Article Text

Abstract
Background/Aim Cardiorespiratory fitness (CRF) is a strong determinant of morbidity and mortality. In athletes and the general population, it is established that high-intensity interval training (HIIT) is superior to moderate-intensity continuous training (MICT) in improving CRF. This is a systematic review and meta-analysis to quantify the efficacy and safety of HIIT compared to MICT in individuals with chronic cardiometabolic lifestyle diseases.
Methods The included studies were required to have a population sample of chronic disease, where poor lifestyle is considered as a main contributor to the disease. The procedural quality of the studies was assessed by use of a modified Physiotherapy Evidence Base Database (PEDro) scale. A meta-analysis compared the mean difference (MD) of preintervention versus postintervention CRF (VO2peak) between HIIT and MICT.
Results 10 studies with 273 patients were included in the meta-analysis. Participants had coronary artery disease, heart failure, hypertension, metabolic syndrome and obesity. There was a significantly higher increase in the VO2peak after HIIT compared to MICT (MD 3.03 mL/kg/min, 95% CI 2.00 to 4.07), equivalent to 9.1%.
Conclusions HIIT significantly increases CRF by almost double that of MICT in patients with lifestyle-induced chronic diseases.
- Cardiovascular
- Aerobic Fitness/Vo2 Max
- Exercise Physiology
- Statistical Review
Statistics from Altmetric.com
Introduction
Lifestyle-induced chronic diseases significantly alter the quality of life of sufferers. In many cases, the disease itself can be potentially avoided or successfully managed with appropriate lifestyle modifications.1 Diseases such as type II diabetes, atherosclerotic cardiovascular disease and the metabolic syndrome are closely related and often stem from the same preventable risk factors. Therapy for most chronic diseases involves exercise training to slow or reverse disease progression. Despite the known benefits of regular moderate-intensity exercise in regulating risk factors in chronic disease, the majority of patients are still physically inactive.2
Rehabilitation for cardiac patients prior to the 1950s comprised abstention from all forms of physical activity. This was thought to diminish the cardiac load and assist in the reparative process of the healing myocardial scar.3 Levine and Lown4 appear to be the first to document challenging the idea of complete immobilisation by introducing the then controversial ‘armchair treatment’ where patients were encouraged to sit in an armchair as much as possible during hospitalisation postmyocardial infarction. When the weight of evidence suggesting the benefits of light-to-moderate activity in patients with chronic disease became irrefutable, exercise guidelines were created for this population.5 Interval training appears to have been first studied in cardiac rehabilitation in 1972, when patients were asked to cycle at high workloads for 60 s with a 30 s rest between intervals. Using the intervals, the patients were able to exercise for at least twice as long as what they were able to do when cycling continuously.6 In 1977, a study on healthy participants examined the effects of a 10-week programme which included a combination of interval and moderate continuous training. Interestingly, the authors found a linear increase in augmenting maximal oxygen uptake (VO2max) over 10 weeks, contrary to the study's hypothesis that VO2 would plateau over time.7 In 1979, it was suggested that high-intensity exercise was required to provoke the necessary training adaptations needed to improve exercise capacity in patients with recent myocardial infarctions.8 One of the first studies to investigate intense exercise in patients with cardiovascular disease found that if the exercise is intense and prolonged enough, then it can instigate a reduction in myocardial ischaemia.9 These findings were revolutionary, as they were established before widespread percutaneous coronary interventions were performed. From there, differing study protocols in the 1980 s and 1990 s in cardiac patients led to conflicting findings that appear to have decreased the interest in this approach.10–12 Forty years after the first reported use of interval training in cardiac patients, the interest in high-intensity interval training (HIIT) in higher risk patients has now led to a number of studies in this area.
HIIT involves alternating short bursts of high-intensity exercise with recovery periods or light exercise. Studies in athletes and the general population have shown that increasing the intensity of exercise amplifies the training stimulus and associated adaptations, such as VO2max, anaerobic threshold, stroke volume and performance.13 ,14 A commonly cited barrier to physical activity is lack of time. Including HIIT in a training programme implies that greater health-enhancing benefits could be gained in less time, making HIIT a more time efficient and attractive option. Moreover, short bursts of activity may address another common limiting factor, lack of motivation, as it may be a more enticing option than the prospect of continuously exercising for an extended period of time. Short work periods at a higher intensity also result in a reduction in the ventilatory response and resultant dyspnoea, which in many patients with chronic disease are limiting factors to continuous exercise.15
VO2max is a strong predictor of mortality.16 Indeed, a 1-metabolic equivalent task (MET) increase is associated with a 10–25% improvement in survival.17 Furthermore, it is established that cardiorespiratory fitness is more cardioprotective than the overall physical activity levels.18 This provides further evidence regarding the benefits of higher intensity exercise compared with lower intensity general physical activity. It seems likely that improving VO2max will improve the prognosis of patients with chronic disease.
The aim of this systematic review is to compare and quantify the effects of HIIT against moderate-intensity continuous training (MICT) in improving VO2max in patients with lifestyle-induced chronic diseases. Furthermore, safety of HIIT will be discussed along with the feasibility of this approach with suggestions to standardise terminology and protocol recommendations.
Methods
Electronic searching of the MEDLINE, PubMed, EMBASE and Cinahl databases were conducted from the earliest available date to April 2013, limited to the English language. The Medical Subject Heading (MeSH) database was employed to establish all related articles on HIIT and chronic disease. The MeSH terms used were ‘cardiovascular diseases’ OR ‘metabolic diseases’ OR ‘chronic diseases’ and their related terms. Text words used in conjunction with the MeSH terms were ‘high intensity training/exercise’, OR ‘interval training/exercise’, OR ‘intermittent training/exercise’, OR ‘low volume training/exercise’ OR ‘aerobic interval training/exercise’. Reference lists of retrieved articles were also searched for in other appropriate studies.
Inclusion criteria
Only full text, randomised control trials were considered for inclusion. The studies were required to have a cardiometabolic chronic disease population, where poor lifestyle is considered to be the main contributor. The main characteristics of such diseases, such as coronary artery disease, heart failure, diabetes, hypertension, obesity and metabolic syndrome, are recognisable by the common presence of cardiovascular risk factors. Other systematic reviews on the effects of HIIT have been conducted with specific conditions: pulmonary disease15 and coronary artery disease.19 Inclusion criteria were: exercise protocols using cardiorespiratory exercise training; a comparator group that completed MICT (matched to HIIT); an accepted measure of intensity (ie, heart rate or rating of perceived exertion); intervention of 4 weeks; appropriate intensities for both groups (eg, 60–75% peak heart rate (PHR) for MICT, 85–95% PHR for the high-intensity intervals or 80–100% peak work rate (PWR)) and a direct measure of the VO2peak/max. Owing to the difficulty patients with chronic disease have in reaching a plateau in the VO2max, the VO2peak was reported in nine of the studies.20–28 Studies including other activities (eg, resistance training) on top of the prescribed aerobic intervention were also included, provided the same volume and modality of resistance exercises were given to the MICT and HIIT groups.
Data collection and analysis
After full text analysis of the retrieved articles, 10 articles were identified to have met the inclusion criteria for the purpose of meta-analysis (table S1—web file only). These trials involved 273 patients consisting of men and women. This included 137 in HIIT groups and 136 in the MICT groups. The corresponding authors of two eligible studies were contacted for VO2 data, but no information was provided.29 ,30
The procedural quality of the studies was assessed by use of the modified Physiotherapy Evidence Base Database (PEDro) scale. Table 1 illustrates that one point was awarded for each of the 10 criteria. Review Manager statistical software V.5.0 (Nordic Cochrane Centre, Copenhagen, Denmark) was used to determine the mean difference and 95% CI. A forest plot is used to portray the treatment effects of each study (figure 1).
Methodology quality of the high-intensity interval training (HIIT) studies conducted in patients with chronic disease

Systematic review process.
Results
Seven of the 10 studies included in this review studied cardiovascular disease; Rognmo et al21 and Moholdt et al22 investigated coronary artery disease and Wisloff et al,20 Roditis et al,23 Freyssin et al,24 Fu et al28 and Iellamo et al27 recruited heart failure patients. Molmen-Hansen et al25 studied participants with hypertension, Schjerve et al26 looked at participants with obesity and Tjonna et al31 investigated the metabolic syndrome. Six of the 10 studies were conducted at the same institute, the Norwegian University of Science and Technology.20–22 ,25 ,26 ,31
The quality assessment of the studies was determined by two reviewers. Where there was a discrepancy, the average was taken. The studies achieved a mean PEDro score of 7.35/10. There was no blinding of all assessors in any of the studies reviewed. A between-group statistical comparison was provided by all studies with measures of variability given for the VO2peak.
Meta-analysis
Nine studies included means and SDs of the VO2peak to allow the calculation of an overall mean difference.20–27 ,31 One study provided means±SE of mean, allowing the SDs to be calculated.28 Homogeneity between the studies was displayed with I2=9%, p=0.36. The mean difference in the VO2peak from the 10 studies was 3.03 mL/kg/min (95% CI 2.00 to 4.07), significantly (p<0.001) favouring HIIT (figure 2).
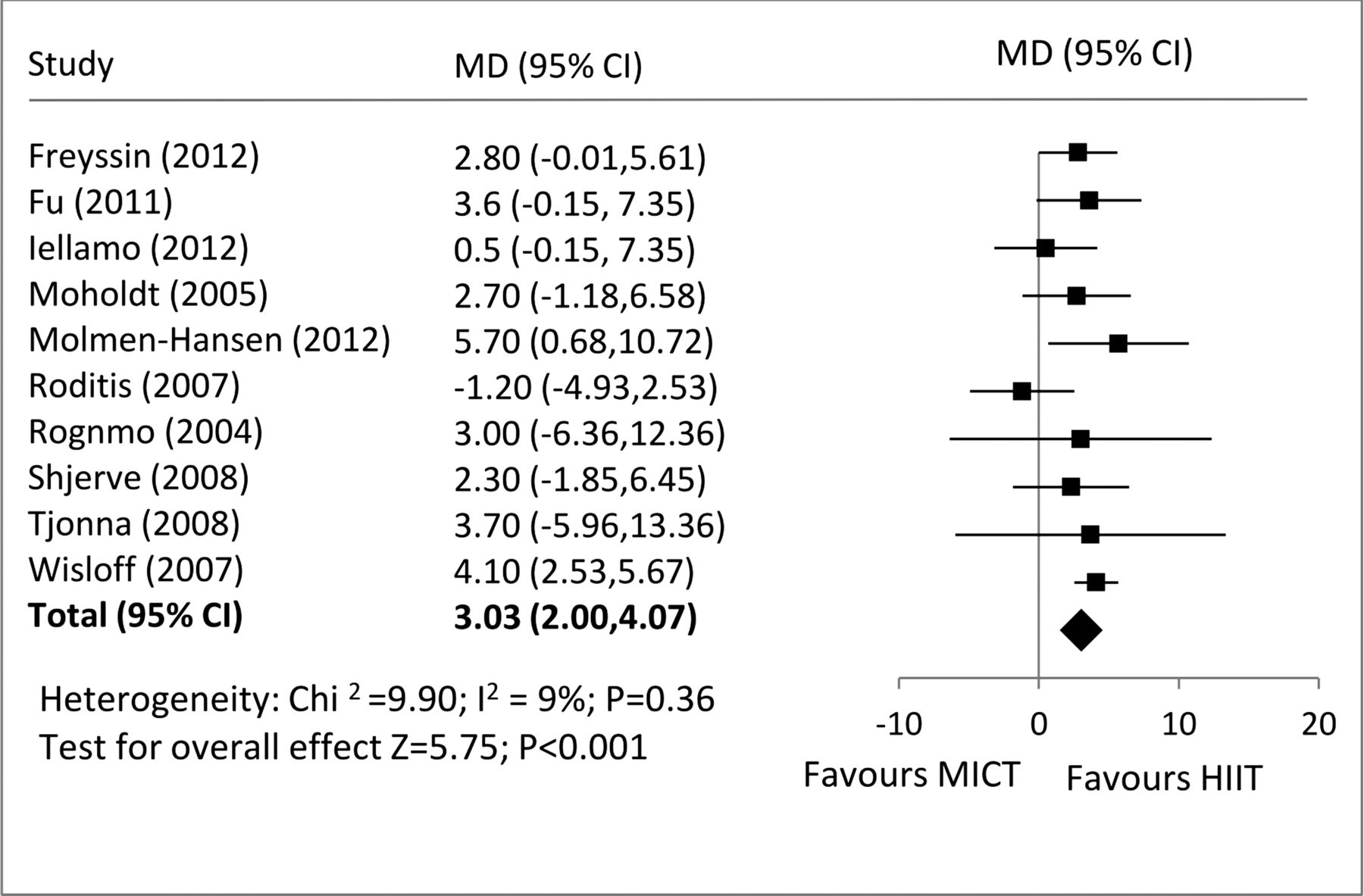
Forest plot of included studies.
Exercise protocols
Mode
Seven studies used uphill walking/running on a treadmill as the primary exercise modality.20–22 ,25–27 ,31 One study described the exercise undertaken as ‘treadmill walking’; therefore, the differences in heart rate between intervals could have been achieved either through a change in speed or a change in incline.22 In three studies, cycle ergometers were used for the duration of the programme.23 ,24 ,28 Freyssin et al24 used strengthening, stretching and relaxing exercises in addition to the treadmill and cycle programme.
Intensity
Intensities were set based on baseline maximal/peak testing data. Six studies used a percentage of PHR or maximal heart rate (MHR), two studies used a percentage of PWR or peak power and a further two studies used the VO2peak/heart rate reserve (VO2peak/HRR). The Norwegian studies used a heart rate of between 85% and 95% for the high-intensity interval with a recovery of 50–75% MHR.20–22 ,25 ,26 ,31 Two studies on the cycle ergometer were set at an intensity of 80% and 120% PWR for the high-intensity interval with a passive recovery.23 ,24 The two studies using the HRR/VO2peak to determine intensity used 75–80% for the interval and 40–50% for an active recovery.27 ,28
Total duration
A common approach to compare the HIIT and MICT sessions is to match the energy expenditure, resulting in the HIIT session being shorter. Seven of the studies differed the duration of the HIIT and MICT sessions so that the training sessions were isocaloric.20–22 ,25 ,26 ,28 ,31 The median duration of exercise times was 38 min for the HIIT group and 46 min for the MICT group. One study kept the duration identical between both groups but altered the mean intensity between the groups.23 Another study used a different method (training impulse method) to alter the duration of each session based on the average change in heart rate.27
Interval duration
Seven of the studies included high-intensity intervals of 4 min with 3 min of active recovery.20–22 ,25–27 ,31 One study included 5×3 min intervals with 3 min recoveries.28 Two studies included shorter interval and recovery periods, with 30 s used for interval as well as recovery,23 and 30 s used for interval and 60 s for recovery.24
Supervision
Three studies included a supervised training component as well as a self-administered home programme,20 ,22 ,26 whereas the remaining were purely supervised sessions. Direct supervision allows the instructor to adjust the intensity, monitor the patient and provide motivation. The length of supervised HIIT or MICT within the studies varied from 4 to 16 weeks. One study was supervised for the first 4 weeks, and thereafter the participants were advised to continue the training programme at home for the following 6 months.22 The studies prescribed 3–6 training sessions/week, with two studies including one home session/week out of the three for the HIIT and MICT groups.20 ,26
Owing to the constant changes in the heart rate response to exercise, supervision allows for a closer monitoring to ensure that the rates are within the desired zones. Therefore, the presence of a supervisor is quite likely to improve the accuracy of the intensity.
Outcomes
Adaptations occurring significantly more with HIIT compared with MICT are shown in box 1.
Adaptations occurring significantly more with HIIT compared to MICT
-
↑VO2peak
-
↓Systolic and diastolic blood pressure
-
↑High density lipoproteins
-
↓Triglycerides and fasting glucose
-
↓Oxidative stress and inflammation
-
↓FATP-1 and FAS
-
↑Adiponectin, insulin sensitivity and β-cell function
-
↑PGC-1α
-
↑Maximal rate of Ca2+ reuptake
-
↑Availability of nitric oxide
-
↑Cardiac function
-
↑Enjoyment of exercise
-
↑Quality of life
FATP-1, fatty acid transport protein 1; FAS, fatty acid synthase; HIIT, high-intensity interval training; MICT, moderate-intensity continuous training
Cardiorespiratory fitness
There were improvements in the VO2peak from HIIT as well as MICT in nine of the ten studies.20–22 ,24–28 ,31 The average of the pretraining values was 22.5 and increased to 27.9 mL/kg/min after HIIT (a 19.4% increase). MICT had baseline values of 22.6 that increased to 25.2 mL/kg/min after the intervention (10.3% increase). The mean difference in the change in the VO2peak between HIIT and MICT was 3.03 mL/kg/min. A measure of exercise capacity (6 min walk test), as well as the VO2peak, was assessed in one study. It was found that the distance walked improved in the HIIT and MICT groups.24
Cardiometabolic risk factors
The study by Tjonna et al31 found that MICT and HIIT both reduced blood pressure, approximately 10 mm Hg systolic and 6 mm Hg diastolic. Molmen-Hansen et al25 also showed a significant reduction of 12 mm Hg for systolic blood pressure in the HIIT group. Other studies showed no change in systolic blood pressure after the interventions. Significant reductions in oxidised low-density lipoproteins were found in HIIT but not MICT.20 ,31 However, in one study, the opposite was found.26 Furthermore, it was established that high-density lipoprotein was increased by 25% in the HIIT group.31 These changes were supported by Wisloff et al20 who also found an increase in high-density lipoprotein, lower triglycerides and improved fasting glucose in the HIIT group. An improvement in triglycerides was identified by Moholdt et al22 for the HIIT and MICT groups. Iellamo et al27 found no significant differences in the metabolic profile (lipids, homeostasis model assessment-insulin resistance (HOMA-IR)), with the exception of an improvement in fasting glucose with HIIT. Fu et al28 found improvements in oxidative stress/inflammatory markers plasma brain natriuretic peptides, myeloperoxidase and interleukin-6.
Two studies demonstrated no positive improvements in weight loss, body mass index or body composition between the HIIT and MICT groups postintervention.27 ,31 Furthermore, one study on obese patients reported a greater decrease in body weight with MICT than with HIIT.26 However, reduced fatty acid transport protein 1 (FATP-1) and fatty acid synthase (FAS) levels (markers of fatty acid uptake and lipogenesis) were identified, which was associated with improvements in anti-insulin receptor activation in HIIT but not MICT.31
The findings from Tjonna et al31 showed increased circulating adiponectin and improved insulin sensitivity and β-cell function in the HIIT group. No changes in adiponectin were found by Moholdt et al22 at 4 weeks; however, after the 6-month intervention, HIIT and MICT increased the circulating levels.
Skeletal muscle
Three studies identified significant increases in PGC-1α, indicating improved mitochondrial biogenesis in the HIIT group.20 ,26 ,31 These studies also significantly increased the maximal rate of Ca2+ reuptake into the sarcoplasmic reticulum by 50–73%. Changes in the total myoglobin concentration and tissue oxygenation in the vastus lateralis were observed in HIIT but not MICT both acutely and after the 12 week intervention.28
Myocardium and vasculature
Flow-mediated dilation was improved after HIIT and MICT in studies that assessed endothelial function.20 ,25 ,26 ,31 An increased availability of nitric oxide was found with HIIT but not MICT.31 Furthermore, a greater increase in antioxidant status, found in HIIT rather than MICT, supports the finding of increased production and availability of nitric oxide.20 An improvement in antioxidant status was not supported by the findings of Schjerve et al.26 Patients with heart failure demonstrated improved left ventricular ejection fraction by 10% and a positive reversal of left ventricular remodelling.20 An improvement in left ventricular ejection fraction was also demonstrated by Fu et al,28 alongside increases in cardiac output and total peripheral resistance. In contrast, Iellamo et al27 found no difference in cardiac output, stroke volume and left ventricular ejection fraction in their patients with heart failure. Patients with hypertension also had significantly improved ejection fraction, stroke volume, systolic flow velocity, end-diastolic volume, early diastolic mitral annulus tissue velocity and isovolumic relaxation rate.25
Adherence
A minimum attendance of 70% and 90% of training sessions was an inclusion criterion for four of the studies.21 ,22 ,25 ,26 Only one participant was excluded from the analysis from one of these studies based on this criterion.21 For the first 4-week supervised period of Moholdt et al's study, the HIIT group attended 82% of sessions and the MICT group attended 84%. The attendance rate during the remainder of the 6-month home programme was not identified.22 Both groups in six of the other studies reported attendance rates above 85%.20 ,21 ,24 ,27 ,28 ,31 One study did not mention adherence to the protocol for either group.23
Enjoyment and quality of life
HIIT was reported to be more enjoyable than MICT.31 Three studies demonstrated that HIIT improved the quality of life more than MICT,20 ,25 ,28 whereas another study showed similar increases between the two groups.22 Anxiety and depression also had similar improvements with HIIT and MICT.24
Adverse events
Reporting of adverse events is important in determining the safety of applying this type of training to high-risk populations. No studies described their adverse event monitoring protocol. However, four reported no adverse events due to the exercise training20–22 ,24 and six did not mention adverse events.23 ,25–28 ,31
Discussion
The main finding from this meta-analysis is that HIIT is superior to MICT in improving CRF in patients with lifestyle-induced chronic diseases. Indeed, the increase in the VO2peak with HIIT was almost twice the increase gained from MICT. In addition, although there are limited data, HIIT appears to be well tolerated and safe.
Efficacy
HIIT increased the VO2peak by 5.4(19.4%) compared with 2.6 mL/kg/min (10.3%) with MICT. It has been shown that a 1-MET (3.5 mL/kg/min) increase is associated with 10–25% improvement in survival.17 Indeed, the protective role of fitness occurs even in the presence of established cardiovascular disease risk factors.32 CRF is an easily modifiable risk factor; therefore, identifying the most effective way to improve VO2peak should be a health priority.
Some of the studies investigated mechanisms explaining the greater improvement of the VO2peak with HIIT. Peripheral adaptations leading to improvements in CRF were investigated by measuring PGC-1α and Ca2+ reuptake into sarcoplasmic reticulum in the skeletal muscles. Mitochondrial dysfunction is central to most chronic diseases and could play a vital role in the reduced CRF that is experienced by these populations. Improvements in mitochondrial biogenesis have been demonstrated by increases in PGC-1α after a single bout of low volume HIIT.33 Studies by Tjonna et al31 and Wisloff et al20 identified significant increases in PGC-1α (138% and 47%, respectively), indicating mitochondrial biogenesis in the HIIT group. Wisloff et al20 found the increase in PGC-1α to be strongly correlated with the improved VO2peak (r=0.72, p<0.01), supporting the influence of mitochondrial function on exercise capacity. Mitochondrial biogenesis is essential to maintain the structural integrity of skeletal muscle. Daussin et al34 concluded that a fluctuation in ATP turnover in interval training, which is different from the usual steady-state conditions of ATP production, activates the signalling pathways, which lead to increases in PGC-1α. The increase in PGC-1α identified by Wisloff et al and Tjonna et al may translate into improvements in aerobic and functional capacity. Both studies also significantly increased the maximal rate of Ca2+ reuptake into the sarcoplasmic reticulum by 50–60%.20 ,31 The increase in calcium cycling reduces skeletal muscle fatigue and would contribute to improvements in muscle function and therefore CRF. The findings by Fu et al28 demonstrate repeated bouts of deoxygenation in HIIT but not MICT, which may contribute to the observed adaptations to the muscles’ oxidative capacity.
Improvement in the VO2peak with HIIT can also be explained mechanistically by central factors. Findings from one of the studies indicate that HIIT improved ejection fraction in patients with heart failure to the same degree as treating with ACE inhibitors and β-blockers, outlining the potential for further left ventricular remodelling with HIIT (Wisloff20). Improvements in cardiac remodelling are supported by the findings of Fu et al,28 with significant reductions in brain plasma natriuretic peptide levels. HIIT may also contest modern medical treatments in improving systolic and diastolic blood pressure, with significant decreases of 12 and 8 mm Hg, respectively, found in patients with hypertension.25 It was also found that the myocardial contractile function was improved with HIIT in terms of stroke volume, mitral annular excursion, ejection velocity and systolic mitral annular velocity. Besides a small reduction in the left ventricular filling pressure with MICT, the aforementioned improvements in systolic and diastolic function with HIIT were not found with MICT.
Conversely, Roditis et al23 demonstrated similar improvements in the VO2peak for the HIIT and MICT groups. Furthermore, the findings suggest that phase II of oxygen kinetics (indirect measurement of muscle oxidative capacity), showed superior improvements after MICT. The use of 30 s Wingate sprint intervals in this study may highlight the need for a longer duration of intervals, such as those used in four of the other studies reviewed.20–22 ,31 Although 30 s intervals are a more time efficient option than endurance training (similar improvements shown with ∼90% less volume), 30 s may not be long enough to induce superior health-enhancing benefits.14 It appears from the studies reviewed that HIIT elicits many superior benefits to MICT in a slightly shorter time period (median 38 vs 46 min, respectively). It seems reasonable to suggest that gaining similar benefits would require either a longer period of MICT or an even shorter period of HIIT, supporting the ideology of HIIT being a more time efficient option. Future studies should identify the minimum amount of HIIT needed to elicit adaptations similar to MICT. There was another study that did not find a greater benefit of HIIT over MICT, which may be due to the method of establishing intensity by assessing blood lactate levels.27
The HERITAGE study has established the influence genetic components have on the trainability of the VO2max in certain individuals, resulting in ‘non-responders’ to exercise training.35 The consistently large improvements in the VO2max seen in a variety of cohorts in the HIIT studies questions whether this type of training can ameliorate the familial dampening of VO2 in these ‘non-responders’. Only one study in 1986 has examined the relationship between HIIT and hereditary trainability.36 Although aerobic capacity was not assessed in this study, it was found that genotype was associated with anaerobic capacity after a HIIT training intervention, suggesting that the effectiveness of HIIT is affected by hereditary factors.36 Indeed, in the studies reviewed in the meta-analysis, the SD of the change in the VO2peak in the HIIT group was 26% (relative to the mean change), whereas the MICT group had only an 8% variance. Future studies are needed to further compare the effects of HIIT and MICT on the VO2peak trainability.
In addition to CRF, efficacy can also be assessed by the effect on cardiometabolic risk factors. The studies reviewed found reductions in risk factors in HIIT notwithstanding the differences in body mass, body mass index or weight loss between HIIT and MICT. These findings are supportive of the theory of ‘fitness over fatness’—in that it is more beneficial to health to improve physical fitness than to focus solely on weight loss. This is supported by Terada et al37 who found similar reductions in body fat percentage in the HIIT and MICT groups after a 5 day/week, 12 week programme. Although weight loss was not different between groups, one study found a reduction in the FATP-1 and FAS levels in the HIIT group, suggesting a suppression of fatty acid uptake and lipogenesis. No studies measured visceral adiposity; however, the existence of increased circulating adiponectin levels found with HIIT but not MICT is suggestive of decreased intra-abdominal obesity.
Owing to the augmented PHR and cardiac output that is experienced in HIIT, it is quite likely that pulsatile and shear stress influence vasculature during periods of intense exercise.38 Interval exercise has been shown to reduce arterial stiffness through increased distensibility of the vessels.38 ,39 A recent study by Smart and Steele40 demonstrated no difference in fitness and cardiac function between moderate training and intermittent training groups matched by the volume of work. However, the intervals were not high intensity, suggesting that to elicit changes, intervals need to increase the heart rate to a certain level. Arterial stiffness is a key contributor to a number of cardiovascular conditions that influence mortality through cardiovascular disease.41 Two studies demonstrated higher endothelial derived nitric oxide production in the HIIT group.20 ,31 It is suggested that shear stress through an increase in pulse and frequency pressure promotes vasodilatory nitric oxide release, thereby increasing arterial compliance.42 This is further supported by Wisloff et al20 and Tjonna et al31 who found greater increases in flow-mediated dilation in HIIT than in MICT. The improvements in endothelial function are supported by the findings from Fu et al.28 The study's findings demonstrate an increase in perfusion and oxygen utilisation between cerebral and muscular tissues, which occurs through increases in shear flow and metabolic stress. The increased perfusion to the vastus lateralis and frontal cortex would promote increased flow and shear stress and therefore the release of NO.
Safety
The reporting of adverse events enables the safety of the intervention to be inferred to the population being studied. Four of the 10 reviewed studies reported no adverse events as a result of the exercise training.20–22 ,24 One study that did not mention adverse events did explain that follow-up testing was not performed on five patients either due to orthopaedic-related problems or the inconvenient programme timetable.23 Other reasons cited for loss of patient follow-up were comorbidities (the group was not cited),22 ankle fracture in the HIIT group and knee injury in the MICT group.21 One participant in the MICT group died from cardiac causes; however, it was stated that this was unrelated to exercise training.20
A recent study by Rognmo et al 43 aimed to assess the safety of HIIT compared to MICT, during and after exercise, in patients with coronary heart disease in cardiac rehabilitation. The study of 4846 participants indicated that the risk of a cardiovascular event occurring is low in MICT and HIIT. During this study, there was one fatal cardiac event during MICT and two non-fatal cardiac events during HIIT. The calculated event rates were 1/129 456 h of moderate-intensity exercise and 1/23 182 h of high-intensity exercise. Moreover, when vigorous intensity exercise was energy matched with moderate-intensity exercise, greater cardioprotective benefits were elicited. To accurately assess a cardiac event occurring during training, the study required a sample size of >20 500 patients. Despite the study being underpowered,44 the results explore the beneficial dose–response relationship associated with HIIT and the negligible risk that is involved.
The safety of HIIT has been controversial among health professionals treating high-risk populations. This has perhaps been created through a common avoidance of anginal episodes, which can sometimes be triggered by high-intensity exercise. Although commonly thought to be a dangerous byproduct of exercise, episodes of controlled ischaemia may actually be beneficial in preventing secondary conditions in coronary artery disease through ischaemic preconditioning.45 Exercise-induced coronary collateral formation is based on the vascular endothelial growth factor, and this adaptation is correlated with exercise intensity. Lu et al46 found that exercise-induced intermittent ischaemia promoted coronary angiogenesis by the vascular endothelial growth factor. The favourable effects of intermittent exercise on angiogenesis is further supported in a meta-analysis on peripheral arterial disease.47 In a study by Lu et al, a normal cardiac troponin I indicated that no myocardial damage occurred when ischaemia was applied. Lu et al state that HIIT is safe even for patients with high-risk chronic disease with stable angina. Rather than promoting the instigation of angina in HIIT, this information is intended to highlight the safety of HIIT in high-risk populations. Caution should be exercised on a case-by-case basis depending on the participant's cardiac history. Indeed, despite the patients in the studies reviewed being a high-risk cohort, they were only included if their diseases were relatively well controlled or stable. Therefore, these findings may not be applicable to some patients in these disease groups. Box 2 provides a suggested guide of contraindications for participation in HIIT in high-risk patients. In summary, when used with appropriate screening and communication with the patient's doctor, HIIT can be a safe option for patients with high risk.
Suggested contraindications to high-intensity interval training (HIIT)
-
Unstable angina pectoris
-
Uncompensated heart failure
-
Recent myocardial infarction (<4 weeks)
-
Recent coronary artery bypass graft or percutaneous coronary intervention (<12 months)
-
Heart disease that limits exercise (valvular, congenital, ischaemic and hypertrophic cardiomyopathy)
-
Complex ventricular arrhythmias or heart block
-
Severe chronic obstructive pulmonary, cerebrovascular disease or uncontrolled peripheral vascular disease
-
Uncontrolled diabetes mellitus
-
Hypertensive patients with blood pressure >180/110 (or uncontrolled)
-
Severe neuropathy
Limitations
Although this review provides the basis for further clinical trials testing of HIIT in rehabilitation of patients with chronic disease, all the studies analysed experienced methodological limitations. Although three of the studies used a different training protocol to the other seven, the heterogeneity of the VO2peak measure was low (χ2=9.90, I2=9%, p=0.36).23 ,24 ,28 Owing to the relatively recent interest with HIIT in chronic disease, HIIT training guidelines have not yet been created. Consequently, current research consists of a variety of intervals, intensities and programme durations. Furthermore, comparison of studies proves difficult when volumes of HIIT and MICT are equated in different ways. There are also discrepancies in the percentage of heart rate used. Some of the studies used a higher definition of moderate intensity (75%) to the general intensity of moderate exercise suggested by Norton et al (55–70% MHR) and the American College of Sports medicine (ACSM; 60–70% MHR).2 ,20 ,21 ,48 Not all studies included assessor blinding of the VO2peak, which may have influenced the testing results. Also, studies in cardiac rehabilitation programmes may have been guided by other confounding factors such as dietary advice or smoking status. A limitation of this review is that 6 of the 10 studies reviewed are from the same research group. It is important that these findings are replicated in future studies at other institutions.
The studies reviewed consisted of small sample sizes, with one study including an unequal male-to-female ratio.20 The current literature is lacking in HIIT studies on all the chronic diseases. This systematic review on the cardiometabolic lifestyle-induced chronic diseases would have benefited from studies with other lifestyle diseases such as type II diabetes and chronic kidney disease. Owing to the limited research in this area, a variety of diverse diseases were included under the title cardiometabolic disease for this meta-analysis. However, the pathophysiology of the varied diseases may mean that HIIT will have different influences on the parameters being compared among different studies. Research on more chronic diseases will allow specific prescription guidelines to be recommended.
Protocol recommendations
Future research is needed to establish the optimal protocol of HIIT. However, based on the findings from this review, recommendations in table 2 are provided. It is important to note that the effectiveness and adherence to different HIIT protocols will always be highly individualised.
Protocol recommendations for HIIT
Mode and intensity
The duration of intervals can differ greatly in various HIIT protocols. Two studies which used shorter duration intervals of 30 s showed no improvements and smaller improvements in the VO2peak, respectively.23 ,24 Studies which demonstrated the biggest changes in the VO2peak after a HIIT intervention used the 4×4 approach (4 intervals at 4 min each between 90% and 95% PHR).20–22 ,25 ,26 ,31 The recommendation of the 4×4 approach (∼40 min duration) in table 2 does not preclude shorter duration HIIT protocols being potentially more appropriate. However, more research is needed to compare a shorter duration of HIIT with the current recommendation. Furthermore, future research comparing HIIT and MICT should ensure that MICT is kept consistent with current definitions of moderate exercise.
Recovery
The intensity and duration of the recovery period in HIIT may play just as integral role as the interval period. Past research has suggested that an active recovery is recommended in order to effectively aid the process of lactate removal.49 However, a study by Dupont et al50 indicated that during the active rest period there was less replenishment of oxygen in myoglobin and haemoglobin and a reduced rate of resynthesis of phosphocreatine from the previous work phase. Meyer et al's study51 on patients with chronic heart failure found that short intervals (30 s) with passive recovery provided the most benefit (longest time to exhaustion in an exercise test). This study also determined that including a passive recovery instigated a lower rating of perceived exertion as indicated on the BORG scale, despite having a higher oxygen pulse, which is dependent on the stroke volume and arteriovenous difference.51 Logistically, it may be more practical and convenient to include an active recovery for the purpose of timing and equipment control, albeit at as low an intensity as possible. To successfully employ HIIT, recovery intensities need to be achieved. If the heart rate is not reducing to the required intensity by the end of the recovery period, the interval work rate should be adjusted accordingly.
Feasibility
Indisputably, the success of an exercise intervention and maximising long-term benefits relies directly on adherence to the exercise programme. Central to adherence is the enjoyment of the activity being prescribed. Bartlett et al52 found that the ratings of perceived enjoyment after HIIT were higher when compared to MICT. It was identified in this study that the rating of perceived exertion had a positive correlation with enjoyment, through a likely combination of stimulation and accomplishment.
Wisloff et al's20 study addresses the feasibility of HIIT being performed independently. During home sessions, participants were provided with heart rate monitors that recorded heart rate data. These monitors were placed so that they could not be seen by the participant. The patients achieved the correct heart rate zones without feedback from the heart rate monitor. The design of this study supports the feasibility of incorporating HIIT into a real-world situation, where a home HIIT programme can be successfully prescribed after a familiarisation period. This is further supported by Moholdt et al,53 who demonstrated that adherence to a home programme of HIIT was as suitable as the usual cardiac residential care.
Future directions
Given the small number of studies conducted thus far, there are still important questions that need to be addressed. Similar to current issues with the dose response of less intensive exercise, much more work is needed to determine if the recommendations provided here provide the optimal approach for future studies. Furthermore, it is realistic that most people will combine HIIT with MICT; therefore, determining the optimal ratio of both types of training over longer periods of time is also important. Similarly, current guidelines for all populations recommend the inclusion of resistance training in an exercise programme; yet the interaction between HIIT and resistance training is unknown. As it is likely that most people will include HIIT and resistance training in the same session, future studies should identify the ratio of HIIT and resistance training needed for optimal benefits.
Analogous to the clinical trial phases in the development of a new pharmaceutical product, the evaluation of HIIT training for patients with cardiometabolic diseases would be in phase 2 (assessing efficacy). Indeed, the guidelines for clinical populations should use the same approach and criteria as other therapies (eg, drugs), with eventual recommendations based on large randomised control trials and not on small feasibility and efficacy studies alone.
Another important question is regarding adherence after the supervised programme. Future studies should determine whether this approach is sustainable in a non-supervised, home-based environment.
Consistency of terminology
The terminology used to describe HIIT varies across research groups. The Norwegian research group that has conducted the majority of studies in this area has preferred the term ‘aerobic interval training (AIT)’. Other prominent groups have used ‘SIT’ to describe all-out supramaximal (>100% VO2max) intervals in studies with healthy individuals14 ,54 or low-volume HIIT when short intervals (∼30 s) with an intensity <95% are used.55 ,56 We suggest that the classification scheme shown in figure 3 is used to standardise terminology in future studies. This approach is based on (1) the widespread media use of the term ‘HIIT’ rather than ‘AIT’ for nearmaximal intensity (80–100% PHR) intervals, (2) the additional information regarding the intensity of the interval provided by HIIT compared to AIT and (3) the need to separate all-out supramaximal sprint interval training from HIIT as there are concerns for the safety of this all-out approach in clinical populations. Furthermore, it is suggested that, in comparative studies, the term ‘moderate-intensity continuous training’ (MICT) should be used, where appropriate.

{kind=link}
{kind=link}
{kind=link}
Suggested classification scheme for interval training based on exercise intensity.
Conclusions
This meta-analysis has identified that HIIT has more physiological benefits than MICT in patients with lifestyle-induced cardiometabolic disease. HIIT significantly improved CRF by almost double that of MICT (19.4% vs 10.3%). This should translate into greater decreases in risks of morbidity and all-cause mortality. Incorporation of HIIT into a rehabilitation programme may be a more achievable way for people with chronic disease to reach a level of exercise that promotes health enhancing benefits. These findings suggest that future exercise guidelines for lifestyle-induced cardiometabolic disease should incorporate HIIT. There are various logistical considerations that contribute to the feasibility of a HIIT programme; however, if participants are adequately screened and the programme is prescribed and supervised by appropriately trained and qualified individuals, then it should be an achievable training option.
What are the new findings?
-
High-intensity interval training (HIIT) is superior to moderate-intensity continuous training in improving cardiorespiratory fitness in lifestyle-induced cardiometabolic diseases.
-
HIIT is well-tolerated, safe and improves the quality of life.
-
Central and peripheral adaptations are responsible for the superior benefits of HIIT.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors KW designed the search criteria, conducted the search, performed the statistical analysis, and drafted and revised the paper. UW assisted in the search and revised the drafted paper. JC assisted in designing the search criteria and revised the drafted paper and is the guarantor.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.