Article Text

Abstract
The present study summarises the work developed by the ALPHA (Assessing Levels of Physical Activity) study and describes the procedures followed to select the tests included in the ALPHA health-related fitness test battery for children and adolescents. The authors reviewed physical fitness and health in youth findings from cross-sectional studies. The authors also performed three systematic reviews dealing with (1) the predictive validity of health-related fitness, (2) the criterion validity of field-based fitness tests and (3) the reliability of field-based fitness tests in youth. The authors also carried out 11-methodological studies to determine the criterion validity and the reliability of several field-based fitness tests for youth. Finally, the authors performed a study in the school setting to examine the reliability, feasibility and safety of the selected tests. The selected fitness tests were (1) the 20 m shuttle run test to assess cardiorespiratory fitness; (2) the handgrip strength and (3) standing broad jump to assess musculoskeletal fitness, and (4) body mass index, (5) skinfold thickness and (5) waist circumference to assess body composition. When there are time limits, the authors propose the high-priority ALPHA health-related fitness test battery, which comprises all the evidence-based fitness tests except the measurement of the skinfold thickness. The time required to administer this battery to a group of 20 youth by one physical education teacher is less than 2 h. In conclusion, the ALPHA fitness tests battery is valid, reliable, feasible and safe for the assessment of health-related physical fitness in children and adolescents to be used for health monitoring purposes at population level.
Statistics from Altmetric.com
Background
Health-related physical fitness refers to those components of fitness that have a relationship with health such as (1) cardiorespiratory fitness, (2) musculoskeletal fitness, (3) motor fitness and (4) body composition.1 Health-related physical fitness can be objectively measured in the laboratory, yet, their use is limited in the school setting due to the necessity of sophisticated instruments, qualified technicians and time constraints. Field-based tests provide a reasonable alternative since they are time-efficient, low in cost and equipment requirements, and can be easily administered to a large number of people simultaneously.
There are at least 15 different fitness test batteries (table 1) and a few key fitness dimensions. For cardiorespiratory fitness, more than 10 field tests are available.2 There is a need for comparable methods that can be used internationally.
Existing field-based physical fitness test batteries for children and adolescents
The ALPHA (Assessing Levels of Physical Activity) study was initiated with the aim of providing a set of instruments for ALPHA and its underlying factors (eg, built environment, transport and worksites) as well as health-related physical fitness in a comparable way within the European Union. The aim of the Work Package 6 (‘Assessing Health-Related Physical Fitness’) was to provide a set of valid, reliable, feasible a safe field-based fitness tests for the assessment of health-related physical fitness in children and adolescents to be used in public health monitoring in a comparable way within the European Union.
We hereby summarise the work developed by the ALPHA Fitness-Group and describe the procedures followed to select the tests to be included in the ALPHA health-related fitness test battery for children and adolescents.
Overall procedure
Here we review three major elements of our work (figure 1). First, we reviewed the evidence on (1) the association between physical fitness and health in young people mainly focused on findings from cross-sectional studies,3 (2) the predictive validity of health-related fitness,4 (3) the criterion validity of field-based fitness tests2 and (4) the reliability of field-based fitness tests in young people.5 Second, we also carried out 11 methodological studies to determine the criterion validity and the reliability of several field-based fitness tests for young people. Third, we performed a study in the school setting to examine the reliability, feasibility and safety of the evidence-based selected tests.

Flow chart of the development of the ALPHA health-related fitness test battery for children and adolescents. BC, body composition; CRF, cardiorespiratory fitness; F, fitness; HG, handgrip; MF, musculoskeletal fitness; SRT, shuttle run test.
Reviewing the evidence
Physical fitness and health
In the first review,3 we concluded from cross-sectional data that high cardiorespiratory fitness and muscular strength are associated with lower cardiovascular disease risk factors in healthy young people, a better quality of life and positive health in both healthy and diseased young people.
Predictive validity of health-related fitness
We reviewed whether low/high physical fitness in children and adolescents (exposure) predicts future disease/better health status (outcome).4
Of 42 studies (38 of high quality based on quality criteria4), we found strong evidence indicating that (1) higher levels of cardiorespiratory fitness in childhood and adolescence are associated with a healthier cardiovascular profile later in life; (2) muscular strength improvements from childhood to adolescence are negatively associated with changes in overall adiposity, and that (3) a healthier body composition at childhood and adolescence is associated with a healthier cardiovascular profile later in life and with a lower risk of death.
Criterion validity of field-based fitness tests
We systematically reviewed the validity of the existing field-based fitness tests used in children and adolescents. We found a total of 12 field tests to assess cardiorespiratory fitness, 24 tests to assess musculoskeletal fitness, 7 tests to assess motor fitness and 7 different field-based measures to assess body composition.2 From a total of 50 high-quality studies (based on quality criteria, see ref 2), we found that the 20 m shuttle run test (20mSRT) is a valid test to estimate cardiorespiratory fitness, the handgrip strength test and the standing broad jump are valid tests to assess musculoskeletal fitness, the skinfold thickness and body mass index (BMI) are good estimates of body composition, and waist circumference is a valid measure to estimate central body fat.
Reliability of field-based fitness tests
Based on a systematic review we identified 32 studies (19 of high quality based on quality-criteria, see ref 5) examining the reliability of field-based fitness tests in children and adolescents.5 We observed that the 20mSRT test is reliable to assess cardiorespiratory fitness; the handgrip strength and the standing broad jump tests are reliable to assess musculoskeletal fitness; the 4×10mSRT is reliable to assess motor fitness; and BMI, skinfolds and waist circumference are reliable to assess body fat.
In summary, we conclude that cardiorespiratory fitness, muscular strength and body composition could be considered as markers of health already at childhood and adolescence, as well as health indicators of future cardiovascular health. The 20mSRT can be considered both valid and reliable to assess cardiorespiratory fitness; the handgrip strength and the standing broad jump tests are valid and reliable to assess musculoskeletal fitness; and BMI, skinfold thickness and waist circumference are valid and reliable measures to estimate body fat. These tests were also among those used in the longitudinal studies4 suggesting that are feasible to be used in the school setting and at population level. We did not find evidence for other tests assessing motor fitness or flexibility due to the lack of studies.
Methodological studies
Criterion validity
Cardiorespiratory fitness
We assessed the criterion validity of the 20mSRT,6 7 the 1 mile run/walk test8 and the 1/2 mile run/walk test9 (table 2). With the aim of improving the estimation of maximal oxygen uptake (VO2max) from the 20mSRT, we developed and validated an artificial neural network (ANN) equation from the 20mSRT performance (last half-stage completed), sex, age, weight and height in adolescents. The error measures were significantly better than those obtained when using the equation reported by Léger et al10 (eg, percentage error 17.1 vs 7.4 for Léger and ANN equation, respectively, p<0.001). We additionally assessed the validity of five different equations (Léger,10 Barnett (a)11 and Barnett (b),11 Matsuzaka,12 and the ANN equation6) for estimating VO2max from the 20mSRT in an independent sample.7 The findings indicated that the equations should only be used at a population level and suggested that the equation reported by Barnett (b)11 and ANN-equation6 seems to be the most accurate to estimate VO2max in adolescents.
Overview of fitness criterion validity studies carried out within the framework of the ALPHA study
We also assessed the criterion validity of Cureton's equation for estimating VO2peak from the 1 mile run/walk test in trained children and adolescents8 and observed that this equation systematically underestimates VO2peak in this population (mean difference 10 ml/kg/min, p<0.001). Moreover, we developed and validated a new equation for estimating VO2peak from the 1/2 mile run/walk time, sex and BMI in children and adolescents,9 which had a lower percentage error than the Fernhall's equation (16.0% vs 50.4%, respectively, p<0.001).
The run/walk tests are not friendly, especially in young people, and the major problem is the participant's capacity to develop an appropriate pace. Participants may either start too fast, so that they are not able to keep the speed all through the test, or they may start too slow that when they want to increase the speed, the test is already finished.
Musculoskeletal fitness (muscular strength)
We conducted a series of studies in children13 and adolescents14 to determine whether there is an optimal grip span for determining the maximum handgrip strength, and if the optimal grip span was related to hand size (table 2). We found that there was an optimal grip span to which the dynamometer should be adjusted when measuring handgrip strength in children13 and adolescents.14 We provided a sex and age-specific equations to adjust the grip span of the dynamometer to the hand size of the individual in order to obtain the actual maximal handgrip strength. We also studied the criterion validity of three different dynamometers (Jamar, DynEx and TKK) in adolescents,15 and found a negative systematic bias – underestimation – for the Jamar and DynEx dynamometer (−1.92 and −1.43 kg, respectively, p<0.05), whereas a marginal positive overestimation was observed for the TKK dynamometer (0.49 kg, p<0.05). We also examined whether the elbow position (extended or flexed at 90°) affects the handgrip strength in adolescents.15 We observed that performing the handgrip strength test with the elbow extended seems the most appropriate protocol to evaluate maximal handgrip strength in adolescents when using the TKK dynamometer.15
We further examined the criterion validity of field-based muscular fitness tests in children and adolescents.16 17 Castro-Piñero et al17 investigated whether the standing broad jump test can be considered a general index of both lower body and upper body muscular fitness in children and adolescents. The results indicated that the standing broad jump test showed the strongest association with the other lower body (ie, vertical jump, squat jump and countermovement jump) muscular strength tests (R2=0.829–0.864), as well as with upper body (ie, throw basketball, push ups and isometric strength) muscular strength tests (R2=0.694–0.851), suggesting that it is a good indicator of overall muscular strength.
Musculoskeletal fitness (flexibility)
We also analysed the criterion validity of the sit-and-reach test and the modified sit-and-reach test for estimating hamstring flexibility in children and adolescents.18 Moreover, we examined the contribution of the main joints involved in the back-saver sit-and-reach test and its validity using angular kinematic analysis.19 We observed that the criterion validity of both the sit-and-reach test and the modified sit-and-reach test was rather weak (R2 ranging from 0.2–0.3),18 whereas the results indicated that the modified sit-and-reach test is a more valid method than the sit-and-reach test.
Reliability
Table 3 shows the fitness reliability studies performed within the ALPHA study. Within the framework of the HELENA Study (Healthy Lifestyle in Europe by Nutrition in Adolescence) we examined the reliability of a set of physical fitness tests: back-saver sit and reach, handgrip strength, standing broad jump, Bosco jumps (squat jump, counter movement jump and Abalakov jump), bent arm hang, 4×10 m shuttle run and the 20mSRT.20 We did not observe a systematic error for any of the physical fitness tests when repeated. Moreover, the results also suggest that the reliability did not differ between male and female adolescents.
Overview of fitness reliability studies carried out within the framework of the ALPHA study
We also carried out a reliability study in the school setting.21 Six physical education (PE) teachers from different schools assessed twice the physical fitness tests that we found to be health related, valid and reliable in the reviews and methodological studies carried out before: the 20mSRT, the handgrip strength and standing broad jump tests, as well as weight, height, triceps and subscapular thickness, and waist circumference.
We observed a good reliability in most of the studied tests, except in height (inter trial difference: 0.73 ± 0.8 cm, p<0.05) and standing broad jump (3.8 ± 12.7 cm, p<0.05) in children, and waist circumference in children (−0.82 ± 1.2 cm, p<0.05) and adolescents (−0.35 ± 0.8 cm, p<0.05). The low skill level of the teachers might explain the lower reliability observed in the anthropometric measures, and we cannot discard the possibility of a learning effect (positive systematic bias) in the standing broad jump test in children.
Feasibility
We also recorded information on how feasible and safe the assessment procedure in the school setting was taking into account all the specific circumstances that take place in the school arena.
Feasibility items recorded were (1) whether the children and adolescents worn appropriate (sport) clothes to perform the tests; (2) whether the tests' instructions were properly understood by the participants; (3) if any participant rejected to perform the measurements, and the reason/s; (4) we also asked the PE teachers about (i) the school's facilities to perform the tests, (ii) if they considered the tests easy or difficult to administer and (iii) their previous experience in administering these tests; (5) furthermore, we registered the time required by the PE teacher to prepare and administer the tests.
The feasibility items assessed presented a ‘positive’ score in 95% of the cases. The average time required to administer the whole fitness test battery to a group of 20 individuals by one single PE teacher was 2 h and 30 min, which equals to approximately three PE sessions of ∼55 min. The time required was shorter if skinfold thickness measurement would not have been included in the battery: less than 2 h to assess 20 persons (ie, two PE sessions of ∼55 min).21
Safety
Knowledge of the current and former health status of the children and adolescents is important in order to enhance safe testing. A pretesting screening should identify young people at high risk, and should be similar to the one typically used to allow the children and adolescents to take active part in the PE lessons. For this purpose, in most/many European countries, children have annual physical examinations by the school doctors who provide detailed information regarding the skeletomuscular, cardiorespiratory, haematocirculatory, psychoneurological and endocrine–metabolic systems. When this service is not available, it is recommendable that the parents or guardians complete at least a pretesting/preparticipation screening questionnaire before the child starts with the PE lessons and/or the fitness testing. A good example of such questionnaire is the Exercise and Physical Activity Readiness Assessment questionnaire.21 In any case, it is important to be alert to the subjective symptoms such as skin pallor, dizziness, syncope and dyspnoea. The tests should be immediately interrupted if there is any sign of problem or risk (see the standard operating procedure for specification).
During the above mentioned reliability study performed in the school setting,21 we recorded the following safety items: (1) instrument allergy, in the case of anthropometric and handgrip assessments; (2) sick feeling, in all the tests; (3) pain in hand or forearm in handgrip test; (4) musculoskeletal injuries during or after the physical fitness assessment; and (5) delayed-onset muscle soreness. We observed that all the safety items assessed presented a ‘positive’ score in 99% of the cases. No complications occurred during the testing procedure, and only one participant interrupted the 20mSRT because of lower body muscle cramp.
Our group has extensive experience in assessing physical fitness in young people. We have been involved in a number of population based studies22 namely the AVENA study,23 24 the EYHS study,25 the HELENA study26 27 and the IDEFICS study,28 where more than 10 000 children and adolescents have been measured. So far, we did not experience any safety issue.
Summary: selected tests to be included in the ALPHA health-related fitness test battery
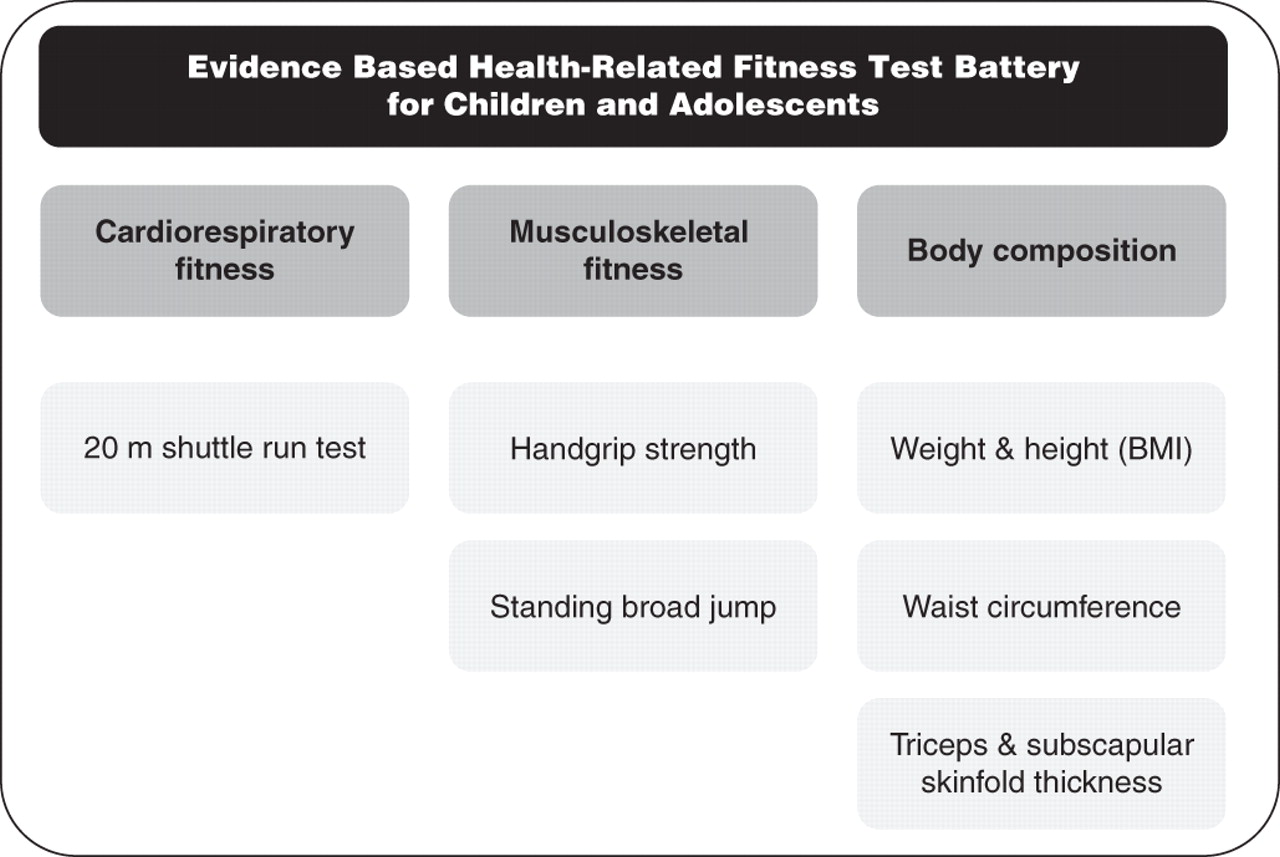
The evidence-based health-related ALPHA fitness test battery includes the following tests (figure 2): (1) the 20mSRT to assess cardiorespiratory fitness; (2) the handgrip strength; (3) the standing broad jump tests to assess musculoskeletal fitness; (4) BMI; (5) waist circumference; and (6) skinfold thickness (triceps and subscapular) to assess body composition. Based on the feasibility study we performed in the school setting, the time needed to administer these fitness test battery to a group of 20 individuals by one PE teacher is around 2 h and 30 min, that is, three PE sessions of ∼55 min.
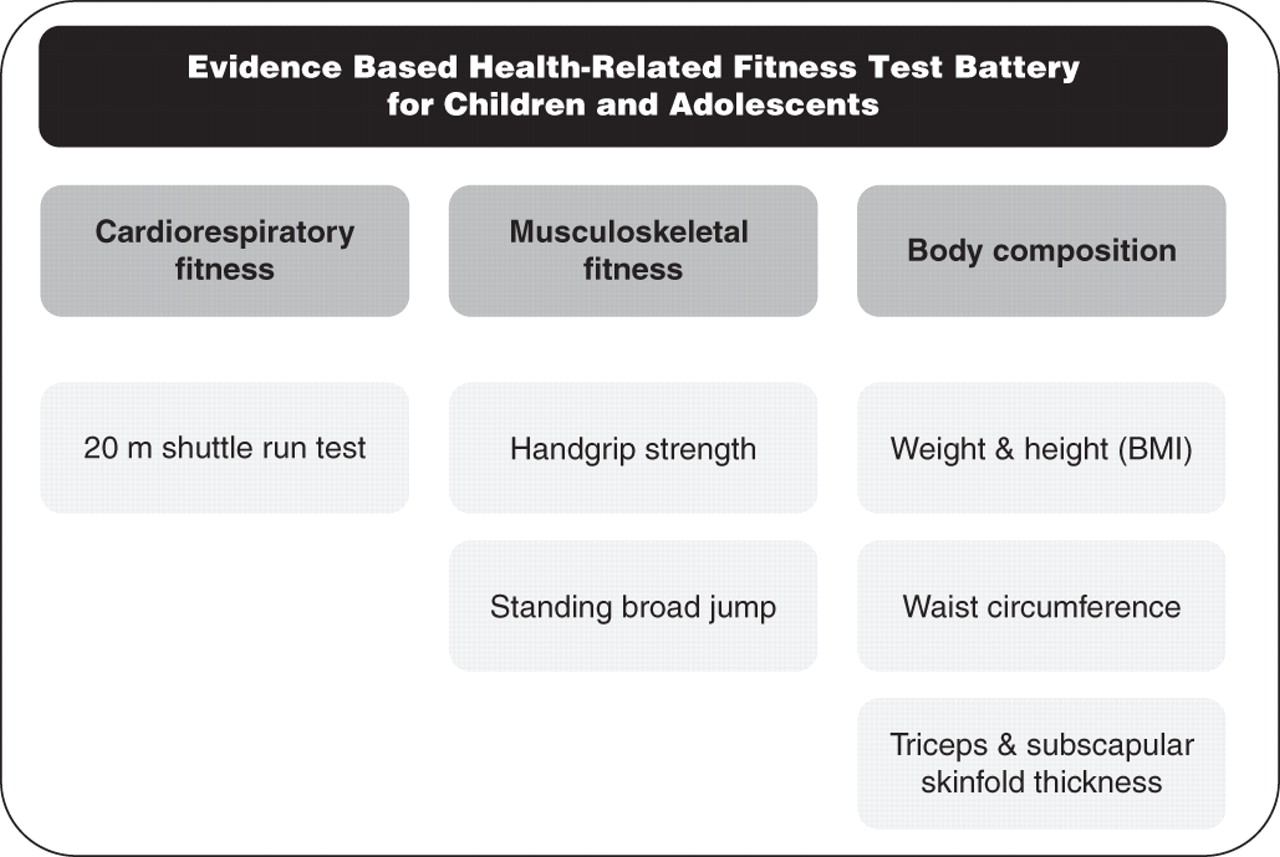
Evidence-based health-related fitness test battery for children and adolescents. BMI indicates body mass index (weight in kg divided by height in metres squared, kg/m2).
Practical implications
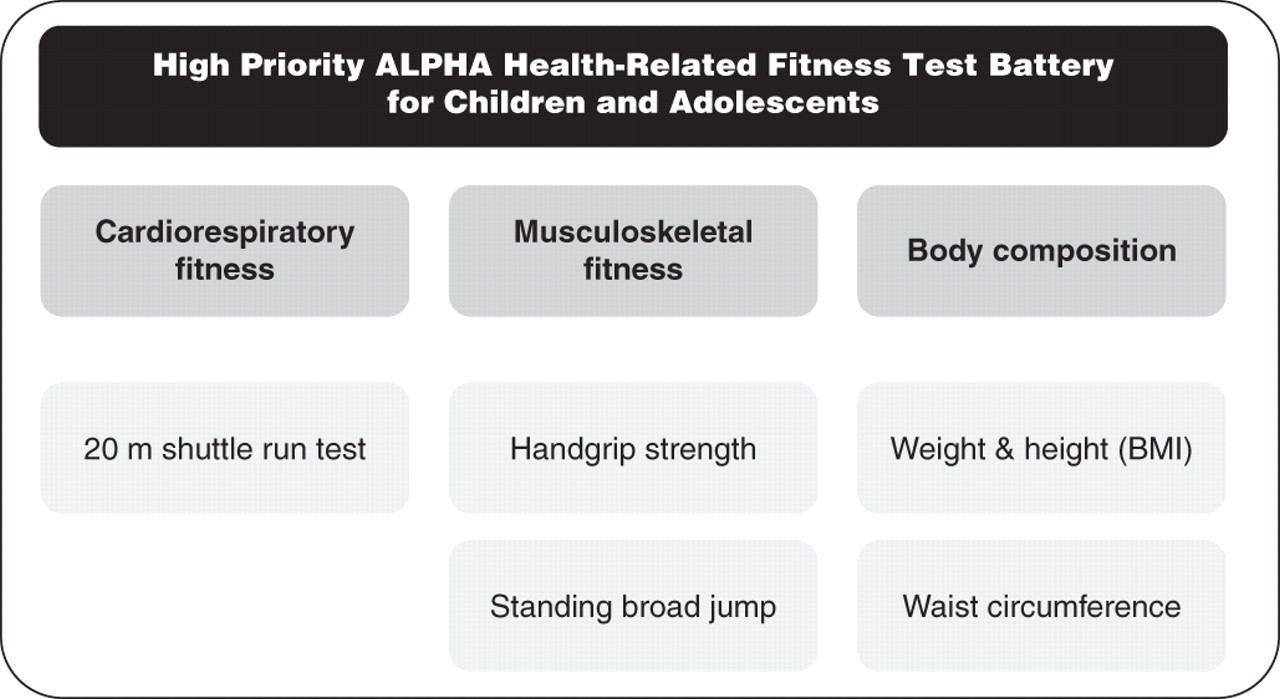
When there are time constraints, as it can be the case in the school setting, we recommend using the tests included in the high-priority ALPHA health-related fitness test battery (figure 3), which comprise all the evidence-based fitness tests except the measurement of the skinfold thickness. The time required to administer this battery to a group of 20 children by one PE teacher is less than 2 h (ie, two PE sessions of ∼55 min).
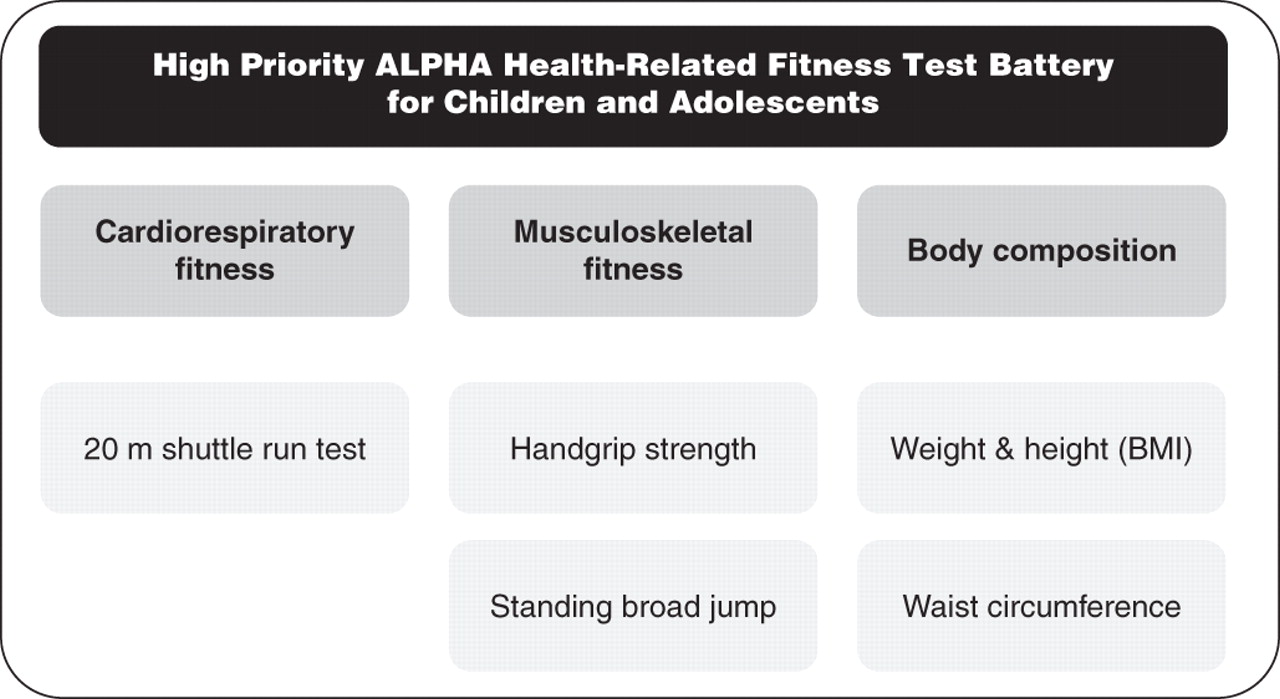
High-priority ALPHA health-related fitness test battery for Children and Adolescents. BMI indicates body mass index (weight in kg divided by height in metres squared, kg/m2).
When there are not time limits, as it can be the case in sports clubs or population-based studies, we recommend using the extended ALPHA health-related fitness tests battery for children and adolescents (figure 4), which includes an additional fitness test, the 4×10mSRT to assess motor fitness. This test is a marker of speed and agility and has been associated with bone mass in young people.3 However, there is no evidence of its predictive and criterion validity.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Extended ALPHA health-related fitness test battery for children and adolescents. BMI indicates body mass index (weight in kg divided by height in metres squared, kg/m2).
An evaluation of the pubertal development of children and adolescents is also of importance due to the fact that childhood and adolescence is a period of life where many changes occur. Though pubertal development should be ideally evaluated by a paediatrician or trained physician through direct observation, this is not feasible in most settings. Instead, trained interviewers can ask the children and adolescents to classify themselves in one of the five stages of pubertal maturity defined by Tanner and Whitehouse.29
There are normative values for each of the suggested tests which will enable a correct interpretation of the fitness status, to evaluate effects of alternative intervention strategies and to identify children and adolescents at risk for the major public health diseases (http://www.thealphaproject.eu/).
The emphasis of monitoring health-related fitness should be on avoiding disease risk as well as on enhancing physical functional capacity for everyday life. Fitness assessments should be considered as an instrument to encourage increase physical activity and exercise and not be an end in itself. We believe that schools play an important role in identifying children and adolescents with low fitness as well as in promoting positive fitness-enhancing behaviours. The leadership of schools as a powerful setting to promote a healthy lifestyle among young populations is supported by the American Heart Association.30
Acknowledgments
The authors would like to thank our group of international experts Prof Pekka Oja, Prof Han CG Kemper, Prof Jorge Mota, Prof Kari Bø, Prof Willem van Mechelen and Prof Robert M Malina for their valuable contribution to the conception and strategy of the development of the ALPHA fitness test battery.
References
Footnotes
-
Funding This work was supported by the European Union, in the framework of the Public Health Programme (ALPHA project, Ref: 2006120), the Swedish Council for Working Life and Social Research (FAS), the Spanish Ministry of Education (EX-2007-1124; AP-2004-2745; and AP2005-4358), and the Spanish Ministry of Education and Science-FEDER funds (Acciones Complementarias DEP2007-29933-E).
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.