Article Text

Abstract
Introduction Prehospital providers are at increased risk for psychological distress. Support at work after critical incidents is believed to be important for providers, but current guidelines are in need of more scientific evidence. This study aimed to investigate: (1) to what extent prehospital providers experience support at work; (2) whether support at work is directly associated with lower distress and (3) whether availability of a formal peer support system is related to lower distress via perceived colleague support.
Methods This cross-sectional study surveyed prehospital providers from eight western industrialised countries between June and November 2014. A supportive work environment was operationalised as perceived management and colleague support (Job Content Questionnaire), availability of a formal peer support system and having enough time to recover after critical incidents. The outcome variable was psychological distress (Kessler 10). We conducted multiple linear regression analyses and mediation analysis.
Results Of the 813 respondents, more than half (56.2%) were at moderate to high risk of psychological distress. Participants did not consistently report support at work (eg, 39.4% were not aware of formal peer support). Perceived management support (b (unstandardised regression coefficient)=−0.01, 95% CI −0.01 to 0.00), having enough time to recover after critical incidents (b=−0.07, 95% CI −0.09 to −0.04) and perceived colleague support (b=−0.01, 95% CI −0.01 to 0.00) were related to lower distress. Availability of formal peer support was indirectly related to lower distress via increased perceived colleague support (β=−0.04, 95% CI −0.02 to −0.01).
Conclusions Prehospital providers at risk of psychological distress may benefit from support from colleagues and management and from having time to recover after critical incidents. Formal peer support may assist providers by increasing their sense of support from colleagues. These findings need to be verified in a longitudinal design.
- paramedics
- psychological conditions
- prehospital care, basic ambulance care
Statistics from Altmetric.com
Key messages
What is already known on this subject?
Previous studies showed that paramedics and other prehospital providers are at increased risk for psychological distress compared with other first responders (eg, police officers, firefighters) and the general population.
Guidelines for psychosocial care of first responders emphasise the importance of a supportive work environment, but are predominantly based on expert consensus and further scientific evidence is required.
What this study adds?
This survey of prehospital providers from multiple western countries shows concerning levels of distress within this population and also suggests the importance of understanding support at work after critical incidents.
Formal peer support systems, having time to recover after critical incidents, informal management and colleague support appear to be associated with lower distress.
Introduction
Prehospital providers are regularly exposed to emotionally charged situations, such as severely injured or critically ill people, the death of a child, violence and suicide.1 2 Most of the time, they cope with these challenges effectively; however, a significant proportion are at risk of developing psychological problems, including anxiety, depression, burnout, post-traumatic stress disorder (PTSD) and sleep difficulties.2–4 Among first responders (eg, police, firefighters and ambulance personnel), prevalence of PTSD is the highest in prehospital providers, possibly due to more frequent exposure to life-threatening incidents (driving from one incident to another, with only brief moments of rest) and few resilience-based selection criteria for employment.5
Evidence-informed guidelines for psychosocial care for first responders involved in critical incidents emphasise the importance of a supportive work environment.6–9 This environment entails a work climate in which first responders feel supported by management and colleagues, formal peer support systems (ie, a formal organisational structure through which trained colleagues offer support after a critical incident) are available and workers at risk of psychological problems are identified, monitored and referred to professional care when needed. Receiving time off to recover from stressful incidents at work is another supportive intervention that appears to be beneficial for prehospital providers’ well-being.8 Time to recover following a critical incident can be granted formally by management or occur informally during the normal work day (eg, having a break between incidents),8 thereby creating an opportunity to foster social support among colleagues.
Previous research showed that frequent exposure to critical incidents, in combination with organisational stress, is an important risk factor for prehospital providers’ psychological health.2 9 10 In contrast, perceived support at work, such as getting along with colleagues, may have a positive influence on well-being.2 9 10 However, whether prehospital providers feel supported in the wake of critical incidents specifically has not yet been studied. In addition, it remains uncertain whether supportive interventions stressed by the guidelines, such as formal peer support structures, have become widely available to prehospital providers.6 7 11 Moreover, these guidelines are predominantly based on expert consensus and little is known about the protective influence of these supportive interventions.12 In particular, the mechanisms through which formal peer support systems influence distress needs more attention.
The primary aim of this study was to investigate to what extent prehospital providers experience a supportive work environment after critical incidents and whether such an environment is associated with lower distress. Building on previous research, we expected to find a negative relationship between a supportive work environment and distress. Finally, we examined whether availability of a formal peer support system was related to lower distress via increased perception of support from colleagues. In particular, since formal peer support is given by trained colleagues, we expected that the relationship between availability of formal peer support and distress would be mediated by perceived colleague support.13
Methods
Study design and settings
This cross-sectional study surveyed prehospital providers from eight western industrialised countries (Australia, Austria, Canada, Germany, New Zealand, Switzerland, UK and USA). The study was conducted in the context of a multinational project on delivering psychosocial care to child patients. As part of this project, we sought to find out more about practitioners’ general health and own psychosocial support.
Participants
We recruited participants via ambulance organisations, unions, university departments of emergency care and other professional associations. We contacted these organisations by email and asked them to distribute the questionnaire to prehospital providers. Providers were also encouraged to distribute the questionnaire to colleagues. Respondents were excluded if they were no longer working as a prehospital provider or submitted an incomplete response. To reduce any barriers to providing a frank account of distress and organisational support, the study design guaranteed complete anonymity for individuals and organisations. For this reason, we were unable to determine response rates. Providers filled out the questionnaire between the end of June 2014 and the beginning of November 2014. Consent was inferred from full completion of the questionnaire. Respondents could opt to go into a draw for one of five $20 Amazon gift vouchers.
Measures
Online supplementary appendix 1 provides a copy of the questionnaire. The questionnaire consisted of a recently developed measure regarding provision of psychosocial care to children (see Alisic et al (2017) for details),14 validated measures on distress and perceived support and some purposely generated items regarding practitioners’ own psychosocial support. All items were pilot tested with providers, ambulance management staff and topic experts. The questionnaire was available in English and accessed through the online platform Survey Monkey (http://www.surveymonkey.com). The measures relevant to this investigation are described below. Participants also had the opportunity to leave comments in seven open-ended questions about prehospital providers’ experiences providing psychosocial care for injured children.
Supplementary file 1
Outcome: psychological distress
Psychological distress was measured with the Kessler 10 (K10),15 which is one of the most widely used short scales to screen for distress,15 identifying symptoms of anxiety and depression. This instrument has strong psychometric properties, good power in discriminating psychological problems from non-cases16 and had high internal consistency in this study sample (Cronbach’s α=0.92). The K10 comprises of 10 items rated from ‘none of the time’ (1) to ‘all of the time’ (5) for how often the item applied to participants in the previous 30 days. Higher scores represent more psychological distress, from medium risk (scores 16–29) to high risk (scores 30–50).
Predictors: support and demographics
Perceived management support (four items) and perceived colleague support (four items) were measured with items based on the Job Content Questionnaire (JCQ) subscales ‘Supervisor Support’ (four items) and ‘Co-worker Support’ (four items).17 The JCQ has good psychometric properties, has been used with a variety of professions18 and had high internal consistency in this sample with Cronbach’s α=0.83 (colleague support) and 0.94 (management support). Based on feedback from paramedics when field testing the survey, several items were tailored to the context of critical incidents (online supplementary appendix 2 shows the original and adjusted items). Sum scores ranged from 4 to 16 with higher scores representing higher perceived support. The items used a 4-option response format: ‘totally disagree’ (1) to ‘totally agree’ (4). Two items were measured dichotomously: ‘I have enough time to recover from distressing incidents at work’ (response options: ‘agree’ and ‘disagree’) and ‘Does your ambulance service have trained peer support officers?’ (response options: ‘yes’ and ‘no’).
Supplementary file 2
Demographic characteristics included gender, age, years of work experience, country or region and having children under the age of 17 years old. We also asked about whether the participant had received professional support after critical incidents, such as external or in-company counselling from a social worker, trained peer-supporter or psychologist, with the following item: ‘Have you received any professional support following a critical incident’ (response options: ‘yes’ and ‘no’).
Statistical analysis
Data were exported from Survey Monkey into IBM SPSS V.22. We performed mean imputation for 15 missing values spread uniformly across the data matrix (0.2% of all values). The total scores on the K10 were slightly positively skewed, as is expected with psychological symptom measures in a general population and had two extreme outliers (scores of 50 and 48). A logit transformation did not improve normality, but resolved the outliers and was used for univariate analyses and regression analyses. As log-scores are less intuitive to interpret but correspond to the original values of the K10, we also report the non-transformed mean values.
To assess univariate associations between distress and the other variables in the study, we used bivariate correlations (Pearson’s), independent sample t-tests and one-way between subjects analysis of variance (ANOVA) (with a posthoc Bonferroni test).
We tested six multiple linear regression models to examine which indicators of a supportive work environment predicted distress, using the following covariates: gender, age, years of experience, country/region, having children under 17 years old and receipt of professional organisational support. A model with the covariates was followed with models with the covariates and one predictor (perceived management support, perceived colleague support, having time to recover or availability of a formal peer support system) and a final model that included the covariates and all of the predictors. The variance inflation factor and tolerance statistic did not indicate a problem with multicollinearity.
We tested the hypothesised mediation effect of colleague support with PROCESS: an add-on for SPSS for statistical mediation process analysis.19 Mediation refers to a situation when the relationship between a predictor (availability of a peer support system) and an outcome variable (distress) can be explained by their relationship to a third variable, the mediator (perceived colleague support). Mediation is said to have occurred if the strength of the relationship between the predictor and outcome variable is reduced by including the mediator. If mediation could not occur because of the absence of a direct effect between the predictor and outcome variable, we tested for an indirect effect in order to fully explore potentially useful mechanisms.20 An indirect effect exists when predictor and outcome variable are not related directly, but they are indirectly related through significant relationships with a linking mechanism (ie, colleague support). To test mediation and indirect effects, PROCESS uses bootstrapping: a technique from which the sampling distribution of a statistic is estimated by taking repeated samples of the dataset. It assesses the CI of the indirect effect and the size of the indirect effect.19 The CI for the unstandardised indirect effect is a BCa (bias corrected and accelerated) bootstrapped CI based on 10 000 samples. If the CI does not contain zero, a significant indirect effect has occurred. The size of the indirect effect is measured with standardised regression coefficients and kappa-squared (κ2).
Results
In total, 813 prehospital providers participated in this study. Most self-identified as paramedics (77.5%) or emergency medical technicians (18.9%); demographic characteristics are presented in table 1. About half of the participants (48.7%) were at moderate risk of psychological distress and 7.5% were at high risk. With a possible maximum score of 16, participants experienced more support from colleagues (mean=12.5, SD=0.08) than from management (mean=9.7, SD=0.12): mean difference=2.8, 95% CI 2.6 to 3.0. For example, 47.6% disagreed with the statement that their management was supportive of staff after critical incidents, while 18.1% disagreed with the statement that their colleagues were supportive. The majority (59.5%) indicated that they had not had enough time to recover after a critical incident. Most participants (60.6%) were aware of a peer support system in their organisation and almost half (46.9%) had used some form of professional support after a critical incident (table 1).
Sample characteristics (n=813)
Several participants commented on how stress was viewed within their service. For some, experiencing distress was seen as a normal part of the job, something that you have to deal with: ‘When we work with injured children it can be stressful, but that stress is part of the job. You either learn to handle it or find another line of work.’
Others remarked on the culture of not talking about stress: ‘I don’t know any paramedic that doesn’t find child trauma calls the most stressful, but paramedics have a history of not asking for help to deal with it!’
Regarding the availability of social support, some strong comments were made: ‘I can barely take the mental load anymore. Managers are unsupportive and create a negative atmosphere coupled with being surrounded by disaster. How can I offer support [---] when we can’t even take care of ourselves?’
Direct relations between support and distress
Univariate analyses showed that prehospital providers reported less distress with greater perceived management support (r=−0.42, 95% CI −0.48 to −0.36) and perceived colleague support (r=−0.27, 95% CI −0.34 to −0.20). Those who reported not getting enough time to recover after critical incidents (mean=1.28, SD=0.15) reported higher distress than those who reported getting enough time (mean=1.16, SD=0.13): mean difference=0.12, 95% CI 0.12 to 0.15. These mean scores of distress correspond to non-transformed mean scores of 20.5 and 15.1, respectively. Those who reported that they had received professional support also reported higher levels of distress than those who had not received professional support (mean=1.25, SD=0.16 vs mean=1.22, SD=0.16; mean difference=0.03, 95% CI −0.04 to 0.00), corresponding to non-transformed mean scores of 18.8 and 17.9, respectively. Female participants reported higher levels of distress than male participants (mean=1.25, SD=0.15 vs mean=1.23, SD=0.16; mean difference=0.02, 95% CI −0.05 to 0.00), corresponding to non-transformed mean scores of 18.9 and 18.0, respectively. The results of the one-way ANOVA suggest a statistically significant difference in distress between countries and regions (P<0.001). A posthoc Bonferroni test indicated that distress was higher in Australia than in USA (mean difference=0.08, P<0.001, 95% CI 0.02 to 0.10), Western Europe (mean difference=0.11, P<0.001, 95% CI 0.04 to 0.15) and New Zealand (mean difference=0.07, P=0.022, 95% CI 0.01 to 0.13). Distress was also higher in Canada compared with USA (mean difference=0.06, P<0.001, 95% CI 0.02 to 0.10) and Western Europe (mean difference=0.09, P<0.001, 95% CI 0.03 to 0.14). Mean scores (including non-transformed values) are presented in table 2. Formal peer support, having children, age and years of experience were not associated with distress.
Mean scores of psychological distress per country/region
The results of the regression analyses are detailed in table 3. Model 1 included only the covariates (eg, country/region) and explained 6.5% of the individual differences in distress. Models 2A–2D included all covariates and each of the predictors of a supportive work environment added one at a time. Perceived support from colleagues and management and having time to recover after distressing incidents most strongly contributed to lower levels of distress. Model 3 included all covariates and all predictors and accounted for approximately one-quarter of the individual differences in distress.
Distress predicted by indicators of a supportive work environment and covariates
Indirect relation between availability of formal peer support and distress
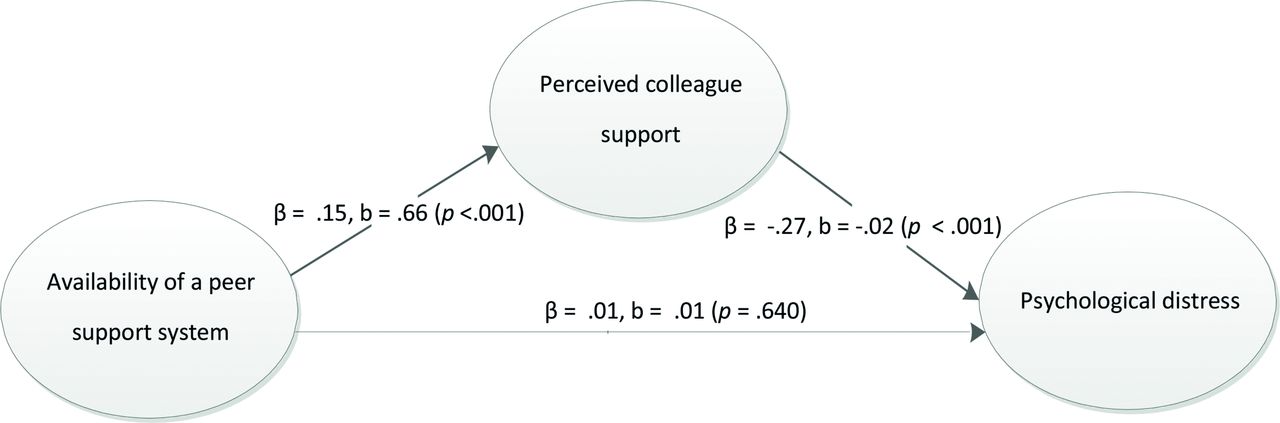
Availability of formal peer support was not directly related to distress (table 3, model 3). There was a significant indirect effect (in the absence of a direct effect20) of availability of peer support systems on distress through perceived colleague support, although the size of the effect was small (figure 1).

{kind=link}
Strength of the relationships between availability of formal peer support, psychological distress and perceived colleague support represented by standardised (β) and unstandardised (b) regression coefficients and p values. The direct effect between availability of a peer support system and psychological distress, while controlling for perceived colleague support, is presented (indirect effect β=−0.04, 95% BCa CI −0.06 to −0.02). The size of the effect was small (κ2 = 0.04, 95% BCa CI 0.02 to 0.06). The total, direct effect between availability of a peer support system and psychological distress (without controlling for perceived colleague support) is also non-significant: β=−0.02, b=−0.01, P=0.502.
Discussion
This study focused on the association between perceptions of support and distress in prehospital providers in the context of critical incidents. We found that perceiving a lack of support from management and colleagues and not having enough time to recover after critical incidents were associated with higher distress. Given that more than half of providers were at moderate to high risk of psychological distress, compared with 31% in the general population,21 studying support at work remains very important.
While most respondents reported that their organisation had a formal peer support system for critical incidents, many prehospital providers also indicated that formal peer support systems were not available and perceived that they had insufficient recovery time after critical incidents. This finding suggests that not every organisation offers the kind of support that prehospital providers may need. Alternatively, it may be that the staff surveyed were not aware of supports that may be available to them. In the prehospital setting, disclosure of mental health impacts from work and seeking support is often viewed as a sign of weakness,22 which was also described by our participants and may be another explanation of these findings. Nevertheless, in the present study, almost half of the prehospital providers had used some form of professional support after a critical incident, such as formal peer support, company counsellor or psychologist. In particular, prehospital providers with higher levels of psychological distress were more likely to report having sought professional support, suggesting that only those with higher distress seek out professional support. It may also reflect selection bias such that those who participated may have been more likely to find support an important process or were less concerned about potential stigma from seeking support, compared with the overall population of prehospital providers.
Given the cross-sectional nature of this study, it is likely that perceiving a lack of support from management and colleagues and not having enough time to recover after critical incidents are bidirectionally associated with distress and no assumptions about the direction of causality can be made. These findings are, however, in line with guidelines that suggest that support from the organisation after critical incidents and promoting well-being may help prevent the development of persistent psychological distress.6 7 11 Granting staff leave after critical incidents is a simple intervention that improves prehospital providers’ well-being.8 However, experiencing insufficient recovery time may occur in settings that have a high workload, which in itself increases risk of burnout, absenteeism and high turnover.23 In that case, spreading the workload may be the first priority of organisations to prevent distress.
The present findings, together with previous research in clinical and trauma settings, align with the social support deterioration deterrence model, such that perceived support (eg, feeling supported by others) mediates the relationship between actual supportive interventions and distress.13 In line with this model, the present study showed that availability of formal peer support systems was associated with prehospital providers’ perceptions of informal colleague support, which in turn was associated with lower distress. This indirect association shows that formal peer support mechanisms may be effective because they help create an environment in which prehospital providers feel more generally supported by colleagues after critical incidents. However, since the effect size of the indirect effect was small, more research is needed to understand the various pathways through which peer support impacts on mental health in this profession. For example, prior studies have found that formal peer support was associated with increased feelings of resilience24 and with more positive attitudes towards emotional expression of thoughts and feelings, which have been found to be associated with decreased PTSD symptomatology.25
Strengths and limitations
This study took a novel, broad approach to examine the prevalence of distress in prehospital providers and the role of perceived work support in psychological well-being. Our focus on multiple western industrialised countries and organisations offers insights into well-being beyond the limits of individual work environments, which have specific organisational and political structures and pressures that also influence worker well-being. This study, however, has some limitations. It had a cross-sectional design and therefore conclusions about causality cannot be drawn. The sample consisted primarily of western industrialised countries from Europe, USA and Australia-New Zealand and English speakers, which limits the generalisability of the findings to other countries. There could have been selection bias in regards to participation, with those more interested in psychosocial care for injured children or within their profession, being more likely to participate. Finally, we focused on mental health difficulties and did not measure resilience and growth, which may also play an important role in well-being in prehospital providers.24 Future studies would benefit from a longitudinal design and may also use in-depth qualitative methods to explore which aspects of formal peer support and time off between jobs are vital for prehospital providers’ well-being.
Conclusion
From a survey of just over 800 prehospital providers, from eight different countries, we found moderate to high levels of psychological distress. Regardless of national differences in work conditions, perceiving a supportive work environment after critical incidents (ie, feeling supported by management and colleagues and having enough time to recover after critical incidents) was found to be related to prehospital providers’ well-being. Moreover, the small indirect effect suggests that availability of formal peer support systems may benefit prehospital providers’ well-being by helping them feel generally more supported by their colleagues. While these findings should be verified in a longitudinal design, we highlight the importance of ambulance organisations’ investment in supportive work culture and programme. It would be valuable to further examine the factors that contribute to a supportive work environment following critical incidents in order to generate more evidence-based strategies to support prehospital providers.
Acknowledgments
We would like to thank all prehospital providers who have participated in the study. Our thanks also go to the many organisations and individuals who have contributed to the tailoring and distribution of the survey, including from Ambulance Employees Association Victoria, St John New Zealand and Paramedics Australasia.
References
Footnotes
Contributors JG-T participated in the acquisition of the data, conducted the main analyses, interpreted the data and drafted and revised the article. MPT contributed to the design of the study and the acquisition of the data, the interpretation of the data and the revision of the article. MJG contributed to the design of the study, the interpretation of the data and the revision of the article. NK-A and MAL contributed to the conception and design of the study, the acquisition and interpretation of the data and the revision of the article. RJK contributed to the interpretation of the data and the revision of the article. EA conceptualised and designed the study, supported the acquisition of the data, contributed to the analysis and interpretation of the data and was a major contributor to the drafting and revision of the article.
Funding EA: Early Career Fellowship (#1090229) from the National Health and Medical Research Council, Australia. MJG: Early Career Fellowship (#1036124) from the National Health and Medical Research Council, Australia. These funding sources had no role in the study design; in the collection, analysis and interpretation of the data; in the writing of the report or in the decision to submit the paper for publication.
Competing interests None declared.
Ethics approval Monash Human Research Ethics Committee (CF14/1167—2014000519).
Provenance and peer review Not commissioned; externally peer reviewed.