Article Text

Abstract
Background For several years, EDs in the UK NHS have faced considerable increases in attendance rates. Walk-in centres (WiCs) and minor injuries units (MIUs) have been suggested as solutions. We aimed to investigate the associations between practice and practice population characteristics with ED attendance rates or combined ED/WiC/MIU attendance, and the associations between WiC/MIU and ED attendance.
Methods We used general practice-level data including 7462 English practices in 2012/2013 and present adjusted regression coefficients from linear multivariable analysis for relationships between patients' emergency attendance rates and practice characteristics.
Results Every percentage-point increase in patients reporting inability to make an appointment was associated with an increase in emergency attendance by 0.36 (95% CI 0.06 to 0.66) per 1000 population. Percentage-point increases in patients unable to speak to a general practitioner (GP)/nurse within two workdays and patients able to speak often to their preferred GP were associated with increased emergency attendance/1000 population by 0.23 (95% CI 0.05 to 0.42) and 0.10 (95% CI 0.00 to 0.19), respectively. Practices in areas encompassing several towns (conurbations) had higher attendance than rural practices, as did practices with more non-UK-qualified GPs. Practice population characteristics associated with increased emergency attendance included higher unemployment rates, higher percentage of UK whites and lower male life expectancy, which showed stronger associations than practice characteristics. Furthermore, higher MIU or WiC attendance rates were associated with lower ED attendance rates.
Conclusions Improving availability of appointments and opportunities to speak a GP/nurse at short notice might reduce ED attendance. Establishing MIUs and WiCs might also reduce ED attendance.
- primary care
- emergency care systems, emergency departments
- emergency care systems, primary care
- emergency department utilisation
- statistics
Statistics from Altmetric.com
- primary care
- emergency care systems, emergency departments
- emergency care systems, primary care
- emergency department utilisation
- statistics
Key messages
What is already known on this subject?
General practice factors affecting attendance in EDs in England have previously been researched, but usually only in isolation or with a limited number of factors, or within limited geographical locations. From those studies age, gender, ethnicity, socio-economic status, deprivation, health status, timely access, satisfaction with phone access and travel distance were associated with ED attendance.
What might this study adds?
We have investigated the relationships between a wide range of practice and practice population characteristics and ED attendance rates for nearly all practices in England active in the financial year 2012/2013. After adjustment for population characteristics and location (rural/urban), our study found that the following general practitioner (GP) practice characteristics were associated with a decrease in ED attendance rate: higher percentages of patients able to make an appointment, higher percentages of patients able to see a nurse or GP at short notice, lower percentages of patients often able to speak to their preferred GP and a higher percentage of UK-qualified GPs in the practice. We also found that a higher use of alternative emergency services such as walk-in centres or minor injuries units was associated with reduced ED attendance.
Introduction
EDs in developed countries are experiencing a rise in the number of attendees.1 This increase in England is a major concern for public health and for NHS sustainability. Research findings show that many patients attending ED could be managed in general practice.2 This suggests that practice-related factors might be associated with ED attendance and that investigating them might highlight potential measures to reduce the pressure on ED.
A recent systematic review identified the following general practice factors which affect ED attendance: access to the practice, distance to an ED, socioeconomic status, timely access, satisfaction with phone access, patient age profile and chronic disease rates.3 Evidence for the effect of ethnicity and gender was mixed, and evidence for continuity of care was mainly found in foreign studies. These findings were mostly from cross-sectional studies and some studies only reported univariable associations, while others focused on specific geographic areas or patient populations by condition.
While ED attendance has increased in the past decade, the increase in minor injuries unit (MIU) and walk-in centre (WiC) attendances has been much greater.4 ,5 WiCs were introduced in 1999 to provide and improve access to primary care for minor injuries and illnesses, but gradually they began to be seen as a way to reduce pressure on EDs.6 MIUs began to appear in the UK in the mid-1990s, typically replacing small EDs, motivated by policies to move healthcare into the community and to rationalise and centralise the provision of emergency care.6 MIUs do not typically deal with patients' routine primary care needs while WiCs do. However, both can be seen either as substitutes for ED use7 or as complementary primary care services.8 ,9 Related to this issue is whether MIUs or WiCs might have led to supply-induced demand of emergency care.10 In this study, we will present MIUs and WiCs first as predictor for ED use and second as an outcome, including them with ED as part of the emergency care system.
This study's aim was to investigate relationships between practice and practice population characteristics, and ED attendances, particularly to replicate findings of a recent systematic review.3 We also address previously untested factors in a contemporary England wide context, such as provision of MIUs and WiCs, and general practitioners (GPs) composition of practices.
Methods
Study design and setting
This study used cross-sectional data from 7462 practices, accounting for 92.5% of all practices in England operative during the whole financial year 2012/2013 and for 97.2% of all practices' population.11 ,12 The excluded practices had incomplete data for one or more variables. This resulted in excluding all practices with <1200 practice population (n=123) or practices where no patients apparently attended an ED (n=33). All data were abstracted from publicly available websites and comprised aggregated practice-level data where neither patients nor GPs could be identified.
Outcome measures
In line with previous research, the first outcome measure was self-referred discharged ED attendances per 1000 practice population standardised according to age and gender at ‘major’ A&E departments (type 1; see online supplementary box S1), either with or without practice follow-up treatment. These visits were identified as likely to be suitable for treatment by another healthcare service such as a GP, MIU or WiC.13 ED attendances resulting in admission, onward referral, transfer to another provider or death were excluded.
Supplemental material
In the UK, MIU and WiC are generally classified as type 3/4 A&E departments (see online supplementary box S1). To explore the association between practice factors and a wider range of emergency care provision, the second outcome measure was a combined ED, WiC and MIU attendance rate. WiC and MIU attendances resulting from emergency service, GPs, other and unknown referrals were excluded. Data were obtained from NHS Comparators (see online supplementary box S2).11
Measures of practice characteristics
GP composition of practice
The percentage of female GPs in practice, GPs whose country of primary medical qualification is the UK (qualified in UK), and GPs younger than 40 years of age in 2012 were obtained from the Health & Social Care Information Centre (HSCIC).12
Access to practice
This study used the definitions of potential access and realised access as described by Andersen et al.14 Realised access data were based on data from the GP Patient Survey 2012–2013 (GPPS-2012-13) on patients' satisfaction with phone access, and opening hours; percentage of patients able to book a convenient appointment to see or speak with a nurse or GP and percentage of patients wanting but not able to speak to a GP/nurse within two workdays.15
Potential access data were obtained by the authors from HSCIC on the number of full-time equivalent GP providers, GP registrars and GP ‘other’ per 1000 practice population.12 Travel distance between practices and the nearest hospital was estimated using urban and rural English postcodes from the Office of National Statistics linked to GP postcodes obtained from HSCIC to identify practice locations.12 ,16 Department for Transport data were used to calculate the average difference in travel time by public transport and/or walking.17
Continuity of care
Measures of continuity of care were based on data from GPPS-2012-13 on the following: the percentage of patients having a preferred GP and of those, the percentage that could see or speak to their preferred GP always or a lot of the time.15
Measures of practice population demographics
The index of multiple deprivation (IMD) is commonly used to characterise socio-demographic profiles. However, IMD includes standardised emergency admission rates as part of the health factor in its definition.18 In this study, life expectancy was used as a health indicator as it is often used to show inequalities in health within countries, and is a more direct measure of health need in a population than the IMD. Unemployment rate was used as an indicator for economic status. Data were used from Public Health England to determine the male life expectancy among practice populations.19 Male life expectancy was used because it correlated more strongly with self-referred ED attendance rates than female life expectancy. Unemployment rates and the percentage of UK whites (ie, respondents who identified themselves with White-English, Welsh, Scottish, Northern Irish or British) among practice populations were obtained from GPPS-2012-13.15
Measures of MIU and WiC attendance
Self-referred attendance per 1000 practice population data standardised according to age and gender for both MIU and WiC were obtained from the NHS Comparators website.11 When defining the presence of a WiC near a practice, this was indicated by a WiC attendance of greater than 1 per 1000, otherwise a nearby WiC was assumed to be absent. We used an analogous definition for the presence of an MIU.
Statistical methods
Multivariable regression models, taking into account clustering by Primary Care Trust (PCT) were used to test for an association between the outcome variables of emergency care attendance and the predictors. The standardised rate of self-referred discharged ED attendance, our first outcome measure, showed a distribution close to normality (figure 1). Departure from normality was fairly modest and unlikely to undermine the results.20 The combined ED, MIU and WiC attendance, the second outcome, was not as close to normality (figure 2) as the first outcome. We have presented results for the same model to assure comparability of predictors' effects. Adjusted regression coefficients, CIs and exact p values were tabulated for each predictor. Furthermore, analysis of variance tests were performed on mean attendance rates to investigate whether presence of MIUs or WiCs were related to either ED attendance or combined ED, MIU and WiC attendance. All analyses were undertaken in Stata 13 MP2 (StataCorp, College Station, Texas, USA).

Frequency distributions of standardised ED attendance.

Frequency distributions of combined ED, minor injuries unit (MIU) and walk-in centre (WiC) attendance.
Results
Self-referred discharged ED attendance
The registered patient population at the 7462 practices made 8 208 516 self-referred ED attendances in England between April 2012 and March 2013, accounting for 63% of all ED visits (13 118 002). Of all the self-referred visits, 5 023 142 were discharged, accounting for 38% of all ED visits and 61% of all self-referred visits. Self-referred discharged rate varied hugely among practice populations: the median (IQR) was 92 (61–127) per 1000 population (table 1).
Descriptive statistics ED, WiC and MIU attendance, and general practice and practice population characteristics in England, April 2012–March 2013 (N=7462)
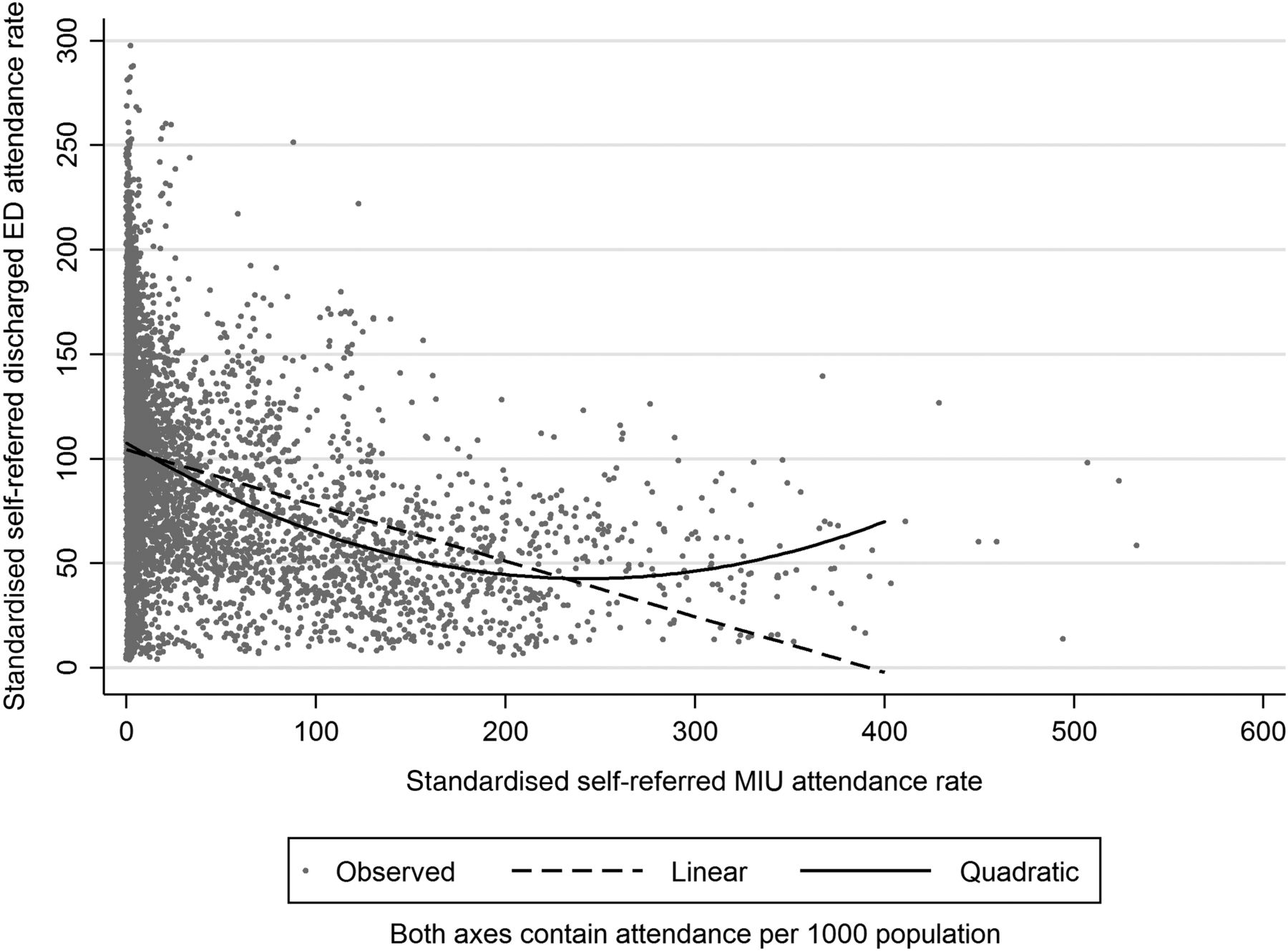
Within the multivariable analysis characteristics associated with higher self-referred discharged ED attendance per 1000 patients included a higher percentage of non-UK-qualified GPs, practices in urban areas which encompasses a number of towns (conurbations), higher percentage of patients unable to make an appointment, higher percentage of patients unable to speak to a GP or nurse within two workdays when wanted, higher percentage of patients that could always or often speak to their preferred GP, and practice populations having higher unemployment rate, higher percentage of UK whites and lower male life expectancy (table 2, model 1). Furthermore, higher MIU or WiC rates were associated with lower self-referred discharged ED attendance rate. Moreover, self-referred MIU attendance showed a nonlinear association. Both low and high MIU attendance rates (compared with medium rates) were associated with higher ED attendance rates (see figure 3). This model accounted for 34% of the variation.
Estimates of B-coefficients from multivariable regression models for the association between GP characteristics and socio-demographic profile of patients and emergency care attendance per 1000 practice population in England, April 2012–March 2013, taking into account clustering at PCT level

{kind=link}
{kind=link}
{kind=link}
Linear and non-linear association of minor injuries unit (MIU) attendance.
In table 2, the coefficients in the standardised B-coefficient (β) column are all in the same standardised units, allowing one to compare these coefficients to assess the relative strength of each of the predictors. When βs were compared, self-referred MIU attendance rates showed the highest association with ED attendance followed by level of urban conurbation, male life expectancy and the proportion of UK whites among the practice population. Among the practice characteristics the proportion of GP staff qualified in the UK showed the strongest association, almost twice the magnitude of percentage of patients being able to make an appointment.
Combined self-referred discharged ED and self-referred WiC and MIU attendances
In model 2 of table 2 the combined ED, WiC and MIU attendance rates had a median of 123.1 per 1000 (table 1). The same factors identified in model 1 were associated with patients attending one of the emergency care provisions. However, the adjusted R2 was about one-third of that in model 1, indicating that the fit of the model to the data is less good when using combined ED, WiC and MIU attendances as an outcome. When comparing coefficients in this model, level of urban conurbation showed the highest association followed by the proportion of UK whites among the practice population and male life expectancy. Among the practice characteristics the proportion of GP staff qualified in the UK and the percentage of patients being able to make an appointment showed the highest associations.
ED attendance rates and local availability of WiCs and MIUs
Table 3 shows mean attendance rates for self-referred discharged ED visits (row 1 of table 3) and for the combined ED, WiC and MIU visits (row 2 of table 3) in four scenarios: when there are no alternative healthcare services nearby; when there is only a WiC in addition to an ED; when there is only an MIU as well as an ED and when all three services are available nearby.
Mean (SD) attendance rates of emergency care services per 1000 GP patient population in relation to the local availability of MIU and/or WiC services, England April 2012–March 2013
The presence of a WiC near a practice was associated with increased rate of attendance at ED (F(17 458)=50.04, p<0.001) and overall attendance rates (ED, WIC and MIU combined: F(17 458)=212.69, p<0.001). The presence of an MIU close to the practice was associated with a highly significant decrease in ED attendance (F(17 458)=117.65, p<0.001) but little increase in overall attendance (F(17 458)=1.17, p=0.279).
Effects of adding availability of MIU and of WiC into model 1 (table 2) are shown in the online supplementary table S1. The adjusted differences were much smaller than the unadjusted differences shown in table 3. However, among practices having a WiC nearby, greater WiC use was associated with lower ED attendance rate.
Discussion
Summary
These results confirm that differences between general practices in their patients' attendance rates at urgent care services including ED, MIU and WIC are related to socio-demographic and geographical factors, as well as aspects of general practice provision. Practices with populations with worse employment rates and life expectancy, a lower proportion of patients from ethnic minority groups and those in urban conurbation areas had higher attendance rates. Practices with a lower proportion of GPs qualified in the UK, as well as those where patients have poorer access to care, also had higher attendance rates. Being able to get an appointment, being able to speak to a GP/nurse within two workdays and being able to speak to the patients' preferred GP were all associated with attendance rates, although these practice factors did not show associations as strong as the population factors. Practices with a nearby MIU had lower ED attendance rates, but total attendances at ED and MIU combined were similar. Having a nearby WIC was associated with increased practice-level ED attendance and in total urgent care service attendances. However, higher attendance rates for both WiC and MIU were associated with lower ED attendance rates.
Strengths and limitations
Data on key indicators were merged from different sources in one database and thus the information used included both survey and routine data (see online supplementary box S2). The GPPS-2012-13 had a median response rate of 38.6% (IQR 30.1–45.6%). Response rates showed a weak inverse correlation with ED attendance rates, but including response rates as a covariate in the models did not alter results. Data from the NHS Comparators website provides only a snapshot of the practice list population.11 Furthermore, we were unable to determine how patients were triaged within the ED to examine the relative effect of MIUs and WiCs on majors and minors work streams within an individual department.
Our analysis of factors related to self-referred discharged ED attendance (primary outcome) assumes that the likelihood of admission is equal for all EDs in England, conditional on these factors. However, if the same factors were positively related to the probability of admission for patients presenting themselves to EDs, this might result in our underestimating their relationship with the primary outcome.
The study uses cross-sectional data, so causality of associations cannot be inferred. Furthermore, given the ecological nature of the data (aggregated to practice level), one cannot infer associations for individual patients.
Comparison with existing literature
We tested the findings of a recent systematic review regarding several practice factors that were identified to affect emergency care attendance.3 Focusing on 2012–2013, practices' access features such as satisfaction with phone access and opening hours were not associated with emergency care attendance. Practices having limited opening hours or phone access in the past might have expanded their opening hours and improved the phone access. Ability to make an appointment was associated with emergency care attendance. Though Harris' study of data for 2007–2009 for north London did not support the hypothesis of timely access to a GP being associated with lower ED attendance, Cowling's nationwide study for 2010–2011 did support this hypothesis.21 ,22 In this study, a higher percentage of patients who wanted to speak a GP/nurse within two workdays but were not able to do so was associated with higher emergency attendance rate.
The percentage having a preferred GP was inversely but not significantly associated with ED attendance. This finding does not support findings from studies from Canada and USA.3 Whereas studies by Cowling and Harris had not found an association between the percentage of practice patients that could see their preferred GP and self-referred discharged ED attendance rates,21 ,22 this study found that practices where patients could see their preferred GP always or often were associated with slightly higher ED attendance rates. Further investigation of this issue may be improved by using individual rather than practice-level data. Unlike Baker et al,23 we did not find an association between patient travel time to a hospital and emergency care attendance rates. This might be connected to the location of MIUs and WiCs, as some MIUs replaced small EDs while some WiCs were also to be found near a hospital. However, after adjusting for patients' extra travel time to the hospital, rural practices were associated with lower emergency care attendance rates.20
Our analyses supported previous studies that ethnicity is of importance as a higher percentage of UK whites among practice populations were associated with higher emergency care attendance rates.23 Furthermore, instead of IMD this study included lower economic status measured by unemployment and practice populations' health condition by life expectancy; higher unemployment and lower life expectancy were associated with higher emergency care attendance rates.
Moreover, this study tested other factors which had not been widely examined, mainly factors related to the GP workforce composition. A higher percentage of GPs qualified in the UK was associated with lower emergency care attendance rates. This factor has not been widely examined but could be related to problems non-UK-trained GPs face when starting to work in the UK as identified by Slowther et al,24 including variable levels of training and support specifically in the areas of communication and decision making, and isolation. Younger GP staff and more female GP staff in a practice were not associated with emergency care attendance rates.
Practice populations showing higher WiC or MIU attendance rates were associated with lower self-referred discharged ED attendance rates (table 2). Conversely, a simple analysis of practice-level ED attendance rates suggests lower ED attendances for practices with a nearby MIU, but higher attendance rates in practices with a nearby WIC (table 3). This finding supports studies by Chalder and Salisbury rather than Arain's study.7–9 The increased ED consultation rate in practices close to WiCs could be interpreted as supply-induced demand. However, a more likely explanation is that WiCs were established by the NHS in areas with high ED attendance rates (or need for healthcare services). Therefore, after allowing for the presence of a nearby WIC (as in the online supplementary table), higher WiC attendance rates were associated with slightly lower ED attendance rate, indicating that more use of WiCs reduced pressure on EDs. For a few practices, however, high MIU attendance rates were associated with higher ED attendance, indicating that this alternative care provision might have led to supply-induced demand.11
Implications for research and practice
Use of other immediate care services, such as MIUs and WiCs, was associated with lower self-referred discharged ED attendances. They might therefore be seen as an alternative source of care for ED. Our data suggest that in some areas practice populations do not have alternative health services close by or these services are less used by them, so establishing those services and encouraging patients to visit them might be a way of reducing the pressure on ED. However, potential unintended consequences such as supply-induced demand should be considered.11
This study showed that the associations with practice population characteristics were greater than most practice characteristics. Since practices with higher percentages of UK whites are associated with higher ED attendance further research is needed to investigate differences in attitude towards ED visits between different population groups. Further research is also needed to understand why unemployment rate was associated with higher ED attendance rates.
About half of the practice population had a preferred GP (table 1), but their emergency care attendance did not differ much from practices where less than half of the patients had a preferred GP. Moreover, practices where relatively more patients could often see their preferred GP was associated with higher emergency care attendance rates. Further investigation is needed into the importance from the patients' perspective of having a preferred GP and the social and health need background of those who visit their preferred GP often.25
Though most patients were able to get an appointment and were able to speak to a GP or nurse within two workdays when wanted (table 1), practices where patients had more difficulty had higher rates of attendance at alternative healthcare services such as an ED, an MIU or a WiC. These results seem to suggest that it might be more important that patients are able to make an appointment or have the opportunity to speak to a GP/nurse within this time frame, rather than to focus on patients' satisfaction with opening hours or phone access. Moreover, practices having a higher percentage of GPs qualified in the UK were associated with lower ED attendance rates: this finding merits further investigation.
References
Footnotes
Contributors PT, DL, RWM and SP designed the study. PT collected and managed the data, and performed the analyses. PT, AH, RWM and SP drafted the first version of the manuscript. RWM, DL, CS, KC and SP contributed to the methodological approach and also added significant input to the results and discussion. All authors contributed to interpretation of the findings and revision and approval of the final manuscript. SP was the lead investigator for the overall project.
Funding This research is funded by the National Institute for Health Research School for Primary Care Research (NIHR SPCR). Grant funded round four, PI SP project number 115. DL is supported by the NIHR Oxford Biomedical Research Centre.
Disclaimer The views expressed are those of the authors and not necessarily those of the NIHR, NHS or Department of Health.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.