Article Text

Abstract
Objective To estimate the prevalence of post-concussive symptoms (PCS) following head injury among adolescents in full-time education and to identify prognostic factors at presentation to the emergency department (ED) that may predict the development of PCS.
Methods An observational cohort study of all head injured patients aged 13–21 and in full-time education presenting to an inner city ED was performed. Subjects were followed up at 1 and 6 months after injury by structured telephone interview to assess for the presence of symptoms or ongoing disability. Presentation data of those identified as having PCS underwent regression analysis to isolate potential prognostic indicators for such problems.
Results Of the 188 patients recruited, 5.9% (95% CI 3.3% to 10.2%) still had some symptoms after 6 months, with half of these claiming that such symptoms were affecting everyday living. Of these patients, 82% were assaulted as the cause of their injury and nearly 40% had no conventional indicators of head injury severity at presentation. After 1 month, 46/188 (24.5%, 95% CI 18.9% to 31.1%) patients had some degree of symptoms, most of whom were discharged directly from the ED. Potential prognostic indicators identified were a reduced Glasgow Coma Score (GCS) (<15) at presentation and being assaulted as the cause of injury.
Conclusion The prevalence of PCS 6 months following head injury for the selected sub-group was 5.9%, and 10.6% if assaulted. Most patients who developed PCS were discharged directly from the ED.
- Craniocerebral trauma
- adolescent
- post-Concussion syndrome
- mental health
- trauma
- head
- wounds
- research
Statistics from Altmetric.com
Introduction
An estimated 700 000 patients attend the emergency departments (EDs) of England and Wales annually, with around 20% admitted. Around 90% of ED attendees experience what is considered a ‘mild’ head injury.1 Most are therefore expected to make a full and prompt recovery, and there is no routine follow-up to assess for sequelae from most hospitals in the UK.2 Disability following even seemingly mild head injury is a recognised problem.3 Simple interventions may reduce the adverse effects of head injury, in both adults and children.4–7 However, providing follow-up for all head injured patients would be an enormous and costly undertaking and many patients will recover without intervention.
Traumatic brain injury has been shown to adversely affect academic achievement by worsening behavioural problems and affecting cognitive functioning.8 9 We considered those in secondary and tertiary education to be a group at particularly heightened risk in terms of impact on future life chances by intrusive symptoms or a period of reduced neurological performance after head trauma. Indeed, study for GCSE, AS and A level examinations spans the age range of 14–19, and coincides with the age group with the highest incidence of head injury in the UK.10 11
Despite this, the effects of head injury on children and young adults discharged from the ED has yet to be assessed in the UK. The aim of this study, therefore, was to identify the point prevalence of disabling symptoms following head injury in a sub-group of patients (aged 13–21 years and in full-time education) at 1 and 6 months following their injury. We also aimed to identify a high-risk group for ongoing symptoms from their ED presentation.
Methods
Local research ethics committee approval was granted to consider patients presenting to the ED at Hull Royal Infirmary for recruitment by nursing and medical staff if they fulfilled the following criteria:
Aged 13–21 years (inclusive).
Presenting with head injury (defined as ‘any blow to the head causing a diagnosis of head injury to be made’).7
In full-time education at the time of their injury.
There were no exclusion criteria for this project in order that the findings may be generalisable to the ED population.
Demographic and injury characteristic data were collected on a pro-forma that replaced the patient record. Major trauma patients required additional, in-depth documentation that was not encompassed within the pro-forma and so data were collected from departmental trauma forms in these cases.
Recruitment took place between August 2005 and February 2006, with follow-up at 1 and 6 months. Only those patients with disability at 1 month were contacted again for the 6-month interview.
To maximise recruitment two strategies were used. First, patients were recruited prospectively, with completion of the data collection pro-forma and obtaining consent at the time of presentation. The secondary method was by review of the medical records for all 13–21-year-olds presenting to the departments during the recruitment period. If eligible patients were identified by the second method, ethical approval was granted to contact them by post, informing them of the project and the desire to include them in our sample with an opt-out from further contact. If no opt-out was received these patients were contacted by telephone for the progress interview and consented at that time.
Outcome assessment
Outcome was assessed with a structured telephone interview using the previously validated Glasgow Outcome Score in its extended form (GOSE) and the King's Outcome Scale for Childhood Head Injury (KOSCHI)—a paediatric adaptation of the GOSE.12–14 The Rivermead Post-Concussion Questionnaire was also used, to outline ongoing symptoms15 (see supplementary files online).
Subjects were contacted by one member of the research team, approximately 1 month after injury. This involved a telephone interview following the structured outcome format from the amalgamation of the GOSE and KOSCHI scores. Following interview, subjects were categorised into one of three outcome groups that corresponded to the GOSE (or KOSCHI) score (see table 1).
Outcome score equivalence
Logistic regression analysis
Data were analysed using binary logistic regression in SPSS for Windows V.14.0. This analysis was with the forward stepwise method of regression and included 95% CIs in the results. Primary analysis was performed on the outcome interview data—that is, those subjects still with symptoms after 6 months. In particular, previously described clinical parameters were assessed as potential prognostic indicators for a poor outcome. Secondary analysis was performed on the progress interview data. First, those in category 4b were identified who went on to require a follow-up interview. This was then expanded to include all those with some symptoms (categories 5a and 4b) after 1 month.
Results
A total of 9726 13–21-year-olds attended the ED during the study period. Of these, 715 (7.6%) patients had a head injury. Two patients died shortly after arrival at hospital. Only 354 of these patients were either in full-time education or with unknown employment status, 166 of which we were unable to contact. These were 13–21-year-olds who had had a head injury with no record of work or education status. The mechanism of injury, CT and admission rate were not significantly different from those in the recruited subject group.
A total of 188 patients, therefore, were followed up over the 6-month period. Of these, 138 (73%) were male, consistent with previous studies.3 11 Seventy-two patients were recruited at the time of presentation, with a completed data collection form, and the remaining 116 by the secondary recruitment method of letter and subsequent telephone call.
Of the 166 un-recruited patients, 62 were under the age of 16. In theory all of those under 16 should still be in full-time education. If this was the case and the ratio of under 16s to older patients in education was consistent with our recruited cohort (64:36), then the expected number of eligible patients missed is 62+(36/64×62)=62+35=97. Using this figure, the calculated recruitment rate for this study was 66% with a 95% CI of 60% to 71%.
One-month follow-up
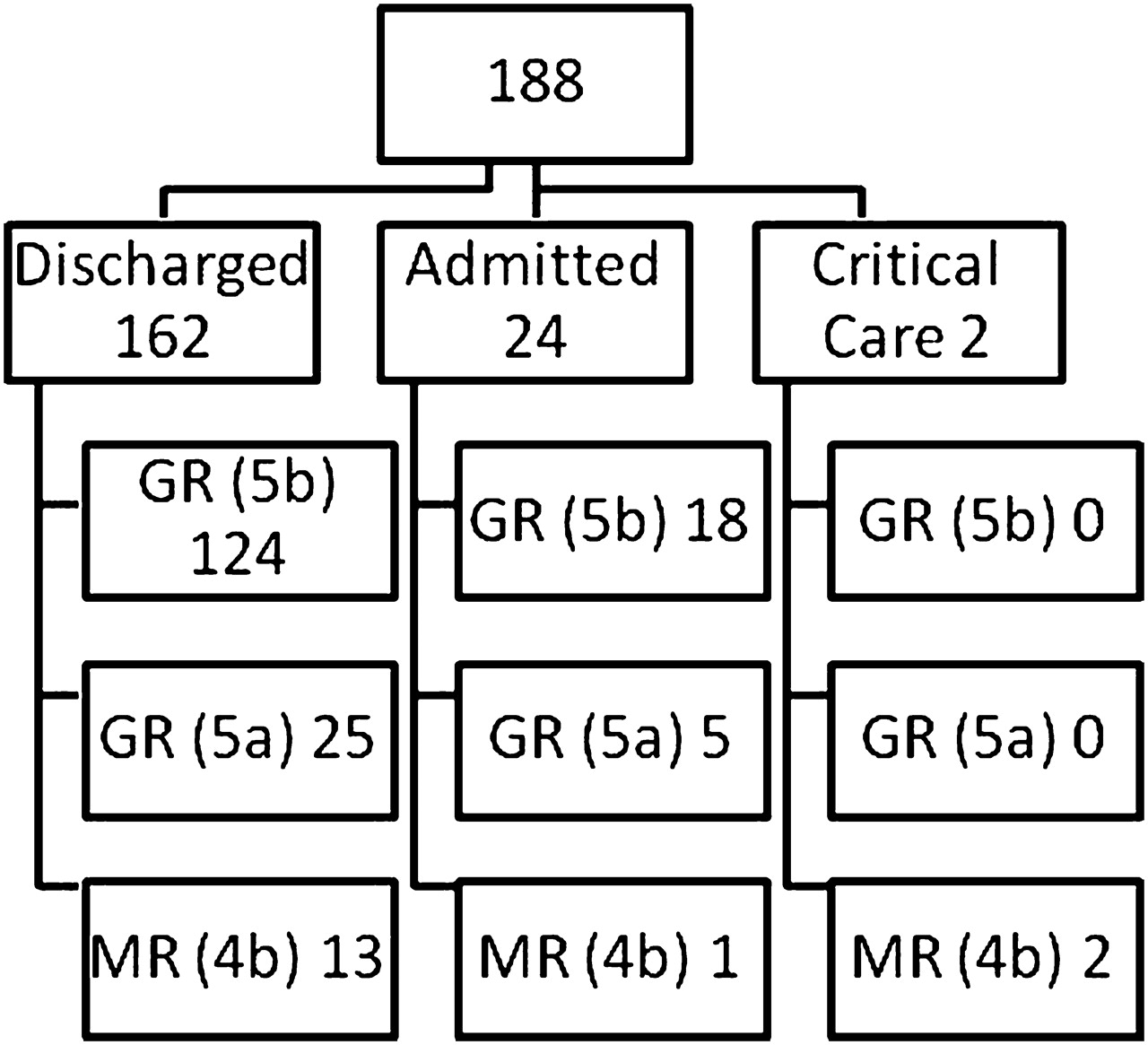
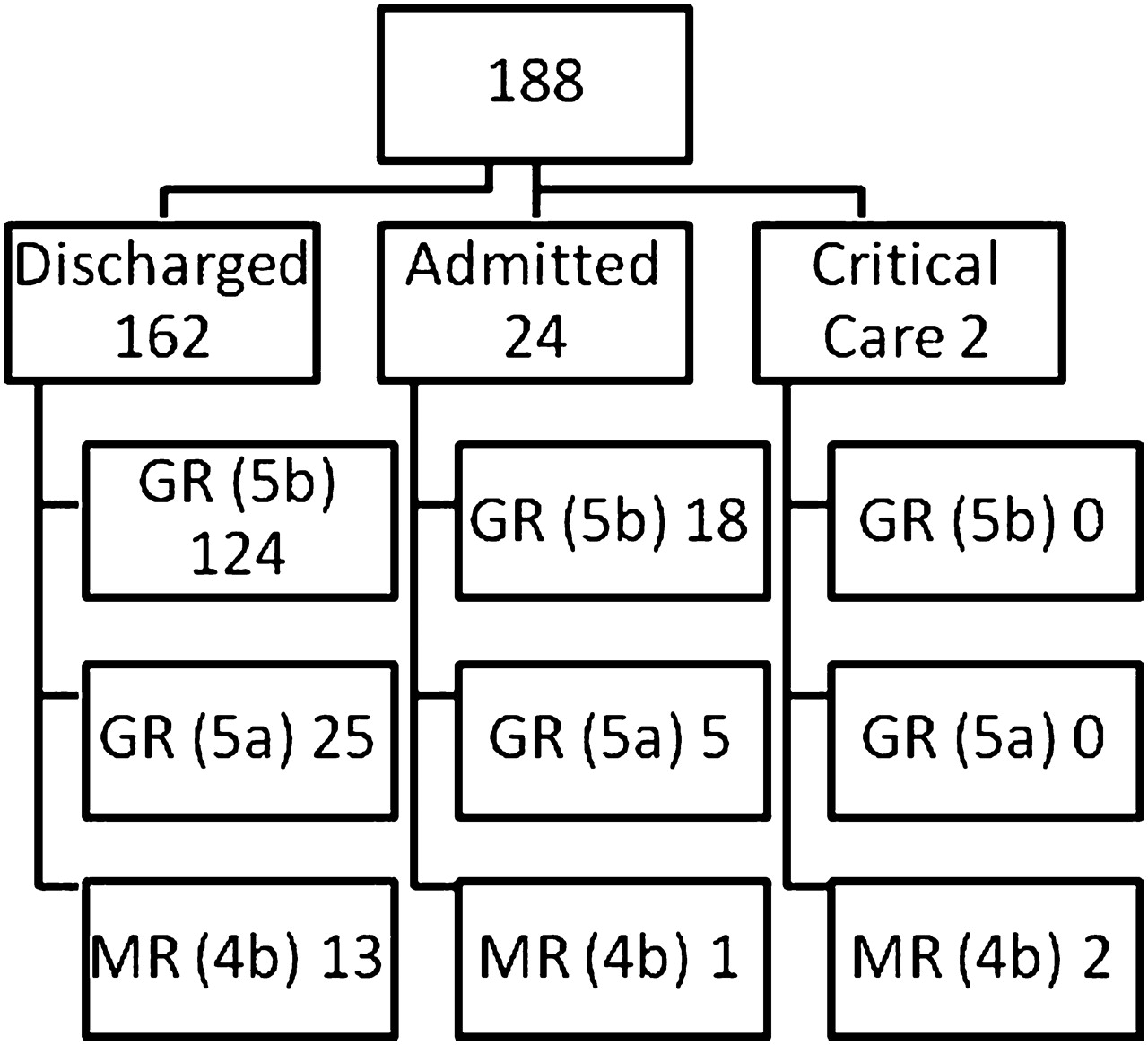
From the 188 subjects, 142 (75.5%) had made a full recovery 1 month following injury (KOSCHI 5b or GOSE 8). Thirty (16%) had mild symptoms but stated that they were not affecting activities—the majority of these were headaches or scarring. This was the good recovery group, category 5a (GOSE outcome of 7). Sixteen (8.5%) were classified as having made a moderate recovery following their injury. This was category 4b (GOSE outcome of 6) or worse.
The outcome scores by admission status are shown in figure 1. Outcome category at 1 month by mechanism of initial injury was assessed (see table 2). The two groups with the highest proportion of subjects with disabling symptoms were those involved in a road traffic collision (15%) and those assaulted (13%). No patients injured while participating in sports appeared to have any significant difficulties at 1 month, with only 5 (13%) having minor symptoms.
{kind=link}
Outcome scores by admission status.
Breakdown of progress interview results by mechanism of injury
Following NICE guidelines, 11 patients (11/188) had a cranial CT for their injury. Seven of these patients had negative scans and had made a full recovery by the 1-month progress interview. The remaining four were positive, with findings and outcomes shown in table 3.
Data for patients with positive CT scans
Six-month follow-up
The 16 patients who had only made a moderate recovery at the progress interview were contacted again, between 6 and 9 months following the initial injury, for a second interview or outcome interview. Four of these 16 were lost to follow-up.
Only one of those interviewed after 6 months had completely recovered with no residual effects. Eleven (5.9%) of those initially recruited continued to have ongoing symptoms 6 months following their head injury. Five (2.7%) of these still had a disability as a direct result of the injury.
Nine of the 11 (82%) subjects still experiencing symptoms at the outcome interview were assaulted as their initial mechanism of injury.
Using the SPSS (V.14) database tools, potential predictive factors for poor outcome were analysed using logistic regression methods (see table 4).
Binary logistic regression model for poor outcome after 6 months
Analysis showed two potential predictors of poor outcome at 6 months in our model. These were:
Assault as the mechanism of injury (when dichotomised into assaulted or not assaulted).
A Glasgow Coma Score (GCS) <15 at presentation (GCS 15 vs GCS <15).
No statistically significant association was shown between the assessment GCS or mechanism of injury and the presence of symptoms after 1 month, as demonstrated with the 6-month outcome results. Admission status, need for CT1 and positive CT did not show any statistically significant association with poor outcome after 1 or 6 months when analysed as individual variables. These latter two variables were not independent of reduced GCS, so analysis was not possible using all three together.
Discussion
We have shown that in head injured 13–21-year-olds in full-time education, 24.5% (95% CI 18.9% to 31.1%) have disabling symptoms 1 month after injury, with 5.9% (95% CI 3.3% to 10.2%) of the total cohort having disability at 6 months. A low GCS and assault as mechanism of injury predict the late disability. Early disability was not predictable by mechanism in our large cohort. Almost 3% experienced disability that continued to affect daily activities. This prevalence of post-concussive symptoms (PCS) after 6 months, in the adolescent population in full-time education, was less than previously reported in the ED population.6 16 17
Variations of definition of head injury and outcome measure may explain some of the difference. Our inclusion criteria were deliberately inclusive, as we were not convinced that head injury consequences are confined to those with accepted notions of a baseline of severity characterised by altered consciousness. We have included many with minimal injury, but in doing so we did identify head injured patients with sequelae that would have been excluded from previous studies. Moreover, the finding that 13/16 (81%) with disability and 38/46 (83%) with any symptoms after 1 month had been discharged directly from the ED would suggest that only identifying and following those admitted to hospital misrepresents the burden of morbidity following head injury.
The factors, identifiable at presentation, relating to poor outcome 6 months after injury, for this study group, were:
Having a Glasgow Coma Score of less than 15 at presentation.
Sustaining the head injury from an assault.
The majority of adolescents presenting to the ED with head injury who are in full-time education appear to recover promptly. However, as other investigators have found, there is a proportion that have persistent disabling symptoms. The cause of these is still not clear. Our study suggests that this is a small proportion of the entirety of those attending the ED with a blow to the head. Given the incidence of head trauma—estimated at one million attendances each year to UK emergency departments,18 this still represents an important health concern.
We found a comparatively large proportion of assaulted patients (45%) in our cohort. Estimates in the adolescent population have been between 1% and 5%,6 9 and 1.4–12% in adults.7 19 One reason may be the exclusion of patients under the influence of alcohol and drugs in a number of early studies. Dikmen et al20 noted that these influences may act as a confounding factor in those patients who might otherwise have a GCS of 15 following their head injury. As such they suggested that future studies include intoxicated patients—as in this current study. It may be a result of the nature of the populations served by the EDs in the study. Hull has the highest rate of violent crime in England and Wales (Public Health Observatory data, 2007).
Assault has been shown to be an independent predictor of outcome in previous studies, and there is a suggestion that post-traumatic stress will confound neurological outcome assessment in these patients.21 22
Limitations of this study
We did not include non-head injured trauma controls in our study. This approach has previously been adopted,16 as a proportion of non-head injured trauma patients demonstrate PCS at follow-up, and a baseline level of symptoms and disability may exist in the target population.
The outcome measures utilised for this study were designed to identify changes in symptoms and function, not just to identify the existence of such problems. The interview was conducted to detect such a change from pre-injury, and so represent an above baseline rate of disability. However, we cannot report whether the outcomes we found relate to traumatic brain injury alone or to other factors related to the episode.
We only followed up those with problems at 1 month to the 6-month time point. This could be considered a significant loss to follow-up rate but the decision was made based on the definition of PCS. While we recognise that it has been reported that some symptoms may manifest themselves later following injury,23 24 and that we would have missed them, the definition of PCS with DSM IV ‘require symptom onset or worsening to be contiguous to the head injury…’. So subjects who are problem free after 1 month could not be considered symptomatic as a direct result of the head injury sustained if found symptomatic after 6 months.
Conclusion
A period of reduced academic function following head injury could produce lifelong effects for the individual. Early intervention4–7 to reduce such effects would need a response initiated in the ED, and should include those discharged directly to the community after assessment. The assaulted population appears to be at increased risk and may be an initial group on whom to focus simple follow-up efforts.
References
Footnotes
Funding The authors would like to acknowledge the financial support of the British Association of Emergency Medicine towards research support staff in Hull.
Competing interests None.
Ethics approval This study was conducted with the approval of the North Humberside LREC.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Primary survey