Article Text

Abstract
Objectives: It has previously been reported that lateral epicondylitis may be diagnosed with colour Doppler ultrasonography (US) by detecting hyperaemia inside the common extensor origin (CEO).This study reports on the association between Doppler US findings and the short-term response of US-guided corticosteroid injection in patients with LE.
Design: Case-only, blinded intervention study.
Setting: Secondary care at a government hospital.
Patients: 62 patients with LE verified by colour Doppler US.
Intervention: One US-guided corticosteroid injection was given into the CEO.
Main outcome measures: Patients were evaluated at baseline before the injection and at 2 weeks of follow-up. Outcome measures were changes in pain score and US parameters (resistive index (RI) and the amount of colour within the CEO). Prognosticators for outcome were: use of computer mouse, symptom duration, elbow strain, RI, colour fraction, Likert pain score, pain at rest, pain during activity, age, height, weight, disease in dominant versus nondominant arm.
Results: All but one patient experienced improvement of general elbow pain perception at follow-up at 2 weeks. In parallel, Doppler US showed significant reduction in colour fraction (mean (standard deviation) with 95% confidence limits: baseline 0.14 (0.10), at follow-up 0.02 (0.02), p<0.0001). All but five patients showed a decrease in colour fraction; 74% decreased to 0. No clinical or US parameter could distinguish responders from non-responders.
Conclusion: Corticosteroid injection has a marked short-term effect on pain and Doppler parameters. The reduction in hyperaemia mediated by an anti-inflammatory drug can be interpreted as evidence of an inflammatory component in LE.
Statistics from Altmetric.com
Tennis elbow or lateral epicondylitis (LE) is a common disease, and a variety of medical and physical treatments have been tried, with varying outcomes.1 2 The unstable response rates to these treatments could to some extent be ascribed to the uncertain diagnostic procedures and an absence of objective measurements of treatment success.
The lateral elbow pain may be caused by very different conditions, including those with pain originating from the neck and shoulder region, and localised conditions of the elbow region. None of these diseases has yet been fully clarified, and no common definition based on solid evidence has been agreed upon regarding the diagnoses.3
Although the term “epicondylitis” suggests an inflammatory condition, biopsies obtained at surgery do not show either acute nor chronic inflammation.4 These findings are in some contrast to the widespread use of local injections of glucocorticoids for epicondylitis, which is also an accepted treatment.5 6
Laser Doppler studies have shown an increased blood flow in the LE and MRI has shown oedema at the common extensor origin.4 7–10 Increased vascular activity in tennis elbow has been shown with power/colour Doppler ultrasonography (US).11 To further clarify the hypothesis of inflammation as part of the pathogenesis in LE, we conducted a comparative study of clinical signs and symptoms with Doppler US changes before and2 weeks after one targeted glucocorticoid injection in patients with well-defined LE.
METHODS
Written informed consent was obtained, and the study was approved by the local research ethics committee of Copenhagen (KF 01-022/00).
Patients
General practitioners were invited to refer patients with suspicion of LE to the outpatient clinic. Included were patients with LE with duration of >30 days. The major exclusion criteria were injections in the elbow within 3 months before the study and other musculoskeletal disease possibly affecting the condition of the elbow.
During the study period, the clinicians in the outpatient clinic saw all patients with LE. In this pre-screening check, patients with uncharacteristic sources of elbow pain, such as neck and shoulder problems, were excluded whereas patients with a significant suspicion of LE were sent for US. In total, 81 patients were eligible for the study. Of these, 19 patients had no Doppler activity, and the other 62 patients (34 men and 28 women, mean age 47 years, range 29 to 71), had a median LE duration of 6 months (interquartile range 2.5 to 18) with diagnosis of LE based on both US and clinical examination. These 62 patients formed the study group; 59 patients had unilateral LE, and 3 had bilateral LE.
METHODS
On the day of treatment (day 0) and at the 2-week follow-up, the following patient data were collected: grip strength of both hands; pain score on a 100 mm visual analogue scale (VAS) for grip strength test; VAS pain score for lifting a 2 kg dumbbell with the extended, pronated symptomatic arm (of these two VAS scores, only the larger was used as a measure of pain at activity); VAS pain score for elbow at rest; general elbow pain perception score (five-point Likert scale). The clinical examination included clinical elbow soreness (0–3) at the common extensor origin, lateral humeroradial joint line, and epicondylus lateralis humeri. Summation of these three sites generated a clinical elbow soreness measure ranging from 0 to 9.
The following parameters were obtained as prognostic indicators of outcome: use of computer mouse (0–3), duration of symptoms, physical strain on elbow (0–3), age, height, weight, and disease in dominant versus nondominant arm.
The patients were examined first clinically and then by US. Grip strength was determined after the US diagnosis and measurements were finished. Finally, injection therapy was given.
Ultrasonography examination
The elbows were examined with a US machine (Siemens Acuson Sequoia; Mountainview, California, USA) equipped with a linear array probe with a centre frequency of 14 MHz. The colour Doppler settings were the same for all patients with a gain setting just below the noise level using our set-up for low flow: Nyquist limit +/−0.014 m/s, lowest wall filter, and 7 MHz Doppler frequency. With this apparatus, all colour pixels in the image correspond to motion—that is, blood flow. We used colour rather than power Doppler, because at present the two methods have the same sensitivity on this particular machine.
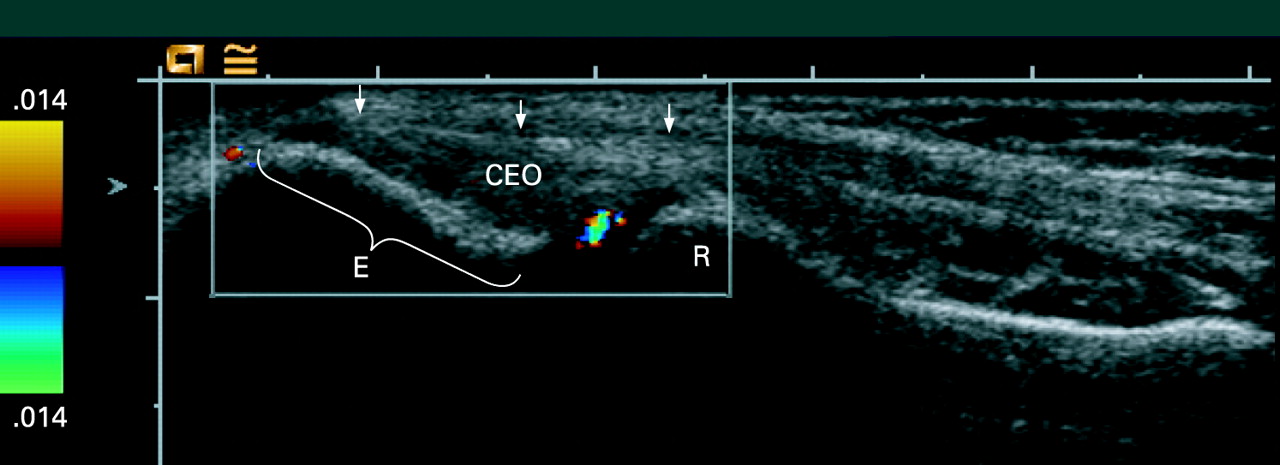
The patient was examined in the supine position with both elbows at 90° flexion and the hands resting on the chest. The elbows were placed on cushions. The transducer was aligned with the long axis of the radius over the common extensor origin (CEO) (fig 1).

The CEO was examined with colour Doppler US in the longitudinal plane by moving the transducer from side to side. Our region of interest (ROI) was limited proximally by the tip of the lateral epicondyle and distally by the humeroradial joint space. The superficial border was the most superficial fibres and the deep border was the bone, thus we included the lateral collateral ligament in the ROI. The medial and lateral limitations were defined by the borders of the head of the radius, thus,# the head of the radius had to be present in the image. Based on colour Doppler findings, the examiner diagnosed each subject as having no, left, right, or bilateral LE. The diagnosis of LE was defined as presence of colour Doppler activity inside the ROI.
If colour Doppler activity was present in the area of interest, the image with maximum colour activity was selected for quantitative analysis. The image was transferred to a processing program (Corel PHOTO-PAINT 7; Corel Corporation, Fremont, California, USA). Using a colour recognition function, the amount of colour pixels was expressed in relation to the total amount of pixels in the ROI (the colour fraction) (fig 2).

The flow pattern was evaluated with quantitative spectral Doppler with automatic calculation of the resistance index (RI) (fig 2). The RI is defined as: (peak systolic velocity−end diastolic velocity)/peak systolic velocity and was determined in three arteries within the ROI if possible, and on one muscular artery distal to the elbow region (for reference). The mean RI was used as an estimate of the inflammation. Low RI values are associated with low peripheral resistance, thus indicating high perfusion of the tissue.12 We used a maximum value of 1.00 for RI, because we had limited the analysis to one side of the Doppler baseline, as we sampled small vessels and most often sampled the artery and its concomitant veins simultaneously. The negative part of the arterial signal (if any) is then drowned out by the venous signal. When spectral Doppler measurements could not be measured due to lack of detectable arteries, the RI was taken as 1.00 (normal resting musculoskeletal tissues).13
Treatment
Symptomatic elbows with Doppler-positive LE were injected with a mixture of 1 ml methylprednisolone (40 mg/ml) and 0.5 ml lidocaine (1%). US was used to guide the needle to ensure that the injection was given into the area with pathological Doppler activity inside the common extensor origin (fig 3). All patients were instructed that the injection would be expected to result in a severe deterioration of the local symptoms for at least 24 hours. The patients were suggested to diminish this local reaction by applying a cold pack to the elbow and to take acetaminophen in doses of 1 g to a maximum of 3 g during the first day.

{kind=link}
{kind=link}
{kind=link}
Blinding of the ultrasonography investigator
In the study period, the US investigator scanned both elbows on all patients attending the clinic (patients with LE and patients with other disorders who had healthy elbows, who acted as controls). The investigator was blinded to the status of the subjects (control, unilateral LE, or bilateral LE) and was not allowed to speak with the subjects during the examination. Another investigator carried out the injection therapy.
Statistical analysis
Paired t test was used to test for differences between day 0 and day 14. Linear regression analysis was performed and coefficients of correlations calculated at both baseline and follow-up for clinical data and US measurements. Level of significance was set at p = 0.05.
RESULTS
Clinical examination
All but one patient had an improvement in the general elbow pain perception (Likert score) at the 2-week follow-up (table 1).
At two weeks follow-up, 82% of the patients experienced a decrease of pain at palpation compared to day 0. Ten percent of the patients had no change, and 8% experienced an increase of pain at palpation.
The VAS pain score on the dumbbell/grip strength test decreased from a mean of 47 (95% CI) 30 mm at baseline to 15 (24) mm after 2 weeks. Only two patients had an unchanged VAS score and none described deterioration.
Apart from immediate flare-ups after injection, lasting no more than 3 days, we found no adverse effects at follow-up. Specifically, no patients had injection induced pain.
Ultrasonography
The colour fraction before treatment was 0.14 (0.10) and 0.02 (0.02) at the 2-week follow-up (p<0.0001). At follow-up, four patients showed an increase in colour fraction, one showed no change, and all other patients showed a decrease in colour fraction. In total, 74% had a colour fraction of 0.
At the 2-week follow-up, the RI of 76% of the subjects who could not be measured and by our definition were therefore scored as 1.00, or had a measured value of 1.00. Nine patients showed a decrease in RI and two showed no change after 2 weeks (p<0.0001).
Association between clinical and US parameters
There was no correlation between any of the pain scores and the US measurements. Use of computer mouse did not correlate with pain scores or the US measurements.
Prognostic factors
Use of computer mouse (0–3), duration of symptoms, physical strain on the elbow (0–3), resistive index, colour fraction, Likert pain score, pain at rest (VAS), pain at activity (VAS), age, height, weight, disease in dominant versus nondominant arm did not predict the outcome at 14 days (Likert score, VAS at activity, pain at palpation, RI, or colour fraction).
Adverse events
Almost all patients reported a flare of symptoms within the first day after the injection. A few patients had a prolonged pain reaction and one patient was unable to use the hand for a full week. However, the degree of post-injection pain did not predict the outcome at follow-up.
DISCUSSION
At 2 weeks after steroid injection, there was an almost uniform disappearance of symptoms and a corresponding reduction of the vascular activity in the CEO. Patients with clinical LE and Doppler activity in the CEO had a 92% chance of reduced pain on palpation 14 days after steroid injection and a 74% chance of full remission of Doppler activity.
What is already known on this topic
Lateral epicondylitis is a tendinopathy in the common extensor origin.
Tendinopathy is regarded a degenerative disease and may have hyperaemia, which is interpreted as neovascularisation.
Lateral epicondylitis may be diagnosed with colour Doppler by detecting hyperaemia inside the common extensor origin.
What this study adds
A US guided steroid injection into the pathological region of the common extensor origin in patients with lateral epicondylitis results in short-term alleviation of symptoms and reduction or disappearance of Doppler pathology.
We interpret this as evidence of an inflammatory nature of the hyperaemia in lateral epicondylitis.
Our Doppler US diagnosis has previously been established with a suggested sensitivity of 0.95 and specificity of 0.88, and the risk of faulty inclusion of other diagnoses would seem low.11 As before, we believe that colour or power Doppler is a valuable tool in the US diagnosis of LE. This is because most of the grey-scale changes used by some investigators in the diagnosis (thickening, intrasubstance tears, calcifications, bone irregularities, focal hypoechogeneity, enthesophytes) take time to develop and are permanent.14 In contrast, as shown in this study, Doppler findings are dynamic and show active disease as well as treatment response. Thus, this study contains a very homogeneous LE population with a precise definition of pathology and of treatment, as all injections were monitored by real-time US, ensuring correct placement.
Hyperaemia is an integral part of inflammation, which is represented as redness and warmth and to some degree as swelling, due to increased vascular permeability.15 The pre-injection hyperaemia and subsequent post-injection reduction in this vascular activity were detected directly with colour Doppler US.11 Steroid is an anti-inflammatory drug, and we therefore attribute the reduction of vascular activity (hyperaemia) to a reduction of inflammation. The RI data also suggest an inflammatory component in the disease. Normal resting musculoskeletal tissue has a high peripheral resistance with no or little flow in the end diastole and the RI is close to 1.00.13 16 Our patient group had an initial RI of 0.74, which is similar to the value of 0.71 recorded in the synovium of inflamed joints in patients with RA and lower than the value of 0.85 recorded in healthy wrist and finger joints.13 17
Thus, both spectral and colour Doppler data show reduction in one of the key features of inflammation (hyperaemia) mediated by an anti-inflammatory drug as evidence of an inflammatory component in LE.
It has been debated that LE is a degenerative condition3 18 and some advocate that the “tendinitis myth” be abandoned.19 In a recent review, the possibility of an initial inflammatory reaction was discussed but no histopathological data supports this theory, which is unsurprising, as surgery is not performed in the acute stages.20 The prevailing theories are the mechanical (related to mechanical overload), vascular (related to areas with poor blood supply), and developing neural (related to a change in neural homeostasis leading to tendon pathology) theories. All three theories have strengths and weaknesses, and tendinitis/tendinosis is far from fully understood. Nevertheless, mainstream theory excludes inflammation and advocates the term tendinopathy to avoid the tendonitis/tendinosis discussion.19 20 The hyperaemia detected with colour/power Doppler is named neovascularisation/neovessels and believed to be part of the degenerative process.
We find the terms “neovascularisation” or “neovessels” premature because they imply that we know that the vessels have been newly formed or at least that they have been formed as part of the disease.21 We do not know this and they may just as well be dilatation of already present vessels. We do not know if the neovascularisation described (but not quantified) in chronic Achilles tendinopathy can be detected with present Doppler equipment.21–23 According to our observations, the hyperaemia seen in the common extensor origin is dynamic in nature and may decrease or disappear after an injection of steroid, which would hardly be the case if the vessels were part of neovascularisation in a degenerative process.
The results of this study cannot be used to recommend the use of steroid injection in the treatment of LE in favour of other treatments. The good short-term effect found in this study may be accompanied by poor long-term prognosis, as shown by Smidt et al., who reported poor long-term prognosis of steroid injection compared to physiotherapy or a “wait and see” policy. The present study focuses on the immediate effect of steroid injection and does not take into account the spontaneous course of the disease as investigated by others.24
We were not able to establish any prognostic indicators, which must be seen in the light of the very high response rate. Our results are in accordance with previous materials showing a very good short-term effect of steroid injections.25 26 The present US findings demonstrate that these patients do, in fact, go into a type of remission, characterised by absence or reduction of visible perfusion, which is otherwise a distinct marker of this disease.7 11 In terms of prognosis, clinical data did not add to the Doppler information. The response rate was the same regardless of usage of computer mouse, level of pain or duration of disease. This is in some contrast to another study, in which manual labour and high baseline pain were found to be associated with poor prognosis, although the treatment did not involve injections of steroid.27
Our injections were all delivered inside the CEO and may be regarded as intratendinous injections, even though the CEO is not a tendon per se. Intratendinous injections are traditionally avoided for fear of injection induced tendon rupture. This reservation is based on casuistic reports of rupture following steroid administration, and there are no published studies evaluating the risk of rupture with or without steroid injection.28 In contrast, we have previously reported on the possible safety of intratendinous steroid injection in the treatment of Achilles tendinopathy in a small material.29 What is meant by ‘in a small material’ in this context? Injection treatment for LE may be different from injection treatment of other tendinous structures, as we have not encountered the reservation for intratendinous injection in this literature where the definitions of the site of injection are imprecise: Injection into region of tenderness;30 ... that the injection was placed as deeply as possible and not into the subcutaneous tissues;31 ... delivered to painful elbow points;32 … was injected deep into the subcutaneous tissues and muscles 1 cm distal to the lateral epicondyle and aiming toward the tender spot;33 ... into the point of maximal tenderness at the extensor origin of the lateral epicondyle of the humerus.34 We believe that most investigators wish to target the tender spot while avoiding injection into the subcutaneous tissues for fear of fat necrosis. and therefore have made the injection deeper. Because the CEO is tender in LE and is placed immediately deep to the subcutaneous tissues it is likely that the CEO has been the target for injection in many of the existing studies. We therefore believe injection into the CEO to be a safe procedure.
In conclusion, the findings in this paper support the notion of an inflammatory component in LE. With Doppler US we are able to diagnose LE and guide injections into a well-defined pathologic area in the CEO. Doppler US seems to be useful in the objective assessment of treatment response.
Acknowledgments
This study was supported by the Hertz Foundation and the Oak Foundation.
REFERENCES
Footnotes
Competing interests: None.
Funding: This study was supported by grants from the Hertz Foundation and the Oak Foundation. The funding bodies had no influence on design or any other aspects of this study.