Article Text

Abstract
Objective To evaluate the relative risk (RR) of serious and non-serious adverse events in patients treated with exercise therapy compared with those in a non-exercising control group.
Design Systematic review and meta-analysis.
Data sources Primary studies were identified based on The Cochrane Database of Systematic Reviews investigating the effect of exercise therapy.
Eligibility criteria At least two of the authors independently evaluated all identified reviews and primary studies. Randomised controlled trials were included if they compared any exercise therapy intervention with a non-exercising control. Two authors independently extracted data. The RR of serious and non-serious adverse events was estimated separately.
Results 180 Cochrane reviews were included and from these, 773 primary studies were identified. Of these, 378 studies (n=38 368 participants) reported serious adverse events and 375 studies (n=38 517 participants) reported non-serious adverse events. We found no increase in risk of serious adverse events (RR=0.96 (95%CI 0.90 to 1.02, I2: 0.0%) due to exercise therapy. There was, however, an increase in non-serious adverse events (RR=1.19 (95%CI 1.09 to 1.30, I2: 0.0%). The number needed to treat for an additional harmful outcome for non-serious adverse events was 6 [95%CI 4 to 11).
Conclusion Participating in an exercise intervention increased the relative risk of non-serious adverse events, but not of serious adverse events. Exercise therapy may therefore be recommended as a relatively safe intervention.
PROSPERO registration number
CRD42014014819.
- evidence based review
- exercise
- exercise rehabilitation
- exercises
- rehabilitation
Statistics from Altmetric.com
Introduction
Exercise therapy and physical activity are core elements in rehabilitation and treatment of chronic disease,1–4 such as depression,5 pain related to hip6 or knee osteoarthritis7 8 and chronic back pain.9 Furthermore, participation in exercise therapy can improve quality of life in people with cancer10 and following heart failure.11
Physical activity is defined as any bodily movement produced by skeletal muscles which results in energy expenditure.12 Exercise is a subset of physical activity that is planned, structured and repetitive and has the improvement or maintenance of physical fitness as a final or intermediate objective.12 Exercise therapy is defined according to MEDLINE’s Medical Subject Headings as a regimen or plan of physical activities designed and prescribed for specific therapeutic goals.13
Many clinical guidelines recommend exercise therapy as a core element of treatment.14 15 In some cases, clinical guidelines recommend exercise, but advise patients to consider specific symptoms related to the disease, such as risk of hypoglycaemia in type 1 diabetes,16 or recommend avoidance of unsupervised exercise, due to the risk of performing the prescribed exercise incorrectly, and thereby increasing the risk of adverse events.17
An adverse event is an undesirable or harmful outcome that occurs during or after the use of a drug or other interventions but is not necessarily caused by it, and any intervention may be expected to include some risk of adverse events.18 Adverse events can be divided into serious or non-serious. A serious adverse event is defined as an event that leads to either death, hospitalisation or a serious risk of deterioration in health. All other reported adverse events such as pain, fatigue and oedema are defined as non-serious (see https://www.fda.gov/Safety/MedWatch/HowToReport/ucm053087.htm). Adverse events in exercise may vary in severity, type and frequency due to differences in patient groups, settings, type of exercise, dose of exercise, whether the exercise is supervised or not and performed in groups or individually.
According to the Consolidated Standards of Reporting Trials, all serious adverse events in each intervention group should be reported.19 Thus, even though adverse events resulting from exercise interventions are expected to be less frequent and less severe compared with pharmaceutical or surgical interventions, it is important to be aware of the severity, type and frequency of such adverse events. So far, no systematic review has evaluated these aspects of adverse events in exercise therapy. Thus, the aim of this systematic review was to evaluate the relative risk (RR) of serious and non-serious adverse events in patients treated with exercise therapy compared with those in a non-exercising control group. An additional aim was to evaluate the impact of patient group (diagnostic groups), type of exercise, duration of exercise intervention, dose of exercise and delivery mode on the RR of serious and non-serious adverse events.
Methods
Protocol
The eligibility criteria were established, and the study selection, data extraction and statistical analysis were performed as specified in a predefined protocol registered in PROSPERO (International prospective register of systematic reviews) (http://www.crd.york.ac.uk/prospero/).
Eligibility criteria
Types of studies
Eligible randomised controlled trials (RCTs) were identified from systematic reviews investigating the effects of exercise therapy and published in the Cochrane Database of Systematic Reviews (CDSR). RCTs, cluster-randomised trials and randomised cross-over studies were included if they compared an exercise therapy intervention with a non-exercising control treatment.
Types of participants
Studies that included participants with or without a medical condition were eligible, except for participants receiving chemotherapy, as all or nearly all these participants are anticipated to experience adverse events. Otherwise, no studies were excluded based on specific characteristics of the participants.
Types of intervention
Exercise therapy was the main intervention and each exercise session had to include active exercise therapy for at least 50% of the total time. Furthermore, the exercise could not be combined with any pharmacological, surgical, or electrotherapeutic intervention.
Besides strength/resistance, aerobic and neuromuscular exercise (defined as exercise interventions targeting sensorimotor deficiencies and functional stability), the following active exercise interventions were also included: dancing, running, cycling, QiGong and Tai Chi. However, interventions like whole body vibration, facial exercises, yoga, stretching or range of motion exercises or bladder training were excluded. There were no restrictions on the setting in which the exercise therapy was performed, that is, classes, gymnasium, etc.
Types of control intervention
Studies with comparators such as a non-exercise therapy control group, usual care, attention intervention, etc. were included, as were nutraceuticals, placebo and education (eg, back school and similar interventions). However, studies where the control group involved any exercise (including stretching), pharmacological, surgical, or electrotherapeutic intervention were excluded.
Type of outcome measures
The outcomes of interest were measures of adverse events. As classifying adverse events as treatment-related is largely subjective, and with unknown validity,20 the current study was not focused on reported adverse effects, but on adverse events as any undesirable event occurring during the study, divided into serious and non-serious adverse events.
Information sources and search terms
As all the primary research studies were identified through Cochrane systematic reviews, the Cochrane Library (www.cochranelibrary.com) was the only source used for this study, searched from the date of inception to November 12th, 2015. The search terms used were ‘exercise’; ‘training’ and ‘exercise therapy’ searched as title, abstract and keywords. No restriction on publication date was applied.
Study selection
Two members of the study team (TI, CLG) independently evaluated the identified Cochrane reviews to identify systematic reviews examining the effectiveness of exercise therapy. Disagreements between reviewers were resolved by discussion.
RCTs were identified through the reference list of the included systematic reviews and imported to a reference system (ie, EndNote, Thomson Reuters, 1988–2016) by AN. After removing duplicates, each of the six authors (AN, TI, CLG, HL, CBJ) independently evaluated a group of the references, examining the title and abstract, with two reviewers independently scrutinising all references. The full text was obtained if a study were deemed eligible by at least one reviewer. The same reviewers independently judged eligibility of the retrieved full text. Disagreements between reviewers were resolved by discussion.
If the same study was published more than once, the publication reporting the highest number of participants with adverse events was included, to minimise the risk of double counting participants included in trials presented in multiple publications.
Data collection
We developed a data extraction sheet (in Excel, Microsoft Office Professional Plus 2016), pilot-tested it, and refined it accordingly.
Two authors (CTJ, AN) independently extracted data on design (eg, origin, setting), participants (eg, medical condition, age, sex, race), interventions (eg, exercise type, components, duration), and serious and non-serious adverse events using the developed data extraction sheet. Disagreements were resolved by discussion between the two review authors; if agreement could not be reached, a third author (CBJ or HL) was included.
Frequency of exercise was defined as the number of exercise days per week. The maximum number of sessions per week was therefore defined as seven, regardless of how many times per day an exercise programme was performed. This was done to avoid an overestimation of the number of sessions.
Whether adverse events were mentioned in the primary studies or not was registered as yes or no. The number of adverse events was registered separately for intervention and control groups, and we distinguished between serious and non-serious adverse events. Furthermore, the number of drop-outs was registered separately for the intervention and control groups.
The different health states included in the primary studies were categorised into 16 subgroups based on medical condition. Table 1 shows how the different health states were grouped together. Recruitment areas were categorised into three groups: hospital (inpatient), nursing home (resident) and outpatient locations. Types of exercise were sorted into four groups: Strengthening exercise, Aerobic capacity exercise, Neuromuscular exercise and any combinations of the three.
Health states evaluated in the included studies subgrouped under the same condition
Risk of bias in individual studies
When the primary studies were identified, four authors (SNS, TI, CLG, AN) independently extracted the risk of bias evaluation from the Cochrane reviews including the primary studies. Risk of bias had been evaluated using different tools across the different Cochrane reviews, and where the evaluation had not used the Cochrane Risk of Bias Tool,21 we re-scored it using that tool, including the following seven domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting and other biases. ‘High risk’ of bias was defined as at least one out of seven domains with high risk of bias. ‘Unclear’ was defined as at least two domains with unclear risk of bias and no high risk of bias. ‘Low risk’ of bias was defined if no domain was scored as high risk of bias, and only one scored as unclear risk of bias.
Statistical analysis
The primary outcome was the RR of serious and non-serious adverse events. Drop-out was analysed as a reference for adverse events. The RR of serious and non-serious adverse events was estimated separately as the rate of adverse events in the intervention group divided by the rate of adverse events in the control group.
A random effects meta-analysis was applied to estimate the overall RR of adverse events in the exercise therapy groups compared with controls.22 For studies that reported no adverse events in either the exercise or control groups, the no adverse event finding was adjusted using Battaglia’s code, ie approximately half an adverse event was added to both exercise and control groups. Heterogeneity was tested using the Cochran Q-test and was calculated as the I2 statistic23 measuring the proportion of variation (ie, inconsistency) in the combined estimates due to between-study variance.24 An I2 value of 0% indicates no inconsistency between the results of individual trials, and an I2 value of 100% indicates maximal inconsistency. Covariates were analysed using a meta-regression analysis.25 26 A relevant study-level covariate is defined as one able to decrease between-study variance (Tau-squared).26 In addition, the number needed to treat for an additional harmful outcome (NNTH) was estimated to express the number of participants treated with exercise therapy that was associated with one additional adverse event.
Subgroup analyses
Covariates were investigated in a stratified meta-analysis when categorical (ie, exercise type, recruitment area etc.), and in meta-regression-analyses when continuous (ie, duration and frequency). The RR of non-serious adverse events in patient groups based on type of exercise, medical condition, whether supervised or not and whether delivered to groups or individuals, was estimated, and differences between subgroups were evaluated in meta-regression analyses. Furthermore, the impact on the RR of adverse events of duration (in weeks) and frequency (exercise days per week) of the intervention was analysed using a meta-regression analysis.
Results
Study selection
The search in the Cochrane Library yielded 645 systematic reviews (see figure 1). Of these, 493 were excluded as they were not investigating the effect of an exercise intervention. From the remaining 180, 3823 primary studies were identified.
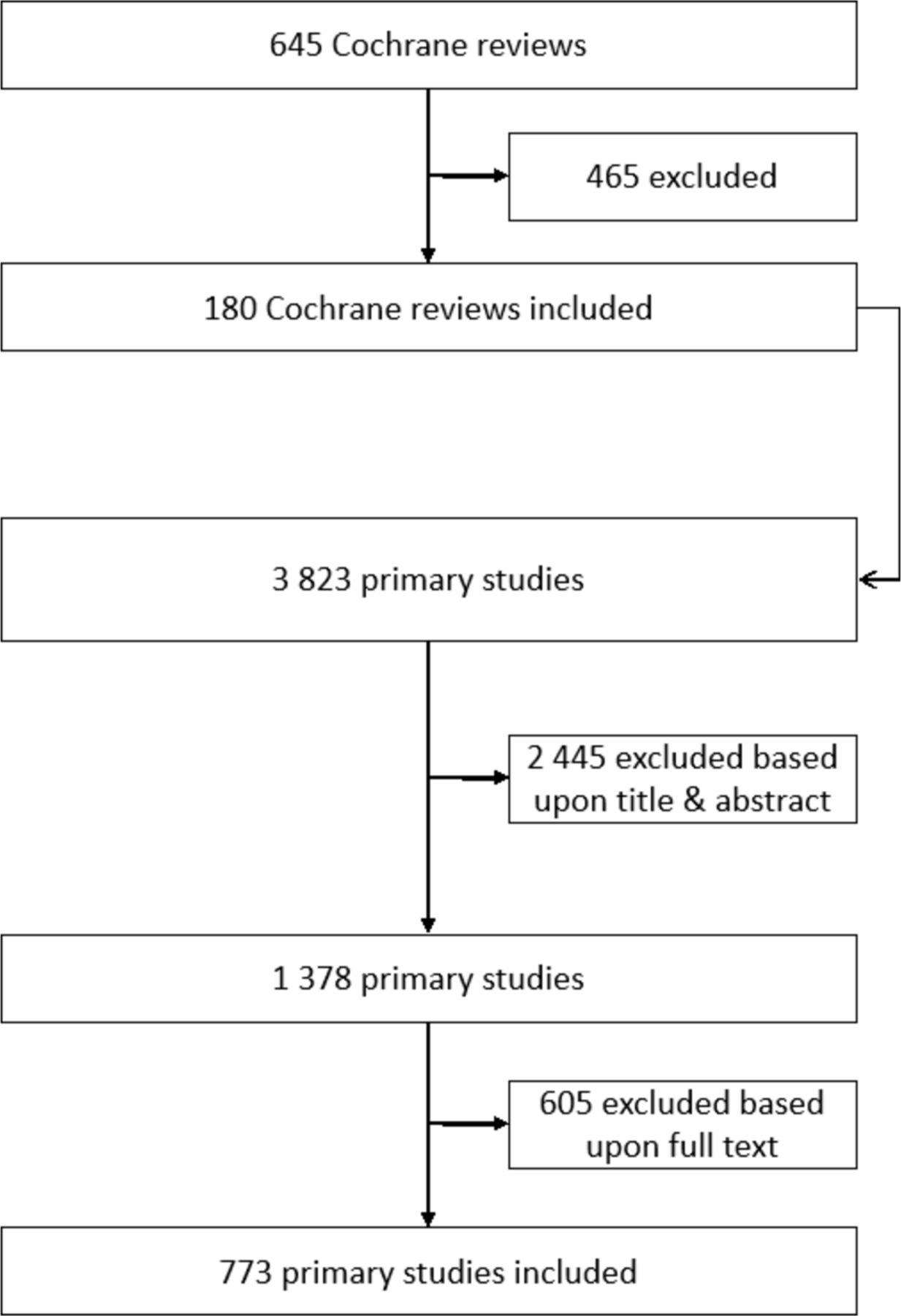
Preferred Reporting Items for Systematic Review and Meta-Analysis flow diagram of the selection process.
Based on title and abstract evaluation, 2445 were excluded (mainly due to duplicates, that is, studies included in more than one review, multimodal interventions and no non-exercise control group), and the remaining 1378 were evaluated in full text. Of these, 161 were excluded due to exercise included in the control group, 139 for reporting results from the same population in another study, 79 for an additional therapy being delivered together with exercise or less than 50% of the intervention being exercise, 69 for the intervention involving vibration therapy, bladder training or other interventions not meeting the inclusion criteria for interventions. Further, 59 were excluded as they were reported in a language other than English, 45 because the full text was not accessible. Lastly, 8 were excluded because data were not extractable, 5 because the thesis was not available and 40 for other reasons. Thus, in total, 773 primary studies (involving 76 429 participants) were included. Of these, 378 primary studies (including 38 368 participants) reported serious adverse events and 375 studies (38 517 participants) reported non-serious adverse events. As there was no increase in RR of serious adverse events (see below), only characteristics and results from studies reporting non-serious adverse events are presented. Only 49% of all primary studies reported non-serious adverse events (375 out of 773 included studies).
Study characteristics
Types of participants
Table 2 presents an overview of the included 375 primary studies that reported non-serious adverse events. Most participants (82%) were recruited as outpatients. Table 3 presents an overview of the number of studies and number of participants for each subgroup. Older adults represent the largest group (26% 11 467 participants), followed by patients with cardiovascular diseases (14% and 5835 participants) and patients with musculoskeletal diseases (11% and 5077 participants).
Characteristics of included studies registering non-serious adverse events, that is, 375 primary studies out of 773 included studies, encompassing 38 517 participants out of 76 429 participants
Number of primary studies and participants for each condition subgroup for the 375 primary studies that registered adverse events, comprising 38 517 participants
Types of intervention
Most often, exercise intervention was performed as a combination of strengthening, aerobic and neuromuscular exercise (47%). The average exercise programme lasted 20 weeks (mean 20.48 weeks (SD 20.13; range from 1.4 to 156)), and the average number of exercise days per week was three (mean 3.42 (SD 1.60; range from 0.5 to 7)). Most of the exercise programmes (53%) were performed as supervised exercise therapy and took place as individual exercise (58%).
Types of comparison
The most frequent comparison groups included a large variety of non-exercising groups such as usual care, education and nutraceuticals.
Types of adverse events
Very few studies used a systematic approach to assess adverse events. However, the most frequent non-serious adverse events reported were pain, fatigue, bursitis, low back pain, oedema. In both exercise and control groups, the most frequent serious adverse events were death, hospitalisation, cerebrovascular accident, stroke and hip fracture.
Risk of bias within studies
Of the 375 studies reporting non-serious adverse events, the risk of bias was found to be low in 58 studies, an unclear risk of bias was found in 51 studies and 266 studies had a high risk of bias. Insufficient blinding of participants, study personnel and outcome assessors was the most frequent issue, as expected in exercise trials, followed by lack of allocation concealment and inadequate handling of missing data.
Synthesis of results
The RR of obtaining a serious adverse event participating in an exercise intervention compared with a non-exercise control was estimated to be 0.96 (95%CI 0.90 to 1.02, I2: 0.0%) and for a non-serious adverse event 1.19 (95%CI 1.09 to 1.30, I2: 0.0%). Thus, the NNTH for a non-serious adverse event was 6 [95%CI 4 to 11), meaning that for every six people participating in an exercise intervention, one non-serious adverse event was reported. Figure 2 presents the RR of a non-serious adverse event divided between the different characteristics of the included primary studies. With the number of drop-outs classified as a proxy for adverse events, the RR of drop-outs was estimated to be 1.08 (95%CI 1.01 to 1.14, I2: 20.4%).

Forest plot: Relative Risk (RR) of non-serious Adverse Events (AE) subgrouped by the different characteristics of primary studies.
Subgroup analysis on risk of adverse events of different intervention characteristics
The RR of adverse events associated with participating in an exercise intervention in outpatients was found to be 1.29 (95%CI 1.15 to 1.45) (figure 2), and the meta-regression analysis explained 40% of the variance, indicating larger risk of non-serious adverse events in outpatients compared with nursing home and hospitalised locations. The RR of adverse events associated with participating in a strengthening exercise intervention was estimated to be 1.42 (95%CI 1.11 to 1.82), (figure 2), but no differences between exercise types were found in a meta-regression analysis. The RR of a non-serious adverse event associated with participating in a supervised exercise intervention was found to be 1.17 (95%CI 1.05 to 1.30), but no differences were found for the risk of adverse events between supervised and un-supervised or between performing exercise in groups and individually (figure 2). The RR of a non-serious adverse event in low risk of bias studies was found to be 1.49 (95%CI 1.16 to 1.91). A trend towards higher RR of non-serious adverse events in the low risk of bias trials was interpreted as the results of the meta-regression analysis explaining all the observed heterogeneity.

Forest plot: relative risks (RR) of non-serious adverse events (AE) in different patient groups.
Subgroup analysis on risk of non-serious adverse events in different patient groups
A subgroup analysis of the 16 different patient groups indicated that participants with back pain, older adults, healthy people and patients with musculoskeletal and osteoporotic complaints had an increased risk of non-serious adverse events when participating in exercise interventions (figure 3).
Dose-Response relationship
There was no significant increase in the RR of adverse events related to the duration of exercise (weeks, slope: 1.00, 95% CI 1.00 to 1.001, I2: 0.0%) (figure 4) and no significant effect of the number of sessions per week (slope: 1.00, 95% CI 0.92 to 1.04, I2: 0.0%). This is supported by the meta-regression analysis not reducing the between-study variance in any of these analyses. Analysis of the impact of intensity was not performed due to poor reporting of the intensity in the included studies.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The relationship between non-serious adverse events and the duration of the exercise intervention in weeks.
Discussion
The main finding of our systematic review and meta-analysis was that while there was no increase in the risk of a serious adverse event when participating in an exercise intervention compared with a non-exercise control (RR=0.96 (95%CI 0.9 to 1.02, I2: 0.0%); there was an increase in the risk of a non-serious adverse event of 19% (RR=1.19 (95%CI 1.09 to 1.30, I2: 0.0%). Thus, the NNTH for a non-serious adverse event was 6 [95%CI 4 to 11), meaning that for every six people who participated in an exercise intervention, one additional non-serious adverse event occurred in the exercise group. However, as there was a trend towards a higher risk of non-serious adverse events in studies with a low risk of bias compared with unclear and high risk of bias, this may underestimate the risk of non-serious adverse events.
To our knowledge, no previous studies have systematically investigated adverse events in exercise therapy studies in different patient groups, and the impact of type of exercise, duration of exercise, settings, dose of exercise, whether the exercise is supervised or not and performed in groups or individually. However, a summary of previous reviews evaluating the effect of exercise therapy identified no indication of harmful effects of exercise or adverse events related to exercise therapy.1 Nevertheless, the authors of previous studies stated that the identified systematic reviews provided little information on the safety aspects of exercise therapy, probably due to inadequate reporting of adverse effects.1
Three systematic reviews specifically evaluated adverse events, one in Tai Chi, one for participants with stroke, and one for participants with spinal cord injury.27–29 Two systematic reviews stated that adverse events might be under-reported.27 28 Liu and Latham reported that 44% of studies had no comments at all on adverse events,27 and Allen et al reported that 72% did not report monitoring of adverse events.28 The kind of adverse events reported in all four reviews could be characterised as non-serious adverse events.1 27–29 However, a recent preliminary cohort study of exercise therapy for patients with chronic obstructive pulmonary disease showed an increased mortality in the high-intensity exercise group compared with the regular intensity group.30 Even though we found no significant increase in serious adverse events, this example indicates that the possibility could not be fully ruled out.
As there was a 19% increased risk for non-serious adverse events, health professionals should weigh the risk of non-serious adverse events with the benefits of exercise therapy for different patient groups. Although only 49% of the primary studies reported adverse events, the large number of studies (375) and participants (38 517) in the analysis of this systematic review may indicate that the identified estimate of increased risk may not change.
Limitations and strengths
We begin by discussing four limitations. First, we did not extract information about how the adverse events were discovered or registered in the primary studies. However, it seems that this information is infrequently reported, that is, the rule of thumb is something along the lines of ‘patients complained about …’ or ‘patients reported …’. In other words, a systematic and standardised collection of information about adverse events is rare.
Second, it was not possible to evaluate the adverse effect of exercise per se, but only adverse events taking place during the observation period of the exercise study. As Chou et al point out ‘methods for classifying adverse events as ‘treatment-related’ are largely subjective, with unknown validity, and such data may be particularly unreliable’.21
Third, five of the 16 patient groups (Back Pain, Older adults, Healthy, Musculoskeletal and Osteoporotic) had an increased risk of non-serious adverse events. Participants with osteoporotic pain show a significant increase in RR, but this was based on six studies with a total of 483 participants, so the results should be interpreted with caution.
Lastly, the primary studies used in this systematic review were RCTs identified from the Cochrane Database of Systematic Reviews. Using RCTs to evaluate harm may introduce bias in the estimation of adverse events or harm.21 One reason is because most of the studies lacked pre-specified hypotheses for harm.21 29 In the current study, only 49% of the identified RCTs reported non-serious adverse events, and as very few had pre-specified hypotheses, they lacked indicators for adverse events. Another reason is that, as adverse events occur infrequently, accurate estimation of the frequency of these events requires a large number of participants and a sufficiently long follow-up period.21 30 A further reason is that many RCTs are designed to be explanatory (efficacy studies), that is, the setting and the population are carefully selected to evaluate the intervention in an ‘ideal’ context. Thus, the participants who are more susceptible to adverse events are often under-represented in these trials.
A major limitation of this review is that only 49% of the primary studies reported adverse events. Furthermore, the original studies were identified through published Cochrane reviews, and we may therefore have missed some relevant newer studies not yet included in a Cochrane review. Restricting the search to reviews published by Cochrane may have reduced the number of eligible studies for inclusion. However, as the number of included studies was very large, and as all analyses showed very low or no heterogeneity, it is unlikely that including non-Cochrane reviews will change the estimates substantially.
Lastly, even though the study by Schaadt et al 30 indicated a need to evaluate the relationship between intensity and adverse events, the way exercise therapy was reported in the included trials did not allow that relationship to be evaluated.
The major strength of this systematic review was that it included 375 primary exercise studies and 38 517 participants. This made it possible to perform subgroup analyses and create a strong basis for a very robust answer to our research question.
Conclusion
Participating in an exercise intervention increased the risk of non-serious adverse events by 19%, but not serious adverse events, and exercise may therefore be recommended as a relatively safe intervention.
Implications for practice
There is no increased risk of serious adverse events when participating in exercise interventions relative to controls, however there is a 19% increased risk of non-serious adverse events, corresponding to an additional non-serious adverse event for every six participants in an exercise intervention. Exercise therapy can therefore be recommended as a relatively safe intervention. However, clinicians should take non-serious adverse events into account when planning an exercise intervention.
Implications for research
As 51% of all primary studies did not report adverse events, there is a need to systematically monitor adverse events in all future exercise therapy studies. This could require an international consensus on what to look for, when to report an adverse event, and how to classify it.
What is already known?
According to the Consolidated Standards of Reporting Trials, all important adverse events in each intervention group should be reported. Thus, even though adverse events resulting from exercise interventions are expected to be less frequent and less serious compared with pharmaceutical or surgical interventions, it is important to be aware of the severity, type and frequency of such adverse events. So far, no systematic review has evaluated any of these aspects of adverse events in exercise therapy.
What are the new findings?
There was a small increase in relative risk of non-serious adverse events during exercise therapy across different patient groups. Thus, this study supports the general assumption that exercise therapy is a relatively safe intervention.
References
Footnotes
Contributors HL, AN, TI, SNS and CLG conceived the research. HL, CBJ, AN, TI, SNS and CLG participated in pilot testing the screening and data abstraction forms, helped conceptualise the analysis and interpreted the data. HL and CBJ wrote the first draft of the manuscript. HL coordinated the study. HL, CBJ, AN, TI, SNS, CTJ and CLG screened citations and full texts, resolved discrepancies. HL and CBJ verified data accuracy and analysis and prepared the tables and figures. HL, CBJ, AN, TI, SNS, CTJ and CLG reviewed the manuscript. CBJ analysed and HL, AN, TI, SNS, CTJ and CLG helped interpret the data and reviewed the manuscript. AN and CTJ carried out risk of bias assessment. HL, CBJ, AN, TI, SNS and CLG provided clinical content expertise, verified categorisation of patient population health condition for analysis. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.