Article Text

Abstract
Background Changes in the organisation of chronic healthcare, an increased awareness of costs and challenges of low adherence in cardiac rehabilitation (CR) call for the exploration of more flexible CR programmes as alternatives to hospital-based CR (H-CR). A model of shared care cardiac rehabilitation (SC-CR) that included general practitioners and the municipality was developed. The aim of this study was to analyse the cost utility of SC-CR versus H-CR.
Methods The cost-utility analysis was based on a randomised controlled trial of 212 patients who were allocated to SC-CR or H-CR and followed up for 12 months. A societal cost perspective was applied that included the cost of intervention, informal time, healthcare and productivity loss. Costing was based on a microcosting approach for the intervention and on national administrative registries for the other cost categories. Quality-adjusted life years (QALYs) were based on the EuroQol 5-Dimensions measurements at baseline, after 4 months and after 12 months. Conventional cost-effectiveness methodology was employed to estimate the net benefit of SC-CR.
Results The average cost of SC-CR was 165.5 kDKK and H-CR 163 kDKK. Productivity loss comprised 74.1kDKK and 65.9 kDKK. SC-CR cost was an additional 2.5 kDKK (95% CI −38.1 to 43.1) ≈ (0.33; −5.1 to 5.8 k€) and a QALY gain of 0.02 (95% CI −0.03 to 0.06). The probability that SC-CR would be cost-effective was 59% for a threshold value of willingness to pay of 300 kDKK (k€40.3).
Conclusion CR after shared care model and H-CR are comparable and similar in socioeconomic terms.
Trial registration number NCT 01522001; Results.
- cardiac rehabilitation
- acute coronary syndrome
- cost-utility
- shared care
- randomised controlled trial
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Cardiovascular disease (CVD) is a global leading cause of productivity loss. Cardiac rehabilitation (CR) facilitates recovery after CVD, but CR is challenged by low adherence even if CR reduces mortality after percutaneous coronary intervention.
What does this study add?
This is the first report of cost utility between shared care CR and hospital-based CR in a randomised design that explores the new structure of healthcare in Denmark in which primary care and the municipality are joined in handling the task of chronic healthcare.
How might this impact on clinical practice?
CR after shared care model and hospital-based CR are comparable and similar in socioeconomic terms. Less focus on the setting and an increased attention on returning to the labour market potentially could reduce productivity loss and hence reduce the total costs to CR.
Introduction
Cardiovascular disease (CVD) is globally the leading somatic cause of loss of productivity. In 2020, CVD is expected to be responsible for the loss of approximately 150 million disability-adjusted life years.1
Cardiac rehabilitation (CR) should facilitate physical and emotional recovery and enable patients to achieve and maintain better health through a combined programme of exercise, education and psychosocial support, leading to lifestyle moderation and adherence to recommended pharmacotherapy.2 Meta-analyses pooling the results of randomised trials on exercise-based CR during the last 40 years show a reduction in mortality, morbidity, reinfarction and readmissions.3 When solely addressing CR after percutaneous coronary intervention (PCI) in trials done during the modern era of cardiology, only a reduction in mortality is seen.4 However an increased pressure to offer CR to more patients with different CVDs and the potential for improving referral and utilisation of CR call for an exploration of more flexible CR programmes.5–8
The recent development of the healthcare system has been characterised by centralisation of care, with larger hospital units focusing on acute and highly specialised treatment in Denmark and other Western countries.9 The task of chronic care, disease prevention and rehabilitation is based on more out-of-hospital treatment in primary healthcare by general practitioners (GPs) supported by the newly established public municipal healthcare centres in Denmark, which offer lifestyle modification programmes. The available community-based programmes have the potential to widen access to and participation in CR, hence improve uptake and adherence. Furthermore, these programmes could be a less costly alternative for healthcare economies than the more traditional hospital-based approach.10
Based on the new organisation of chronic care in Denmark, a shared care programme for phase II CR (SC-CR) was established at seven municipalities in the Central Denmark Region, and the adherence to and efficacy of SC-CR were compared with hospital-based CR (H-CR) after hospital admission for acute coronary syndrome (ACS) in a randomised controlled trial.11 Economic evaluations of community-based CR have not previously been reported.12–14 The objective of this study was to assess the cost utility of SC-CR versus H-CR in patients with ACS from a societal perspective.
Methods
Study design and population
The study was designed as an open 1:1 randomised controlled trial to compare SC-CR in seven municipalities with H-CR at three hospitals in the Central Denmark Region. The participants in this trial included 212 patients between 18 and 80 years who had been admitted with ACS and with no prior participation in CR. Detailed information on the trial’s inclusion and exclusion criteria and on the clinical results has been published previously.11 15 We found adherence to phase II CR high in both groups, but SC-CR did not improve adherence or efficacy.15 Randomisation was computer-generated and stratified by hospital to ensure equal distribution of SC-CR and H-CR at each hospital. Of the 212 patients, 106 were randomised to the SC-CR arm and 106 to the H-CR arm. All patients were offered 12 weeks of CR and were followed up for 1 year.
Intervention
SC-CR
In SC-CR, the GP played a more prominent role in phase II CR than in the hospital-based model, but the same level of lifestyle moderating was offered. After the initial visit at the hospital for clinical assessment and risk factor evaluation by a cardiologist, the GP managed the risk factors for CVD and pharmacological treatment. All patients were encouraged to consult their GPs a few weeks after discharge and at the end of the phase II CR programme. The municipal healthcare centres provided courses on smoking cessation, nutrition and exercise training, and contributed to disease education and psychosocial support. Details of the components of SC-CR are shown in table 1.
Components of shared care cardiac rehabilitation in the different municipalities
H-CR
The H-CR was performed entirely within the hospital outpatient clinics and included smoking cessation, nutrition, exercise training, disease education, psychosocial support plus risk factor evaluation and pharmacotherapy by educated staff. Details of the components of H-CR are shown in table 2.
Components of hospital-based cardiac rehabilitation in the different hospitals
Costs
Resource use was measured from a societal perspective, and opportunity costs were used to estimate the average cost of providing the intervention. The societal perspective was made up of CR provision cost, healthcare use in primary care and in hospitals, and productivity losses due to inability to participate in the labour force.
In H-CR, rehabilitation is considered a part of outpatient care, and hence the cost is included in the national registries. A microcosting approach was used to calculate the cost of SC-CR except for the formal visits to GPs and cardiologists, which were informed from national registries.
The intervention includes the cost of both the formal and informal time of all persons involved. The cost of staff formal time was loaded with a factor of 1.5 to account for non-productive time obtained by interviewing the individuals involved in the rehabilitation programme. Their productive time was assumed to amount to 45 min of each hour (load of 0.25) due to pauses, walking distance between locations, private time and others. The remaining load (0.25) was considered to include absence from work due to vacation, sickness, participation in seminars and educational courses, and others.
The valuation of formal care was based on the average gross salary of the professionals. A standard overhead rate of 3.1% (the formal rate for the Central Denmark Region) was applied to account for capital costs. The valuation of patients’ informal time was undertaken using the opportunity cost method, in which the value of a person’s time is reflected by his or her wage rate. National average gender-matched and age-matched salaries were used to value the leisure time (net salary) and productive time (gross salary).16
The patients’ time in CR was calculated as the number of patients participating in each CR component multiplied by the course duration. Transportation times and modes of travel to the centres (GP, hospital, municipality) were recorded. The government tariff for transportation by private car for 2013 was used.
Data on primary healthcare use (number of visits and the related activity-based tariffs) were extracted from the National Health Insurance service register,17 and the data on the use of secondary healthcare services (number of services and national average diagnostic-related grouping tariffs) were extracted from the National Patient Registry.18
The DREAM database, which contains information on all social benefits, was searched for events of inability to work. Productivity losses are due to sickness leave, early pension and reschooling, and were calculated using weeks of inability to work. Complete data on costs were obtained from administrative national registers with full coverage, and all cost estimates were adjusted for time preference and inflated to the common price year of 2013, using the consumer price index where relevant.
Effect parameter
The EuroQol 5-Dimensions (EQ-5D) three-level questionnaire was administered at baseline and at 4 and 12 months of follow-up.19 Danish preference weights were used to convert responses into single indices of health-related quality of life.20
To avoid loss of information on effect parameters, the missing values were imputed by a mean within each randomisation group. Furthermore, sensitivity analysis was conducted for the alternative analytical choice of carrying the baseline observation to impute missing values after 4 months and carrying the 4-month follow-up observation to impute missing values at 12-month follow-up.
Quality-adjusted life years (QALYs) were estimated as the area under the health utility curve over time using linear interpolation between observations or between the last observations, and zero if missing data of an individual were due to death. The linear interpolation method in QALY estimation was selected because it is the most commonly used approach in the cost-effectiveness analysis (CEA) literature and due to the negligible difference between baseline EQ-5D scores.21
Statistical methods
Baseline characteristics were summarised using conventional summary statistics. Resource use, costs, health-related quality of life, QALY and net benefit of SC-CR over H-CR were analysed using arithmetic means with bootstrapped SEs.22 Non-parametric bootstrapping with 10 000 replications was applied due to the skewed nature of individual parameters, and a general significance level of 0.05 was used.
The analytical strategy was implemented for two scenarios: cases with complete response and all cases based on an imputed data set in which the missing values of health-related quality of life were imputed with the mean within the randomisation group. The latter scenario was considered the main analysis. All analyses were conducted in STATA V.13.
Cost-utility evaluation
We estimated the net benefit using a range of hypothetical threshold values for decision-makers’ willingness to pay for a QALY (from 0 DKK to 500 000 DKK) since Denmark does not have a formal threshold, and presented the probability of the intervention being cost-effective in a cost-effectiveness acceptability curve (CEAC).23 24 The analysis was repeated for alternative scenarios in a sensitivity analysis by (1) conducting an alternative strategy for imputation of missing values on effect parameters and (2) analysing costs from a healthcare perspective.
Ethical consideration
The study was conducted in accordance with good clinical practice and the ethical principles described in the Helsinki Declaration. All participants provided written informed consent.
Results
Baseline characteristics
Table 3 details the baseline characteristics of the randomisation groups. The study population consisted of 75% men with a mean age of 60. There was no statistical difference regarding baseline characteristics between groups. The transportation time for the SC-CR group was on average 19 min to the municipality, whereas it took about 26 min for the H-CR group to reach the hospitals.
Baseline characteristics of study population
Resource use and cost
The provision of CR in the shared care group was estimated to incur an average cost of 1721 DKK based on the microcosting analysis (table 4).
Resource use and cost of cardiac rehabilitation in the shared care arm
Table 5 details the estimated mean of patients’ informal time and number of trips, as well as resource utilisation. The patients’ time in transportation and the number of trips to the centre were statistically higher in the hospital group than in the shared care group. The SC-CR group had more visits to a GP than the hospital group, while the hospital group had more visits to outpatient clinics. The other differences in resource use between the two groups were not statistically significant (table 5).
Resource use during 1-year follow-up
Table 6 shows the mean cost during the 12 months of follow-up. The total costs were highest for SC-CR with 165.5 kDKK versus H-CR 163 kDKK, with 95% CI of −38.1 to 43.1 kDKK. The difference was 2.5 kDKK (95% CI −38.1 to 43.1) ≈ (0.33; −5.1 to 5.8 k€), which is 1.5%. The patient-borne costs (informal time, transportation, productivity loss) was highest for SC-CR with 78.5 kDKK and for H-CR 71.5 kDKK, with a difference of 7.0 kDKK. Costs to productivity loss made up the majority of the patient-borne costs (SC-CR vs H-CR: 74.1 vs 65.9 kDKK). The costs of the patients’ time in transportation and the patients’ transportation costs were significantly higher in the H-CR arm. Concerning outpatient visits, the H-CR group incurred an extra cost of 3849 DKK (€517) as compared with the SC-CR group, which was the biggest significant cost difference between the groups. No difference with regard to hospital admission and the number of bed days was found between the two groups; the average cost per patient of H-CR was 3.2 kDKK (k€0.4) (95% CI −21.0 to 14.7 kDKK) more than SC-CR. Concerning production losses, the SC-CR group incurred an excess production loss cost of 8.2 kDKK (k€1.1) (95% CI −23.2 to 39.6 kDKK) compared with the H-CR group; however, the difference was not statistically significant.
Costs during 12 months’ follow-up (DKK) (€1=7.45 DKK)
Health outcomes
The results showed that health scores in both groups declined from baseline to 4 months after intervention and improved marginally at 12 months, with a QALY gain in the SC-CR group of 0.02 (95% CI −0.03 to 0.06) (rounded off) compared with the H-CR group (table 7). The imputation-based analysis showed similar results.
Health outcomes
Cost utility
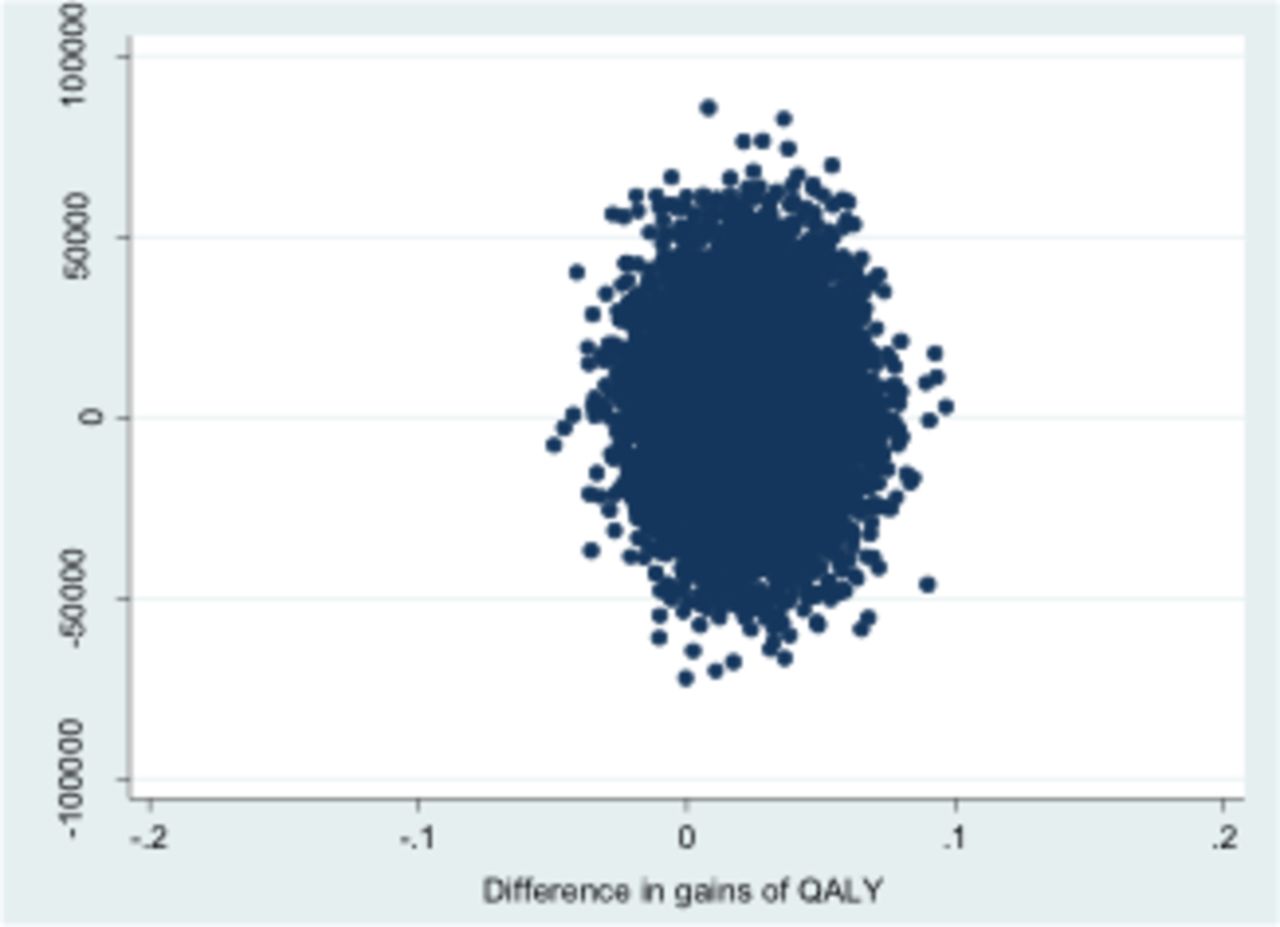
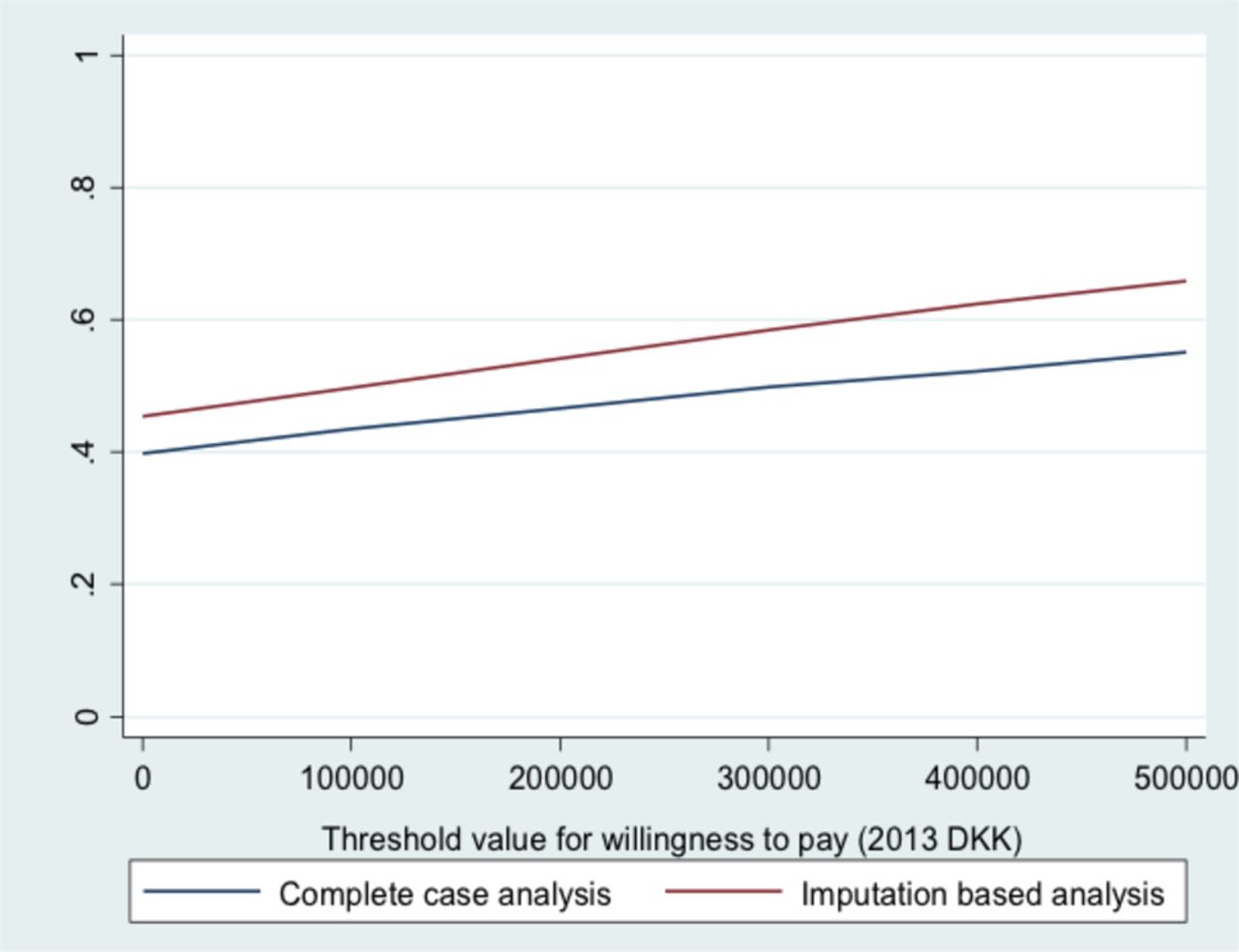
The statistical variation surrounding the results is illustrated in the cost-effectiveness plane in figure 1. Figure 2 shows the probability of the intervention being cost-effective on a continuum of hypothetical threshold values for decision-makers’ willingness to pay for an additional QALY. At a willingness to pay of 300 kDKK (k€40.3), there is 59% probability that SC-CR is more cost-effective than H-CR.
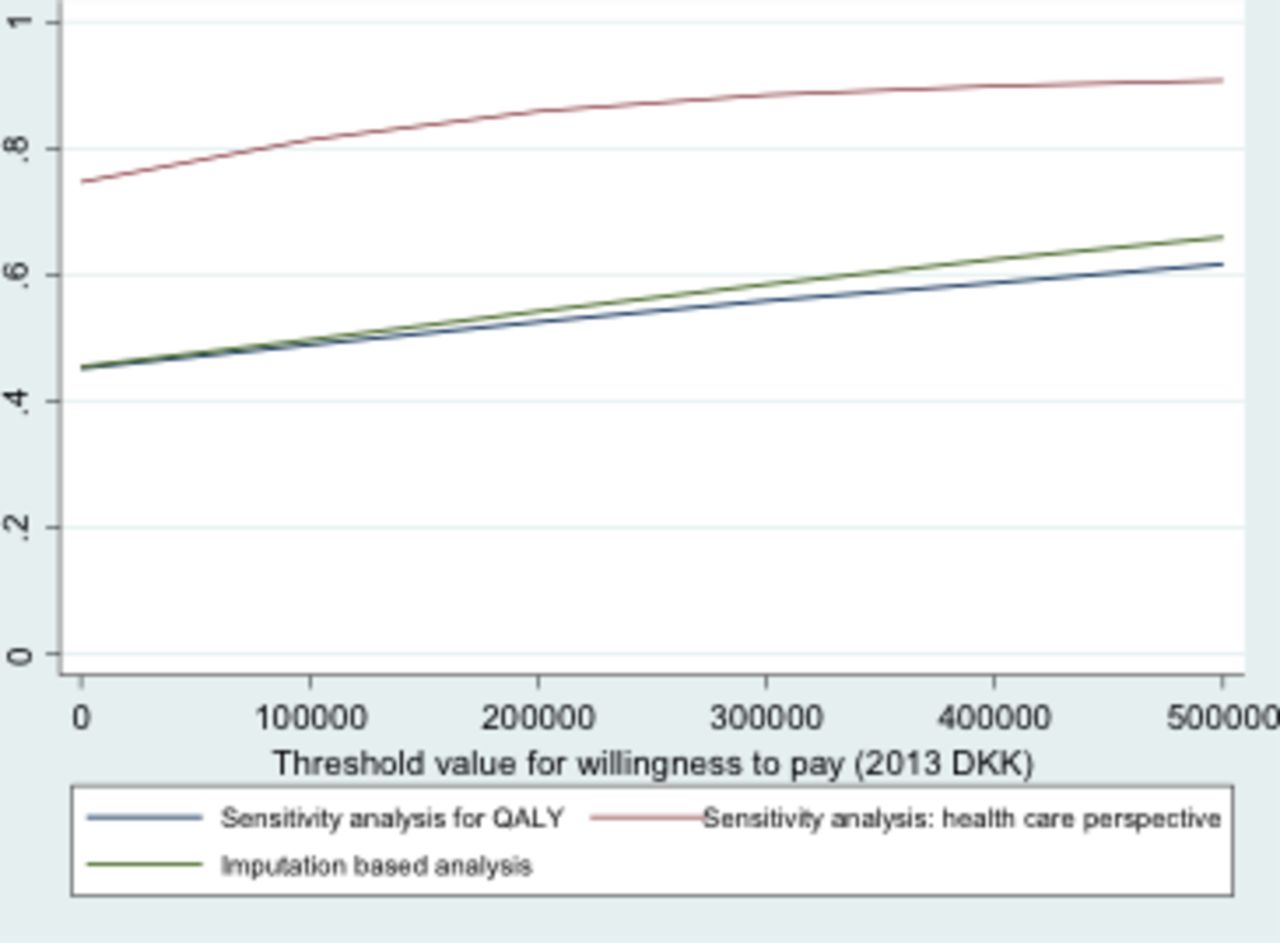
The results of sensitivity analysis for complete case analysis and alternative imputation strategy of the last observation carried forward supported the robustness of the main findings. Analysis based on costing from a healthcare perspective increased the probability of cost-effectiveness by 29%, as shown in figure 3.

Consequences of shared care cardiac rehabilitation. Bootstrapped difference in costs and quality-adjusted life years (QALY).
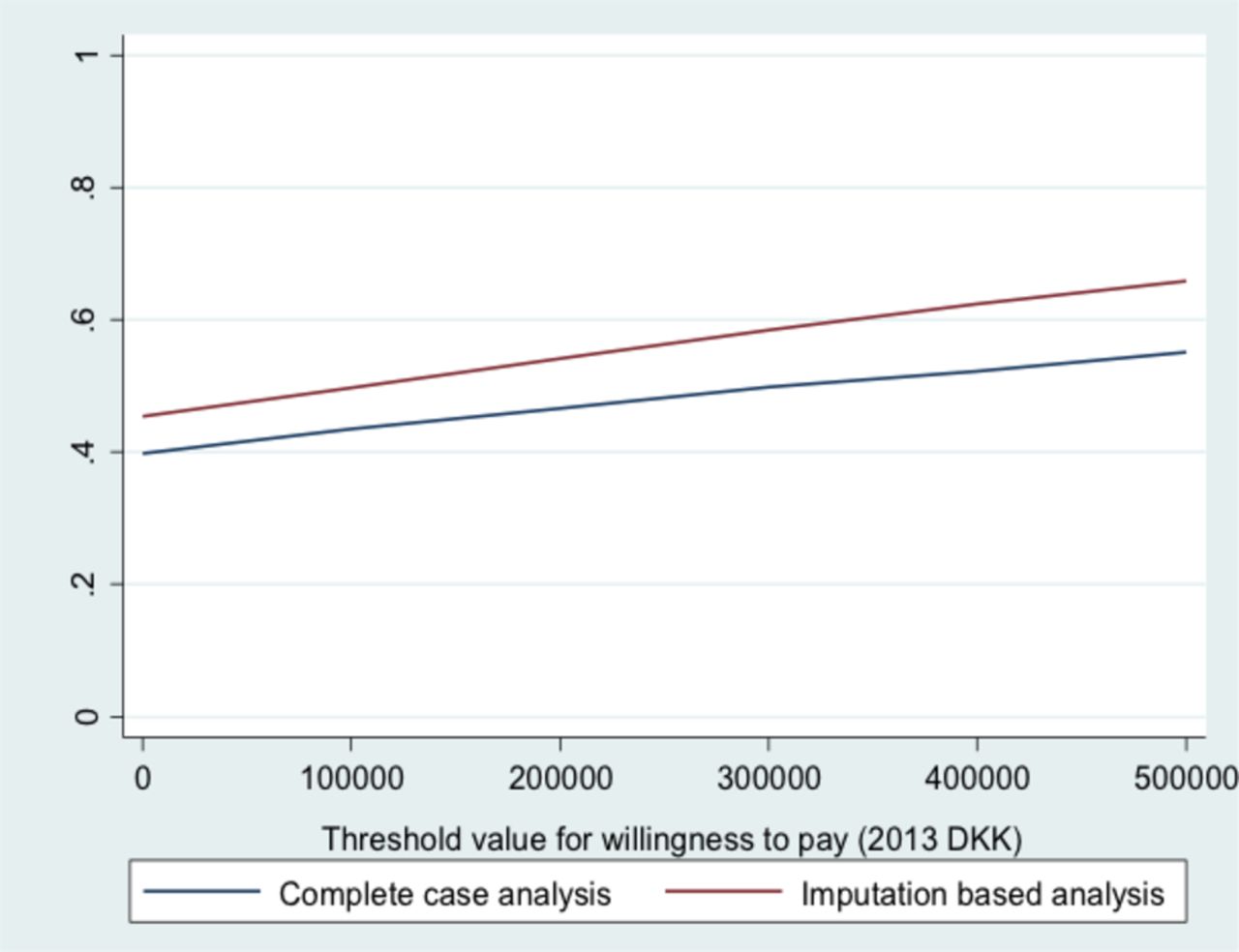
The probability that shared care cardiac rehabilitation will be cost-effective over hospital cardiac rehabilitation.

{kind=link}
{kind=link}
{kind=link}
The probability of cost-effectiveness for alternative analytical scenarios. QALY, quality-adjusted life years.
Discussion
SC-CR and H-CR after ACS seemed comparable in socioeconomic terms. The cost of SC-CR was an additional 2.5 kDKK (95% CI −38.1 to 43.1), with a QALY gain of 0.02 (95% CI −0.03 to 0.06), compared with H-CR. As expected, SC-CR had higher costs for formal GP visits and lower costs for transportation and outpatient visits. SC-CR incurred a higher productivity loss.
To our knowledge this was the first report that compared cost utility between H-CR and SC-CR in a randomised design that exploited the new structure of healthcare in Denmark. A recently published study by Dehbarez et al reported the learning and coping strategies were unlikely to be cost-effective compared with standard education in CR because of an average additional cost of 6 kDKK (€811) and a statistically insignificant gain in QALY of 0.005.25 Papadakis et al26 in a systematic review showed that CR reduced the costs compared with usual care; however, the review was made in a general cardiac population before PCI was systematically performed and at a time when data on CR outside hospitals were limited.
Other studies have compared the costs of H-CR and home-based CR after PCI. Taylor et al27 found that running a home-based rehabilitation programme costs less than a hospital-based programme (−€44 per patient), and the difference was largely the result of reduced personnel costs. Over the 9 months of the study, no significant difference was seen between the two groups with regard to overall healthcare costs. Jolly et al,28 however, found the average cost of home-based rehabilitation to be greater than hospital-based rehabilitation (£198 vs £157). When costs for patient travel and time were included, the cost for hospital rehabilitation rose close to that of the home programme (£157–£181). In the first reported study that included patients older than 80 years, Marchionni et al29 found both lower costs and prolonged positive clinical effects of home-based CR compared with H-CR and suggested that home-based CR be chosen for low-risk older patients. Our study addressed patients with ACS after coronary angiography, all of whom were at low risk, and the intervention of SC-CR was performed in the local community, limiting transportation time and limiting costs to outpatient visits; however, this difference was balanced by increased costs of primary healthcare.
The intention of CR was that a rather short investment in a patient’s health would lead to a profit, with reduced health costs in the long term. The comparison of long-term costs showed a 3-year net savings when usual care was compared with a hospital-based 1-year lifestyle modification programme for patients with symptomatic coronary heart disease among Medicare beneficiaries.30 A Belgian study found CR to be cost-effective, with €636/patient less in the CR group than in the control group not receiving CR after 4.5 years’ follow-up.31
We found a great variation in productivity loss and a tendency towards a higher productivity loss in the SC-CR group that seemed to be caused by a longer period of sick leave, early retirement or reschooling. The cause of this difference is unclear. Biering et al32 found patients’ self-rated health 4 weeks after PCI to be a stronger predictor for return to work than left ventricular ejection fraction in a Danish study of return to work after elective and acute PCI among patients younger than 67 years. This may imply the importance of psychosocial support in CR. We found no difference in self-rated health between the two groups in our study. This may be related to the main difference between the groups being the organisation of care, whereas the components in the programme were identical.
Strengths and weaknesses
The strength of our study was the meticulous selection of eligible patients, who were considered fully revascularised, with an ejection fraction ≥40% when starting CR, plus the comprehensive healthcare costing and the high EQ-5D response rates. Also, the microcosting approach including the time cost of the patients was considered a strength of the study. Data were available for the experimental SC-CR and microcosting was applied. We mimicked the methodology for the development of formal tariffs in order to preserve internal validity. However we cannot rule out that a future, routine-based tariff will be lower if learning curve aspects, economies of scale and others affect productivity of SC-CR provision.
A weakness of the study was its power, primarily regarding the major clinical endpoints like mortality, morbidity and continued ability to work. Regarding economy, the observed differences between the two strategies were so small that even a very large study would be unlikely to reach a different result. We found no difference in our primary outcome in the clinical trial,15 programme adherence, and whether CR was conducted at the hospital or in shared care. A study of 212 patients introduced susceptibility for higher costs due to adverse events (eg, infection in prosthesis), and the inclusion of both different hospitals and of different municipalities meant that there were small differences in the rehabilitation courses. General measures of quality of life like the EQ-5D may be less sensitive than disease-specific instruments. Also, the EQ-5D had some ceiling effect, being less sensitive at detecting changes towards the top of the scale.33 34 Due to the exclusion of heart failure and very elderly patients, care had to be taken when these patients were compared with other patients. The bootstrapping procedure was based on independent draws from costs and outcomes, ignoring correlation between costs and outcomes. Due to the large CIs around cost and QALY, one should interpret the CEAC with caution. It might be wise to invest in rather additional research to reach a firm decision to implement the rehabilitation programme.35
Using age-matched and gender-matched average salaries to value patient time is a conventional methodological choice in order not to conflict with equity. If the study population is less active at the labour market than the age-matched and gender-matched general population, it is likely that we have overestimated their time value. Given that the SC-CR group spends less time on transportation but demonstrates a relatively heavier tendency for more sick leave, this is a potential bias against H-CR.
In conclusion, CR after shared care model and H-CR are comparable and similar in socioeconomic terms. Increased attention in reducing productivity loss potentially could reduce costs.
References
Footnotes
Contributors JBB, KLC, BC, JR and HK designed the RCT. RS, NTD, BC, KLC and JBB designed the economic evaluation. NTD drafted the method and results sections. JBB has made the first complete paper draft. All authors contributed to the final manuscript.
Funding The study was financed by a grant from the Danish Heart Association.
Competing interests None declared.
Ethics approval The Central Denmark Region Committees on Biomedical Research Ethics (j.nr. M-20110135) and the Danish Data Protection Agency approved the study protocol (j.nr. 2011–41-6533 changed to 2014–41-3342 in 2014).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.