Article Text

Abstract
Background There are plausible mechanisms whereby leisure time physical activity may protect against low back pain (LBP) but there have been no quality systematic reviews and meta-analyses of the subject.
Objective This review aims to assess the effect of leisure time physical activity on non-specific LBP.
Methods Literature searches were conducted in PubMed, Embase, Web of Science, Scopus and Google Scholar databases from their inception through July 2016. Methodological quality of included studies was evaluated. A random-effects meta-analysis was performed, and heterogeneity and publication bias were assessed.
Results Thirty-six prospective cohort studies (n=158 475 participants) qualified for meta-analyses. Participation in sport or other leisure physical activity reduced the risk of frequent or chronic LBP, but not LBP for > 1 day in the past month or past 6–12 months. Risk of frequent/chronic LBP was 11% lower (adjusted risk ratio (RR)=0.89, CI 0.82 to 0.97, I2=31%, n=48 520) in moderately/highly active individuals, 14% lower (RR=0.86, CI 0.79 to 0.94, I2=0%, n=33 032) in moderately active individuals and 16% lower (RR=0.84, CI 0.75 to 0.93, I2=0%, n=33 032) in highly active individuals in comparison with individuals without regular physical activity. For LBP in the past 1–12 months, adjusted RR was 0.98 (CI 0.93 to 1.03, I2=50%, n=32 654) for moderate/high level of activity, 0.94 (CI 0.84 to 1.05, I2=3%, n=8549) for moderate level of activity and 1.06 (CI 0.89 to 1.25, I2=53%, n=8554) for high level of activity.
Conclusions Leisure time physical activity may reduce the risk of chronic LBP by 11%–16%. The finding, however, should be interpreted cautiously due to limitations of the original studies. If this effect size is proven in future research, the public health implications would be substantial.
- Back pain
- epidemiology
- exercise
- hospitalisation
- incidence
- leisure activities
- sport
Statistics from Altmetric.com
Introduction
Low back pain (LBP) is a major global health problem.1 The prevalence of LBP in the past 12 months ranges between 25% and 40%2–5 and that of chronic LBP ranges between 4% and 25%.4 6 Both the prevalence and incidence of LBP increase with age.2 6 7 Of lifestyle risk factors, smoking8 9 and obesity10 11 are associated with increased risk of LBP and clinically verified sciatica. The role of leisure time physical activity in LBP is uncertain.
Leisure time physical activity is any bodily movement produced by the contraction of skeletal muscles that requires energy expenditure, such as walking or climbing stairs.12 Exercise is a specific form of leisure time physical activity that is a purposeful, planned and repetitive activity (eg, swimming, cycling or running), often with the goal of improving or maintaining physical fitness or other health benefits.12 In general, the intensity of leisure physical activity is light to moderate and that of exercise is moderate to strenuous.13 To date, several systematic reviews of observational studies found either no evidence for a relationship between leisure time physical activity and LBP14–17 or an increased risk of LBP in active individuals.18 Some systematic reviews showed no associations of leisure time physical activity with new episodes of LBP,15 LBP intensity, disability due to LBP or healthcare utilisation for LBP.16 Moreover, a systematic review found no evidence for an association between sedentary lifestyle or prolonged sitting during leisure time and LBP.19 On the other hand, another systematic review of observational studies found an increased risk of LBP in individuals performing strenuous physical activity during their leisure time.18
LBP is a common recurrent condition. There may be a reverse causation between leisure time physical activity and LBP. Individuals with LBP may limit their leisure time physical activities due to fear of pain.20 Individuals with LBP may also practice physical activities during leisure time due to medical recommendation. Many previous reviews14 16 18 on leisure time physical activity combinedboth cross-sectional and cohort studies or combinedthe results of studies conducted exclusively in patients with LBP with the results of studies conducted in individuals without LBP. Cross-sectional studies are more prone to reverse causation bias than prospective cohort studies.21 In a meta-analysis of prospective cohort studies,22 we found that moderate to high level of physical activity during leisure time protects against the development of lumbar radicular pain, while in a meta-analysis of cross-sectional studies,22 we found an increased prevalence of lumbar radicular pain in active individuals compared with inactive participants. In the current systematic review and meta-analysis, we aimed to determine the effects of moderate and high levels of leisure time physical activity on different types of non-specific LBP. To limit reverse causation bias, we restricted our meta-analysis to prospective cohort studies only.
Methods
This section is similar to that published in Shiri et al.22
Search strategy
The PRISMA statement23 was used when developing the review protocol and meta-analysis. Comprehensive literature searches were conducted in PubMed, Embase, Scopus, Web of Science, Google Scholar and ResearchGate databases from their inception through July 2016, using predefined combinations of Medical Subject Headings terms (PubMed, see online Supplementary table 1), Emtree terms (Embase) and text words. There were no restrictions on language and age or sex of participants. The reference lists of included articles were also hand-searched for additional reports that might be relevant. The full text of studies on body mass index and smoking in relation to LBP were also looked at in case they reported results for leisure time physical activity.
Inclusion and exclusion criteria
The titles, abstracts and full texts of potentially relevant reports were screened to identify studies on the association of leisure time physical activity/inactivity with LBP. Only prospective cohort studies were eligible for inclusion in the review if they studied the effect of leisure time physical activity on non-specific LBP and at least some of the participants were free from LBP at baseline. We excluded studies on specific low back disorders such as sciatica, spinal stenosis or other spinal pathologies; studies that enrolled exclusively patients with LBP; studies on back pain combined with neck pain; studies on muscle-strengthening exercise and pregnancy-related LBP; and studies that did not report quantitative data to estimate a relative risk. The corresponding authors of eight studies24–31 were contacted for additional results; of them, six26–31 provided us with the new results.
Outcome
Following the outcomes used in the eligible studies, LBP outcomes of interest were as follows: LBP in the past month, LBP in the past 6–12 months, frequent (recurrent) LBP; chronic LBP; sick leave due to LBP and hospitalisation for LBP. Chronic LBP was defined as pain that lasts for 3 months or longer or pain for more than 30 days in the past 12 months.32
Exposure
Following the approach of studies that were eligible for inclusion, being physically active was defined as participation in a sport or other physical activity during leisure time,33–45 at least 1–2 times a week,5 27 29–31 46–50 at least 0.5–1.0 hour per week4 51 or being in the middle or upper third of the distribution of leisure time physical activity in a study sample.7 26 28 52–55 Moderate level of physical activity was defined as participation in such activity 1–3 times a week,5 29 31 49 1–3 hours per week48 51 or being in the middle third of the distribution of leisure time physical activity in a study sample.7 26 28 53–55 High level of physical activity was defined as participation in leisure time physical activity, ≥ 3–4 times per week,5 29 31 49 56 more than 2–4 hours per week3 24 35 51 57 or being in the upper third of the distribution of such activity in a study sample.7 26 28 53–55 We conducted meta-analyses comparing active versus inactive, moderate versus low activity, high activity versus low activity and high versus low or moderate activity.
Quality assessment
The methodological quality of the included studies was assessed independently by both reviewers using criteria adapted from the Effective Public Health Practice Project tool.58 We assessed four sources of bias: selection bias, performance bias, attrition bias and confounding (see online Supplementary table 2). Disagreements between raters were resolved through discussion.
Meta-analysis
From each study, we abstracted maximally adjusted risk estimates for the exposures and outcomes of interest, together with their 95% CIs. For the prospective cohort studies that reported ORs, we converted ORs into risk ratios (RRs).59 For one study52 that did not report a CI for the HR, the SE was calculated using the following formula: SE=log(HR)/Z value.60
Several studies4 5 38 42 43 48 52 used high or moderate/high level of physical activity as a comparison group and explored the associations of inactivity versus activity, low versus high and moderate versus high level of leisure time physical activity with LBP. An RR for high level of physical activity was calculated by inversing the RR for physical inactivity, and an RR for moderate level of physical activity by dividing the RR for moderate activity by the RR for inactivity. The SE of the estimate for physical inactivity was then used to calculate 95% CI for high level of activity. For moderate level of activity, its own SE was used. SE and 95% CI were calculated using natural logarithm of lower and upper limits of the CI. A reanalysis of data from two31 54 of the included studies showed that this approach is valid.
Some studies reported two or more risk estimates for the associations of different types of sport activities with LBP,36 49 50 two or more risk estimates for the association between physical activity and LBP for different follow-up periods24 or the association of physical activity with two or more outcomes.42 In these studies, some participants contributed data to more than one risk estimate. In this case, results were combined by a fixed-effect meta-analysis to give an overall pooled estimate for physical activity versus physical inactivity for the study. Moreover, the variance of the pooled estimate was corrected using a method suggested for combining multiple outcomes or multiple timepoints within a study.61
A fixed-effect meta-analysis was used to combine the independent subgroups of a single study and a random-effects meta-analysis was used to combine the estimates of different studies.60 The presence of heterogeneity across the studies was assessed by the I2 statistics.62 An I2 statistic less than 25% indicates small inconsistency and more than 50% indicates large inconsistency.63 Sensitivity analyses were performed with regard to the presence or absence of LBP at baseline, age of participants, adjustment for confounding factors and other methodological quality of included studies. Meta-regression64 was used to explore, whether study-level covariates accounted for the observed heterogeneity and to test for differences in the RR between two or more subgroups. The influence of each individual study on the summary estimate was examined by repeating the meta-analysis with one study out at a time. A funnel plot was used for exploring publication bias, and Egger’s regression test was used for examining funnel plot asymmetry. Furthermore, the trim and fill method was used to adjust for missing studies due to publication bias.65 66 Stata, V.13, was used for the meta-analyses.
Results
Study selection
Our electronic searches of multiple databases identified 12 434 publications (see online Supplementary figure 1). We screened the full text of 561 relevant publications on the association between physical activity and low back disorders. Of 52 eligible studies on LBP, we excluded five on back pain combined with neck pain, seven with insufficient data to estimate an RR, one that assessed both physical activity and LBP at follow-up, one that combined leisure time physical activity with physical activity at work, one on muscle-strengthening exercises and, lastly, one in pregnant women (see online Supplementary figure 1).
Finally, 36 studies (37 reports, n=158 475 participants)3–5 7 24 26–31 33–57 67 on relationship between leisure time physical activity and LBP qualified for meta-analyses. The countries with the largest number of included studies comprised Finland (n=7), Denmark (n=6), UK (n=4), USA (n=4), Netherlands (n=3), Norway (n=3), Australia (n=2) and Israel (n=2). Canada, France, Italy, Hong Kong and Thailand provided one study each (see online Supplementary table 3).
Leisure time physical activity
Of 36 included studies, 26 inquired participation in organised sport or other leisure time physical activities and 10 studies7 24 28 31 33 38 41 43 48 67 participation in organised sport activities only (see online Supplementary table 3). Only two studies26 55 measured physical activity by an accelerometer, and only three studies28 52 54 defined the levels of physical activity by using a physical activity index or metabolic equivalent of task (MET). Seven studies27 29 30 34 41 47 49 defined the levels of physical activity based on frequency of weekly physical activity, five24 35 43 45 51 defined the levels based on number of hours per week, seven3 4 37 39 42 53 57 defined the levels based on number of hours and intensity of activity, four5 7 46 48 defined the levels based on frequency and duration of activity, one31 defined the levels based on frequency and intensity of activity and one56 defined the levels based on frequency, duration and intensity of activity. Moreover, participation in sport or other leisure time physical activities was based on a yes/no question in six studies,33 36 38 40 44 67 which only one36 considered duration and one44 considered intensity of activity.
Methodological quality of included studies
Eight studies were rated as having low risk of selection bias, 19 studies were rated as having moderate risk and nine were rated as having high risk of selection bias (see online Supplementary table 3). Nine studies were assessed as having low risk of performance bias, 23 were assessed as having moderate risk and four were assessed as having high risk of performance bias. Fifteen studies were rated as having low risk of attrition bias, 14 were rated as having moderate risk and seven were rated as having high risk. Twenty-eight studies controlled their risk estimates for some confounding factors such as age, sex and body mass index.
Association between leisure time physical activity and low back pain
Low back pain in the past month and low back pain in the past 6–12 months
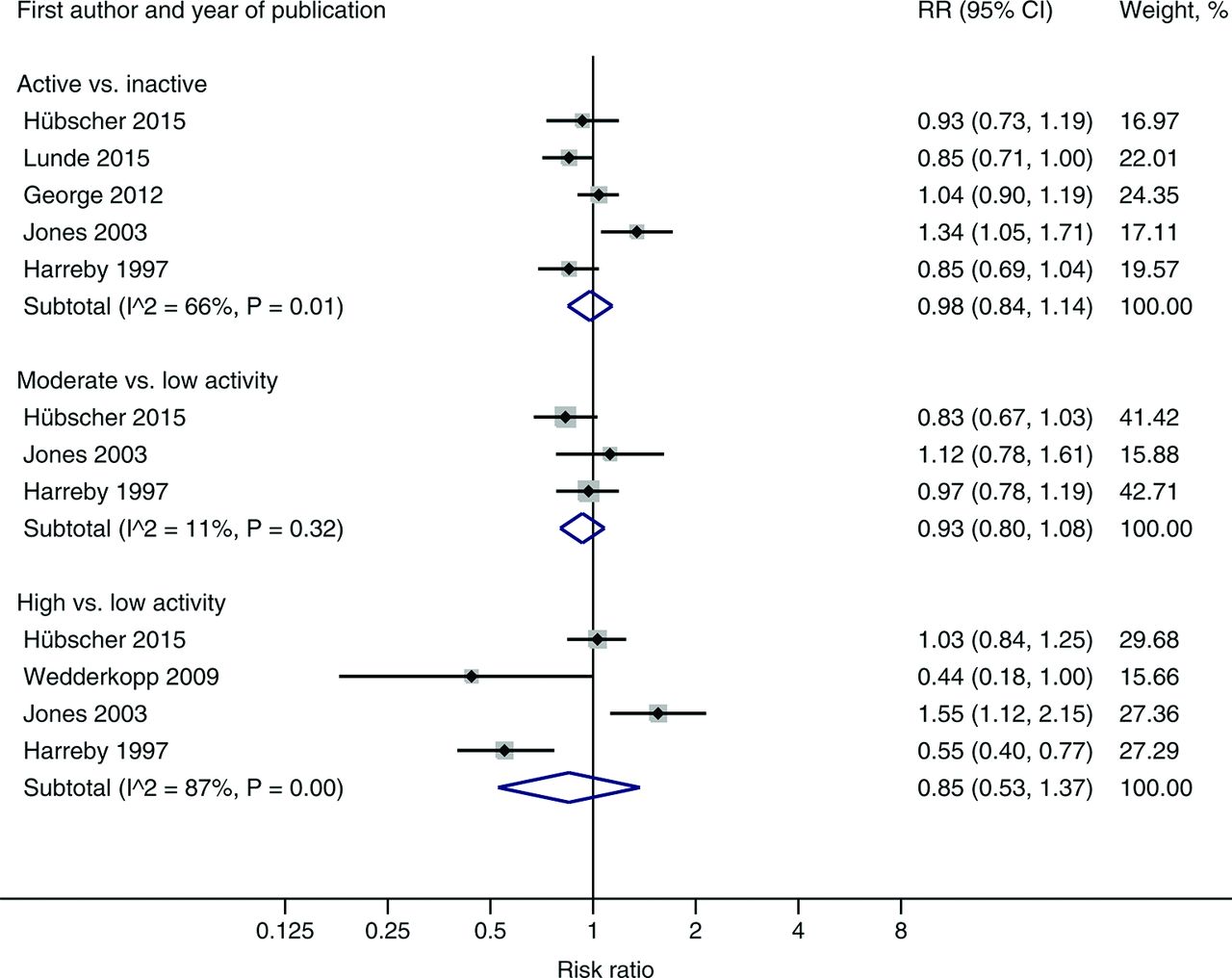
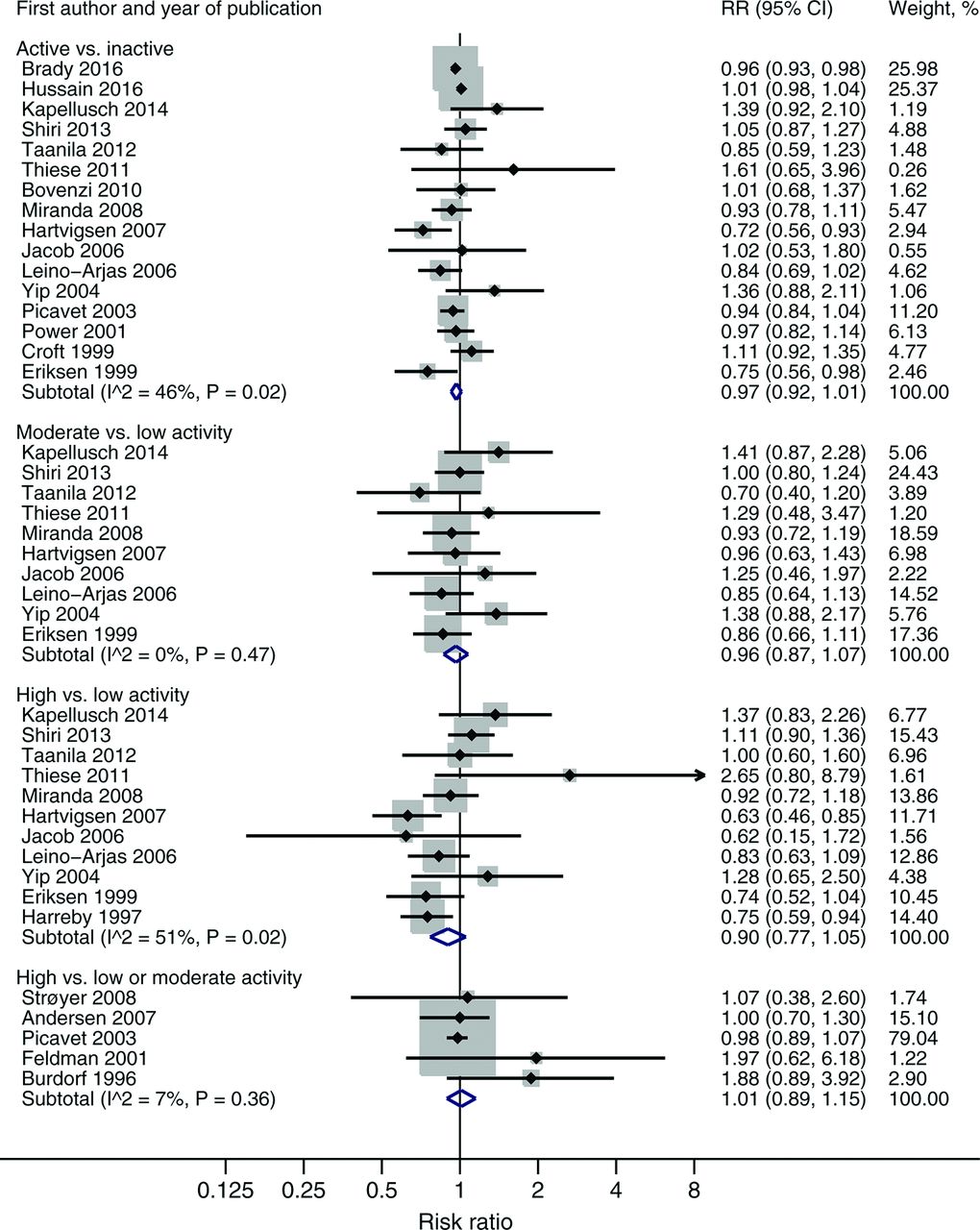
Leisure time physical activity was neither associated with LBP in the past month (table 1 and figure 1) nor associated with LBP in the past 6–12 months (table 1 and figure 2). Compared with individuals with no regular physical activity, pooled RR of LBP for > 1 day in the past 1–12 months was 0.98 (CI 0.93 to 1.03, I2=50%, 16 studies, n=32 654 participants) for physically active individuals, 0.94 (CI 0.84 to 1.05, I2=3%, eight studies, n=8549) for moderately active individuals and 1.06 (CI 0.89 to 1.25, I2=53%, nine studies, n=8554) for highly active individuals in a meta-analysis of studies that controlled their risk estimates for some potential confounders (table 2). The association of leisure physical activity with LBP in the past 6–12 months did not differ between men and women (table 1).

A meta-analysis of six studies on the effect of leisure time physical activity on low back pain in the past month. The size of the grey-shaded area indicates the weight of each study. Horizontal lines show the 95% CIs. RR, risk ratio.

A meta-analysis of 21 studies on the effect of leisure time physical activity on low back pain in the past 6–12 months. The size of the grey-shaded area indicates the weight of each study. Horizontal lines show the 95% CIs. RR, risk ratio.
Sex-specific meta-analysis of prospective cohort studies on the association between leisure time physical activity and low back pain
Sensitivity analyses with regard to adjustment for publication bias, presence of low back pain at baseline, age of participants, adjustment for confounding factors and other methodological quality of included studies
Five studies3 4 24 57 67 on LBP in the past 6–12 months compared participants with high level of leisure time physical activity with those with low or moderate level of activity. The pooled RR across these five studies was 1.01 (CI 0.89 to 1.15, I2=7%, n=6151, figure 2). Of the five studies, four3 4 57 67 controlled their risk estimates for some confounding factors.
Frequent or chronic low back pain
Of two studies46 47 on frequent LBP and seven4 33 34 37 39 51 52 studies on chronic LBP, eight studies inquired participation in a sport or other leisure time physical activity and one33 participation in an organised sport activity only. Three studies4 37 39 defined the levels of leisure physical activity based on number of hours per week and intensity of activity, two34 47 were based on frequency of weekly physical activity, one51 was based on number of hours per week, one46 was based on frequency and duration of activity, one52 was based on a physical activity index and one33 was based on a yes/no question. Of two studies on frequent LBP, one46 defined it as experiencing at least 10 times LBP, while the other study47 did not report the frequency of pain. In the latter study,47 however, 61% of the participants had pain on a daily or weekly basis.
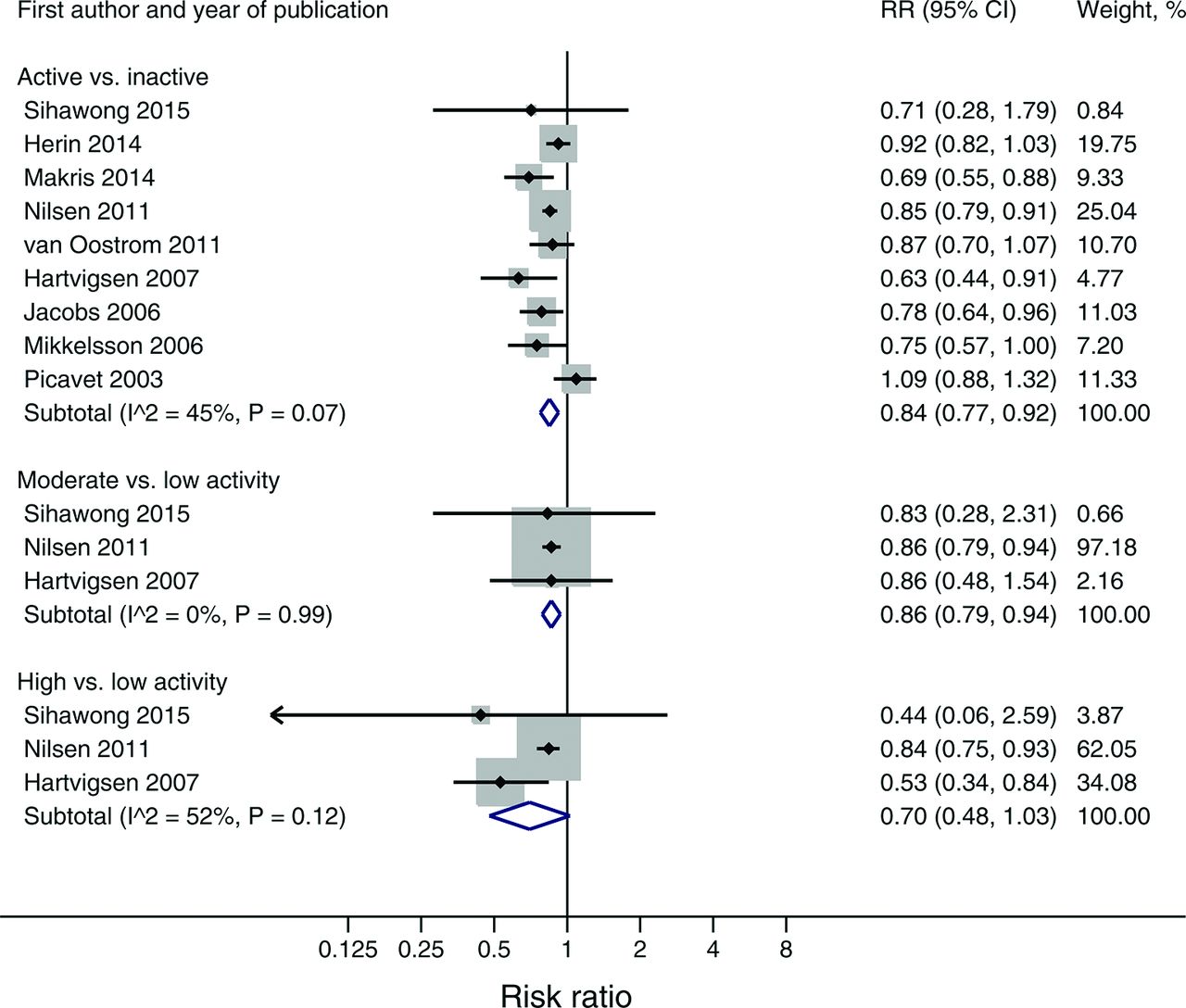
Participation in a sport or other leisure time physical activity was inversely associated with frequent or chronic LBP (table 1 and figure 3). In a meta-analysis of six studies that controlled their risk estimates for some potential confounders, the risk of frequent or chronic LBP was lower by 11% (RR=0.89, CI 0.82 to 0.97, I2=31%, six studies, n=48 520, table 2) in physically active individuals, 14% (RR=0.86, CI 0.79 to 0.94, I2=0%, two studies, n=33 032) in moderately active individuals and by 16% (RR=0.84, CI 0.75 to 0.93, I2=0%, two studies, n=33 032) in highly active individuals in comparison with individuals with no regular physical activity. All the six studies controlled the estimates for age, five controlled also for sex and body mass index, two controlled for smoking,37 51 one controlled for educational level,37 one controlled for job demands,34 one controlled for social class33 and one controlled for occupation.51 Excluding the largest study51 did not change the main results (table 2). The associations of moderate and moderate/high levels of physical activity with frequent or chronic LBP were statistically significant in both men and women, whereas the effect of high level of physical activity was statistically significant in men only (RR=0.68, CI 0.46 to 0.99 for men, and RR=0.82, CI 0.55 to 1.20 for women). One39 of the included studies recruited a representative sample of twins and conducted a co-twin control design to control for environmental and genetic factors. The analysis of twins' pairs discordant for high level of physical activity at baseline showed a strong protective effect of physical activity against chronic LBP (see online Supplementary table 3).

{kind=link}
{kind=link}
{kind=link}
A meta-analysis of nine studies on the effect of leisure time physical activity on frequent or chronic low back pain. The size of the grey-shaded area indicates the weight of each study. Horizontal lines show the 95% CIs. RR, risk ratio.
Sick leave and hospitalisation for low back pain
Leisure time physical activity was not associated with sick leave or hospitalisation due to LBP. In both sexes combined, the pooled RR of sick leave due to LBP was 0.97 (CI 0.77 to 1.22, I2=0%, two studies, n=5106) for active compared with inactive. Pooled RR of hospitalisation due to LBP for participation in a sport club was 1.04 (CI 0.90 to 1.21) for males, 1.26 (CI 0.73 to 2.17) for females and 1.07 (CI 0.84 to 1.35, I2=50%, two studies, n=66 424) for both sexes.
Heterogeneity and publication bias
Overall, the level of heterogeneity was low to moderate. Heterogeneity across studies on frequent or chronic LBP was explained fully by selection bias and adjustment for confounding factors (tau-square=0, adjusted R2=100%, I2 residual=0%). The pooled RR across four studies33 37 46 51 with low or moderate selection bias that controlled their risk estimates for some confounders was 0.86 (CI 0.82 to 0.91, I2=0%, n=44 146) for active versus inactive. Heterogeneity across studies on LBP in the past 1–12 months was partly explained by selection bias.
Egger’s test did not show publication bias for LBP in the past 1–12 months as well as for frequent or chronic LBP. For LBP in the past 1–12 months, p value for Egger’s test was 0.78 for 20 studies on active versus inactive (see online Supplementary figure 2), 0.12 for 12 studies on moderate versus low physical activity and 0.89 for 13 studies on high versus low physical activity. The trim and fill method did not impute any missing studies due to publication bias showing no or harmful effect for leisure time physical activity (table 2), whereas it imputed three missing studies showing protective effect for moderate level of physical activity on LBP in the past 1–12 months (see online Supplementary figure 3) and the pooled RR reduced to 0.92 (95% CI 0.83 to 1.02) after adjustment for missing studies. p Value for Egger’s test was 0.38 for nine studies on frequent or chronic LBP for active versus inactive (see online Supplementary figure 4). The trim and fill method, however, imputed three missing studies due to publication bias (see online Supplementary figure 4), and the pooled RR increased to 0.88 (95% CI 0.80 to 0.96) after adjustment for publication bias.
Sensitivity analysis
An adjustment for funnel plot asymmetry using the trim and fill method did not change the pooled estimates for both LBP in the past 1–12 months and frequent or chronic LBP (table 2). The pooled RR of frequent or chronic LBP for active versus inactive was stronger in elderly (70+) than in adults (RR 0.73 vs 0.90, table 2). However, all five studies4 33 34 37 51 in adults controlled their risk estimates for some confounders, whereas none of the three studies39 47 52 in elderly controlled for any confounding factor. The studies that did not adjust their risk estimates for any confounding factor reported a stronger inverse association between physical activity and frequent or chronic LBP than the studies that controlled their estimates for some confounders. Other methodological quality of the included studies had no impact on the pooled estimates (table 2).
Of the six studies on frequent or chronic LBP that controlled the estimates for some confounding factors, only two33 51 were rated as having low risk of both selection bias and attrition bias. The combined RR across these two studies was 0.87 (CI 0.81 to 0.94, I2=25%, n=39 210) for active compared with inactive. Both studies controlled the estimate for age, sex and body mass index; one33 controlled further for social class and one51 controlled for occupation and smoking. However, one51 of the studies defined the levels of leisure time physical activity based on the number of hours spent on physical activity per week, and the other one33 was based on a yes/no question only.
Discussion
This meta-analysis suggests that moderate to high level of physical activity during leisure time protects against frequent or chronic LBP by 11%–16%. However, leisure time physical activity is not associated with changes in risk of LBP in the past month or in the past 6–12 months.
Chronic low back pain
In the current meta-analysis, the studies on chronic LBP, except one, included participants free from chronic LBP at baseline in the analysis. The possibility of reverse causation bias is therefore less likely. However, individuals may have had LBP before entering into the studies. Individuals with a history of frequent or chronic LBP are more likely to become less active during their leisure time than those without LBP.20 Furthermore, a history of LBP is a strong predictor of future LBP.34 In line with the current review, in a meta-analysis of prospective cohort studies, we found that high level of leisure time physical activity reduces the risk of lumbar radicular pain by 16%.22 Physical activity during leisure time may have a role in preventing chronic LBP.
The mechanisms underlying the preventive effect of physical activity against chronic LBP are unclear. Physical activity interventions for LBP are commonly proposed to work by changing things like posture and muscle activation. Yet, there is a lack of evidence linking the effects of exercise in LBP to changes in the musculoskeletal system.68–70 However, changes are seen in variables like fear, catastrophising, self-efficacy and beliefs.71 72 There is now strong evidence that LBP is best understood from a biopsychosocial perspective as it can involve combinations of different psychological, social, lifestyle and physical factors.73 Therefore, future research on physical activity interventions for LBP should involve measuring an array of biopsychosocial variables to further our understanding of mechanisms of effect of physical activity in this population.
Other types of low back pain
Leisure time physical activity has no preventive effect on LBP for ≥1 day in the past month or LBP in the past 6–12 months. LBP for a day within a year is a common condition with a prevalence of 25%–40% in the general population.2–5 This type of outcome is non-specific and can be a part of a healthy lifestyle. We also found no association between leisure time physical activity and sick leave or hospitalisation due to LBP. The current meta-analysis had low statistical power for sick leave or hospitalisation. There were only two studies on hospitalisation and two studies on sick leave due to LBP. One49 of these studies was large (n=57 408), but only 1.1% of the study population had been hospitalised for LBP during 11 years follow-up. Furthermore, the studies on sick leave or hospitalisation looked at different types of sport activities and did not consider all leisure activities using a physical activity index or MET. Of the four studies, one41 defined inactive as practising physical activity <2 times per week and one43 as <3 hours per week. This misclassification can underestimate the effect of leisure time physical activity on sick leave or hospitalisation due to LBP.
Limitations
The current meta-analysis had some limitations. The included studies recruited various population groups. Due to a small number of cohort studies conducted in adolescents and elderly people, this meta-analysis had a low statistical power to determine whether age modifies the association between leisure time physical activity and LBP. In older people, inactivity is more likely to be a consequence of chronic LBP.17 Our sensitivity analysis, however, showed similar association in adults and elderly people. Furthermore, 22% of included studies did not control their risk estimates for any confounding factor. The pooled estimates, however, changed only slightly after excluding the studies that reported unadjusted estimates only. Of studies on frequent or chronic LBP, only very few controlled the estimates for smoking and occupational physical and psychosocial risk factors, and none controlled for depression and fear avoidance beliefs. Individuals with physically strenuous jobs,74 smokers74 and those with depression75 are less likely to engage in leisure time physical activity than individuals with non-manual jobs, never smokers or those without depression. Occupational factors,76 smoking8 and depression77 are also risk factors for LBP; thus, not adjusting the estimates for these known determinants of both leisure time physical activity and LBP may have led to overestimation of protective effect of leisure physical activity on frequent or chronic LBP.
The included studies classified the levels of leisure time physical activity in different ways and used different cutpoints for moderate and high levels of leisure time physical activity. Several studies classified individuals with 2–3 hours per week physical activity during leisure time as inactive. This type of exposure misclassification can lead to underestimation of an association between leisure time physical activity and LBP. We recalculated RRs where possible to compare moderate versus low physical activity and high versus low physical activity. However, some studies allowed classification to active versus inactive only. These studies did not, therefore, contribute to meta-analyses comparing moderate with low physical activity and high with low physical activity.
Only a few studies objectively measured leisure time physical activity, computed total weekly leisure physical activity or considered physical activity during commuting to work. Physical activity assessment methods may have a significant impact on the association between leisure time physical activity and LBP. To date, there is little information on the selection of an appropriate physical activity assessment tool for large epidemiological studies.78 However, self-reports of physical activity can overestimate as well as underestimate the levels of physical activity.79 80 Individuals with LBP may also underestimate or overestimate their level of physical activity.80 81 It is therefore unclear whether using self-reported measures of physical activity have led to underestimation or overestimation of the observed association between leisure time physical activity and LBP.
Implications and recommendations for research
Consistent assessments of both physical activity and LBP across studies are needed to understand the effect of physical activity on LBP. In addition to new episodes of LBP, future prospective studies should also explore the effect of leisure time physical activity on LBP severity, chronicity and disability. Studies on LBP should consider not only all dimensions of physical activity (type, frequency, duration and intensity) but also all domains of physical activity (leisure time, household, commuting and work). The levels of leisure time physical activity should be defined based on total weekly moderate-intensity physical activity and vigorous-intensity physical activity. Furthermore, future studies should control the association between physical activity and LBP for all known confounding factors, including age, sex, education, social class, smoking, body mass index, occupational physical and psychosocial factors, depression and fear avoidance beliefs.
Conclusions
Leisure time physical activity may have a modest protective effect on the development of frequent or chronic LBP. The results, however, should be interpreted cautiously due to limitations of the original studies.
What is already known on this topic?
The role of leisure time physical activity in low back pain is uncertain.
Previous studies have reported inconsistent results regarding the relationship between leisure time physical activity and non-specific low back pain.
What this study adds?
Leisure time physical activity has no preventive effect on low back pain for >1 day in the past month or past 6–12 months.
Leisure time physical activity may provide modest protection against frequent or chronic low back pain.
The protective effect of leisure physical activity on chronic low back pain is seen in both men and women as well as in both adults and older people.
Acknowledgments
This study was supported by the Finnish Ministry of Education and Culture (grant no 253715). We thank Professor Massimo Bovenzi,30 Dr Tamar Jacob,28 Dr Jay M Kapellusch,29 Mr Lars-Kristian Lunde,27 Dr Henri Taanila31 and Dr Matthew S Thiese26 for providing us with additional results.
References
Footnotes
Contributors RS developed the review protocol and conducted the literature searches. Both authors screened the eligible studies and rated the quality of included studies. RS extracted the data, performed the meta-analyses, interpreted the results and drafted the manuscript.
Funding The Finnish Ministry of Education and Culture (grant no 253715).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This paper has been amended since it was published Online First. Owing to a scripting error, some of the publisher names in the references were replaced with ‘BMJ Publishing Group’. This only affected the full text version, not the PDF. We have since corrected these errors and the correct publishers have been inserted into the references.
Linked Articles
- Warm up