Article Text

Abstract
Objective To perform a systematic review and meta-analysis to explore the relationship between prenatal exercise and glycaemic control.
Design Systematic review with random-effects meta-analysis and meta-regression.
Data sources Online databases were searched up to 6 January 2017.
Study eligibility criteria Studies of all designs were included (except case studies and reviews) if they were published in English, Spanish or French, and contained information on the population (pregnant women without contraindication to exercise), intervention (subjective or objective measures of frequency, intensity, duration, volume or type of acute or chronic exercise, alone (‘exercise-only’) or in combination with other intervention components (eg, dietary; ‘exercise+cointervention’) at any stage of pregnancy), comparator (no exercise or different frequency, intensity, duration, volume and type of exercise) and outcome (glycaemic control).
Results A total of 58 studies (n=8699) were included. There was ‘very low’ quality evidence showing that an acute bout of exercise was associated with a decrease in maternal blood glucose from before to during exercise (6 studies, n=123; mean difference (MD) −0.94 mmol/L, 95% CI −1.18 to −0.70, I2=41%) and following exercise (n=333; MD −0.57 mmol/L, 95% CI −0.72 to −0.41, I2=72%). Subgroup analysis showed that there were larger decreases in blood glucose following acute exercise in women with diabetes (n=26; MD −1.42, 95% CI −1.69 to −1.16, I2=8%) compared with those without diabetes (n=285; MD −0.46, 95% CI −0.60 to −0.32, I2=62%). Finally, chronic exercise-only interventions reduced fasting blood glucose compared with no exercise postintervention in women with diabetes (2 studies, n=70; MD −2.76, 95% CI −3.18 to −2.34, I2=52%; ‘low’ quality of evidence), but not in those without diabetes (9 studies, n=2174; MD −0.05, 95% CI −0.16 to 0.05, I2=79%).
Conclusion Acute and chronic prenatal exercise reduced maternal circulating blood glucose concentrations, with a larger effect in women with diabetes.
- exercise
- pregnancy
- glucose
Statistics from Altmetric.com
Introduction
During a healthy pregnancy, a cascade of hormonal events result in physiological insulin resistance at the level of the skeletal muscle to ensure an adequate supply of nutrients to the growing fetus.1 However, in 6%–9% of pregnancies, maternal circulating blood glucose rises to pathological values, and gestational diabetes mellitus (GDM) is diagnosed.2 A diagnosis of GDM is associated with an increased risk of complications such as pre-eclampsia, macrosomia, caesarean delivery, neonatal hypoglycaemia and neonatal intensive care unit admission.3 Therefore, strategies to prevent the development and improve the management of this disease are critical3; exercise may be one such strategy. Habitual prenatal exercise has been suggested to reduce the odds of developing GDM by ~40%.4 Additionally, prenatal exercise after diagnosis of GDM is also recognised as a beneficial adjunct therapy to nutritional or medical management due to its glucose-lowering effects.5 6
It is established that in non-pregnant adults an acute bout of exercise stimulates the translocation of glucose transporters (predominantly the GLUT 4 isoform) onto the surface of skeletal muscle cells, thereby improving glucose uptake.7 Indeed, exercise can lower circulating blood glucose values and improve insulin sensitivity for up to 72 hours postexercise in individuals with type 2 diabetes mellitus.8 However, the unique metabolic adaptations to pregnancy may alter the effects of exercise on maternal glucose control. It has been suggested that pregnant women are hypoglycaemic (<3.3 mmol/L) more frequently than their non-pregnant counterparts9 and that the blood glucose-lowering effects of exercise may increase the risk of hypoglycaemic events.10 At present, the impact of acute and chronic exercise on maternal glucose control and hypoglycaemic events has not been systematically reviewed.
The present systematic review and meta-analysis was conducted as part of a series of reviews, which will form the evidence base for the development of the 2019 Canadian guideline for physical activity throughout pregnancy (herein referred to as the Guideline).11 The current Canadian guideline was developed in 2003 and did not consider glycaemic control.12 Therefore, the objective of the current systematic review and meta-analysis was to explore the relationship between prenatal exercise and glycaemic control.
Methods
In October 2015, the Guidelines Consensus Panel assembled to identify priority outcomes for the Guideline update. The Panel included researchers, methodological experts, a fitness professional, and representatives from the Canadian Society for Exercise Physiology (CSEP), the Society of Obstetricians and Gynaecologists of Canada (SOGC), the College of Family Physicians of Canada, the Canadian Association of Midwives, the Canadian Academy of Sport and Exercise Medicine, Exercise is Medicine Canada, and a representative health unit (the Middlesex-London Health Unit). Twenty ‘critical’ and 17 ‘important’ outcomes related to prenatal exercise and maternal/fetal health were selected by the Panel. One of the ‘critical’ outcomes (ie, glucose control) and one of the ‘important’ outcomes (ie, hypoglycaemia) were examined in this review. This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, and the checklist was completed.13
Protocol and registration
Two individual systematic reviews examining the impact of prenatal exercise on maternal health outcomes and fetal health outcomes were registered a priori with PROSPERO, the international prospective register of systematic reviews (maternal health: trial registration number CRD42016032376; fetal health: trial registration number CRD42016029869). Since the scope of the current systematic review encompasses both fetal and maternal health, records identified through both search strategies were reviewed for inclusion in the current study.
Eligibility criteria
The participants, interventions, comparisons, outcomes and study design (PICOS) framework was used to guide this study,14 as listed below.
Population
The population of interest was pregnant women without contraindication to exercise according to the SOGC/CSEP and the American Congress of Obstetricians and Gynecologists (ACOG) guidelines.12 15 Based on the SOGC and ACOG guidelines, absolute contraindications to exercise were defined as ruptured membranes, premature labour, persistent second or third trimester bleeding, placenta previa, pregnancy-induced hypertension or pre-eclampsia, gestational hypertension, incompetent cervix, intrauterine growth restriction, high-order pregnancy, uncontrolled type 1 diabetes, hypertension or thyroid disease, or other serious cardiovascular, respiratory or systemic disorders. Relative contraindications to exercise were defined as a history of spontaneous abortion or premature labour in previous pregnancies, mild/moderate cardiovascular or respiratory disease, anaemia or iron deficiency, malnutrition or eating disorder, twin pregnancy after the 28th week, or any other significant medical condition. Studies that included women with absolute or relative contraindications, as reported by individual study authors, were excluded.
Intervention (exposure)
The intervention/exposure of interest was objective or subjective measures of frequency, intensity, duration, volume or type of exercise. Interventions including exercise alone (termed ‘exercise-only’ interventions) or in combination with other interventions (such as diet; termed ‘exercise+co-interventions’) were considered. Exercise-only interventions could include standard care. Acute (ie, a single exercise session) or chronic (ie, usual activity) exercise, as well as ‘exercise-only’ or ‘exercise plus cointervention’ (ie, diet or lifestyle counselling), interventions were included in the current systematic review. For this review, we used the terms exercise and physical activity interchangeably, defined as any bodily movement generated by the skeletal muscles resulting in energy expenditure above the resting levels.16 Studies were excluded if exercise was performed after the beginning of labour.
Comparison
Eligible comparators were no exercise, or different frequency, intensity, duration, volume or type of exercise, different intervention duration, or exercise in a different trimester.
Outcome
Relevant outcomes were indicators of glucose tolerance: insulin use, glycaemic response to an acute bout of exercise or to chronic exercise, as well as hypoglycaemia. Glycaemic response to acute exercise (a single bout) was defined as the mean difference (MD) in blood glucose values from before to during or after (within 15 min) a single bout of exercise. Glycaemic response to chronic exercise was determined by fasting blood glucose values and insulin use (number of women requiring insulin and number of units) at the end of the exercise intervention comparing women who exercised with those who did not. The prevalence of hypoglycaemic events in response to prenatal exercise was determined as defined by the study authors.
Study design
Original studies of any design (randomised controlled trial (RCT) and observational) were eligible for inclusion except for case studies or reviews. Acute data were from studies of any design that examined response from before to during or before to following a single bout of exercise (whether in the context of an RCT or a non-randomised intervention, or an observational study where the glucose response to a single bout of exercise was assessed). In contrast, for chronic data, data were combined within study designs only (ie, RCTs pooled with RCTs, non-randomised interventions with non-randomised interventions, and so on).
Information sources
A comprehensive search was created and run by a research librarian (LGS) in the following databases: MEDLINE, EMBASE, PsycINFO, Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, Scopus and Web of Science Core Collection, CINAHL Plus with Full Text, Child Development & Adolescent Studies, Education Resources Information Center, SPORTDiscus, ClinicalTrials.gov and the Trip Database up to 6 January 2017 (see the online supplementary materials for complete search strategies). The searches combined keyword terms and controlled vocabulary terms (when available) for each of the following concepts: (1) exercise/physical activity; (2) pregnancy; and (3) outcomes of exercise during pregnancy, including insulin, glucose, hypoglycaemia or glycaemic control (see the online supplementary materials for complete search strategies).
Supplementary file 1
Study selection and data extraction
The titles and abstracts of all retrieved articles were independently screened by two reviewers. Full-text articles were retrieved when at least one reviewer deemed the abstract to have met the initial inclusion criteria. Before extraction, full-text articles were independently screened by two reviewers for study inclusion criteria. When one reviewer recommended a paper be excluded, it was sent to MHD and/or S-MR for further review before a final decision on exclusion was made. In the event of a disagreement after further discussion, the study characteristics were presented to the Guidelines Steering Committee who oversaw the systematic reviews (MHD, MFM, S-MR, CEG, VJP, AJG and NB) in order to come to a final decision regarding inclusion/exclusion by consensus. Included papers from both the maternal health and fetal health search were imported into DistillerSR (Evidence Partners, Ottawa, Ontario, Canada) for data extraction. Studies were combined in the DistillerSR from the maternal and fetal search and were considered as one review from here on.
Methodological experts and the Guidelines Steering Committee were consulted to create data extraction tables in DistillerSR. Data from all papers that met the inclusion criteria were extracted by one person, and then independently verified by a content expert (MHD, MFM or S-MR). When outcomes from a single study were reported in multiple papers, the most recent or complete publication was selected as the ‘parent’ paper. Relevant data from all related publications were then extracted in conjunction with the parent paper. Extracted data were study characteristics (ie, year, study design, country) and characteristics of the population (eg, number of participants, age, prepregnancy body mass index (BMI), gestational age, parity, and pregnancy complications including pre-eclampsia, gestational hypertension and gestational diabetes), intervention/exposure (prescribed and/or actual exercise frequency, intensity, time and type of exercise, duration of the exercise training, measure of physical activity, trimester) and outcomes (maternal hypoglycaemia, glycaemic control (eg, fasted blood glucose), glycaemic response to exercise and insulin use). When data were unavailable for extraction, the corresponding authors were contacted to request for additional information. Data that were only available in figures were extracted by two individuals independently using GetData Graph Digitizer (V.2.26). If the data obtained from the two individuals differed by more than 5%, it was sent to a third individual and reviewed by MHD to ensure accuracy.
Quality of evidence assessment
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework was used to assess the quality of evidence across studies for each study design and health outcome.
Evidence from RCTs began with a ‘high’ quality of evidence rating and was graded down if there were concerns regarding risk of bias, indirectness, inconsistency or imprecision because these factors reduce the level of confidence in the observed effects.17 Evidence from all non-randomised intervention and observational studies began with a ‘low’ quality rating and, if there was no cause to downgrade, was upgraded if applicable according to the GRADE criteria (eg, large magnitude of effect, evidence of dose–response).18
The risk of bias in RCTs and non-randomised intervention studies was assessed following the Cochrane Handbook,19 and the risk of bias in observational studies was assessed using the characteristics recommended by Guyatt et al,20 which have been used by other physical activity systematic reviews.21 All studies (RCTs, intervention studies and observational studies) were evaluated for potential sources of bias, including selection bias (RCT: inadequate randomisation procedure; observational: inappropriate sampling), reporting bias (selective/incomplete outcome reporting), performance bias (RCT: compliance to the intervention; observational: flawed measurement of exposure), detection bias (flawed measurement of outcome), attrition bias (incomplete follow-up, high loss to follow-up) and ‘other’ sources of bias. Risk of bias across studies was rated as ‘serious’ when studies having the greatest influence on the pooled result (assessed using weight (%) given in forest plots or sample size in studies that were narratively synthesised) presented ‘high’ risk of bias. The greatest influence on the pooled result was determined as follows: the studies that had the greatest individual % contribution in the meta-analyses, when taken together, contributed to >50% of the weight of the pooled estimate. Serious risk of bias was considered when the sample size of studies that were narratively synthesised was similar to the total sample size of studies contributing to >50% of the weight of the pooled estimate in the meta-analyses. Performance bias was rated as ‘high’ when <60% of participants performed 100% of prescribed exercise sessions or attended 100% of counselling sessions (defined as low compliance) or when compliance to the intervention was not reported. Attrition bias was rated as ‘high’ when >10% of data were missing at the end of the study and in cases where intention-to-treat analysis was not used. Given the nature of exercise interventions, it is not possible to blind participants to group allocation. Therefore, if the only source of bias was related to the blinding of allocation, the risk of bias was rated as ‘low’.
Indirectness was considered serious when exercise-only interventions and exercise+cointerventions were combined for analysis or when the effect of exercise+cointervention alone on an outcome was evaluated. Inconsistency was considered serious when heterogeneity was high (I2≥50%) or when only one study was assessed (I2 unavailable). Imprecision was considered serious when the 95% CI crossed the line of no effect, and was wide, such that interpretation of the data would be different if the true effect were at one end of the CI or the other. When only one study was examined, imprecision was not considered serious because inconsistency was already considered serious for this reason. Finally, in order to assess publication bias, funnel plots were created if at least 10 studies were included in the forest plot (see online supplementary figure 2). If there were fewer than 10 studies, publication bias was deemed non-estimable and not rated down. Due to time constraints and feasibility, one reviewer evaluated the quality of the evidence across each health outcome using the protocol and a second person reviewed the GRADE tables as a quality control measure. Quality of evidence assessment is presented in online supplementary tables 2–4.
Statistical analysis
Statistical analyses were conducted using Review Manager V.5.3 (Cochrane Collaboration, Copenhagen, Denmark). For all dichotomous outcomes, ORs were calculated. Inverse-variance weighting was applied to obtain OR using a random-effects model. For continuous outcomes, mean differences between exercise and control groups were examined and MDs were calculated. Significance was set as p<0.05.
For the acute exercise data, change scores were calculated using the generic inverse-variance method (Cochrane Collaboration).22 The proportion of hypoglycaemic events in response to acute exercise was obtained through random-effects pooling of logit-transformed proportions in R (V.3.4.1). Additional details can be found in the Evidence synthesis section of the online supplementary materials.
For studies examining the glucose response to chronic exercise, meta-analyses were performed separately by study design. A sensitivity analysis comparing exercise-only interventions with exercise+cointerventions was conducted for RCTs and non-randomised interventions. A staged approach was used to determine inclusion of study designs other than RCTs. For each outcome related to chronic exercise interventions, evidence from RCTs was initially examined. If fewer than 2000 women were included in the exercise-only RCT meta-analysis, the impact of prenatal exercise on the specific outcome was examined further using non-randomised interventions and observational evidence (cohort, cross-sectional and case–control studies). When possible, the following a priori determined subgroup analyses were conducted for exercise-only interventions and observational studies: (1) women diagnosed with diabetes (gestational, controlled type 1 or type 2) compared with women without diabetes; (2) samples of women with overweight or obesity (mean BMI>25.0 kg/m2) prior to pregnancy compared with samples of women who were of various BMI (mean BMI<25 kg/m2 but possibly with some individuals with BMI>25.0 kg/m2; (3) women >35 years of age compared with women <35 years of age; and (4) women who were previously inactive compared with those who were previously active. If a study did not provide sufficient detail to allow it to be grouped into the a priori subgroups, then a third group called ‘unspecified’ was created. For each outcome related to acute exercise glucose responses, evidence from all study types was combined. The following post-hoc subgroup analyses were conducted for acute exercise responses to identify the source of high heterogeneity: (1) glucose response to exercise of low intensity compared with moderate and vigorous intensity23; and (2) glucose response to exercise duration of ≤20 min compared with duration of 21–39 min and >40 min. Tests for subgroup differences were conducted, with statistical significance set at p<0.05. Effects within subgroups were only interpreted when statistically significant differences between subgroups were found. In general, the number of women presented in the results reflects the number of women in the study. However, when the results were presented for women in the exercise group only, the number of exercisers was indicated.
In studies where there were no observed events in the intervention or control group, data were included in forest plots, but were considered ‘not estimable’ and excluded from the pooled analysis as per the recommendation in the Cochrane Handbook.19 When repeated measures (eg, multiple time points) were reported for each participant, the sample size was divided by the number of time points to avoid exaggerating the sample size through double (or triple and so on) counting. Furthermore, if the number of participants varied at each time point, the weighted n was used to determine the SE. For outcomes where a meta-analysis was not possible, a narrative synthesis of the results was conducted, organised around each outcome (ie, qualitative synthesis). Within each outcome, the results are presented by study design and included in the GRADE tables (online supplementary materials).
Dose–response meta-regression was carried out by weighted no-intercept regression of log OR with a random-effects model for study, using the metafor package in R V.3.4.1.24 It was determined that an accepted cut-point for a clinically meaningful decrease in glycaemic change does not exist in the literature. As such, a reduction that was statistically significant was chosen based on expert opinion. Models did not include an intercept term since the log OR are assumed to be zero when the exercise dose is zero. Restricted cubic splines with knots at the 10th, 50th and 90th percentiles of the explanatory variable were used to investigate whether there was evidence for a non-linear relationship. Fitting was by maximum likelihood, and non-linearity was assessed using a likelihood ratio test. Linear models are presented unless the fit of the spline was significantly better (p<0.05).
Results
Study selection
The initial search was not limited by language. However, for feasibility reasons, the Guidelines Steering Committee decided to exclude studies published in languages other than English, Spanish or French. A PRISMA diagram of the search results, including reasons for exclusion, is shown in figure 1. A comprehensive list of excluded studies is presented in the online supplementary materials.

Flow diagram of selected studies. *One study included in both the narrative and quantitative syntheses.
Study characteristics
Overall, 58 studies (8699 women; 31 RCTs, 7 non-randomised interventions, 8 cohort studies and 12 cross-sectional) from 21 countries were included. Among the included exercise interventions, the frequency of exercise ranged from 1 to 7 days per week, the duration of exercise ranged from 15 to 60 min per session, and the types of exercise included were aerobic exercise, yoga, resistance training and pelvic floor muscle training. Details regarding the acute exercise bouts and additional details regarding the studies can be found in online supplementary table 1 and the Study characteristics section.
Quality of evidence
Overall, the quality of evidence ranged from ‘very low’ to ‘high’ (see online supplementary tables 2-4). The most common reasons for downgrading the quality of evidence were (1) serious risk of bias, (2) inconsistency and (3) indirectness of the interventions being assessed. Common sources of bias included poor or unreported compliance with the intervention and inappropriate treatment of missing data when attrition rate was high. No evidence of publication bias was observed among the analyses where it was possible to systematically assess this using funnel plots.
Synthesis of data
Glycaemic response during an acute bout of prenatal exercise
There was ‘low’ quality evidence from 6 studies (123 women) showing a decrease in blood glucose of 0.94 mmol/L from before to during exercise (95% CI −1.18 to −0.70, I2=41%; see online supplementary figure 1).25–30 Meta-regression analyses revealed a dose–response relationship, where greater volumes of exercise (intensity × duration of exercise expressed as metabolic equivalents (MET) minutes per session) resulted in greater reductions in glucose during exercise (see online supplementary figure 2; p<0.01). No information was available to conduct additional a priori subgroup analyses. The tests for post-hoc subgroup differences were not statistically significant (see online supplementary figures 1, 3 and 4).
Glycaemic response following an acute bout of prenatal exercise
There was ‘very low’ quality evidence from 23 studies (490 women) examining changes in blood glucose from before to after exercise.26 28–49 The quality of the evidence was downgraded from ‘low’ to ‘very low’ because of inconsistency between studies. The pooled estimate was based on 17 studies and demonstrated that prenatal exercise resulted in a 0.57 mmol/L reduction in blood glucose from before to following exercise (95% CI −0.72 to −0.41, I2=72%; see online supplementary figure 5).26 28–34 36–41 43 46 47 Six studies could not be included in the meta-analysis (see online supplementary table 1 for additional details). One study measured glycaemic responses to a 2.4 kilometers jog (vigorous-intensity exercise) in the third trimester of pregnancy and observed a 1.2 mmol/L decrease in blood glucose following exercise.42 Three studies measured glycaemic responses to acute moderate-intensity exercise, no change in blood glucose was observed in two studies,45 48 while a decline in blood glucose was observed in one study.35 Finally, two RCTs assessed acute glycaemic responses during an exercise intervention.44 49 Participants in the first study were women with GDM. Larger decreases in blood glucose in response to an acute exercise bout were reported at the end of the 6-week exercise and diet intervention as compared with the start of the intervention.44 In contrast, participants in the second study were women without GDM.49 By the end of the ~18-week intervention (third trimester), larger decreases in blood glucose in response to an acute exercise bout were reported for women in the control condition as compared with the exercise condition.
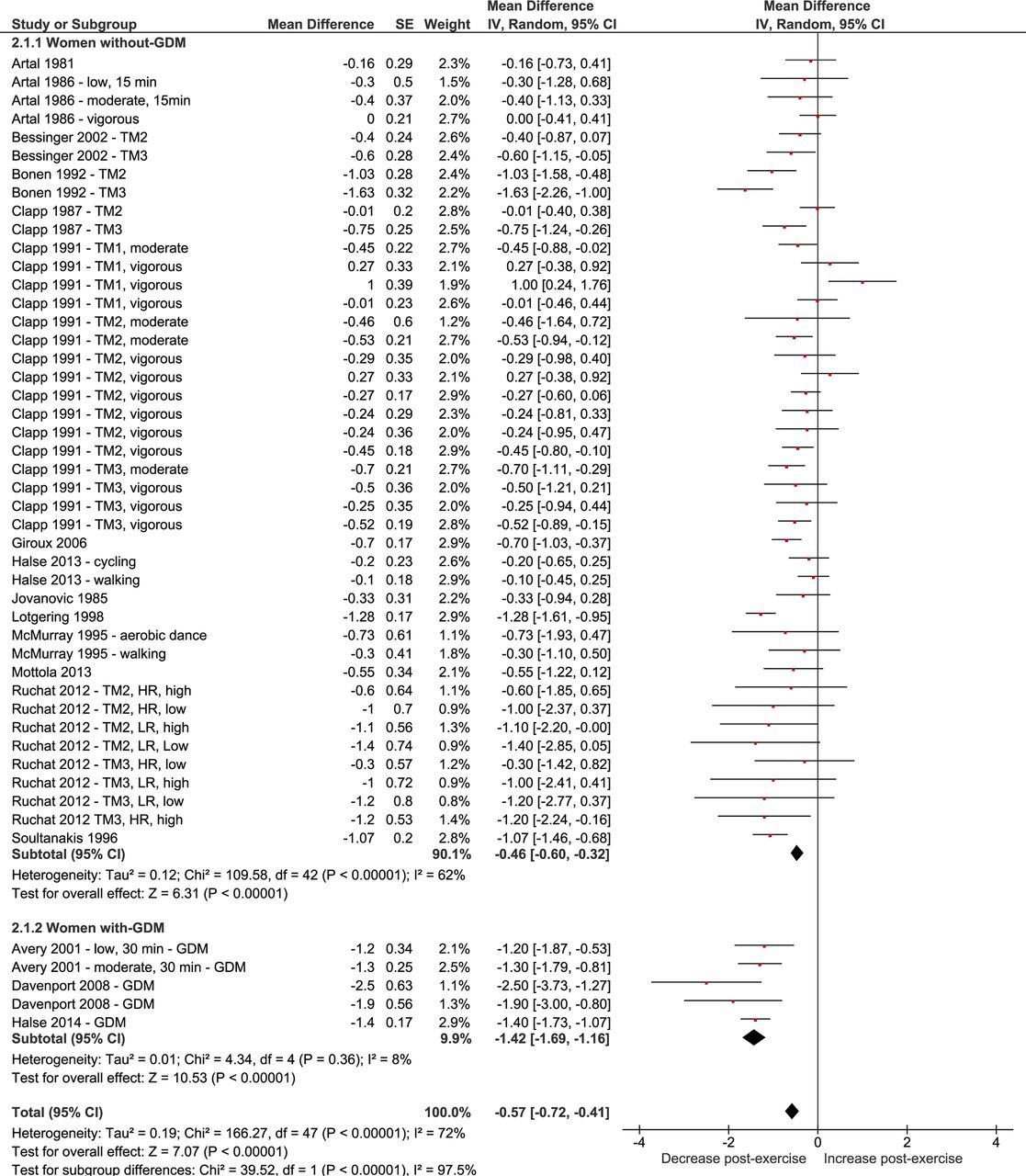
Meta-regression analyses demonstrated an inverse dose–response relationship between volume of exercise (MET minutes per sessions) and glycaemic response postacute exercise, indicating that larger volumes of exercise translated into greater reductions in blood glucose after an acute bout of exercise (see online supplementary figure 6). This relationship is consistent with findings from subgroup analyses, which demonstrated that both exercise intensity (tests for subgroup differences, p=0.01) and duration (tests for subgroup differences, p<0.001) influenced glycaemic responses after acute exercise (online supplementary figure 5 and figure 2, respectively). In both cases, the quality of evidence was downgraded from ‘low’ to ‘very low’ due to serious inconsistency. Furthermore, subgroup analyses revealed larger reductions in blood glucose after acute exercise in women with GDM (‘low’ quality evidence) compared with women without GDM (p<0.0001; ‘very low’ quality evidence, downgraded due to inconsistency; see figure 3). Since glycaemic responses postacute exercise varied by GDM status, sensitivity analyses were conducted removing studies that included women with GDM exclusively. Once these studies were removed, only exercise duration (p<0.001) but not intensity (p=0.15) influenced glycaemic responses after acute exercise. Finally, the test for subgroup differences was significant, indicating there were larger decreases in blood glucose after acute exercise in women who were previously inactive (p=0.002; ‘very low’ quality evidence, downgraded due to inconsistency) compared with women who had an unspecified previous physical activity level (‘very low’ quality evidence, downgraded due to inconsistency) or were previously active (‘low’ quality of evidence; see online supplementary figure 7).
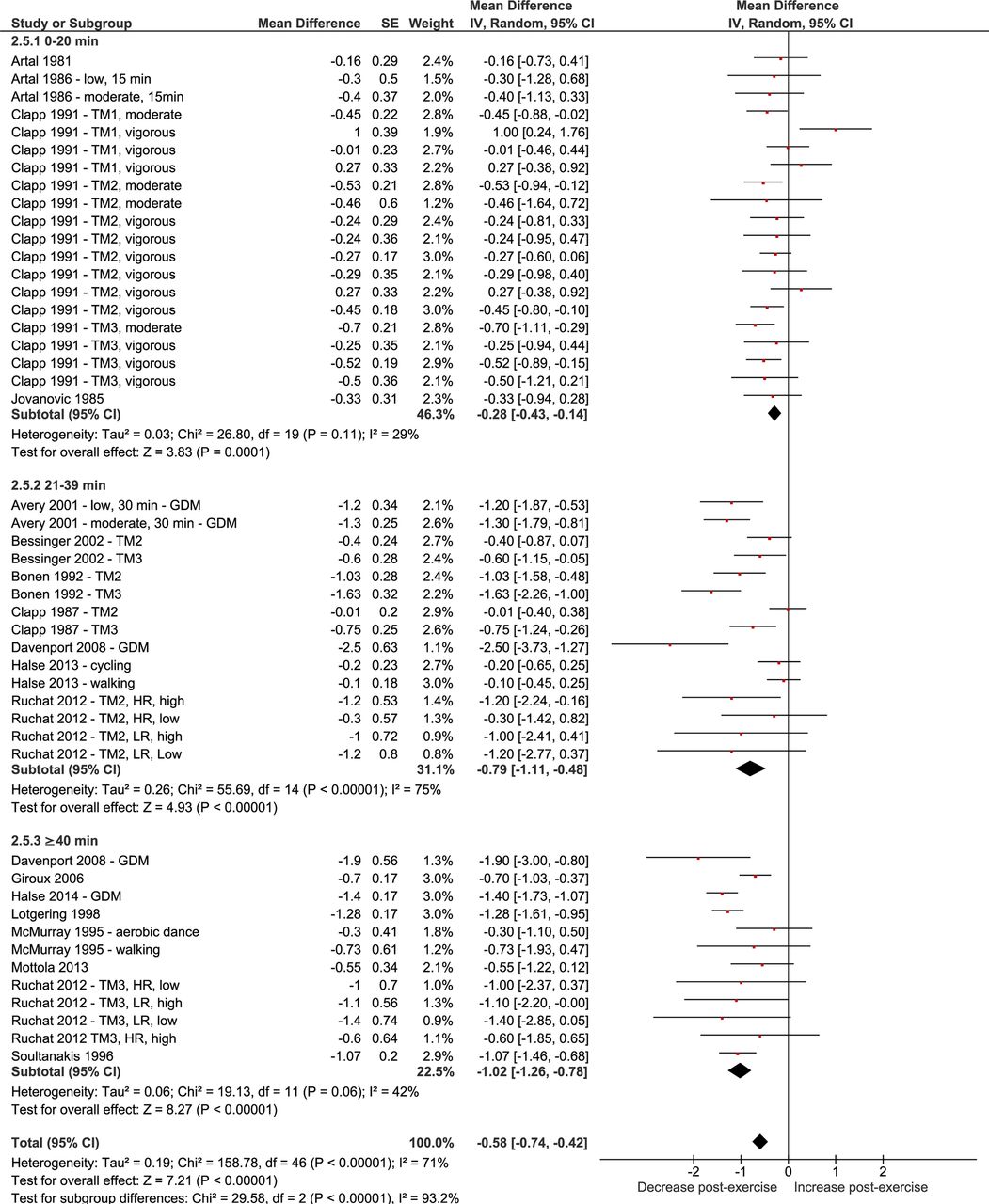
Impact of acute prenatal exercise on glycaemic response from pre-exercise to postexercise. Subgroup analyses were stratified by exercise duration (≤20, 21–39, ≥40 min). Blood glucose values reported in mmol/L. Analyses conducted with a random-effects model. GDM, gestational diabetes mellitus; HR, high risk of GDM; IV, inverse variance; LR, low risk of GDM; TM1, first trimester; TM2, second trimester; TM3, third trimester.
{kind=link}
{kind=link}
{kind=link}
Impact of acute prenatal exercise on glycaemic response from pre-exercise to postexercise. Subgroup analyses were stratified by pregnancy complication (women without and with GDM). Blood glucose values reported in mmol/L. Analyses conducted with a random-effects model. GDM, gestational diabetes mellitus; HR, high risk of GDM; IV, inverse variance; LR, low risk of GDM; TM1, first trimester; TM2, second trimester, TM3, third trimester.
Proportion of hypoglycaemia
There was ‘low’ quality evidence from 8 studies (n=194 exercisers) showing an overall proportion of hypoglycaemia of 0% (95% CI 0% to 4%; online supplementary figure 8).36 38 39 41 44 46 50 51 There was also ‘low’ quality evidence from subgroup analyses indicating the proportion of hypoglycaemic events in women without GDM to be 1% (95% CI 0.00 to 0.66)36 39 46 and in women with GDM to be 0% (95% CI 0.00 to 0.04).38 41 43 50 51 Of the eight studies, two reported no hypoglycaemic events following acute exercise in women who were previously inactive,50 51 one reported no hypoglycaemic events following exercise in women who were previously active,39 and one reported a proportion of hypoglycaemic events in women with overweight or obesity prior to pregnancy of 1% (95% CI 0.00 to 0.04).38
Glycaemic response to chronic prenatal exercise
There was ‘very low’ quality evidence from 23 RCTs (6183 women). The quality of evidence was downgraded from ‘high’ to ‘very low’ due to serious risk of bias, inconsistency and indirectness. The pooled estimate was based on 20 studies and revealed that postintervention fasting blood glucose among women randomised to an exercise intervention was 0.32 mmol/L lower than women randomised to the control group (CI −0.45 to −0.19, I2=96%, p<0.001; online supplementary figure 9).41 44 52–72 Three studies could not be included in the meta-analysis.57 60 62 Of these studies, two were RCTs that included exercise only.57 60 One study included women with obesity prior to pregnancy,57 and the other included women at high risk of developing GDM.60 In both studies, glycaemic control was not different between the exercise and control groups postintervention. However, in women with a history of GDM, fasting blood glucose was significantly reduced at the end of an intervention that combined exercise and diet counselling.62
The pooled estimate for the exercise-only interventions was not significantly different from the pooled estimate for the exercise+cointervention subgroups (p=0.08). Both exercise-only interventions (12 RCTs, n=2244; MD −0.48, 95% CI −0.76 to −0.19, I2=97%) and exercise+cointerventions (13 RCTs, n=3688; MD −0.20, 95% CI −0.32 to −0.07, I2=93%; online supplementary figure 9) showed similar blood glucose reduction. Additional RCT subgroup analyses are described in online supplementary figures 10–13 and the Synthesis of data section.
Use of insulin for the management of GDM
There was ‘low’ quality evidence from 11 RCTs (n=2105) indicating that prenatal exercise did not reduce the odds of requiring insulin for the management of GDM compared with no exercise (n=1840; OR: 0.75, 95% CI 0.48 to 1.18, I2=21%; online supplementary figure 14).41 44 51 53 63 72–77 One study that could not be included in the meta-analysis found no difference in the number of women who required insulin between women who did exercise during pregnancy compared with women who did not.77 The quality of evidence was downgraded from ‘high’ to ‘low’ because of serious indirectness and imprecision. One study included in the meta-analysis reported additional adjusted data that supported the findings (OR: 0.84, 95% CI 0.26 to 2.70, after adjusting for age, prepregnancy BMI and metabolic equivalents at baseline).53
The pooled estimate for the exercise-only interventions was not significantly different from the pooled estimate for the exercise+cointervention subgroups (p=0.79). Both exercise-only interventions (n=2) and exercise+cointervention (n=8) did not affect the odds of requiring insulin for GDM management (see online supplementary figure 14).
Other study designs
Similarly, there was ‘very low’ quality evidence (rated down due to serious imprecision) from two non-RCTs showing that interventions did not affect the odds of requiring insulin for the management of GDM (n=126; OR: 0.83, 95% CI 0.39 to 1.78, I2=0%; online supplementary figure 15).38 78 The pooled estimate for the exercise-only interventions was not significantly different from the pooled estimate for the exercise+cointervention subgroups (p=0.81).
Amount of insulin required for the management of GDM
There was ‘moderate’ quality evidence from three RCTs (n=45) showing that women with GDM who were randomised to an intervention required 0.08 units/kg less insulin per day compared with non-exercising women (CI −0.16 to −0.01, I2=16%; online supplementary figure 16).41 51 74 The quality of evidence was downgraded from ‘high’ to ‘moderate’ because of serious indirectness. The pooled estimate for the exercise-only interventions was not significantly different from the pooled estimate for the exercise+cointervention subgroups (p=0.39).
Other study designs
Findings from one non-randomised intervention were consistent with the results from RCTs. There was ‘very low’ quality of evidence (rated down due to serious inconsistency) demonstrating women in the exercise-only intervention required 0.34 units/kg less insulin per day than control women (95% CI −0.56 to −0.12, I2=not available; online supplementary figure 17).38
Discussion
The current systematic review and meta-analysis showed that there was a mean reduction in maternal blood glucose of 0.94 mmol/L from before to during acute exercise that persisted into the recovery period (mean reduction of 0.57 mmol/L from before to following acute exercise). The glycaemic response during and following exercise was influenced in a dose–response manner, such that higher volume exercise (intensity × duration) was associated with a larger reduction in blood glucose. Despite the observed reduction in maternal blood glucose, the incidence of maternal hypoglycaemia was minimal. Overall, exercise-only interventions (ie, exercise performed regularly) reduced fasting blood glucose by 0.48 mmol/L compared with before the intervention. Subgroup analyses revealed a significant reduction in fasting blood glucose values in women with GDM, women with overweight/obesity and previously active women from before to chronic exercise. However, since the quality of the evidence was between ‘very low’ and ‘low’, future research is warranted to elucidate the impact of exercise alone on blood glucose in healthy and complicated pregnancies. The clinical significance of these results is unknown; however, it would appear that acute and chronic exercise does appear to beneficially impact glucose and insulin responses during pregnancy without increasing the risk of hypoglycaemia.
Glycaemic response to an acute bout of prenatal exercise
Overall, we identified that an acute bout of prenatal exercise resulted in a reduction in circulating blood glucose concentrations during and following exercise. Subgroup analysis identified that with longer exercise duration, the decrease in blood glucose values was greater, whereas with increased exercise intensity, the decrease in blood values was attenuated. However, meta-regression analysis showed a dose–response relationship whereby higher volumes of exercise were associated with larger reductions in blood glucose during and following exercise. In non-pregnant women, glucose initially declines in the first 20 min of exercise followed by a return to pre-exercise values with longer duration exercise as hepatic glycogenolysis occurs.79 80 Yet pregnancy is associated with lower hepatic glycogen stores, resulting in a continued decline in blood glucose values.80 81 Importantly, in our study there was a low proportion of hypoglycaemic events in response to acute exercise, reported as 0% in most38 39 41 44 46 50 51 but not all studies.36
Glycaemic response following chronic exercise
Overall, our analyses demonstrated that the fasted blood glucose values of pregnant women randomised to an exercise-only intervention were 0.48 mmol/L lower on average than their non-exercising counterparts. However, sensitivity analyses identified that this reduction was driven by women diagnosed with diabetes. Since reductions in fasting blood glucose are an indication of the efficacy of prenatal exercise in improving glycaemic control, these results suggest prenatal exercise may be an important component of GDM management. However, caution should be taken when interpreting the above results, since it is not known whether the use of insulin or other glucose sensitising agents may confound the observed results.
Despite the reduction in glucose following an intervention, the need for adjunct insulin did not change. However, the amount of insulin required by women who exercised was lower than those who did not. This suggests that women who exercise regularly in pregnancy have improved glycaemic response since they can maintain lower blood glucose in conjunction with insulin therapy as compared with women who do not exercise regularly in pregnancy. Further investigation is warranted as the number of women requiring insulin and/or the amount of insulin used was often not reported.
To our knowledge, this is the first systematic review and meta-analysis examining glycaemic responses during and following acute exercise, as well as in response to exercise-only chronic interventions. A previous meta-analysis examined the impact of chronic exercise on fasting glucose values in women with GDM and found similar results (MD −0.59, 95% CI −1.07 to −0.11, I2=73%; 4 studies, n=363)82; however, this meta-analysis did not further examine the effect of exercise alone, nor did it examine acute exercise.
Although exercise is established to improve glycaemic control in non-pregnant populations with diabetes,8 the unique metabolic adaptations to pregnancy, including increased hepatic glucose production and enhanced beta-cell function, may mediate the impact of exercise on maternal glycaemic control.83 By late pregnancy, reductions in glucose uptake manifest despite rising circulating insulin levels.83 Although the mechanisms by which advancing gestation is associated with peripheral insulin resistance are not well understood, pregnancy may be associated with an impaired insulin signalling cascade leading to a decrease in GLUT 4 translocation, and therefore reduced glucose uptake. In contrast, the reductions in fasting blood glucose in response to chronic prenatal exercise may be related to enhanced GLUT 4 translocation in the skeletal muscle.1 Future research is required to elucidate the impact of pregnancy complications, prepregnancy BMI and previous levels of activity, as well as exercise characteristics, including duration and intensity, on fasting glycaemic response to determine the most effective interventions to maintain adequate glycaemic control in pregnancy.
Strengths of the current study include the synthesis of available literature spanning 21 countries and the use of GRADE methodology. Meta-regression analyses were performed to examine possible dose–response relationships between characteristics of acute exercise and blood glucose values. Finally, both acute and chronic exercise studies were stratified by the presence or absence of diabetes in pregnancy to better understand the impact of exercise on glycaemic response in these two metabolically distinct groups. A limitation of this review was that we did not explore the potential impact of maternal eating patterns before exercise on glycaemic response to exercise. Timing of the last meal or snack before exercise may affect glucose response to exercise.38 Second, we were unable to identify the source of heterogeneity observed in the acute responses to prenatal exercise. Possible explanations include the relatively small sample size (<2000 women), differences in trimester, variability in the timing of glucose measures and/or timing of the pre-exercise meal. Despite these limitations, the present systematic review and meta-analysis provides important insight into the impact of acute and chronic prenatal exercise on glycaemic control.
Conclusion
The current systematic review and meta-analysis demonstrated a reduction in blood glucose concentrations in women with and without diabetes in pregnancy during and following acute prenatal exercise, as well as following chronic exercise interventions. Pregnant women had a low incidence of hypoglycaemia, suggesting that prenatal exercise does not increase the risk of hypoglycaemic events. Of interest, greater reductions in blood glucose values were observed in women with diabetes and those women categorised as overweight or obese. Finally, prenatal exercise as a management strategy for GDM did not alter the use of insulin but did reduce the required dose of insulin. Further research is warranted given the ‘very low’ to ‘low’ quality evidence on which these conclusions are based.
What is already known
During healthy pregnancy, insulin resistance at the level of the skeletal muscle develops to ensure adequate supply of nutrients to the fetus.
In 6%–9% of pregnancies, gestational diabetes mellitus develops.
Exercise has been suggested to reduce the risk of gestational diabetes mellitus.
What are the new findings
Acute bouts of exercise demonstrated a dose–response relationship, where greater volumes of acute exercise (intensity × duration of exercise) resulted in greater reductions in glucose during and following exercise.
The risk of hypoglycaemia following exercise was low.
Chronic exercise during pregnancy was associated with a reduction in fasting blood glucose values in women with, but not without, diabetes at the end of pregnancy.
References
Footnotes
Contributors MHD, S-MR, MFM, GAD, KBA contributed to the conception of the study. MHD, S-MR, MFM, GAD, KBA, AJG, NB, VJP, CEG, LGS, RB contributed to the design of the study and development of the search strategy. LGS conducted the systematic search. FS, RJS, VLM, LR, MJ, TSN, A-AM completed the acquisition of data. FS, MHD, NB performed the data analysis. All authors assisted with the interpretation. FS, MHD were the principal writers of the manuscript. All authors contributed to the drafting and revision of the final article. All authors approved the final submitted version of the manuscript.
Funding The study is funded by a Canadian Institutes of Health Research Knowledge Synthesis Grant (140995). MHD is funded by an Advancing Women’s Heart Health Initiative New Investigator Award supported by Health Canada and the Heart and Stroke Foundation of Canada (0033140). RJS is funded by a Canadian Institutes of Health Research Doctoral Research Award (146252). A-AM is funded by a Fonds de Recherche du Québec - Santé Doctoral Research Award (34399).
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.