Article Text

Abstract
Defining research priorities in a specialty as broad as emergency medicine is a significant challenge. In order to fund and complete the most important research projects, it is imperative that we identify topics that are important to all clinicians, society and to our patients. We have undertaken a priority setting partnership to establish the most important questions facing emergency medicine. The top 10 questions reached through a consensus process are discussed.
- priority setting partnership
- James Lind Alliance
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Emergency medicine (EM) is a broad specialty, and the research both underway and planned is such a vast undertaking that we need to focus on the most important research questions to answer the most pressing uncertainties.1 Defining research priorities in a specialty like EM is a significant challenge. In order to fund high-quality and important research projects, it is imperative that we can identify topics that are important to the multidisciplinary clinical team working in our EDs, society and of course to our patients.
Over the last 18 months, the Royal College of Emergency Medicine (RCEM) has worked in collaboration with the James Lind Alliance (JLA) to seek, review, highlight and finally rank the most important questions facing our specialty. The JLA process engaged clinicians, patients, carers and the public to prioritise research questions in EM in a consensus process to determine the top 10 questions (box 1). This paper outlines briefly the process that was undertaken and its results.
The top 10 research priorities in emergency medicine (EM)
What is the best way to reduce the harms of ED crowding and exit block? We need a better measure of crowding that drives sensible improvements for the seriously ill and injured, adolescents, and the frail elderly.
Is a traditional ED the best place to care for frail elderly patients? Would a dedicated service for these patients be better (involving either a geriatric ED or geriatric liaison services within the ED), or given that this population is expanding should our current services be tailored towards this group?
How do we optimise care for mental health patients, including appropriate space to see patients, staff training, early recognition of symptoms, prioritisation compared with physical illness and patient experience?
With regard to how ED staff development is managed, what initiatives can improve staff engagement, resilience, retention, satisfaction, individuality and responsibility?
How can we achieve excellence in delivering end-of-life care in the ED, from the recognition that a patient is dying, through symptomatic palliative treatment, potentially using a dedicated member of staff to work with palliative patients and their relatives, and handling associated bereavement issues?
The effects of implementing new techniques in assessing patients with chest pain (which include new ways of using high-sensitivity troponin tests, and decision rules such as the MACS rule and the HEART score) in practice. Would patients like a say in what is an acceptable risk, and should these tools be used alongside shared decision making to provide safe and appropriate care, and minimise unnecessary risk and inconvenience for patients?
What is the ideal staffing for current UK EM practice, including doctors, nurses, healthcare assistants, porters, radiographers, clerical and reception staff?
Do early undifferentiated (broad-spectrum) antibiotics in suspected severe sepsis have a greater benefit and cause less harm to patients than delayed focused antibiotics in the ED?
In adults who are fully alert (Glasgow Coma Scale 15) following trauma, does cervical spine immobilisation (when compared with no cervical spine immobilisation) reduce the incidence of neurological deficit, and what is the incidence of complications?
Which trauma patients should be transferred to a major trauma centre rather than going to another hospital first?
Priority setting partnership
The JLA was established in 2004 and has a well-established process to prioritise research topics.2 The core elements of the JLA philosophy are that addressing uncertainties about the effects of a treatment should be seen as a standard part of clinical practice, and that patients, carers and clinicians should work together to agree which, among those uncertainties, matter most and deserve priority attention. By defining the research priorities in a subject area, funding organisations are able to target themed calls in those areas to ensure research is undertaken to address the most important uncertainties.
The EM Priority Setting Partnership (PSP) is the 46th project coordinated by the JLA, with previous PSPs including intensive care medicine3 and anaesthesia.4 The EM PSP was launched in September 2015 and culminated in January 2017.
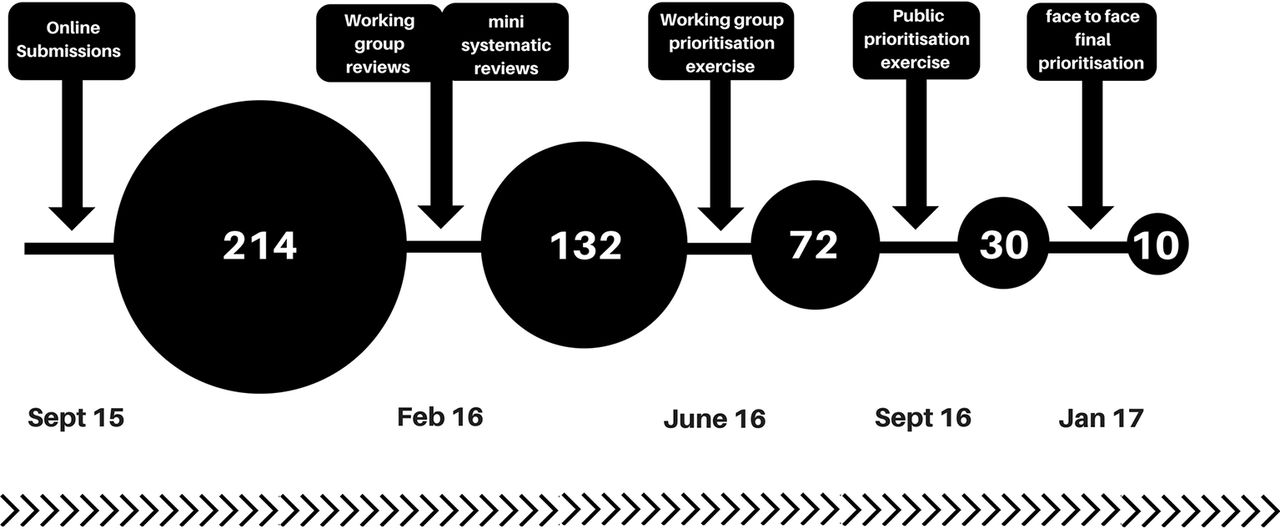
The PSP process begins with seeking a broad range of questions from any interested individuals or organisations, typically through online polling. For this project, RCEM members and fellows, other clinicians working in EDs, patients and carer organisations were invited to participate through advertisements, social media and direct request. This initial approach yielded 214 research questions that were submitted through an online survey, either in free text or in PICO (population, intervention, comparator, outcome) format (figure 1).

{kind=link}
The evolution of research questions within the priority setting partnership
A working group reviewed the submitted questions, and a broader group of interested clinicians were invited to conduct mini-systematic reviews to identify which of the questions remained unanswered and relevant to the PSP. Reviews were structured according to the established BestBETs format.5 Reviewers were encouraged to submit these reviews to the online BestBETs database so that they are accessible to those undertaking future searches. Ninety-six of these reviews were undertaken.
Duplicates were noted, questions were checked to ensure they were within the scope of this process, and those with existing answers were removed, leaving 132 questions to go forward to the next stage. These unanswered questions underwent prioritisation by the EM PSP Steering Group (through an online survey) to establish a longlist of 72 questions. Those that were submitted more than once were automatically prioritised to the next stage.
This longlist of 72 unanswered questions were taken forward to the next open prioritisation stage. We used an online survey directed at RCEM members and fellows, patient organisations, carer organisations and clinicians to review and score these 72 questions. Participants in the survey were asked to rank whether each question should be researched as a priority as definitely, maybe, maybe not, definitively not or don’t know. Five-hundred thirteen people participated, allowing each question to be scored and ranked. The longlist of 72 questions is available on the RCEM and JLA websites.6 7
The top 30 research questions from this process entered the final workshop in Manchester on 19 January 2017. Thirty-four individuals including doctors, nurses, patients and carers congregated to discuss, debate and finally identify the top 10 research priorities for our specialty. This final face-to-face process, which was based around small group debate and discussion, was an opportunity to challenge and explore the final questions before a final plenary ranking session where the entire group reached a consensus on the top 10 research priorities.
One of the many challenges faced by the steering group was deciding whether to report the research priorities for all topics within EM or whether to divide into subspecialty areas (eg, trauma, mental health). However, in order to achieve maximum impact, we have reported a single top 10 in keeping with established JLA methods. One consideration during the final prioritisation workshop was to ensure that the top 10 broadly represented EM practice and to try and avoid multiple questions on one particular topic or area of practice, for example, sepsis or major trauma. Consequently, the top 10 has a very broad feel and will hopefully encourage research funding across a wide-ranging topic base covering many aspects of EM. Other factors that were discussed on the day included the prevalence of the condition in question (and how many patients are affected by it), potential crossover with other specialty PSPs and whether the group were aware that there was already ongoing work in that area that might answer the question.
Inevitably the style of questions varied, leading to debate regarding the broader intention or application of some questions. For example, question 6 relates to the implementation of decision rules and investigation strategies in patients with chest pain, but also has a clear statement of intent regarding shared decision making. It was this aspect in particular that the workshop participants were keen to prioritise. There was also some discussion around whether some of the questions could have been reworded to achieve greater clarity and potential usefulness.
We discovered an interesting paradox in the pursuit of patient involvement. Despite the ED being used by nearly everybody, the specialty lacks specific national patient interest groups as typified in other JLA PSPs. This resulted in less direct patient involvement than expected and a realisation that EM needs to explore ways to hear the patient voice in a consistent and accessible way. One successful model has been described where a patient group has input to research projects from one institution on a regular basis.8
Despite these concerns, 19% of responses to the prioritisation survey were submitted by patients and the public, and we are therefore confident that the voice of the patient has been heard in establishing the top 10.
The success of the JLA process will be defined not by the top 10 questions, but rather in the empowerment of patients, carers and clinicians to obtain funding for and deliver high-quality research in these important, relevant and high-priority topic areas. It was thus encouraging and no surprise that the National Institute of Health Research and other research funding bodies were present in an observer capacity in the final stages of the JLA process. This bodes well for the future of EM research and will act as the catalyst for future efforts to identify groups within academic EM to take forward these priorities and ultimately mould them into deliverable research studies.
Conclusion
The top 10 research priorities represent a landmark in EM research. This is the first time that such a broad group has come together to define research priorities for our specialty, and the specialty, the public, researchers and funding bodies should heed these questions.
The top 10 priorities are a significant and important achievement, but it should be noted that there are many worthy and important research questions in the top 72. All of these questions represent opportunities for research in EM, and they are highly likely to gain the attention of researchers and funding organisations. Whether you are an established or aspiring researcher, we hope that you feel inspired and energised by the results. It is clear to all of us who took part in this process from the start that EM research matters, that it has the potential to make a real impact on patients and clinicians, and that EM is undoubtedly an area where high-quality research will happen. Indeed, the JLA process has identified a broad range of topics that could sustain and support EM research for many years.
Acknowledgments
We thank all those individuals, including patients, carers, members of the public and clinicians for submitting their research questions, responding to the survey requests and participating in the final prioritisation workshop.
Footnotes
Contributors JS was the clinical lead for the PSP and drafted the initial version of the manuscript. RM chaired the steering group and edited the manuscript. All other authors were on the steering group and edited subsequent versions of the manuscript.
Funding Funding was received from the Royal College of Emergency Medicine to support this PSP.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Collaborators The JLA EM PSP Steering Group members include Helen Allen, Justine Amero, Simon Carley, Douglas Findlay, Lynsey Flowerdew, Melanie Gager, Liza Keating, Ben McCullough, Hazel McCullough, Sam McIntyre, Richard Morley, Rachel O’Brien, Miranda Odam, Ian Roberts, Jason Smith and Katharine Wylie.