Article Text

Abstract
Background Stress fractures are common overuse injuries with up to 95% occurring in the lower extremities. Among runners, stress fractures account for 15–20% of all musculoskeletal injuries.
Purpose We systematically reviewed and critiqued the evidence regarding risk factors associated with increased risk of lower extremity stress fractures in runners.
Study design Systematic review.
Methods A systematic, computerised literature search of Medline, Embase, PubMed, SPORTDiscus, and CINAHL databases (from database inception through 9 January 2014) using keywords related to risk factors and stress fractures. This systematic review with meta-analysis utilised the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines for the search and reporting phases of the study. Inverse variance meta-analyses, using a random effects model were used to summarise ORs.
Results 8 articles met the inclusion criteria; 7 were considered low risk. 4 articles qualified for meta-analysis. Results of the meta-analysis identified previous history of stress fracture and female sex as the primary risk factors for future stress fracture with a pooled OR of 4.99 (95% CI 2.91 to 8.56; p<0.001; I2=0%) and 2.31 (95% CI 1.24 to 4.29; p<0.01; I2=0%), respectively.
Conclusions Currently, only previous history of stress fracture and female sex are risk factors for lower extremity stress fractures strongly supported by the data.
- Risk factor
- Running
- Lowever extremity
- Stress fracture
Statistics from Altmetric.com
Introduction
Stress fractures are among the most common overuse injuries reported by active individuals, with up to 95% occurring in the lower extremities.1 Runners, in particular, are at increased risk with stress fractures accounting for 15–20% of all musculoskeletal-related injuries.2 Given the many benefits of running and the widespread participation combined with the high incidence of stress fractures, preventing injury among runners has major implications not only for competitive athletes but also for public health.3
While it often presumed that risk factors for stress fractures in runners are well known, many recommendations are derived from studies involving military personnel rather than recreational and competitive runners.4 Additionally, a number of recommendations for prevention of stress fractures in runners are based on cross-sectional studies5 or theory/opinion. The objective of this study was to conduct a systematic review and meta-analysis of the literature identifying risk factors associated with increased risk of lower extremity stress fractures specifically in runners.
Methods
This systematic review was conducted and reported according to the protocol outlined by Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) using a research question developed by PICOS methodology. The PRISMA checklist for this study is available as an online supplementary file. (PICOS is an acronym for population (eg, runners), intervention (eg, risk factors associated with stress fracture), comparison (eg, control group), outcome (eg, OR), and study design (eg, cohort)).
Identification and selection of the literature
A systematic review was performed to identify risk factors associated with stress fractures in runners. For the purposes of this study, runners are defined as cross-country, track and field, triathlon, duathlon, and recreational running athletes. Articles were identified by searching various databases, including Medline, Embase, PubMed, SPORTDiscus, and CINAHL from database inception through 9 January 2014. Search terms included (‘stress fracture’ OR ‘fatigue fracture’ OR ‘insufficiency fracture’ OR ‘march fracture’ OR ‘overuse fracture’ OR ‘stress lesions’ or ‘stress injur’ OR ‘stress reaction’ OR ‘bone stress’ OR ‘bone strain’ OR ‘repetitive stress injur’) AND (‘risk’ OR ‘cohort studies’ OR ‘mortality’). A hand search was also conducted which included the authors’ private collections and the searching of previous related systematic reviews.
Selection criteria
To qualify for inclusion, studies had to (1) include original data, (2) identify a criterion standard for diagnosis of stress fracture, (3) include an analytical component (ie, the study examined the relationship between risk factor and stress fracture), or sufficient data for these to be calculated, (4) be derived from a prospective cohort of subjects, (5) include lower-extremity stress fractures, (6) be available in full text and (7) written in the English language. Studies were excluded if they did not meet the above inclusion criteria, if they were not specific to the running population, or they failed to include a comparison group of non-injured running athletes.
To identify relevant articles, titles and abstracts of all database-captured citations were independently screened by two reviewers (AAW and JMS) applying the a priori inclusion/exclusion criteria. Full text articles were retrieved if the abstract provided insufficient information to establish eligibility, or if the article passed the first eligibility screening. In situations where disagreement concerning whether to include an article occurred, the two authors discussed the issues and came to a consensus. All criteria were again independently applied by the same two reviewers to the full text of the articles that passed the first eligibility screening. In case of disagreement, a consensus method was used to discuss and solve the disagreement. In the event that agreement could not be reached, a third author (KRF) served as the deciding vote.
Quality assessment
The two reviewers (AAW and JMS) independently assessed the methodological quality of each study using a risk of bias tool originally derived for measurement of prevalence studies (table 1).6 The tool includes 10 items to evaluate internal (six items) and external (four items) validity, measurement bias, selection bias and bias related to the analysis (high or low risk), and provides a summary risk of bias assessment based upon the 10 items (low, moderate or high). Item nine, which from the initial risk of bias tool originally dealt with prevalence, was modified to represent the longitudinal nature of risk factor assessment, by characterising studies as high risk if they used a follow-up period of 12 months or shorter. Items were then qualitatively summarised and rated based on an overall assessment of risk bias defined as low (0–3 high-risk items), moderate (4–5 high-risk items), or high risk (6 or greater high-risk items).7 Disagreements among the reviewers were discussed during a consensus meeting.
Methodological quality assessment scores of included articles
Data extraction
Two reviewers (KRF, JBT) independently extracted information and data regarding study population, study design, patient demographics, reference standard, risk factors and strength of association statistics (eg, OR, adjusted rate ratio (AOR), risk ratio (RR), HR) associated with the risk factors. Reported risk factors only identified by mean differences between groups (ie, p values) were not included.
Statistical analysis
For studies that provided an OR or RR, calculations were evaluated for accuracy and reported in the analysis. If ORs or RR were not provided, but summary injury data were provided, ratios were calculated by the authors (KRF, JBT) of the current study.8
Exploratory meta-analyses were conducted on each risk factor that was described in three or more studies and for which ORs were reported or able to be calculated from included data. Inverse variance meta-analyses, using a random effects model were performed using Comprehensive Meta-Analysis Software (V.2.2, Biostat, Englewood, New Jersey, USA). CIs of 95% were calculated, with p<0.05, indicating that the true ORs were different than 1.0. Heterogeneity was assessed using an I2 statistic, with values <25% deemed as low.9
Results
Initially, the search yielded 6957 citations (Medline 1483, Embase 594, PubMed 779, SportDiscus 1700, Cinahl 2401). Of these, 3129 duplicates were deleted, resulting in 3832 titles with abstracts for review. After the first screening, the full texts of 69 potentially eligible citations were retrieved. Following a consensus meeting, a total of eight studies,10–16 reporting on four independent cohorts, were included in the review (figure 1).

Flow diagram of the literature screening process.
The results of the quality assessment are shown in table 1. Of the eight included studies, seven10–14 ,16 were classified as low risk, and one study15 was classified as moderate risk. Most methodological shortcomings concerned the following items: the study's target population was clearly not representative of the national population, a random sample was not used, data was collected via a proxy (eg, questionnaire) as opposed to directly from the subject, and failure to calculate appropriate statistics (eg, OR).
A summary of the individual study characteristics is presented in the online supplementary table. Three studies13–15 investigated nutritional status/dietary habits, four studies10 ,13 ,15 ,17 investigated use of oral contraceptives, two studies investigated training regimen;10 ,15 three studies12 ,13 ,15 investigated history of previous fractures, three studies12 ,15 ,16 investigated sex, three studies10 ,13 ,15 investigated menstrual status, and three studies11 ,13 ,15 investigated body composition and bone density. The number of patients with follow-up ranged from 95 12 to 701.15 The mean follow-up duration ranged from 11.4 months 15 to 3616 months. A positive stress fracture diagnosis was based on four different criteria: conventional radiograph, MRI, nuclear scintigraphy, or CT.
Risk factors and associations with stress fracture
Extrinsic variables
Nutrition/dietary habits
Three studies reported on dietary intake and eating behaviours with conflicting findings.13–15 Nieves14 reported higher consumption of calcium (HR 0.53, 95% CI 0.29 to 0.97), servings of dairy product per day (HR 0.60, 95% CI 0.40 to 0.89), skim milk (HR 0.38, 95% CI 0.16 to 0.90), total milk consumption (HR 0.43, 95% CI 0.20 to 0.89), and high dairy/low fat dietary patterns (HR 0.32, 95% CI 0.10 to 0.96) were related to a significantly reduced rate of stress fracture (see online supplementary table). Kelsey et al13 found that lower average daily servings of dairy products (per one serving decrease) were related to an increased rate of stress fracture (RR 1.41, 95% CI 1.01 to 1.96). Interestingly, when reported as calcium intake per 100 mg decrease, Kelsey et al13 found no significant association between calcium intake and decreased or increased rate of stress fractures. Tenforde et al15 found that female athletes who used a calcium supplement were at 3 times higher risk of stress fracture (OR 3.36, 95% CI 1.4 to 7.9). The same was not true for male athletes (OR 0.90, 95% CI 0.19 to 4.28). Limitations regarding study protocol were questioned as athletes were asked late in the study regarding calcium intake and calcium supplementation was also strongly correlated to previous history of stress fracture. Therefore, injured athletes may have been prescribed calcium supplementation as part of their treatment plan versus primary prevention. History of diagnosed eating disorder (anorexia nervosa or bulimia nervosa) was reported in a single study15 with a significant association with increased risk of stress fracture (OR 259.8, 95% CI 30.8 to 2193.40).
Use of oral contraceptives
Four studies10 ,13 ,15 ,17 reported on the use of contraceptives among female athletes. In all four studies, use or non-use of an oral contraceptive was not significantly related to a reduced or increased rate of stress fracture with ORs ranging from 0.55 to 2.22 (see online supplementary table).
Training regimen
Two studies10 ,15 reported on training regimen as a risk factor. Tenforde et al15 defined training regimen as the average weekly running distance in the past year. Athletes running >32 km/week were found to be at 2 times higher risk of injury (OR 2.40; 95% CI 1.20 to 4.82). Females, in particular, running >32 km/week were at 3 times increased risk of stress fracture as compared with those running <32 km/week (OR 3.08, 95% CI 1.31 to 7.20). Bennell et al10 found no significant associations between premenarcheal training and increased risk of stress fracture.
Intrinsic variables
Previous history of stress fracture
Three studies12 ,13 ,15reported on previous history of stress fracture and its association with increased risk of future stress fracture. All three studies had similar findings in that athletes with a previous history of fracture were at increased risk of developing a future stress fracture with ORs ranging from 2.90 to 6.36. An exploratory meta-analysis confirmed the individual study results with runners with a previous history of stress fracture at 5 times higher risk of a future stress fracture (figure 2, table 2; OR 4.99; 95% CI 2.91 to 8.56; p<0.001; I2=0%).
Pooled estimates from meta-analysis

Pooled OR with 95% CI for previous history of stress fracture. Kelsey et al;13 *OR calculated from adjusted rate ratio.
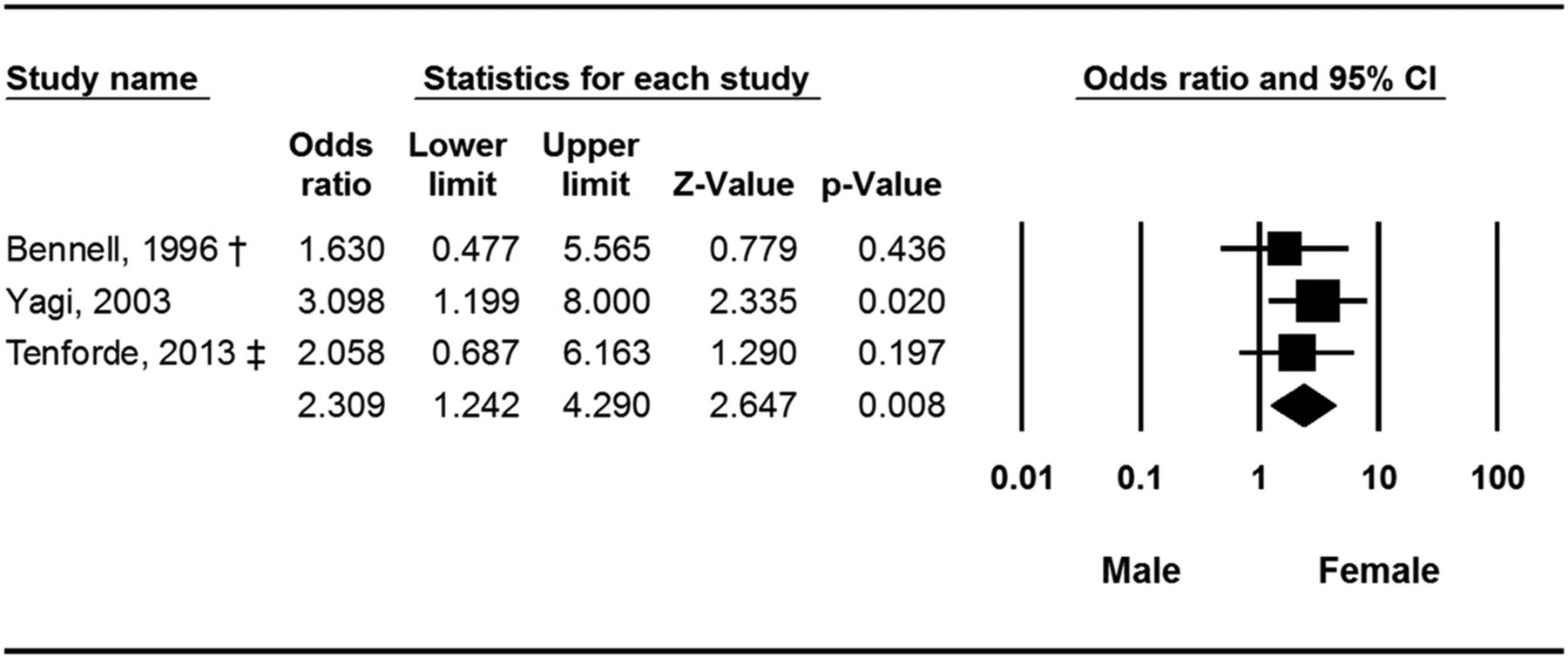
Sex
Three studies reported on sex and its association with increased risk of stress fracture with conflicting findings.12 ,15 ,16 Yagi et al16 found an increased risk of stress fractures among females (OR 3.10, 95% CI 1.20 to 8.00). Specifically, 5% of males compared to 15% of females sustained a stress fracture during the prospective study of high school running teams. By contrast, Bennell et al12 (OR 1.08, 95% CI 0.40 to 2.91) and Tenforde et al15 (OR 1.35, 95% CI 0.65 to 2.82) found no significant association between sex and increased risk of stress fracture. An exploratory meta-analysis with study subgroups focused specifically on distance runners was performed based on the increased risk of stress fracture in females compared with males (figure 3, table 2). Females were at 2.3 times higher risk compared with males (figure 3; OR 2.31; 95% CI 1.24 to 4.29; p=0.008; I2=0%).

{kind=link}
{kind=link}
{kind=link}
Menstrual characteristics
Three studies10 ,13 ,15 reported on menstrual characteristics for female athletes defined in terms of age at menarche, amenorrhoeic, or oligomennorrhoeic with conflicting findings. Bennell et al10 found no significant association between female athletes currently defined as oligomennorrhoeic or amenorrhoeic and increased risk of stress fracture (OR 3.43, 95% CI 0.62 to 18.88). Past history of oligomennorhoea (OR 1.32, 95% CI 0.29 to 5.99) or amenorrhoea (OR 2.60, 95% CI 0.62 to 10.96) was also found not to be significantly associated with increased risk of stress fracture.10 Kelsey et al13 also reported no association between history of menstrual irregularity and increased risk of stress fracture (RR 1.90, 95% CI 0.66 to 5.51). By contrast, Tenforde et al15 found that female athletes with later age of menarche (≥15 years) and currently amenorrhoeic were at five times (OR 5.30, 95% CI 2.11 to 13.34) and nearly three times (OR 2.73, 95% CI 1.16 to 6.4) increased risk of stress fractures, respectively.
Body composition and bone density
Two studies11 ,13 reported on varying aspects of bone mineral content defined as total bone mineral content, bone mineral density, and whole-body skeletal area and their association with increased risk of stress fracture. Neither of these studies provided enough information to calculate an OR. Kelsey et al13 found significantly lower values for whole-body bone mineral content (RR 1.79, 95% CI 1.02 to 3.13), spine bone mineral density (RR 1.89, 95% CI 1.04 to 3.45) and whole body skeletal area (RR 1.89, 95% CI 1.06 to 3.33) in women who developed stress fractures (see online supplementary table). Kelsey et al13 also reported a significant association between lean body mass (per kg decrease) and increased risk of stress fracture (OR 1.14, 95% CI 1.01 to 1.28). Tenforde et al15 found a significant association between BMI<19 and increased risk of stress fracture (OR 2.76, 95% CI 1.18 to 6.46).
Discussion
Our systematic review aimed to identify risk factors associated with increased risk of lower extremity stress fractures in the running population. In this review of eight studies, there was a striking lack of conclusive evidence for any risk factor, but with two exceptions: previous history of stress fracture and female sex-predicted increased risk of future stress fracture.
Although history of a previous stress fracture is an intrinsic, non-modifiable risk factor in terms of prevention, this finding stresses the importance of identification of modifiable risk factors responsible for the initial injury and subsequent effective rehabilitation to reduce risk of future stress fracture. The deficient evidence highlighted in this systematic review identifies the need for further research.17
Why is the evidence scant?
It has previously been acknowledged that prospective studies examining stress fractures are difficult to perform given the large populations that must be followed for long time periods, and thus, retrospective studies are often pursued, even though they are unable to establish a causal relationship.18 Additionally, one could argue that the lack of available evidence may be secondary to the complex nature of stress fracture research in the running population. One of the complications in stress fracture research in runners is the interdependence of variables and how individual differences may influence response to confounding factors. Tenforde et al's15 findings, in which some apparently significant risk factors (eg, training volume, body mass, racing performance) became non-significant when multivariate analysis was conducted, serves as a prime example of the interdependent nature of risk factors for stress fractures. While many of these factors were examined in various studies that met the inclusion criteria, they were often not examined synchronously. The individual nature of stress fracture risk, and thus, the need to identify risk factors to prevent them, is also clear when one considers athletes performing nearly identical training regimens within a team. While some athletes remain injury free, others develop soft tissue injuries (eg, tendinopathy), whereas other develop stress fractures at different sites. Finally, there is emerging evidence that various single nucleotide polymorphisms may be associated with stress fractures in athletes,19 however, considerable research is necessary before more definitive conclusions can be made regarding genetic risks for stress fractures in runners.
Bone mineral density and calcium as risk factors
Mechanical loading is associated with increased bone mineral density,20 thus, runners with greater training volumes should, theoretically, have higher bone mineral density. Although ORs could not computed from mean data, bone density in runners with a history of stress fracture was lower than those without stress fractures, yet greater than that of non-athletes.10 This suggests that healthy bone mineral density requirements of active running individuals may be greater than that required by the general public.
This systematic review found conflicting results regarding whether calcium supplementation is associated with increased15 or decreased13 ,14 risk for stress fractures. Though dietary interventions focused on calcium intake are theoretically beneficial to reduce risk of stress fracture in runners, no prospective clinical trial data is available to support this recommendation. A full understanding of dietary risk factors is further complicated by differences in methodology used to assess nutrition, as well as variety and crossover in predictor variables (eg, dairy intake vs calcium intake).
Menstrual dysfunction
Although menstrual dysfunction is commonly cited as a risk factor for stress fractures in athletes, Tenforde et al's15 was the only study identified which described an association between the variables, in that age of menarche and current amenorrhoea were associated with significant increases in risk for stress fracture. Conflicting findings in this realm may relate to fallacies within the traditional ‘female athlete triad’ paradigm.21 ,22 Menstrual dysfunction may be considered simply as one group of signs which occurs secondary to the issue of ‘relative energy deficit in sports (RED-S)’.21 It is possible that female athletes who experience RED-S, and are at elevated risk of stress fracture, have suboptimal menstrual function that is not clinically apparent,21 ,22 and such subclinical issues are not recognised in risk factor studies.
Biomechanical risk factors
Biomechanical factors, including kinetic, kinematic and static alignment variables, are commonly implicated as a risk factor for stress fractures, however, no studies which met the inclusion criteria examined biomechanical factors. One commonly cited study prospectively links biomechanical variables (average and instantaneous vertical loading rate, tibial shock) to stress fractures in competitive female runners, however, it is not a peer-reviewed article, but rather a 2004 research abstract with only five individuals with stress fractures.23 Other studies which have focused on biomechanical ‘predictors’ in runners have chiefly examined biomechanical differences (ie, peak hip adduction, knee rotation, rearfoot eversion angle) in individuals with a previous history of stress fracture,24–27 or have examined biomechanical variables which, theoretically, could lead to stress fracture without prospectively tracking the incidence of injury.28–30 Also noticeable by its absence is the almost complete lack of investigation of the association of biomechanically relevant clinical examination components with stress fracture risk such as arch height, alignment of lower extremity, range of motion, and leg-length inequality.
Military population data should not be translated directly to runners
A wealth of research has been conducted on risk factors associated with stress fractures; however, much of this data comes from studies involving military personnel, with far more sampling populations and considerably larger sample sizes than those specific to runners.4 Studies involving military personnel include smokers and individuals with poor overall physical fitness, both of whom would not be expected in a population of serious runners, yet are significantly associated with stress fractures31 and overall training-related injuries.32 ,33 Military recruits often run <10 miles per week34 and often take 12 weeks to accumulate 40 miles of running,35 whereas runners often perform 40 miles of running at various intensities within 1 week, with some competitive runners exceeding 100 miles per week.36 Additionally, soldiers regularly carry heavy loads37 and use footwear that is not as effective for injury prevention as typically found in running shoes,38 further prohibiting a direct comparison with running athletes. Stress fractures in the military often occur within the first 16 weeks of training,4 but risk factors during this initial acclimation period are not likely applicable to athletes who experience their first stress fracture after years of running. Although military data are commonly extrapolated to the general running population, this is likely inappropriate due to major differences between these populations.
Clinical implications
We found little or conflicting evidence for extrinsic or modifiable risk factors such as training regimen, nutritional status, or biomechanics. Only one study reported on training volume (eg, mileage) associated with increased risk of stress fracture, however, the reported threshold for increased risk was a relatively low volume (32 km/week) in relation to the training regimens many runners undertake.36 ,39 Additionally, running volume itself is not an overall indicator of mechanical stress placed upon the musculoskeletal system. A typical training week may involve a combination of different intensities of running, which place different magnitudes of load on the skeleton. Rapid changes in training volume and intensity are often considered in the development of injuries, though this is difficult to quantify in epidemiological studies.
Thus, future research examining training factors should also consider incorporating a holistic measure, such as training impulse,40 while also seeking to describe the stability of training practices, and reporting injury rates in terms of both time (eg, injuries per week) and volume (eg, injuries per mile). In the absence of methodologically sound high-quality studies which quantify training practices, including volume, intensity and progression, clinicians have little evidence to support the widespread anecdote that higher mileages are associated with increased risk of stress fracture, or the corresponding recommendation that reducing running volume can prevent stress fractures.
Limitations
There is an overall lack of prospective studies focused on stress fractures within the running population, some of which do not include the OR associated with the identified risk factor which is recognised as the proper method for reporting risk factor ratios. Only four independent cohorts made up the eight included studies of this review highlighting the complete lack of research performed in the running population. While three of the cohorts exclusively focused on middle and long distance runners, one cohort included a small sample of track and field athletes from other events.12 Likewise, this systematic review focused on lower extremity stress fractures, but some cohorts included isolated cases of pelvic stress fractures. Studies which examined stress fracture risk in a heterogeneous group of athletes,41 or those which examined general risk factors for all types of running injuries42 were not included, as data reported in these broader studies are not sufficient to determine the risk factors specific to stress fracture in runners.
The available data may be at risk of bias given the considerable variation among the studies with respect to diagnostic criteria (radiograph, nuclear scintigraphy, or MRI), with studies using scintigraphy and MRI potentially reporting a higher incidence. With only a single cohort43 reporting distribution of stress fracture by site and mode of diagnosis, risk factors for stress fractures at specific anatomic sites (eg, fifth metatarsal vs femoral neck) could not be considered, and this may be important if the mechanism of injury varies by location.
In conclusion, our systematic review revealed little evidence for most risk factors for stress fracture within the running population. Previous stress fracture was identified as the greatest risk factor for a stress fracture, however, it is unknown whether this represents new injuries or a previous stress fracture which was not fully healed. Female runners appear to be at greater risk of stress fractures than their male counterparts, and the evidence is inconclusive as to whether this risk may be elevated in females with a history of menstrual dysfunction, low bone mineral density, low calcium intake, and training at higher volumes.
Given the current state of literature, perhaps the most important role for clinicians to reduce the impact of stress fractures are through proper education and time-efficient diagnosis. When patients present to clinicians for pre-participation physicals prior to team sport enrolment or beginning a self-guided training programme, they should be encouraged to beware of the signs of musculoskeletal injuries and to take appropriate measures at the onset of suspected injury.
What are the new findings
Only eight studies, composed of four unique data sets, have specifically examined stress fracture risk factors in runners.
Runners at greatest risk of stress fracture are those with a previous history of stress fracture and females.
There are conflicting findings regarding nutritional factors/dietary history and menstrual status/history as risk factors for stress fractures in runners.
There is no evidence that use of oral contraceptives is related to stress fracture risk in runners.
One study found that running >32 km (>20 miles) per week was a risk factor for stress fracture, however, this relatively low volume of training commonly was exceeded by most runners.
Future research should investigate how running-specific training practices, nutritional factors, biomechanics and other factors influence the risk of stress fractures in runners.
How might it impact on clinical practice in the near future
Female runners with a history of a stress fracture in combination with clinical findings suggestive of a lower extremity stress fracture should warrant early referral for diagnostic imaging.
Surprisingly, there was no evidence to suggest training practices (eg, surface, terrain, volume) is associated with increased risk of stress fracture in runners.
Clinicians are encouraged to use caution in extrapolating risk factor findings from military studies to the running population given the major differences between populations.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors The authors declare that all named authors made substantial contributions to the conception or design of the work; drafting and revising the work, final approval of the manuscript to be published, and are in agreement to be accountable for all aspects of the work.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.