exercise is a clinically relevant treatment and should be an adjunct to disease therapy in oncology.
- Exercise
- Cancer
- Quality of life
- Fatigue
- Meta-analysis
Statistics from Altmetric.com
Introduction
Cancer is an important global condition.1 ,2 Many cancer survivors have a normal life expectancy.3 Physical inactivity is associated with an increased likelihood of developing a range of cancers, including colorectal cancer,4–9 breast cancer10–13 and prostate cancer.14–16 Cancer care itself is increasingly directed towards developing interventions such as exercise to improve (health related) quality of life (QoL) and prognosis.17–21 Although exercise may increase QoL during or after therapy, few RCTs have tested exercise as a therapy in this setting, and exercise has yet to be implemented as standard care for patients with cancer. Therefore, the methodological quality and evidence of RCTs that have investigated the impact of exercise on patients with cancer were systematically evaluated and summarised.
Methods
Search strategy
A computer-aided search of Embase, Medline (OvidSP) and the Cochrane Library was performed to identify relevant RCT studies. The search terms used were (exercise OR kinesiotherapy OR physical activity OR kinesitherapy OR walking OR swimming OR cycling) AND (neoplasm OR chemotherapy OR radiotherapy OR cancer OR tumour OR glioma OR lymphoma OR myeloma OR melanoma) AND (prognosis OR QoL OR prognosis OR survival OR mortality OR QoL OR cancer prognosis OR cancer survivor OR cancer mortality) AND (random OR factorial OR crossover OR placebo OR double OR single OR blinded OR assigned OR allocated OR volunteered OR meta-analysis OR crossover OR double-blind procedure OR randomised controlled trial) NOT (animals). One reviewer (JKWG) performed the initial search in association with a senior associate of the library service of Erasmus Medical Centre, who verified the search. Reference lists of the studies were searched for additional valuable studies. No restrictions were made regarding the language in which the study had been written or the year of publication.
Inclusion criteria and data collection
To be included in the systematic review, all RCTs had to have examined the effects of exercise during or after treatment (chemotherapy and radiotherapy) or after surgery, compared with a placebo, controlled comparison or standard care. Studies that used exercise as intervention to improve the patients’ (health related) QoL were reviewed. QoL was assessed by self-reported questionnaires such as the EORTC-QLQ-30, the Functional Assessment of Cancer Therapy: FACT-G (FACT-An, FACT-B, FACT-C, FACT-P), or the Short Form (36) Health Survey (SF-36). Exercise was defined as ‘a planned, structured and repetitive bodily movement, the objective of which is to improve or maintain physical fitness.’22 Examples of exercise are purposeful walking, running, cycling and strengthening exercises, performed under supervision or at home.
Only completed RCTs meeting the PICO format23 of this study where full-text versions were available were included (figure 1). PICO (Population Intervention Comparison Outcome) restrictions were made for intervention (relaxing exercises or yoga as primary intervention were excluded) and outcome: eligible primary outcomes were QoL and self-reported health-related QoL (HRQOL). Secondary outcomes included fatigue, physical functioning and performance, length of hospital stay, general practitioner visits, social functioning and peak oxygen consumption. Studies were excluded if they were not of RCT design, did not meet the PICO format of this study, were only available in abstract form, or were currently in progress.

Selection process of eligible RCTs. RCT, randomised controlled trial; PICO, Patient Intervention Control Outcome.
Assessment of methodological quality
The methodological quality of the studies was assessed according to 7 of the 9 criteria of the Delphi criteria list:24 use of well-described appropriate randomisation; concealment of treatment allocation; equivalence or similarity of groups at baseline; specification of the eligibility criteria; blinding of the assessment of outcomes; reporting of point estimates and measures of variability for the primary outcome measures; and use of an intention-to-treat analysis. Since it is impossible to blind patients and care providers to treatment assignment, two of three criteria responsible for assessing blinding procedures were not rated. For each of the remaining seven criteria, two rating categories were used; either reported (+), or not-reported (−). The Delphi criteria were used, because they offer both an easy and effective way to qualitatively assess the methodology of a study, and offer the potential to compare studies thoroughly.
Comparison between studies
In order to analyse the studies in a broader perspective, a comparison between the studies was made (table 1). Type of cancer, type of exercise, frequency of the intervention, duration of the intervention, length of follow-up, total exercise time and timing of the intervention, were compared. Studies that were unique in the type of cancer population or intervention frequency investigated were excluded due to the impossibility of comparison with other studies.
Comparison of exercise interventions between studies
Statistical analysis
Standardised mean differences and their 95% CI were calculated from raw data using patients from usual care as control groups. A meta-analysis was performed with QoL as the outcome measure using Review Manager Software (RevMan, 5.3; http://ims.cochrane.org/revman).
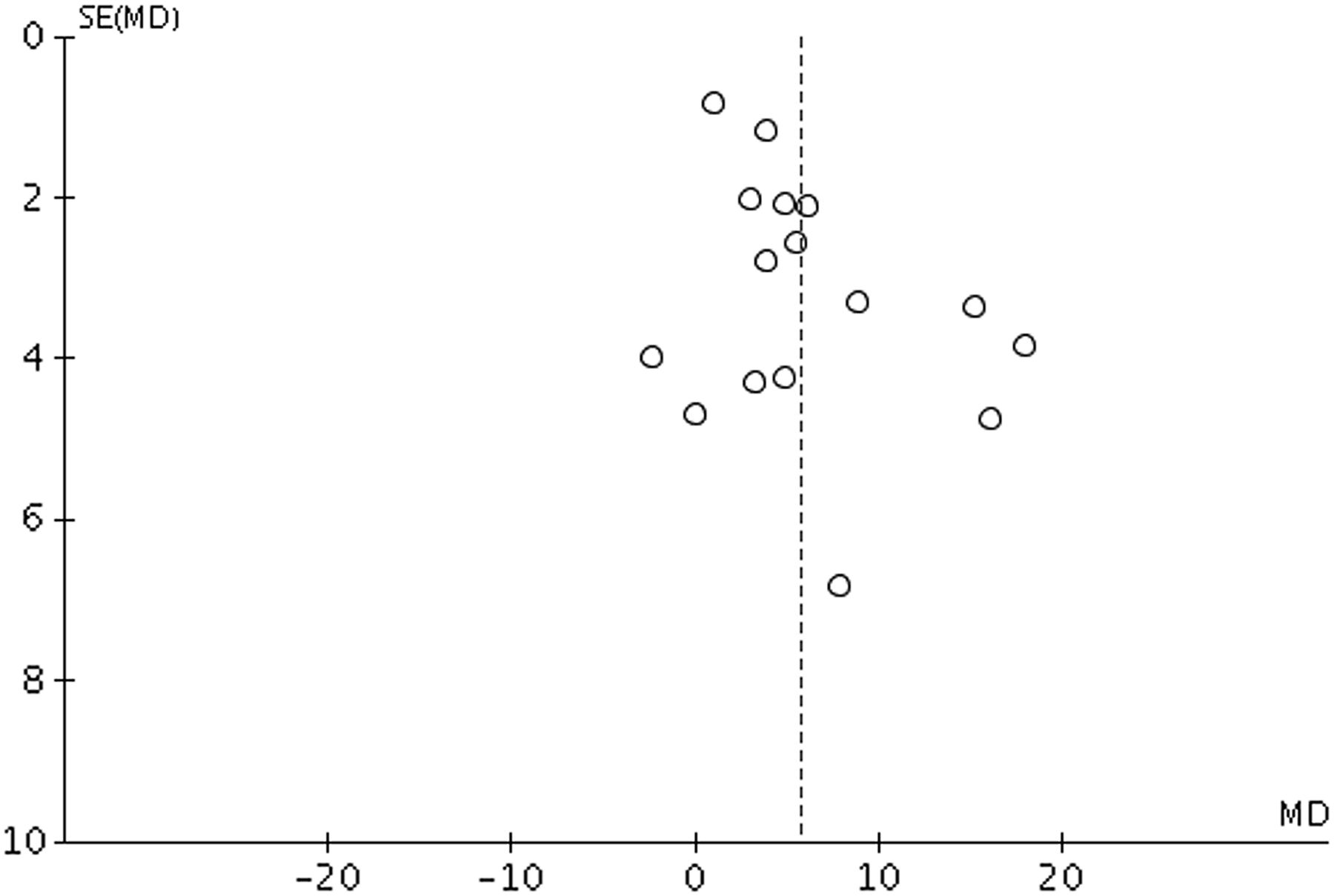
A random-effect model was used as opposed to a fixed-effect model due to the fact that study heterogeneity had to be taken into account. Because it was expected that scale differences of the QoL between studies might be present, the standardised mean difference was used. It has the advantage of resulting in a summary estimate that is free of the original measurement scale. Each study was weighted by sample size. Heterogeneity of treatment effects between studies was tested using the Q (heterogeneity χ2) and Ι2 statistics (Ι2 ≥50% indicating presence of heterogeneity). Overall effects were determined using a Z-test. To detect publication bias in the included studies, funnel plots were investigated for asymmetry.
Results
Study characteristics
The initial search yielded 6545 records, of which 5122 remained after duplicates were removed. Seven additional records were identified through alternative search strategies, mainly by searching the reference lists of the studies, increasing the total number of records identified to 5129. Following screening by title and abstract, 156 articles were considered relevant and were assessed for eligibility. Review of these 156 articles led to the inclusion of 16 studies in the qualitative synthesis. Studies varied significantly in methodology, exercise regimen, interventions and reported outcomes (table 2).
Description of studies of exercise in patients with cancer
All articles were of RCT design, 14 with usual care controls, one with an aerobic versus relaxation group and one with an immediate exercise group versus a delayed exercise group. Study groups included patients with mixed, breast, lymphoma, colorectal, prostate and lung cancer, respectively, in six, five, two, one, one and one article(s). Sample size ranged from 21 to 269 patients.
A variety of exercise modalities were employed, varying in: type, walking,27 ,31 ,33 ,35 ,38–40 cycling,25–34 ,36 strength training,25 ,37–39 swimming,27 stability training,36 elliptical trainer;38 intensity, with most programmes at 60–80% of the estimated VO2 maximum heart rate; frequency, ranging from two times a week to five times a week; and duration, ranging from 3 weeks to 16 months.
Primary and secondary outcomes
QoL summary estimates were based on data from all 16 studies. The standardised mean difference summary estimate, based on 877 patients in the exercise groups and 858 in the control groups, was 5.55 (95% CI (3.19 to 7.90), p<0.001). In other words, exercise significantly improved QoL, in comparison to usual care, among patients with cancer (figure 2). Additionally, the funnel plot did not suggest the presence of significant publication bias in this review (figure 3).

Forest plot.

{kind=link}
{kind=link}
{kind=link}
Funnel plot.
Eight studies (50%) showed a significant improvement in QoL in the exercise group in comparison with the usual care group,26 ,31–34 ,36 ,38 ,39 and an additional three studies reported a borderline statistically significant improvement of QoL.25 ,35 ,37 Significant improvements were also reported in relation to peak oxygen consumption,26 ,28 self-esteem,28 physical functioning,29 ,30 ,37 ,39 fatigue,25 ,31 ,34 ,40 length of hospital stay and general practitioner visits33 and social functioning.35
Assessment of methodological quality
The median criteria score on the Delphi list (range, 1–7) was 6, and the mean score was 5.3 (table 3). Two studies25 ,26 (13%) met all seven methodological criteria. All studies performed a method of randomisation. Nine studies25 ,26 ,28–33 ,35 (56%) avoided potential selection bias, using an appropriate method to conceal the allocation of the treatment. Fourteen studies26–39 (88%) reported group similarity at baseline. All 16 studies explicitly stated the eligibility criteria. The outcome assessors were blinded in 3 of 16 studies.25–27 All studies provided point estimates and measures of variability for primary outcome(s). Twelve studies (75%) performed an intention-to-treat analysis.25–34 ,36 ,38
Methodological quality of studies
Comparison between studies
Three studies with mixed types of cancer (50%) reported a significant improvement in QoL. Two of these studies reported a significant improvement in physical performance,30 ,37 and three of these studies reported a decrease in fatigue.25 ,31 ,34 Three studies on patients with breast cancer (60%) reported a significant improvement in QoL. Four of these studies also reported a significant improvement in peak oxygen consumption,26 self-esteem,28 length of hospital stay and general practitioner visits33 and social functioning.35 One of the lymphoma studies (50%) reported a significant improvement in QoL.36 In another of these studies, a significant improvement in physical functioning was also reported.29
Frequency of the exercise intervention varied between two and five times a week. One study with an intervention frequency of two times a week reported a significant improvement in QoL (50%), and one study reported a significant improvement in physical performance37 (50%). Four studies with an intervention frequency of three times a week reported a significant improvement in QoL (50%), and eight studies (100%) reported a significant improvement in peak oxygen consumption,26 ,28 self-esteem,28 physical functioning,29 length of hospital stay and general practitioner visits33 and a decrease in fatigue.25 ,35 ,40 Three studies with an intervention frequency of five times a week reported a significant improvement in QoL (60%), and four studies (80%) reported a significant improvement in physical performance,31 ,40 social functioning35 and a decrease in fatigue.31
Duration of each exercise intervention differed between 15 and 90 min, with an average of 42.5 min. For comparative purposes, studies where the intervention duration was 45 min or under were assigned to one group, and studies where the intervention duration was over 45 min were assigned to a second group. Five studies among those with an intervention duration of ≤45 min (50%) reported a significant improvement in QoL, and six of the studies (60%) reported a significant improvement in peak oxygen consumption,26 ,28 self-esteem,28 physical functioning and performance,29 ,30 ,40 length of hospital stay and general practitioner visits38 and social functioning.35 Three studies among those with an intervention duration of >45 min (50%) reported a significant improvement in QoL, and five of the studies (83%) reported a significant improvement in physical performance60 and a decrease in fatigue.25 ,31 ,34 ,40
The duration of follow-up differed between 3 and 65 weeks, with an average of 17.2 weeks. The authors classified the studies into a group of studies with a follow-up duration of ≤16 weeks and a group with a follow-up duration of >16 weeks. Five studies with a follow-up duration of ≤16 weeks (45%) reported a significant improvement in QoL, and eight of the studies (73%) reported a significant improvement in fatigue,25 ,34 ,40 peak oxygen consumption,25 physical functioning and performance,29 ,30 ,37 and length of hospital stay and general practitioner visits.33 Three studies with a follow-up duration of >16 weeks (60%) reported a significant improvement in QoL, and five of the studies (80%) reported a significant improvement in self-esteem,28 peak oxygen consumption,28 social functioning,35 physical performance39 and a decrease in fatigue.30
Studies in which the intervention took place during cancer treatment were assigned to one group, and studies with a post-treatment intervention were assigned to a second group. Six studies with patients receiving the exercise interventions during cancer treatment (46%) reported a significant improvement in QoL, and 12 of these studies (92%) reported a significant improvement in self-esteem,28 peak oxygen consumption,28 physical functioning and performance,29 ,30 ,37 ,39 length of hospital stay and general practitioner visits,33 social functioning35 and a decrease in fatigue.25 ,31 ,34 ,40 One study with patients receiving the exercise interventions after cancer treatment (33%) reported a significant improvement in QoL, and one of the studies (33%) reported a significant improvement in peak oxygen consumption.27
Discussion
Studying QoL in patients with cancer is important because of the implications that it can have on new treatments and health protocols. QoL is increasingly recognised as an important topic in patients with cancer. Decisions to prolong life for only a short length of time using costly drugs should be weighed against a possible decrease in QoL. Prescribing these costly drugs must also be weighed against the cost of alternative treatments. If no effective cure is available, an emphasis should be placed on improving health-related QoL. We found that regular exercise in patients with cancer may increase QoL and QoL-related factors.
Definition of exercise
As stated earlier, exercise was defined as ‘a planned, structured and repetitive bodily movement, the objective of which is to improve or maintain physical fitness’.22 Notice that the term ‘exercise’ differs from ‘physical activity’. Physical activity is defined as ‘any bodily movement produced by skeletal muscles that results in energy expenditure’.22 The key difference is the planned character of exercise, rather than the unstructured character of physical activity, which means that exercise is easier to measure and compare. However, by defining these terms one may have the impression that they are separate entities, despite a significant practical overlapping in the real world, with physical activity often as intense as structured exercise.
Methodology
The methodological quality of the studies was measured. The median score on the assessment was 6, and the mean score was 5.3. These scores were based on a full-score of 7, representing excellent methodological quality of the study in question. Most commonly observed omissions were blinding of the outcome assessor (81%)28–40 and concealing the treatment allocation (44%).27 ,34 ,36–40 The studies of Adamsen25 and Courneya26 scored the highest on methodological criteria with optimum score. Although the methodological quality of the studies could be considered adequate, future RCTs could be optimised if authors were to take all the information requested by the Consort checklist into consideration before submitting manuscripts for publication.41 Uniformity in future high quality designed trials will further optimise QoL in patients with cancer.
QoL and related factors
Based on our meta-analysis, exercise significantly improved QoL in patients with cancer in only eight RCT's (50%) as compared to usual care (table 2). However, exercise was associated with superior outcomes for variables closely related to QoL in 11 RCTs (70%), including peak oxygen consumption,26 ,29 self-esteem,28 physical performance and functioning,29 ,30 ,37 ,39 fatigue25 ,31 ,33 ,41 and social functioning.34 Moreover, the exercise groups had shorter hospital stays and less general practitioner visits.33 Although physical performance and social functioning are important features, fatigue, especially, is now recognised as the most common and distressing adverse effect of cancer and cancer therapy.42 Fatigue usually increases during radiotherapy, chemotherapy and hormonal and/or biological therapies.42 The estimate prevalence of fatigue during treatment ranges from 25% to 99%, depending on cancer population and treatment regime. Fatigue has a negative impact on work, social relationships, mood and daily activities, causing significant impairment in QoL during and after treatment. The highly selected RCT's convincingly show the effect of exercise on fatigue and other QoL-related factors in patients with cancer.
Frequency, duration and timing of exercise
Frequency of the exercise intervention varied between two and five times a week. Exercising at a frequency of five times a week was not significantly better in improving QoL than exercising two or three times a week (table 1). However, exercising more frequently than two times a week did significantly improve outcomes closely related to QoL, such as peak oxygen consumption, self-esteem, fatigue and length of hospital stay and general practitioner visits. When exercising at least five times a week, only a significant improvement in social functioning was observed.
Duration of each exercise intervention averaged 42.5 min. Short workouts were not superior in improving QoL than longer workouts: half of the studies with a workout duration of, <45 min and >45 min, found significant improvements in QoL. However, studies with shorter workouts found significant improvements in peak oxygen consumption, self-esteem, physical functioning and performance, length of hospital stay and general practitioner visits, and social functioning. Studies with longer workouts also found significant improvements in physical performance and fatigue, but not in other QoL-related aspects, for example, self-esteem and social functioning. It can therefore be concluded that short, intense bursts of exercise lead to both, physical and mental improvement, but longer workouts will only improve physical fitness in patients with cancer.
Timing of intervention was important: exercise improved QoL or related outcomes significantly more often in studies with an exercise as an intervention during cancer treatment, as compared to studies with exercise as a post-treatment intervention. Moreover, exercise during cancer treatment was associated with both, physical and mental improvement, whereas exercise after cancer treatment only improved physical fitness.
The findings in this study show that patients with cancer profit from regular exercise at least three times a week, and most preferably five times a week, with short intense exercises. The exercises will have most impact on QoL and related factors during treatment with radiotherapy or chemotherapy. This is most probably explainable by the negative impact of radiotherapy and chemotherapy on fatigue and the positive effect of exercise on this factor.
Type of cancer
Improvements in QoL did not differ greatly between types of cancer. Half of the studies examining the effect of exercise in patients with mixed types of cancer and lymphoma reported a significant improvement in QoL, whereas 60% of the studies examining patients with breast cancer reported a significant improvement in QoL. In all types of cancer, a significant improvement in physical fitness was reported. Significant improvements in self-esteem and social functioning were reported only in patients with breast cancer, indicating that these patients were not only physically—but also mentally—benefitting from the exercise programme. It is important to report that none of the 16 RCT's reported adverse effects of exercise. The most common cancer types are susceptible to the beneficial effects of exercise and can thus be implemented in the standard care of these patients. However, the effects of exercise on patients with rare cancer types—such as high grade glioma—are unknown and should be researched further.
Limitations
Examining QoL in RCTs could have some limitations. First, exercise itself cannot be blinded in the control group. The possibility that patients allocated to the exercise intervention subjectively feel better and therefore report to have better QoL cannot be ruled out. In future trials, biomarkers of health, exercise and QoL should be developed and be used as objective factors in new trials. Ideally, studies with a long follow-up period are needed in order to investigate and determine the effect of exercise on the recurrence of cancer and the prognosis of the patients, in terms of survival and long-term QoL as solid endpoints. QoL and longevity benefits resulting from exercise may vary as a function of the specific medical treatment of the patients, the stage of cancer, the type of cancer and the patients’ current lifestyle. Second, in studies examining QoL, patients commence the programmes with different initial QoL values and, as a result, some patients have more room for improvement in QoL than others. This phenomenon is called the ‘floor and ceiling effect’.43 The floor effect refers to patients who have a low QoL, and therefore have ample room for improvement. On the other hand, patients with an initial high QoL can improve to a lesser extent: the ceiling effect. Consequently, these effects could skew a certain treatment's effectiveness (or lack thereof), since patients with a low initial QoL are more likely to benefit from almost any intervention, while patients with a high QoL are less likely to improve from the same intervention. This is confirmed by Scherr et al,44 who examined the effect of carotid artery stenting (CAS) on the cognitive performance. Their data suggest that ignoring floor and ceiling effects might underestimate the positive effect of CAS on cognitive performance. When accounting for these effects, their sample showed significant improvements in cognitive performance, while they were not significant before accounting for floor and ceiling effects.
Third, studies that rely on patient-reported outcomes are susceptible to response shift bias.45 A patient's value, view or expectation can change during the course of the study, adding another factor of change on the end results. Surveys investigating QoL should therefore be recalibrated over time during the study to compensate for this shift.
Conclusions
In summary, exercise improves the QoL in patients with cancer and survivors in 50% of the RCT's but physical, psychological and social factors closely related to QoL improve in almost 70% of the RCT's. The study does not give answer to the optimal FITT (frequency, intensity, time, type) to improve QoL in patients with cancer. However, we found that exercising more frequently (three to five times a week) improves peak oxygen consumption, self-esteem, social functioning and fatigue, and decreases length of hospital stay and general practitioner visits. The study shows that shorter workouts significantly improved physical, psychological and social factors, whereas longer workouts only significantly improved physical factors. Finally, exercise during cancer treatment was associated with, physical and mental improvements, whereas exercise after cancer treatment only improved physical fitness. These findings indicate that short exercise workouts should be implemented at least three times a week in cancer treatment during standard care as an adjunct therapy to improve QoL and QoL-related factors such as fatigue. Therefore, exercise programmes warrant consideration as part of standard care in the treatment of cancer.
What are the findings?
Exercise significantly improved the health-related quality of life.
Exercise significantly improved physical, psychological and social factors.
Exercise should be implemented in standard care for patients with cancer.
How might it impact on clinical practice in the future?
Exercising three to five times a week yields the best results.
Intense, short workouts are superior to longer workouts.
Exercise should be implemented during standard care as an adjunct treatment.
References
Footnotes
Contributors JKWG and AJPEV were involved in the conception and design, acquisition of data and analysis and interpretation of data. Furthermore, they also involved in the involved in the drafting of the manuscript and critical revision of the manuscript for important intellectual content.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.