Article Text

Abstract
Objective To determine the impact of the GP-led walk-in centre (WIC) in Sheffield (England) on the demand for emergency department (ED) care.
Methods A survey of patients visiting the Sheffield GP WIC was conducted over 3 weeks during September and October 2011. A short, postvisit questionnaire was also sent to those who agreed to determine if the patient had used another NHS service for the same problem. Routine data were obtained from the adult and children's EDs and minor injuries unit in Sheffield, 1 year before and 1 year after the opening of the GP WIC. A linear model of the number of minor daytime attendances (GP type) per month was used to estimate the impact of opening the GP WIC, after controlling for seasonal variation and a linear time trend.
Results A total of 529 patients responded to the survey (response rate 51%). Based on their self-reported intentions, 64 of these patients (53 adults and 11 children) were diverted from going to ED in the 3-week survey period as a result of the establishment of the GP WIC. From this we would have expected around a 26% monthly reduction in GP-type attendances at adult ED, and 7% reduction at children's ED. However, routine data only showed an 8% (95% CI 1% to 16%) reduction at the adult ED. Reductions in GP-type attendances at the children's ED and the minor injury unit at the time of the opening of the GP WIC were also found, but were not statistically significant. The estimated impact on children's ED was a 14% reduction (95% CI −38% to 8%), and for minor injuries unit (MIU) a 4% reduction (95% CI −18 to 9%).
Conclusions There was a statistically significant reduction in GP-type daytime attendances at the adult ED after the opening of the GP WIC. Since this reduction was not mirrored in changes in night-time attendances (when the GP WIC was closed), and our survey responses suggested some people were diverted from going to the ED, it is possible that the opening of the GP WIC caused this reduction.
- emergency care systems, admission avoidance
- emergency care systems, primary care
- emergency departments
- prehospital care
- primary care
Statistics from Altmetric.com
- emergency care systems, admission avoidance
- emergency care systems, primary care
- emergency departments
- prehospital care
- primary care
Key messages
-
What is already known on this subject
-
Nurse-led walk-in centres have been proposed as an alternative source of care for unscheduled patients.
-
Previous studies also show that they have not reduced demand for other NHS services such as ED care.
-
GP-led walk-in centres, or urgent care centres, were introduced in 2009 but there is little published evidence about their effectiveness and impact.
What this study adds
-
This single centre study found that 18% of patients using a GP-led urgent care centre reported that they would have used ED if the urgent care centre had not been open.
-
The GP-led urgent care centre produced small changes to attendances at local EDs during daytime working (64 patients over 3 weeks), fewer would have been estimated from the patients' reported intentions.
Introduction
GP led walk-in centres (WICs), also known as Darzi centres, or polyclinics, were established in England in 2009. These centres were designed to improve access to GPs as well as to prevent unnecessary attendances at emergency departments (ED).1 First attendances at EDs in England have increased by 60% in the last decade and now stand at over 20 million per year. Such increases are common throughout the developed world, and a recent systematic review of the drivers of this change found that as well as changes in population demographics and patient expectations, changes in the organisation and delivery of alternative healthcare services were important.2
Many studies have reported that a large proportion of patients attending ED consist of patients with minor illness who could be seen by a healthcare provider in a primary care setting. There is some evidence that increases in these visits are another driver for the overall increase in ED attendance.2 Accordingly, the provision of alternative healthcare services for patients with minor conditions may help curb the increasing demand for ED care.
Previous attempts to reduce ED attendance through the development of nurse-led WICs did not show any significant impact on ED attendance.3 There are several reasons why patients with minor illness present to ED, including easy access to a doctor, 24 h availability, and lack of information about the availability of alternative services. Sometimes it is difficult for a patient to choose the right service among many options.4 A recent population survey showed that patients prefer to use GP services for unscheduled care, and that changes to service provision have little impact on this behaviour.5
To help address these sorts of concerns, a GP-led WIC was opened in Sheffield in April 2009. The purpose of this study was to examine the impact of the opening of this GP WIC on the use of the local EDs. We conducted two surveys of patients visiting the GP WIC, one at the time of the GP WIC visit and the other 4 weeks after the visit, to determine whether or not patients had used other NHS services for the same problem. We also looked at routine data on the use of other NHS services. This paper presents the findings related to the impact of the GP WIC on the use of the adult ED, children's ED and the MIU in Sheffield.
Methods
The Sheffield GP WIC was established in April 2009, and the centre provides walk-in services from 8:00 to 21:00, 7 days a week. All patients attending the WIC between 26 September 2011 and 9 October 2011 were asked to complete a validated questionnaire6 to determine why they used the walk-in service, how satisfied they were with the location and opening hours of the centre, what they would have done in the absence of the GP WIC service, their satisfaction with the service, and if they were treated at the centre or referred to ED or another NHS service. Complete details of the survey methods have been described in an earlier paper.7 This paper focused on the impact of the GP WIC on some other urgent care services in Sheffield.
We used an interrupted time series design to determine the effect of the opening of the GP WIC on other urgent care services. Secondary data from the adult ED, children's ED and the minor injury unit (MIU) in Sheffield were obtained for the period of 2 years from April 2008 to March 2010, 1 year before and 1 year after the opening of GP WIC. To examine the impact of the GP WIC, we only used data on attendances by GP-type cases. For this study, minor cases (GP-type cases) were defined as those patients who were referred or discharged from the ED without needing any investigation, or only some low-cost investigations as defined by the tariff codes used by the primary care trust (PCT). These two categories accounted for about 53% of all cases presented at these services during the study period. The excluded cases were those who needed hospital admission, or needed high-cost investigations (such as X-rays, CT scans and MRI) and those who did not survive. The reason why only minor cases (GP type) were included was because the GP WIC cannot be expected to have had any impact on the attendances rate of patients with serious health problems who need hospital admission or need high-cost investigations. For the primary analysis, we only used patients’ attendances at ED during the opening hours of the GP WIC (8.00–21.00) to determine any change in the attendance rates. For the secondary analysis, we adjusted the change in daytime attendances with the change in night-time attendances.
Data were entered and analysed in SPSS V.19. A General Linear Model (GLM) was used to fit a ‘regression discontinuity model’ to the monthly counts of attendances to determine the effect of the opening of the GP WIC on patient attendances at the EDs and MIU. A regression discontinuity model was used instead of a time series model which would assume some form of serial dependence because the autocorrelations between the residuals from the monthly counts were negligible. Seasonal effects (fitting a categorical variable with six annual values representing each two consecutive months) and a linear time trend were fitted. The analysis was repeated using night-time GP-type attendance rates as a covariate to act as a control.
Arch GIS V.10 was used to map the distribution of patients’ home addresses and the locations of the urgent care services.
Ethical approval of the study was obtained from the NHS ethical review committee (REC reference number 10/H1304/31). No written consent was required as it was a self-report questionnaire, and consent was considered given if a patient filled in and returned the questionnaire.
Results
A total of 1045 questionnaires were distributed, of which 529 patients participated in the study by completing all or part of the visit questionnaire, a response rate of 51%. Of these, 448 completed the questionnaire. The survey sample was compared with the WIC's routine data to examine the representativeness of the responding sample and no major differences were found between the two datasets in terms of age, sex and different timings of attending the centre. Most of the patients arrived without an appointment for the service. However, 4% of the patients had a prior appointment before coming to the centre. Figure 1A,B show the location of residence of the patients who presented at the GP WIC during the survey period. It shows that patients came from diverse areas of Sheffield and Rotherham, and a few came from Barnsley and the countryside south of Sheffield in Derbyshire. A total of 19% of patients were resident within 1 mile of the GP WIC, and the geographical spread appears wider on weekdays than at the weekends.

(A) and (B) Location of the patients presented to the Sheffield GP led walk-in centre.
Around 18% (n=80, 65 adults and 15 children under 16 years) of the patients said that they would have gone to ED if the GP WIC had not been there, but only 3.6% (n=16) reported their intention to attend ED after consultation. Thus, the net number of patients in the sample of respondents potentially diverted from ED as a result of the establishment of the GP WIC was 64 (14%). Based on the average number of patients presenting at the GP WIC each month (data not shown) and the average monthly counts of minor illness/injury patients presenting to the EDs, the expected reductions in GP-type attendances at the Sheffield children's ED and the Sheffield adult ED were 6.7% and 20.6%, respectively.
There were 121 postvisit survey respondents (response rate 50%). These were used to see whether those who stated they intended to visit the ED after the consultation actually did so. The postvisit survey found that only nine patients actually visited the ED.
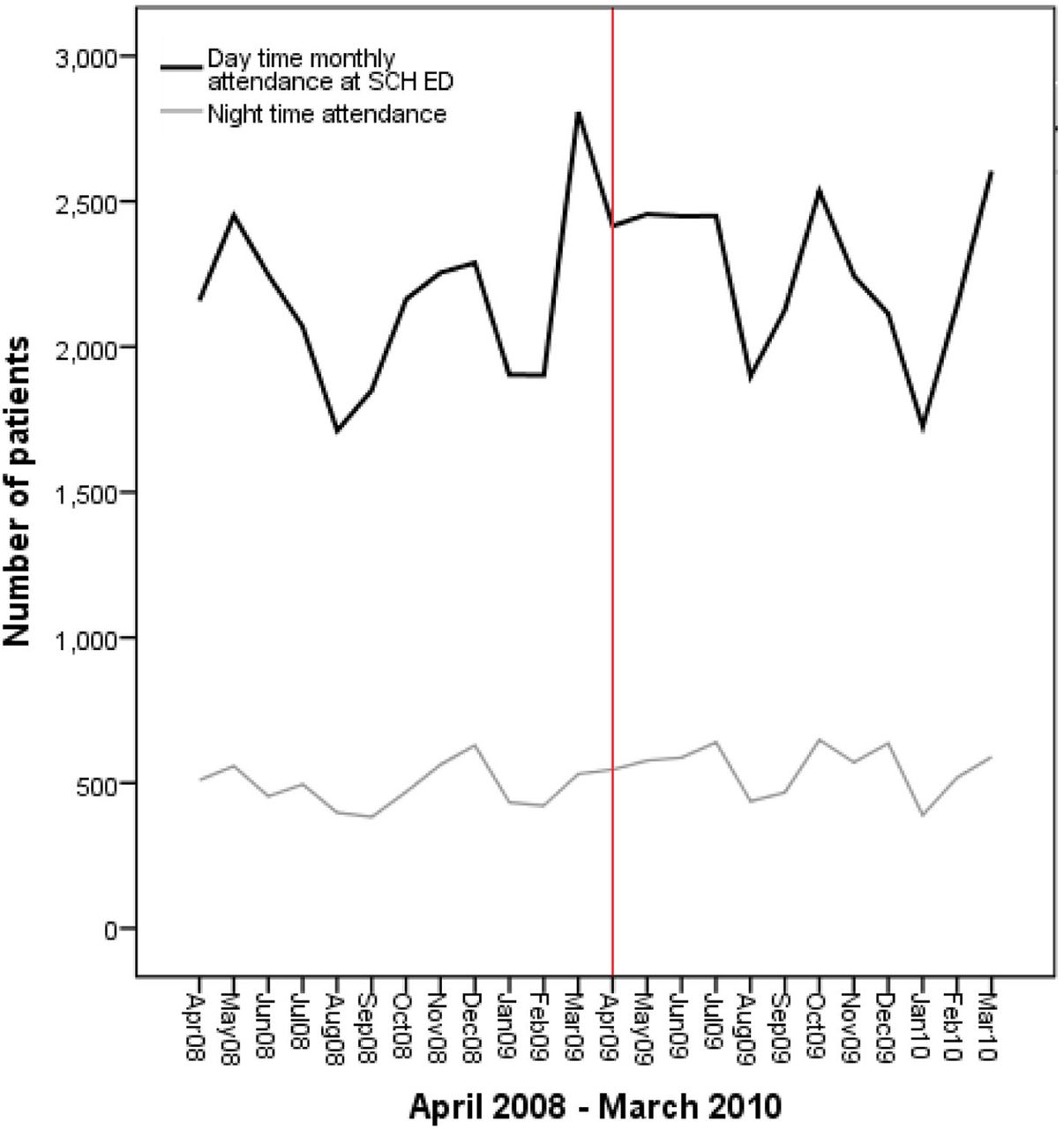
Figures 2–⇓4 show monthly counts of minor attendances (GP type) at the Sheffield Children's Hospital ED, the adult ED and the MIU over the period of 2 years, from 2008 to 2010. The 2-year period included monthly counts at these services 1 year before and 1 year after the opening of the GP WIC. The effect seen on the adult ED was an 8.3% (95% CI 1% to 16%) reduction in daytime GP-type attendances which is statistically significant (p=0.03). The effect on adult ED was a 5% reduction (95% CI 1% to 9%) if night-time attendances were used as a control (p=0.02). The estimated effect on the children's ED was a 14.9% reduction (95% CI −37.8% to 7.9%); however, the effect was not statistically significant (p=0.19). The estimated effect on the MIU (a 4.3% reduction in attendances; 95% CI −17.8% to 9.2%) was also statistically non-significant (p=0.51) ( table 1).

Sheffield Children Hospital emergency department patients’ count, 1 year before and 1 year after the opening of the GP walk-in centre (WIC). The midline shows the month of the opening of WIC.

Sheffield Northern General Hospital (adult emergency department) patients’ count, 1 year before and 1 year after the opening of the GP walk-in centre (WIC). The midline shows the opening of the WIC.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Sheffield minor injury unit patients’ count, 1 year before and 1 year after the opening of the GP walk-in centre (WIC). The midline shows the opening of the WIC.
Mean monthly count (daytime GP-type attendance) 1 year before and 1 year after the opening of the GP walk-in centre
Discussion
This study has estimated the potential impact of a GP WIC on other NHS services. This is an important issue as some similar centres have been closed because of lack of evidence of having any beneficial effect on the NHS.8 There is evidence from the international literature about decreases in ED attendances in the presence of better primary care services.9 However, studies in the UK on NHS nurse-led WICs did not show any significant impact on other NHS services.10 ,11 The effect of a GP-led WIC on ED attendances has not previously been studied, and this is the first paper to report the GP WIC impact on other NHS services.
The survey results suggest that based on the patients’ stated intention to visit ED, the centre has the potential of reducing GP-type attendances at the adult ED by about 20%, and by 7% at the Sheffield children's ED. Routine data on attendances showed that the GP WIC may have reduced GP-type daytime attendances at the adult ED, but by only 8%. This suggests that respondents were over-reporting their intention to visit ED in the questionnaire survey. However, there are number of other factors which might have resulted in there being little impact on ED. When a new service like a GP WIC starts, it may lead to increased demand for healthcare services, which could also lead to a rise in patients going to the ED. The balance of new demand leading to more ED attendances, and the redistribution of existing demand leading to fewer attendances could explain why there was a smaller reduction in the routine data than in the survey data. Another possible explanation of the discrepancy between the routine data and survey data is that patients sometimes confuse WICs, MIUs and EDs in questionnaire surveys of the use of urgent care services.12
The location of the centre is also important. The GP WIC is about 3 miles distance by road away from the adult ED, and 1 mile from the children's ED, and it might be expected that the centre would have had more impact on ED attendances if it were colocated with the ED. However, previous studies were unable to show that WICs colocated with EDs had any reduction in patient load at ED.13 Nevertheless, the impact of colocated WICs has only been studied for the traditional nurse-led WIC rather than GP-led WICs. Furthermore, some patients may not be aware of the presence of all the available urgent care services. One study identified that more than half the patients presenting at the ED in Sheffield were unaware of the WIC or of GP out-of-hours services.14 Additionally, it may be difficult for patients to determine the severity of their problems, and so they prefer to go to the ED to prevent any potential harm. This may be one of the reasons why most alternative urgent care services have failed to show any reduction in ED use,15 including the new NHS 111 telephone service.16
The GP WIC might also be having some impact on surrounding GP practices and possibly on out-of-hours services. In the light of the recent changes in NHS commissioning, it might become more difficult to commission GP-led WICs if they have the potential to attract patients from the surrounding GP practices as a result of their longer opening hours and walk-in facilities. It has also been observed for ED that patients living closer to an ED are more likely to use the ED service for unscheduled care.17 However, our results show that patients from a wide spread of residential areas in Sheffield use the GP WIC, and there is only on a small gravitational effect seen for the nearby residents to use this service as seen in figure 1A,B. The differences between the residential patterns for weekday and weekend users shown in figure 1A,B may indicate that some of the weekday use is by commuters who live outside the normal catchment area.
Our study has some limitations. First, the survey was based on a self-reported questionnaire, where data quality is dependent on the response rate. However, the first on-site survey had a reasonable response rate in this study, and the characteristics of respondents were similar to the routine data of the centre. The postvisit survey had a lower response rate. Nevertheless, the data from the postvisit survey was not used to determine the impact on ED, but was only used to assess the validity of responses in the main survey. Second, we had no control arm for estimating the impact on the MIU. For ED data, we used night-time attendances when the GP WIC is not open, as a control group to see any effect as a result of the GP WIC opening. This assumes that any external changes which might have affected daytime attendances would also have affected night-time attendances. The MIU's openings hours were similar to the GP WIC, hence, we were not able to have a control arm for this service.
The results of this study also need to be interpreted with care. First, it must be remembered that the reduction in patient load at adult ED shown in this paper is a reduction in minor daytime attendances (GP type attendances) only, and not total ED attendances. The estimated reduction in total attendances is only 2.8% for adult ED, 7.8% for children's ED and 2.5% for the MIU. Second, our data only show a reduction in attendances at adult ED occurring at the time the GP WIC opened in April 2009, and it is questionable whether we can infer that these reductions were the result of the opening of the GP WIC. However, we think the causal inference is justified by the fact that no similar reduction was found in night-time attendances, and that the patient survey clearly indicates a change in self-reported service use.
It is important to give consideration to the impact on the demand for healthcare when we choose to open a new service or close an existing service. Opening of a new service may help to meet unmet needs of the population, but at the same time, it may also create new demand for health services. Once the demand has been created, it may cause significant impact on patient load in the ED and other services, as well as on cost, especially if the service has to be closed in the future.
We have found evidence that the opening of the GP WIC in Sheffield has resulted in a reduction of 8% in adult ED GP-type daytime attendances. There was also an estimated 14% reduction in attendances at the children's ED, but because of bigger variability in the counts of monthly attendances, this reduction was not statistically significant. Only a small 4% reduction in attendances at the MIU was found. Our data also suggest that self-reported intentions in survey questionnaires are unreliable, and can greatly exaggerate the impact on EDs.
Acknowledgments
The research was supported by a NIHR senior investigator award made to Jon Nicholl. We also acknowledge the studentship funding support to Mubashir Arain by Dow University of Health Sciences, Pakistan. We gratefully acknowledge the support of the GP walk-in centre's staff and managers for providing access and support in data collection, and the PCT commissioners for supporting the study. We are also grateful for the support of Mark Wilkinson, head of information, Sheffield Primary Care Trust.
References
Footnotes
-
Contributors All authors were involved in the planning and designing of this project. MA collected data and prepared the initial draft. MJC analysed data and helped in preparing tables. JPN critically reviewed the paper and also contributed in data analysis. All authors reviewed and approved the final draft.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval NHS, Yorkshire and the Humber region REC.
-
Provenance and peer review Not commissioned; externally peer reviewed.