Article Text

Abstract
Background Not meeting functional performance criteria increases reinjury risk after ACL reconstruction (ACLR), but the implications for osteoarthritis are not well known.
Objective To determine if poor functional performance post-ACLR is associated with risk of worsening early osteoarthritis features, knee symptoms, function and quality of life (QoL).
Methods Seventy-eight participants (48 men) aged 28±15 years completed a functional performance test battery (three hop tests, one-leg-rise) 1 year post-ACLR. Poor functional performance was defined as <90% limb symmetry index (LSI) on each test. At 1 and 5 years, MRI, Knee injury Osteoarthritis Outcome Score (KOOS) and International Knee Documentation Committee (IKDC) subjective form were completed. Primary outcomes were: (i) worsening patellofemoral and tibiofemoral MRI-osteoarthritis features (cartilage, bone marrow lesions (BMLs) and meniscus) and (ii) change in KOOS and IKDC scores, between 1 and 5 years.
Results Only 14 (18%) passed (≥90% LSI on all tests) the functional test battery. Poor functional performance on the battery (all four tests <90% LSI) 1 year post-ACLR was associated with 3.66 times (95% CI 1.12 to 12.01) greater risk of worsening patellofemoral BMLs. A triple-crossover hop <90% LSI was associated with 2.09 (95% CI 1.15 to 3.81) times greater risk of worsening patellofemoral cartilage. There was generally no association between functional performance and tibiofemoral MRI-osteoarthritis features, or KOOS/IKDC scores.
Conclusion Only one in five participants met common functional performance criteria (≥90% LSI all four tests) 1 year post-ACLR. Poor function on all four tests was associated with a 3.66 times increased risk of worsening patellofemoral BMLs, and generally not associated with decline in self-reported outcomes.
- anterior cruciate ligament reconstruction
- osteoarthritis
- magnetic resonance imaging
- patient reported outcomes
- rehabilitation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- anterior cruciate ligament reconstruction
- osteoarthritis
- magnetic resonance imaging
- patient reported outcomes
- rehabilitation
Introduction
Rupture and subsequent reconstruction of the ACL (ACLR) substantially increases the risk of knee osteoarthritis (OA) development and poor quality of life (QoL).1 2 Yet not everyone after ACLR develops OA; radiographic OA is evident in approximately one-in-two,3 4 and one-in-three will have symptomatic radiographic OA within 10–15 years of injury.3 4 MRI can detect OA features within 5 years of ACLR,5–7 and can be used to identify individuals who may be on an accelerated trajectory towards radiographic, symptomatic OA.8 Understanding modifiable factors associated with structural changes early after ACLR is a priority to inform secondary OA prevention strategies.
Impaired functional performance, often measured through hop tests, is common following ACLR,9 and may influence the development of early knee OA and symptoms. Quadriceps weakness is a risk factor for the development of radiographic and/or symptomatic OA, based on the theory of impaired shock absorption, consequent excessive load to joint structures, initiating a degenerative process.10 Hop-test batteries provide a clinically feasible method to assess multiple aspects of lower-limb muscle function (including quadriceps strength, sensorimotor control) and may indicate reduced ability to control mechanical loading in the knee,11–13 thus influencing joint degeneration and/or potential symptoms. Functional performance impairments may represent lack of confidence in the limb,14 and be reflected in reduced physical activity and worse patient-reported outcomes (PROs).
Following ACLR, the link between functional performance and worsening symptomatic and early structural OA outcomes is unclear. While a single hop-for-distance test at 1 year post-ACLR was associated with the presence of tibiofemoral radiographic OA at 10 years,15 other studies have reported minimal association between postoperative functional performance and future radiographic OA 5–15 years post-ACLR.4 16 17 Prior studies focus on radiographic tibiofemoral OA, and do not evaluate early structural change (ie, worsening) in individual joint features. Despite the patellofemoral joint being burdensome post-ACLR,18 19 few studies consider the patellofemoral joint structure. Radiographic measures lack the sensitivity to detect early structural changes which are identifiable on MRI over shorter follow-up.20 21 No studies have reported the relationship between functional performance and early (<5 years) structural changes on MRI in an ACLR population.
Evaluation of risk factors for early OA after ACLR should also include concurrent assessment of change in PROs, given the discordance between knee imaging findings and symptoms.22 23 Functional performance may possess differing relationships with change in individual early OA features and PROs. Functional performance deficits at the time of return to sport (RTS) are often associated with worse PROs 2–3 years after ACL injury,16 24–28 with few studies evaluating the change in PROs beyond 3 years, due to cross-sectional design. It is this change in PROs and structural outcomes that equates to the problematic accelerated trajectory of symptomatic OA in young adults post-ACLR.
If early functional impairments are related to worsening structural or symptomatic OA, functional deficits can be targeted through exercise therapy to halt or slow the trajectory towards radiographic, symptomatic OA. The aims of the current study were to determine if functional performance 1 year post-ACLR is associated with risk of worsening patellofemoral and tibiofemoral MRI-OA features and change in PROs between 1 and 5 years.
Methods
Study design and participants
A longitudinal prospective cohort study assessed the trajectory of PROs, functional performance and early OA features 1–5 years post-ACLR. Individuals assessed 1 year post-ACLR (ie, baseline for the current study) (n=111; 64% male, median age 27 (range 19–51) years)5 were eligible for 5-year follow-up. Descriptions of baseline eligibility criteria, ACLR technique and postoperative rehabilitation have been published.5 Briefly, all participants underwent a primary single-bundle hamstring-tendon autograft ACLR. Exclusion criteria were: knee injury/symptoms prior to ACL injury, >5 years between ACL injury and reconstruction and any secondary injury/surgery to the ACLR knee (between ACLR and 1 year post-ACLR). Participants with a secondary injury between 1 and 5 years were invited to participate in the 5-year assessment, as this is common occurrence and represents the wider ACLR population. Of the 112 participants who completed baseline PROs, 81 (72%) completed PROs at 5 years. Of the 111 who underwent baseline MRI evaluation, 78 (70%) were re-imaged at 5 years (figure 1).
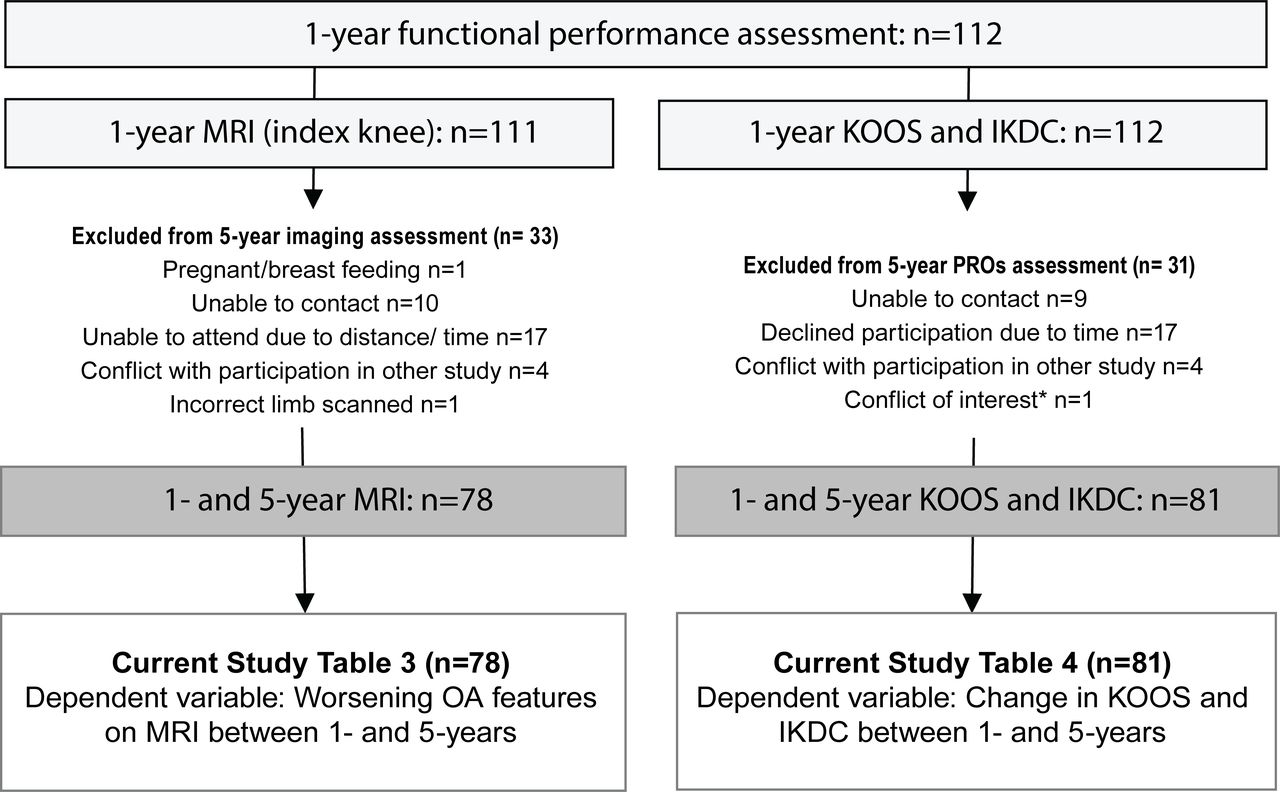
Flow chart of participant recruitment into the study. IKDC, International Knee Documentation Committee; KOOS, Knee injury Osteoarthritis Outcome Score; OA, osteoarthritis. *Participant at 1 year was involved in research team at 5 years.
Demographic, injury and surgical factors
Participant age, sex, height, weight, injury history, activity level (defined as level 1 pivoting/jumping sports to level 4 sedentary29) was obtained at the 1-year and 5-year assessments. Participants were classified as having a ‘combined injury’ if they had (at the time of ACLR): (i) significant cartilage defect identified arthroscopically (Outerbridge grade ≥2)30 or (ii) surgical resection or repair of meniscus. To determine the presence of tibiofemoral and patellofemoral OA in the ACLR limb, posteroanterior and lateral weightbearing, and non-weightbearing skyline views were taken, and graded according the Osteoarthritis Research Society International atlas definitions.31 Radiographic OA was defined as joint space narrowing of grade ≥2, sum of osteophytes ≥2 or grade 1 osteophyte in combination with grade 1 joint space narrowing.31
Functional performance
At 1 and 5 years post-ACLR, participants completed a battery of functional tests in the following order: single-hop, triple-crossover hop, side-hop and one-leg rise. The left leg was always tested first after two to three practice trials. The single-hop assessed the maximum distance (cm) achieved from a stationary position with a balanced landing (≥2 s without placing the other foot to the floor).32 The triple-crossover hop assessed the cumulative distance (cm) achieved with three consecutive hops with a balanced landing, with each hop crossing over two parallel lines 15 cm apart.33 Hops were repeated for the single-hop and triple-crossover until three successful trials were recorded, and until no increase in distance was seen, due to the known learning effects.34 The side-hop assessed the number of hops over two parallel lines 40 cm apart in 30 s.32 The one-leg rise is the maximum number of times (up to 50) the participant can rise on one leg from 90° knee flexion, at a consistent speed of 45 beats per minute (using a metronome).35 A hop test or one-leg rise test was scored zero if the participant was unable (due to lack of strength/balance/confidence) to perform one successful trial. The one-leg rise test was stopped if the participant received three warnings for deviating from speed or touching the ground with opposite foot. The one-leg rise was added to the traditional battery of hops as it also assesses endurance, and has been associated with the development of radiographic OA in those with chronic knee pain.35
The raw score (ie, distance hopped) and limb symmetry index (LSI) (% score of ACLR knee/contralateral knee) were recorded for each test. Poor functional performance on an individual test was defined as <90% LSI, a common benchmark used to define return-to-sport readiness,9 36 and is associated with risk of reinjury.37 38 Poor function on the battery was defined as <90% LSI on all four tests, to specifically capture individuals with poor function.
MRI-OA features
At 1 and 5 years post-ACLR, participants had unilateral (index) knee MRI scans acquired using a single 3T system (Philips Achieva, The Netherlands), as previously described.5 7 The three-dimensional proton density-weighted VISTA sequence was acquired at 0.35 mm isotropically (repetition time/echo time (TR/TE) 1300 ms/27 ms, field of view (FOV) 150 mm2 and echo train length 64 ms) and reconstructed in coronal and axial planes. The sagittal short-tau inversion-recovery sequence was at 2.5 mm thickness, 1.2 mm slice gap and an inversion time of 180 ms was applied with TR/TE 3850 ms/30 ms, FOV 160 mm2 and voxel size 0.45×0.50×2.5 mm. The axial proton-density turbo spin-echo sequence was obtained with imaging parameters of TR/TE 3850 ms/34 ms, slice thickness 2.5 mm, slice gap 2.0 mm, corresponding voxel size 0.5×0.55×2.5 mm and FOV 140 mm2. All MRI scans were evaluated using the MRI-OA Knee Score (MOAKS) by a musculoskeletal radiologist (AG) with 19 years’ experience of semi-quantitative MRI analysis of knee OA, and established inter-rater and intrarater reliability (kappa=0.61–0.80).39 The 1-year and 5-year images were read paired (not blinded to time-points), but blind to clinical information. The MOAKS divides the knee into subregions to score specific OA features. For the current study, cartilage defects, bone marrow lesions (BMLs) and meniscal lesions were semi-quantitatively graded.
Four subregions defined the patellofemoral joint (medial and lateral patella, medial and lateral trochlea) and 10 subregions defined the tibiofemoral joint (medial and lateral: femur central and posterior, tibia anterior, central and posterior). For grading of meniscal lesions, six subregions (medial and lateral: anterior, posterior and central) were combined. Cartilage defects and BMLs were graded from 0 to 3 based on size (percentage of surface area relative to each subregion, where 0=none, 1=<33%, 2=33%–66%, 3=>66%). Cartilage defects were also scored on severity based on depth of the lesion (percentage of lesion which is full thickness; 0=no full-thickness loss; 1=<10%; 2=10%–75%; 3=>75%). A meniscal tear was defined as an area of abnormal signal that extends to both meniscal articular surfaces, and meniscal macerations were defined as loss of morphological substance of the meniscus. Meniscal lesions were described as absent or present, and by type (a tear was either vertical, horizontal or complex; and maceration was partial, progressive or complete). These abnormalities were scored according to MOAKS scoring system. Meniscal extrusion was graded by size 0 (<2 mm); 1 (2–2.9 mm); 2 (3–4.9 mm) or 3 (>5 mm) in each of the subregions. Meniscal extrusion, while based on the amount of extrusion in mm, was also scored using the MOAKS.
Worsening OA features in each subregion was defined as any increase in the size or severity of the feature. Therefore, either progression of an OA feature (ie, increase in severity) or a new OA feature (ie, from absent to present) from 1 year to 5 years was classified as worsening. New OA features were defined as those with size=0 at baseline, and size >1 at follow-up. Increase in severity was defined as an increase in size or depth of an existing OA feature at 1 year by ≥1 point on the MOAKS. Worsening OA features in the patellofemoral and tibiofemoral compartment was defined as worsening in any corresponding subregion for that compartment, as previously described.7 40 This definition of worsening is reliable and sensitive to change in ACL-injured patients.6 7
Patient-reported outcomes
Participants completed the Knee injury Osteoarthritis Outcome Score (KOOS) and the International Knee Documentation Committee (IKDC) subjective knee form 1 and 5 years post-ACLR, with respect to their knee condition during the previous week. The KOOS and IKDC have established reliability and validity in people with ACL injuries.41 Four of the five subscales of the KOOS were assessed (activities of daily living subscale excluded due to ceiling effects in ACL populations). They were completed in by pen and paper or via an online portal (MySQL, Oracle, California, USA and Promptus, DS PRIMA, Melbourne, Australia) with matching instructions to the original paper version, as previously described.22 26 The KOOS and IKDC raw scores were recorded and converted to a percentile score, with 100 being the best possible score (ie, no knee problems). The absolute change (5-year score minus 1-year score) was calculated for each subscale (a negative value indicating worsening knee problems).
Statistical analyses
Generalised linear models with Poisson regression and generalised estimating equations (GEE) (accounting for correlations between subregions within the same participant) assessed whether functional performance at 1 year post-ACLR (both as a dichotomous (poor function≤90% LSI) and a continuous (ACLR limb raw score in cm/repetitions) variable) was associated with risk of worsening MRI-OA features. Risk ratios (RR) and 95% CIs were calculated. A RR >1.0 represents an increased risk of worsening OA features in the presence of poor functional performance (<90% LSI) or a lower functional performance score (ie, fewer repetitions). The GEE regression was adjusted for presence of a combined injury (noted at time of ACLR, or secondary injury to the index knee), 1-year age, sex, height and weight, due to their potential influence on function and MRI-OA features.7 Linear regression (β, 95% CI) determined the relationship between 1-year functional performance, and change in KOOS/IKDC scores between 1 and 5 years (adjusted for combined injury (noted at time of ACLR, or secondary injury to the index or contralateral knee), 1-year age, sex, height, weight and baseline KOOS/IKDC score, due to their potential to influence function and PROs22). Analyses were performed using Stata V.14.2 with α=0.05.
Results
Demographics of the 81 participants who completed PROs at 1 and 5 years are presented in table 1. Of the 81 participants, 10 (12%) had poor functional performance (<90% LSI) on all four tests, while only 14 (18%) would have passed the test battery (>90% on all four tests) at 1 year post-ACLR. The proportion of participants with <90% LSI on individual tests, and functional performance outcomes are presented in table 2. Of the 78 participants with radiographs at 5 years, the prevalence of any radiographic OA increased from 6% to 19% between 1 and 5 years (table 1). In those with poor function on the battery at 1 year (n=9/78), 33% (n=3) had patellofemoral or tibiofemoral radiographic OA at 5 years.
Participant characteristics at 1 and 5 years post-ACLR*
Functional performance 1 year post-ACLR*
Imaging outcomes
Worsening compartment-specific MRI-OA features and radiographic OA prevalence are reported in detail previously.7 Briefly, patellofemoral and tibiofemoral cartilage worsening (34 (44%) and 16 (21%) participants, respectively) was more common than BML worsening (14 (18%) and 12 (15%) participants, respectively). Seventeen (22%) participants displayed worsening meniscal lesions. Five (6%) participants displayed worsening of all three features, while 20 (26%), 4 (5%) and 7 (9%) had isolated cartilage, BML and meniscal worsening, respectively. Worsening osteophytes were not included in the current study due to low numbers in the patellofemoral (n=7) and tibiofemoral (n=9) compartments.7
Functional performance and risk of worsening early OA features
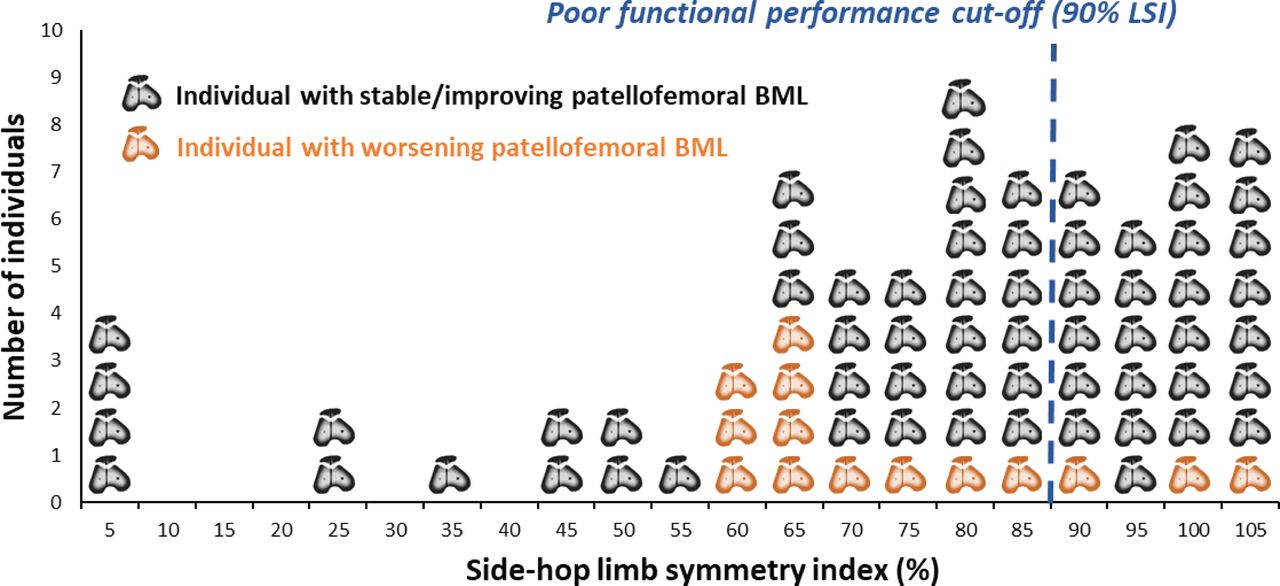
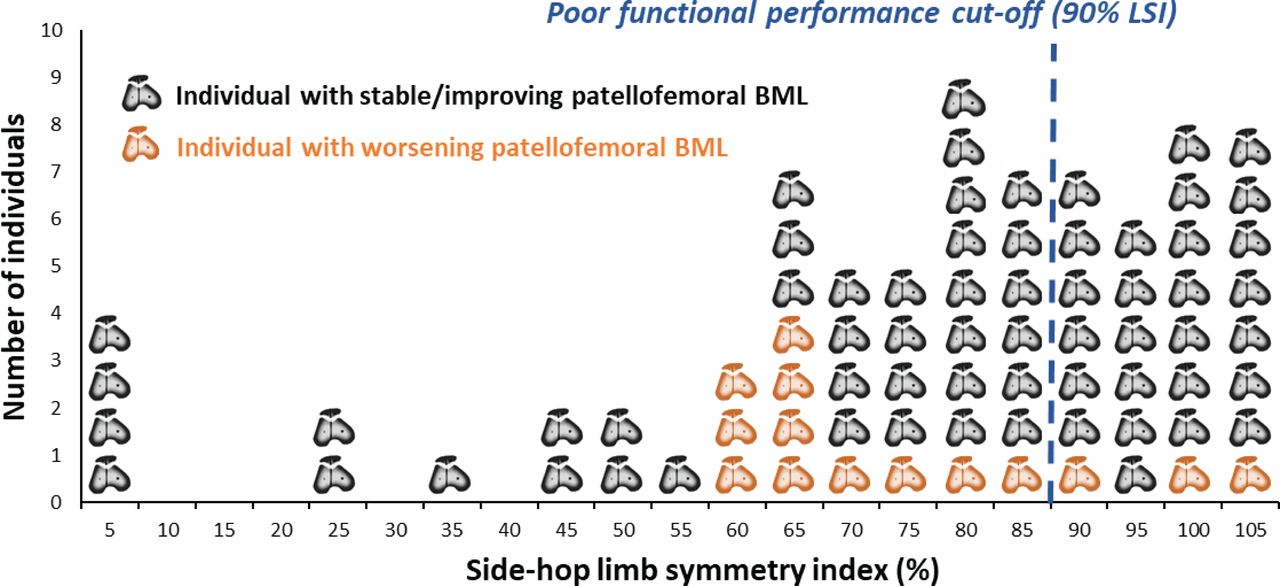
Poor functional performance on the test battery (<90% on all four tests) resulted in an increased risk of worsening patellofemoral BMLs (RR 3.66; 95% CI 1.12 to 12.01) (table 3). The majority (86%) of those with a worsening patellofemoral BML had <90% LSI on the side-hop (figure 2). Individuals with <90% LSI on the triple-crossover hop-for-distance had an increased risk of worsening patellofemoral cartilage lesions (RR 2.09; 95% CI 1.15 to 3.81). Individuals with <90% LSI on the single hop-for-distance, side-hop and one-leg rise had an increased risk of worsening patellofemoral BMLs (RR 4.17, 95% CI 1.37 to 12.72; RR 3.77, 95% CI 1.15 to 12.43 and RR 2.92, 95% CI 1.19 to 7.18, respectively). Fewer side-hop repetitions was associated with an increased risk of worsening patellofemoral BMLs (RR 1.08; 95% CI 1.01 to 1.15). In contrast, fewer one-leg rises was associated with a small reduction in risk of worsening tibiofemoral cartilage lesions (RR 0.96; 95% CI 0.94 to 0.99) (table 3).
Functional performance at 1 year and risk of worsening early osteoarthritis features up to 5 years*
{kind=link}
{kind=link}
Individuals with and without change in patellofemoral BMLs and respective side-hop limb symmetry index.* *LSI scores are presented in categories of 0%–5%, 5%–10% in increasing increments of 5% for purposes of visualisation. BML, bone marrow lesion; LSI, limb symmetry index.
Functional performance relationship with KOOS and IKDC
The 1-year and 5-year KOOS and IKDC scores (n=81) have been reported in detail previously.22 Significant (p<0.05) improvement (ie, less knee symptoms, better function and QoL) was observed for all KOOS subscales (except KOOS-Symptoms) and IKDC between 1 and 5 years.22 The mean±SD changes were: pain: 2.8±9; symptoms: 0.5±16.1; sport: 6.0±18.2; QoL: 10.0±18.9 and IKDC: 4.7±10.9. Generally, functional performance 1 year post-ACLR was not associated with change in KOOS or IKDC scores between 1 and 5 years (table 4). Participants with <90% LSI for the side-hop test had a mean 8-points higher KOOS-QoL change value (β: 8.08; 95% CI 1.56 to 14.61).
Functional performance at 1 year post-ACLR: relationship with change in KOOS and IKDC between 1 and 5 years*
Discussion
Only one in five participants met common functional performance criteria (≥90% LSI on all hopping, one-leg rise tests) 1 year following ACLR—a time when function is typically expected to be restored. In this first evaluation of the implications of not meeting functional performance criteria on early OA outcomes after ACLR, poor function (<90% LSI) was consistently associated with 2–4 times increased risk of worsening patellofemoral BMLs. While performance on the triple-crossover hop was also associated with worsening patellofemoral cartilage over the subsequent 4 years, weak/no associations were generally observed between poor function and tibiofemoral cartilage, bone marrow and meniscal lesions and changes in PROs.
Poor function and risk of worsening patellofemoral OA features
Poor functional performance was associated with an increased risk of worsening patellofemoral OA features, particularly BMLs. An LSI <90% on all four tests in the battery was associated with 3.66 times greater risk of worsening patellofemoral BMLs. When considered as a continuous variable (ie, number of repetitions), the side-hop test was associated with worsening patellofemoral BMLs—each one repetition decrease on the side-hop test could be interpreted as having an 8% increased risk of worsening patellofemoral BMLs (RR: 1.08). Given the association of BMLs with incident symptoms, future damage to adjacent features (ie, cartilage) and incident radiographic OA,8 42 43 these findings may help identify individuals on an accelerated trajectory towards radiographic OA.8 There is need to validate these findings in larger cohorts and to confirm which factors influence functional recovery. Previous cross-sectional evaluation of this cohort at 1 year post-ACLR found worse hop-test performance at 1 year post-ACLR was associated with patellofemoral pain, kinesiophobia, lower psychological readiness for RTS and worse knee confidence.14 19 Other factors that have been linked to functional recovery after ACLR, such as motivation, stress and self-efficacy,44 may also be important to target during supervised rehabilitation45 to optimise function. Future interventional studies should determine if improving functional performance can positively impact long-term patellofemoral joint health.
Do tibiofemoral and patellofemoral post-traumatic OA have different risk profiles?
Functional performance 1 year post-ACLR had little association with worsening tibiofemoral OA features in the following 4 years, concurring with other studies reporting minimal association between greater postoperative function or muscle strength and tibiofemoral radiographic OA 5–15 years later.4 17 The tibiofemoral and patellofemoral compartment may have a different association with function for the development of post-traumatic OA. Our results extend those from non-traumatic older OA populations, where lower-limb function (ie, quadriceps muscle strength) was more strongly associated with risk of patellofemoral disease progression than tibiofemoral.46 In contrast to patellofemoral disease worsening, our results indicate that poorer function (fewer one-leg rises) reduced the risk of tibiofemoral disease worsening. The mechanism underpinning this inverse (and unexpected) relationship is uncertain but is consistent with results in military recruits (aged 18 years), where lower quadriceps strength reduced the incidence of tibiofemoral OA 20 years later.47 Taken together with demographic and surgical-related factors which display compartment-specific relationships with post-traumatic OA progression,7 22 48 future studies should evaluate the patellofemoral and tibiofemoral compartments independently to determine distinct risk profiles—particularly as they may have differing impacts on disease burden.18 For example, patellar alignment (lateral patellar displacement) was weakly associated with worsening patellofemoral cartilage in this cohort,49 although when added as a covariate to the current statistical models, the relationship between function and worsening patellofemoral bone marrow and cartilage lesions did not change (data not shown). There is emerging appreciation of the greater risk of early5 7 and long-term radiographic patellofemoral OA,50 and potential contribution to symptoms,18 compared with tibiofemoral OA.
Challenges in predicting PROs
Functional performance 1 year post-ACLR was mostly not associated with change in PROs between 1 and 5 years. The only significant finding was that individuals with poor function (<90% LSI) for the side-hop test had an 8-point greater improvement in KOOS-QoL compared with those with good function (<90% LSI). Due to a low proportion (12%) scoring <90% LSI on all four tests, a sensitivity analysis calculated the RRs for poor function (<90% LSI) on any one, two or three tests, or at least one, two or three tests (ie, at least 2=all participants with two, three or four tests <90% LSI) (see online supplementary file 1). Similarly, poor function at 1 year on any or at least two tests was associated with 8–12 points greater improvement in KOOS scores. While 8–12 points approaches a clinically meaningful difference for the KOOS (≥8–10 points),41 these results should be interpreted with caution. Individuals with poor function 1 year post-ACLR have greater potential for future improvement in physical and self-reported function, compared with those who have already restored good function. Only seven (9%) had a KOOS-QoL >90 at 1 year, demonstrating majority of the cohort had not reached a ceiling point, and may continue to improve between 1 and 5 years.
Supplemental material
The only other study to evaluate the relationship between function at the time of RTS and PROs beyond 2 years reported conflicting findings.51 Greater between limb asymmetry on the one-leg rise test 6–15 months post-ACL injury was associated with worse KOOS scores at 5 years.51 Due to the multifactorial fluctuating nature of life for a young active adult, it is likely many other subjective factors influence change in KOOS and IKDC scores, hence predicting PROs post-ACLR is challenging.16 52 Further research should consider potential psychosocial and contextual influences on PROs such as fear avoidance, confidence, coping and healthcare utilisation.53–57
Limitations
This prospective study lost 31 (28%) participants between 1 and 5 years. However, there were no significant differences in preinjury activity level, age, sex, body mass index or combined injury presence at the time of ACLR, between those who did and did not participate in follow-up.7 The current study included six (8%) participants who did not participate in jumping or cutting sports preinjury (ie, level 3 or 4),29 which may influence the raw hop-test scores at 1 year. The current study may have been underpowered to detect potential relationships with functional performance for some outcome variables (ie, tibiofemoral worsening), affecting the statistical stability of some regression models. Future approaches should combine large sets of individual level data from multiple sites to provide sufficient power to detect risk factors and develop a risk profile for early OA development and progression in this young active population. Mechanical (eg, movement patterns,58 physical activity,59–61 time from injury to ACLR7) and systemic factors (eg, adiposity)62 may influence the development of post-traumatic OA61 and warrant consideration in future risk profiles.
The LSI has inherent limitations and may overestimate knee function due to the bilateral neuromuscular deficits observed post-ACLR.63 Also, discrete cut-offs (ie, >90% LSI) as an independent risk factor may result in overestimation of risk estimates.64 Therefore, we considered both magnitude of performance as a continuous outcome (repetitions or distance), as well as symmetry (LSI%), with generally a closer association observed between worsening OA features and dichotomised outcomes (<90% LSI). A floor effect for the functional performance tests should be noted as some participants scored zero on their ACLR limb (table 2), with reasons (anecdotally reported) as lack of physical capability (strength/power/control) or confidence to attempt the task. Future studies should explore reasons for poor functional performance, to better direct intervention strategies.
Clinical considerations
Despite the limitations of the LSI, better limb symmetry in hop tests has been associated with greater likelihood of return-to-sport, and reduced reinjury risk.38 65 Our results show restoring limb symmetry is also an attractive intervention target, given only 18% ‘passed’ the test battery (>90% LSI all four tests), and poor function was associated with increased risk of worsening patellofemoral bone marrow and cartilage lesions. Our sensitivity analysis (see online supplementary file 1) demonstrated the highest RRs for worsening patellofemoral cartilage, patellofemoral BMLs, tibiofemoral meniscal lesions were observed when any three tests, or at least two or three tests were failed (<90% LSI). A battery of tests assessing multiple functional domains (ie, strength, endurance, balance) may better categorise individuals with poor functional performance, and be more predictive of clinical outcomes.38 Multifaceted neuromuscular deficits may affect joint loading,12 and consequently joint health. Regardless of return-to-sport aspirations, continuing rehabilitation to achieve ‘functional criteria’ on a test battery may optimise future joint health. Future studies should continue to investigate the relationship between symptomatic and structural changes in a post-traumatic OA population after ACLR. Underlying early stages of OA without the presence of symptoms may not be ‘incidental’ in those at risk of OA, and may lead to future symptomatic radiographic OA.8
Conclusion
Only one in five participants met common functional performance criteria (≥90% LSI all four tests) 1 year post-ACLR. Poor function was consistently associated with 2–4 times increased risk of worsening patellofemoral (but not tibiofemoral) BMLs. These results highlight the importance of optimising function beyond the short-term re-injury risk, as functional performance may help identify individuals on an accelerated trajectory towards (patellofemoral) radiographic OA.
Patient and public involvement
There were no funds or time allocated for patient and public involvement so we were unable to involve patients. We have invited patients to our knowledge translation events, to help inform our dissemination strategy and future research questions.
What are the findings?
Individuals with poor functional performance 1 year following ACL reconstruction (ACLR) had 2–4 times increased risk of worsening patellofemoral bone marrow lesions (BMLs) in the following 4 years.
Less than one in five passed the functional performance battery (≥90% limb symmetry index on all four tests) 1 year after ACLR, highlighting a need to implement treatments capable of improving functional recovery.
Poor functional capacity on hop testing and a one-leg rise at 1 year post-ACLR may help identify individuals at an increased risk of worsening patellofemoral BMLs, and developing early onset post-traumatic patellofemoral osteoarthritis.
How might it impact on clinical practice in the future?
Clinicians should evaluate patient-specific barriers and enablers to implement evidence-based rehabilitation, given only 18% passed the functional test battery at 1 year post-ACLR.
Regardless of an individual’s desire to return-to-sport, restoring lower-limb function may be important to mitigate the risk of future joint degeneration.
Acknowledgments
The authors would like to thank all the participants, Imaging@Olympic Park for assistance in obtaining all MRIs and Olympic Park Sports Medicine Centre for use of their facility for clinical data collection.
References
Footnotes
Twitter @Knee_Howells, @DrChrisBarton
Contributors BP, AG and KAC conceived and designed the study. HGM and TSW assisted with recruitment of participants. BP, JS and AGC conducted the statistical analysis and interpretation of data, with input from CB and KMC. BP drafted the manuscript with input from AG, CJB, KAC, JS, HGM, TSW and KAC. All authors have read and approved the final manuscript.
Funding Support for this study was provided by Arthritis Australia, La Trobe University Sport, Exercise and Rehabilitation Research Focus Area, the Queensland Orthopaedic Physiotherapy Network, the University of Melbourne (Research Collaboration grant) and the University of British Columbia Centre for Hip Health and Mobility (Society for Mobility and Health). BP was the recipient of the Felice Rosemary-Lloyd Travel Scholarship, which assisted with travel and data analysis to visit coauthor JS at the University of Delaware. BP, AC and CB are recipients of National Health and Medical Research Council awards (post-graduate scholarship No. 1114296, Neil Hamilton Fairley Clinical Fellowship No. 1121173 and MRFF Translating Research into Practice No. 11163250, respectively). JS is supported by a NIH/NIGMS grant U54-GM104941.
Competing interests AG received consulting fees for grading of MRI images at baseline and follow-up. He is a shareholder of Boston Imaging Core Lab (BICL) and a consultant to Merck Serono, Pfizer, GE Healthcare, Galapagos, Roche and TissueGene.
Patient consent for publication Not required.
Ethics approval Ethical approval was granted by the La Trobe University Human Ethics Committee (HEC15-100) and all participants signed informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request. Reuse will be permitted by the corresponding author, and can occur up until 2027, which corresponds with the conditions of the La Trobe University Human Ethics committee that indicates data will be kept for at least 10 years following completion of data collection.