Article Text

Abstract
Exercise can provoke asthma symptoms, such as dyspnoea, in children with asthma. Exercise-induced bronchoconstriction (EIB) is prevalent in 40–90% of children with asthma. Conversely, exercise can improve physical fitness. The purpose of this paper is to provide a systematic review of the literature regarding the effects of exercise training in children with asthma, particularly in relation to: EIB, asthma control, pulmonary function, cardiorespiratory parameters and parameters of underlying pathophysiology. A systematic search in several databases was performed. Controlled trials that undertook a physical training programme in children with asthma (aged 6–18 years) were selected. Twenty-nine studies were included. Training had positive effects on several cardiorespiratory fitness parameters. A few studies demonstrated that training could improve EIB, especially in cases where there was sufficient room for improvement. Peak expiratory flow was the only lung function parameter that could be improved substantially by training. The effects of training on asthma control, airway inflammation and bronchial hyper-responsiveness were barely studied. Owing to the overall beneficial effects of training and the lack of negative effects, it can be concluded that physical exercise is safe and can be recommended in children with asthma. A training programme should have a minimum duration of 3 months, with at least two 60 min training sessions per week, and a training intensity set at the (personalised) ventilatory threshold. Further research is recommended regarding the effects of exercise on underlying pathophysiological mechanisms and asthma control in children with asthma.
- Children and exercise
- Training
- Physical activity promotion in primary care
- Respiratory
- Fitness testing
Statistics from Altmetric.com
Introduction
Asthma is one of the most common chronic diseases in children. Despite a recent decrease in the prevalence of asthma in several Western countries, the worldwide burden of asthma continues to rise.1 ,2 A major trigger for asthma symptoms is exercise, which can lead to exercise-induced bronchoconstriction (EIB). EIB is a condition which usually occurs during, or a few minutes after exercise and is defined as reversible narrowing of the airways, resulting in shortness of breath.3–5 According to the ATS guidelines, EIB is defined by a drop of ≥10% in Forced Expiratory Volume in one second (FEV1) after exertion on an exercise test.6 The prevalence of EIB in children with asthma ranges from 40% to 90%.4 ,7 ,8 There is an ongoing debate about the mechanism whereby physical exercise can provoke EIB in asthma. It is likely to be caused by an increased ventilatory rate as a result of physical exercise.9 According to the osmotic theory, the inhalation of an increased volume of dry air requires humidification, which leads to the loss of water from the respiratory mucosa.10 ,11 This loss of water from the respiratory mucosa causes an increase in osmolarity in the airway surface, which in turn leads to the release of bronchoconstricting mediators from inflammatory cells such as eosinophils and mast cells.10–14 These mediators, for example histamine, prostaglandins and leukotrienes, interact with effector cells (eg, smooth muscle cells) which can cause a transient bronchoconstrictive response.10 ,12 ,15 A second theory, the thermal theory, states that vasoconstriction during exercise due to inhalation of the relatively cold and dry air followed by rapid rewarming after exercise, leads to a rebound vasodilatation.11 This results in a reactive hyperaemia of the bronchial microvasculature and oedema of the airway wall which causes airway obstruction.12 ,15 ,16 Asthma medication, such as short-acting β2-adrenergic receptor agonists, can be used before exercise to prevent or diminish bronchoconstriction during or after exercise.8 Despite this, EIB often leads to avoidance of physical activity in children with asthma.2 ,17
Several studies demonstrated a reduced physical activity level and physical condition in asthmatic children compared with children without asthma.2 ,18–20 In contrast, other studies could not demonstrate such a difference in both physical condition and physical activity level.21 ,22 Several interconnected factors can affect the physical activity participation of asthmatic children, including the asthmatic children's belief that their asthma limits their physical activity level and the concerns and misinterpretation of family members and teachers about asthma and exercise.23 There is increasing evidence that low physical fitness could play a role in the increase of asthma severity while, in contrast, high physical fitness has been related to fewer asthma symptoms.2 ,19 ,24 Therefore, physical training programmes could be important in the treatment of asthmatic children.
The objective of this manuscript is to provide a concise overview of the effects of exercise training on EIB and underlying asthma pathophysiology, physical fitness, lung function, disease control and quality of life in children with asthma. Also, an overview of the most effective components of a training programme for children with asthma is provided.
Methods
Search and review strategy
Databases of PubMed, Cochrane and EMBASE were used to select relevant studies. The following keywords/Mesh terms were used: ‘asthma’ combined with (1) ‘child’ or ‘adolescent’ and (2) ‘exercise’, ‘physical activity’, ‘physical training’, ‘aerobic fitness’, ‘physical conditioning’ or ‘training’ (figure 1). Limitations in the search strategy were set to studies in children (6–18 years) and with the English language. Titles, abstracts and full-text articles of potentially useful studies were independently screened by three researchers. Furthermore, the reference lists of the included articles were scrutinised to detect studies not captured by the electronic search. Searches were carried out on literature published up to, and including, October 2012.

Flow chart of literature search. Summary of evidence search and selection according to the PRISMA flowchart.78
Criteria for considering studies for inclusion in this review
Articles were included in this review which met the following inclusion criteria: a study population of children with asthma with an age range of 6–18 years, a training programme provided, availability of the full text in English and the use of a control group of children with asthma. Data from the included studies were summarised for outcome variables. Outcome measures are described and summarised in tables 1 and 3. Data were not pooled. A quality assessment of the articles was executed according to the Delphi criteria list.25 The quality of the included articles was assessed independently by three researchers.
Characteristics of the included studies
Results
Description of included studies
A total number of 29 studies were included in the review (figure 1). In total, 1045 children with asthma were investigated, with ages ranging from 6 to 18 years. All studies were reported between 1972 and 2010. Fourteen of the studies were conducted in Europe, five in Brazil, four in the USA, two in Taiwan, two in Australia, one in Japan and one in South Africa. The characteristics of the studies with regard to training intervention, sample size, mean age and outcome measures are summarised in table 1.
Characteristics of the exercise programmes
The quality assessment of the articles is summarised in table 2 by using the Delphi list.25 In general, the quality of the studies could be classified as poor to moderate. For example, only 15 of the 29 selected studies performed randomisation. Other quality criteria, such as blinding of patients, are difficult to fulfil in a training intervention, which results in lower scores on the Delphi list. We decided not to exclude any of the selected studies for this review.
Quality of the included studies according to the Delphi list 25
All studies differed on the following characteristics: type of training, intensity, frequency, duration and length of the training programme. Seven studies used a training programme that consisted of swimming training 36 ,39 ,48 ,49 ,50–52 and 16 studies used other aerobic physical training, such as basketball, running, soccer or cycle ergometer training.2 ,3 ,26 ,28 ,29 ,31 ,32–35 ,37 ,40–44 Four studies used swimming training as well as other aerobic physical training 30 ,45–47, while one study used Tai Chi Chuan training 27 and another study used respiratory therapy as a type of training.38 The duration of the programmes ranged from 6 weeks to 20 months, except for the intervention of Dean et al29 which only lasted for 5 days. The frequency of sessions ranged from once a week to seven times a week, with a duration per session ranging from 30 min to 2 h.
Results of the main outcome parameters
As listed in table 3, the most studied outcome parameters include lung function parameters, cardiorespiratory fitness parameters, EIB and quality of life. A summary of the main findings follows. Detailed information about all the outcome parameters is provided in online supplementary table 1 and Web only file 1. In order to distinguish the effective components of a training programme, all training programmes were compared with each other according to the Delphi quality score, training type, number of participants, patient group, intensity, duration and frequency of exercise (tables 1⇑–3). For the three most studied parameters (measurements of bronchoprovocation, lung function and cardiorespiratory parameters) the effective components of training are summarised below.
Summary of the main outcome parameters
Measurements of bronchoprovocation and inflammation
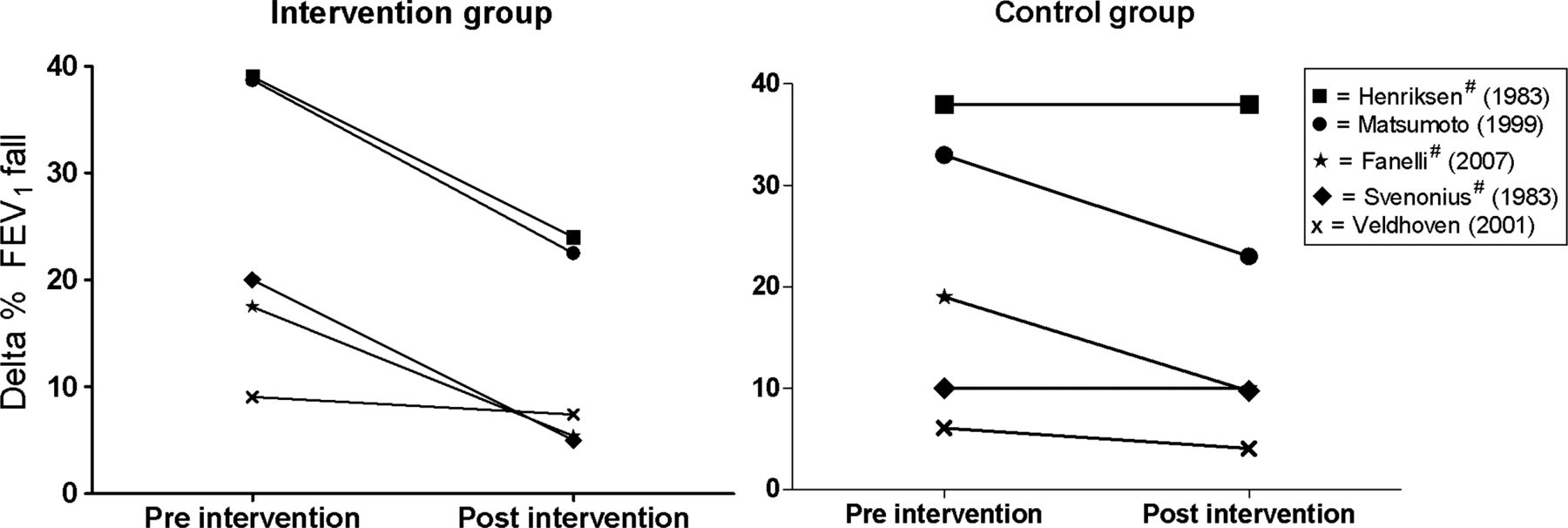
EIB is an important clinical feature of bronchial hyper-responsiveness (BHR) in asthma. Seven studies described the training effects on BHR by using the indirect bronchoprovocation measure for EIB (figure 2).2 ,31 ,34 ,37 ,39 ,41 ,47 EIB was measured by the decrease in FEV1 after running on a treadmill,2 ,31 ,34 ,37 ,47 cycle ergometer test,39 ,41 or swimming ergometer test.39 EIB decreased in all studies, and this decrease was statistically significant between the intervention and control groups in three of seven studies (figure 2).31 ,34 ,47 The patient groups that demonstrated significant improvements in EIB after training consisted mainly of children who were selected for the study specifically because of their EIB problems or severe asthma.31 ,34 ,47 The studies that did not show significant differences in EIB after training included mainly children with moderate asthma with no or minor EIB problems.2 ,37 ,39 ,41

{kind=link}
{kind=link}
Exercise-induced bronchoconstriction (EIB) preintervention and postintervention*, * This figure for illustrative purposes includes studies which measured EIB as the delta of forced expiratory volume (FEV1) fall (in%) preintervention and postintervention. Data have been extracted visually from figures in two studies (Svenonius 1983 and Matsumoto 1999). In the study of Henriksen (1983) intervention group 3 was chosen as intervention group. # Significant difference (p<0.05) between intervention and control group.
Three studies investigated the effects of training on BHR by using direct bronchoprovocation with methacholine and histamine.39 ,40 ,52 The study with the highest number of participants (n=61) was the only one in which a significant decrease was demonstrated in BHR after training.52
EIB can be considered as an indirect measure for airway inflammation. Moreira et al40 investigated the effects of regular exercise on airway inflammation in asthmatic children. In this study no significant change in inflammatory markers was found after 12 weeks of exercise (exhaled nitric oxide (FeNO), blood eosinophil number, serum eosinophil cationic protein (ECP), and serum C reactive protein (CRP)). The authors hypothesised that the balance between the proinflammatory and anti-inflammatory effects of exercise in asthma is null. However, the small sample size might have limited the power to measure the exercise effects on airway inflammation.
In addition to inflammation, oxidative stress is an important component of asthma pathophysiology. Onur et al42 found that markers of oxidative stress in blood serum (malondialdehyde, total nitric oxide (NO)) were reduced in children with asthma after exercise.
Lung function parameters
Twenty-four studies measured the effects of training on lung function parameters (online supplementary Web only file 1).2 ,3 ,27–35 ,38 ,40–44 ,46 ,47–49 ,50–52 At baseline, percentage of predicted lung function ((FEV1 and forced vital capacity (FVC)) was reduced in the vast majority of the studies (online supplementary Web only file 1). FEV1 could be improved in 3 of 20 studies by exercise training,27 ,42 ,44 whereas the FVC improved in only two studies.27 ,42 Peak expiratory flow (PEF) was the main lung function parameter that was improved, albeit mildly, by exercise. Only four of nine studies demonstrated a mild improvement in PEF.27 ,29 ,38 ,50 No significant improvements after training were reported for the other lung function parameters such as FEV1/FVC, functional residual capacity, thoracic gas volume, total lung capacity and maximum expiratory flow rate at 50% of the vital capacity.
This review cannot elucidate any successful aspects of training that are accountable for the improvements in PEF or FEV1 that was demonstrated in some studies.2 ,3 ,34 ,40 ,51
Cardiorespiratory parameters
The effects of training on aerobic capacity and physical condition were tested in 17 studies. The cardiorespiratory parameters were measured with an incremental exercise test on a cycle ergometer or treadmill,2 ,26 ,28 ,30–33 ,37 ,39 ,41 ,43 ,47–49 5/6 minute continuous running test,34 a steady-state submaximal exercise test35 or at resting condition.45 Ten studies determined the training effect on maximal oxygen uptake (VO2max) (online supplementary Web only file 1).2 ,26 ,28 ,32–34 ,37 ,41 ,48 ,49 Six of 10 studies reported that VO2max increased significantly after training. The ventilatory threshold, as well as the maximum oxygen pulse (O2pulsemax) increased in all studies that assessed these parameters.2 ,26 ,48 ,49 Two of six studies revealed a significant increase in maximal minute ventilation (VEmax) in the intervention group.2 ,28 ,33 ,35 ,48 ,49 Maximum heart rate (HRmax),26 ,28 ,33–35 ,48 and maximum power (Wmax) 2 ,26 ,33 ,35 were significantly improved following exercise training in half of the studies. Working capacity, defined as percentage of the individual's maximal aerobic power, improved in one of three studies reporting this parameter.30 ,43 ,47
VO2max was the most commonly studied cardiorespiratory parameter, and is accepted as a gold standard measure of aerobic fitness. Four of the six studies that showed improvements in VO2max after training, had a training intensity at the ventilatory threshold for at least 60 min.26 ,28 ,48 ,49 The studies that did not show improvements in VO2max after training had intensities that were not well described,33 ,35 low,32 or at the ventilatory threshold for only 30 min.41 In addition to a training intensity at the ventilatory threshold the studies that improved VO2max with exercise training, had at least 120 min exercise per week, consisted of at least two training sessions and had a training programme duration of at least 3 months.2 ,26 ,28 ,48 ,49
Asthma control and quality of life
Three studies described the effects of exercise training on quality of life in asthmatic children.3 ,31 ,40 Basaran et al3 and Fanelli et al31 found a significant improvement in quality of life after training, which is in contrast to the study of Moreira et al40 This might be explained by a good quality of life at baseline with little room for improvement in the latter study.
EIB is an important measure of asthma control. Further to EIB, 13 studies used other measures to describe the effects of training on asthma control, such as school absenteeism, symptom score and hospitalisations.2 ,3 ,27 ,29 ,31 ,36–38 ,41 ,43 ,46 ,50 ,51 The limited amount of data point to a decrease in number of asthma attacks and days of wheezing (online supplementary Web only file 1).36 ,38 ,46 Moreover, symptom scores improved in one of three studies reporting this parameter3 ,27 ,51 and medication scores did not improve.3 ,37 ,41
Discussion
The main finding of this systematic review is that exercise training induces clear positive effects on cardiorespiratory fitness parameters, whereas a beneficial effect on lung function is limited to the PEF. It appears that EIB can be improved in children with more frequent and severe EIB problems, although evidence is limited. The limited amount of data regarding quality of life and asthma control point to an increase in quality of life and a decrease in number of asthma attacks and days of wheezing after exercise training. In this review we demonstrate that optimal VO2max improvements in children with asthma can be derived when a training programme consists of training intensities set at the (personalised) ventilatory threshold, for at least 120 min/week divided over two or three sessions with a duration of at least 3 months.2 ,26 ,28 ,48 ,49 In non-asthmatic children, it has been stated previously that training at the ventilatory threshold53 or at an intensity higher than 80% of HRmax54 induces greater and more often significant improvements in aerobic fitness than training below the ventilatory threshold or 80% of HRmax.
This positive effect of exercise training on cardiorespiratory fitness is found across numerous parameters, such as VO2max, O2pulsemax and ventilatory threshold. The improvements in aerobic parameters are a common result of training. The cardiorespiratory improvements are measured both in children who demonstrate improved EIB and in children with unaltered EIB.2 ,31 ,47 Some studies suggest that children with asthma have a reduced physical condition.2 ,18–20 Yet this review shows that children with asthma are able to improve their cardiorespiratory fitness. Improvements in cardiorespiratory fitness are beneficial for the prevention of several comorbidities of childhood asthma, such as obesity and mental disorders.55–57
In our review we show that the degree of EIB improved in all studies after training, although only significantly in three studies. In the studies that did not demonstrate a significant improvement in EIB, it was not reported clearly whether EIB was severe enough to improve, and whether ceiling effects could have hampered the results.2 ,37 ,39 ,41 Two of the three studies that did show improvements in EIB after training had a population consisting of children with recent, frequent complaints of EIB.31 ,47 Therefore, it might be concluded that EIB in children with asthma can be improved by training, particularly when EIB symptoms are more prevalent or severe. Moreover, it can be concluded that as regular physical activity does not have a negative effect on EIB, exercise can be executed safely in most individuals. However, more research is needed on this topic. Optimal control of EIB is most often obtained with inhaled corticosteroids, which has inhibitory effects on airway inflammation.15 To prevent or reverse EIB during exercise, treatment with bronchodilators, such as short-acting or long-acting β2-adrenergic receptor agonists or ipratropium bromide should be used when needed before physical exercise.58 Besides medication, there are also other methods to limit EIB, such as breathing through the nose instead of the mouth, or exercising in a warm, humidified environment.9 ,59 In some asthmatic patients, warm-up exercise before intense physical exercise might also help prevent EIB.60
As pointed out before, cardiorespiratory fitness can be improved with exercise training in children with asthma. Children with improved cardiorespiratory fitness require lower minute ventilation during exercise for a given workload compared with a pretraining situation.61 ,62 As an increased ventilatory rate is probably the cause of EIB, a lower minute ventilation would lead to a less-intense EIB stimulus. However, the extent of improvement in VO2max after training could not explain the degree of improvement in EIB. This is in accordance with the study of Thio et al63 who found no relation between EIB and cardiovascular fitness. Hence, it can be assumed that other factors relating to exercise training may be responsible for the improvement in EIB.
As EIB was improved by exercise training in some of the study populations, there is a need for more understanding of the underlying mechanisms and pathophysiology of EIB. It is most likely that bronchoconstriction is caused by airway drying, which is generated by hyperpnoea during exercise. In addition to inducing bronchoconstriction due to an increased ventilatory rate during physical exercise, exercise also has a bronchodilating effect due to the release of mediators such as prostaglandin E2 and NO. Furthermore, deep inspirations during exercise initiate increased mechanical stretching of the smooth muscle cells which bronchodilate the lower airways. During exercise training there seems to be a balance between the bronchodilating and bronchoconstrictor responses in healthy persons, which prevents EIB during physical exercise.5
There is increasing evidence that a single bout of exercise can induce acute oxidative stress which initiates augmented airway inflammation leading to an increase in EIB.64 ,65 This inflammatory response is reflected by increased levels of CRP, FeNO, serum ECP concentration and BHR to histamine.65 Conversely, it is also suggested that regular exercise might decrease airway inflammation and oxidative stress, as shown by a decrease in inflammatory markers such as sputum eosinophil count, FeNO and oxidative stress after training.40 ,42 ,65–67 Several studies in this review investigated the effects of exercise training on inflammatory markers. Onur et al42 found that markers of oxidative stress were reduced after exercise training, while Wicher et al52 found a decreased BHR after exercise training, which could be attributed to changes in airway inflammation; however, it could also be an effect of relaxation of the smooth muscle cells in the airways. Murine models demonstrated that regular exercise decreases airway inflammation by immune-regulatory mechanisms of the airway epithelium.68 As this review demonstrates that EIB can be slightly optimised after exercise training, more research should focus on inflammatory markers after exercise training. Furthermore, investigations should be conducted into whether the inflammatory response of asthmatics after exercise is different from that of non-asthmatics. Currently, the invasiveness of the techniques available to measure airway inflammation, such as biopsy, hampers this objective. However, there is an increasing interest in the non-invasive assessment of exhaled inflammatory markers, such as FeNO and solutes in exhaled breath condensate. Such feasible techniques can facilitate research on inflammatory responses and exercise in children.
Children with asthma have a lower health-related quality of life compared with healthy children.69 ,70 It is probable that exercise training can improve the quality of life in children with asthma. However, only three studies investigated the effects of exercise training on quality of life; therefore more data are needed.
No studies used validated instruments such as the Asthma Control Questionnaire,71 Childhood Asthma Control Test72 or Asthma Control Test 73 to assess the clinical control of asthma. However, indirect measures of asthma control, including number of asthma attacks and days of wheezing, seemed to be improved by training. As asthma control parameters are not yet studied extensively, more research into this essential aspect of asthma is vital.
In this review we have demonstrated that lung function in general does not improve after training in children with asthma. This is in accordance with studies in adults, suggesting that lung volumes and lung function cannot be improved with regular exercise.74 The PEF seems to be the only lung function parameter which is slightly improved by training, probably due to increased strength of the respiratory muscles after training. This view is strengthened by the finding that changes in PEF after training are not accompanied by changes in FEV1.
The results of our review are in accordance with the results of three previous systematic reviews.17 ,75 ,76 Alongside an update of the literature we provided an overview of additional parameters, such as the effects of exercise training on EIB and pathophysiological pathways.
Based on the studies in this review, some recommendations for new interventions can be made. First, it seems that intensity rather than type of training (eg, running, aerobic or swimming training) is one of the most important factors in determining the success of an intervention. It is important to individualise the training intensity for each individual. Some studies used the same training intensity for all individuals, which could have decreased the effectiveness of training in these studies.2 ,29 ,30 ,36 ,40 ,45 ,51 To improve oxygen uptake, the training intensity should be set at the (personalised) ventilatory threshold.31 ,54 To train at this intensity, it is recommended that children have adequate asthma control, which can be achieved through appropriate pharmacological therapy. Second, the duration and frequency of the training programme are important for achieving a training effect. Exercise for at least 120 min/week, divided across at least two training sessions, with a training programme lasting for at least 3 months is recommended. Third, the quality of future studies could be improved by increasing the number of individuals, performing an intention-to-treat analysis, specifying the eligibility criteria more precisely and clearly, and blinding of the outcome assessor. Finally, it would be of interest to add measurements of habitual physical activity (eg, accelerometers) as Santuz et al77 demonstrated that habitual physical activity is an important factor for improving exercise performance in children with asthma.
Since this review provided no clear evidence that exercise can improve lung function parameters, while EIB in some cases can be improved in children, it is important to investigate whether exercise influences the underlying pathophysiology of asthma. It is necessary to investigate the effects of both single bouts of exercise and exercise training on asthma-related (inflammatory) markers. This might be non-invasively assessed by measuring inflammatory markers in exhaled breath such as FeNO.
This review has demonstrated that an individualised exercise training programme improves cardiorespiratory fitness and has the potential to improve EIB in children with asthma. Physical activity should be recommended to children with asthma by healthcare providers as it can be considered safe and beneficial. However, exercise has minimal impact on lung function in asthmatic children.
What this study adds
-
Exercise training has a minimal impact on lung function in children with asthma.
-
Cardiorespiratory fitness and exercise-induced bronchoconstriction can improve as a result of exercise training in children with asthma.
-
An effective training programme for children with asthma consists of
-
A personalised training intensity;
-
A duration of at least three months;
-
At least two 60-min training sessions/week.
-
-
Physical exercise is safe and can be recommended in children with asthma.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Correction notice One of the authors' surnames was incorrectly tagged in the xml as ‘Kant’. The correct surname is ‘van de Kant’.
-
Contributors VHMW, MW and KDGvdK were responsible for inclusion of studies, quality assessment, data extraction and writing of the manuscript. ED contributed to the coordination and writing of the manuscript. All authors read and approved the final manuscript. KDGvdK is identified as the guarantor of the paper, thereby taking responsibility of the integrity of the work.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.