Article Text

Abstract
A number of emergency departments have introduced non-invasive positive pressure ventilation (NIV) and continuous positive airway pressure (CPAP) for patients presenting with acute respiratory failure. It is thought that early non-invasive respiratory support will avoid the need for invasive ventilation in many cases. This literature review studied current knowledge of NIV and CPAP in the acute setting with the aim of creating simple guidelines for hospitals initiating early non-invasive ventilatory support in emergency departments. NIV is effective in reducing intubation and mortality rates in patients with acute exacerbations of chronic obstructive pulmonary disease (COPD) and CPAP is effective in reducing mortality in patients with cardiogenic pulmonary oedema, especially when implemented early. NIV and CPAP were also found to be effective in some other causes of acute respiratory failure. There is a role for non-invasive respiratory support in emergency departments.
Statistics from Altmetric.com
Non-invasive ventilation has been possible since Woillez invented the first workable iron lung in 1876, working on the same principles as the machine popularised by Drinker in the late 1920s. These early mechanical ventilators relied on negative pressure for chest expansion and managed to support patients with respiratory failure due to poliomyelitis. These devices fell out of favour in the 1950s and 1960s as newer ventilators relying on positive pressure were introduced. Positive pressure ventilation was found to be more effective, but for many years required invasive routes for gas exchange to occur in the lungs which has its own disadvantages.
Non-invasive methods of gas exchange subsequently evolved in the form of non-invasive positive pressure ventilation (NIV) and continuous positive airway pressure (CPAP). These have been used to great effect in the treatment of chronic conditions such as chronic obstructive pulmonary disease (COPD) and obstructive sleep apnoea. More recently their role in the emergency setting has been evaluated for acute respiratory failure (ARF) on a background of COPD or cardiogenic pulmonary oedema (CPO).
CPAP and NIV assist ventilation by reducing inspiratory work, recruiting collapsed and poorly ventilated portions of lung and improving alveolar ventilation, therefore enabling more efficient gas exchange. The alternating pressures in NIV (inspiratory positive airway pressure (IPAP) and expiratory positive airway pressure (EPAP)) enable improved ventilation and recruitment, respectively.
In 2000, Cross carried out a review of the role of NIV in the emergency department with the aim of reviewing its effects in ARF, and concluded that it appears to be effective and safe. However, it was noted that there was limited published experience, especially with regard to indications and contraindications.1 Since this review there has been an increase in the knowledge base for NIV and CPAP, but there are currently no specific guidelines for emergency department staff for the use of NIV or CPAP in patients who may benefit from early ventilatory assistance. This literature review creates simple-to-use guidelines for hospitals initiating their general use in emergency departments. It presents a flow chart for the use of NIV and CPAP in ARF which is validated and evidence-based, and examines some of the practicalities of their use including indications and contraindications.
METHODS
A literature review was conducted using Medline, Embase and the Cochrane database for entries up to and including week 3 of December 2006. Keywords used were “NIV”, “Non-invasive ventilation”, “NIPPV”, “Non-invasive positive pressure ventilation”, “BiPAP”, “Bilevel Positive Pressure Ventilation”, “CPAP” and “Continuous positive airway pressure”. Limits on the search were: (1) age ⩾13 years; (2) English language; (3) human subjects. The search results were reviewed and articles relating to the use of NIV and CPAP outside the acute setting were manually removed (eg, the treatment of obstructive sleep apnoea). Abstracts for the remaining articles were reviewed and full journal submissions were retrieved where available.
RESULTS
General considerations regarding the use of NIV and CPAP in emergency departments
General indications
At present there are three reasons for implementing NIV/CPAP in patients with ARF. These are:
as a treatment to improve or prevent worsening of ARF;
as an initial alternative to intubation in selected patients which could then be used if NIV fails;
as a ceiling of ventilatory support for patients where invasive ventilation would not be initiated if NIV/CPAP failed. This would be applicable where intubation is not suitable or is not deemed appropriate at the outset. An example might be patients with ARF in the terminal phases of a chronic illness.
Endotracheal intubation is an effective method of mechanically ventilating a patient with ARF but it has associated risks. NIV and CPAP offer an advantage over intubation as they reduce the level of intubation-associated complications such as nosocomial pneumonia.2 Another advantage of NIV and CPAP is that patients can be treated while they are still conscious. This allows the patient to communicate their condition to clinicians and therefore feel more integrated in their management, as well as allowing for better intake of nutrients.
Contraindications
Current information regarding contraindications is derived from exclusion criteria for trials and studies. There are few absolute contraindications to the use of NIV and CPAP and, arguably, none in cases where they are the ceiling of ventilatory support. The most important contraindications are:
coma/impaired consciousness
inability to protect airway or high risk of aspiration
life-threatening hypoxia
cardiorespiratory arrest
haemodynamic instability
facial trauma/upper airway burns or oedema
undrained pneumothorax
copious respiratory secretions
recent facial, upper airway or upper gastrointestinal tract surgery
Other more relative contraindications include:
confusion/agitation and uncooperativeness (this may be largely overcome by one to one nursing);
severe co-morbidities (should not necessarily preclude the use of NIV as this may be more suitable than admission to the ITU (intensive therapy unit) for some patients with multisystem disease);
high risk of pneumothorax (the risk of barotrauma from NIV and CPAP is generally believed to be low but patients with COPD may have bullae and therefore be at higher risk of developing a pneumothorax which can subsequently be made larger by NIV/CPAP; a more cautious approach with higher levels of monitoring may be required in these patients rather than not using these therapies).
Practicalities of NIV and CPAP therapy
NIV and CPAP can be delivered though several ventilator-patient interfaces. These include full face masks (covering the nose and mouth), nasal masks which rely on the patient keeping his/her mouth shut during treatment and helmets. Kwok et al3 found that full face masks tended to be slightly better than nasal masks and had a higher level of tolerance in patients with ARF. Face masks may also be more appropriate because patients with ARF are usually mouth-breathing when tachypnoeic so the use of a nasal mask would lead to excessive air leak. Racca et al compared the use of CPAP helmets with a face mask in patients with ARF and found that the helmet was inferior in unloading respiratory muscles with pressure support ventilation.4 Other authors have concluded that they may be of use, but have not compared them with other interfaces.5
As a minimum, routine monitoring should include continuous Spo2 monitoring over at least the first 24 h, arterial blood gas analysis at T = 0 and 1 h, and 1 h after alterations in ventilator settings and regular clinical evaluation (chest wall movement, coordination with ventilator, use of accessory muscles, heart rate, respiratory rate, patient comfort and mental state).6 It may be possible to use capillary gas monitoring rather than arterial blood where facilities exist. Results from routine monitoring should enable adjustment of ventilation to optimise treatment. It is possible to treat patients on general wards rather than in ITUs, although ITU admission for at least the first few hours of treatment should be considered, especially in the more severe cases of ARF or in patients at higher risk of complications. This can help prevent any unnecessary delay in intubation in patients whose condition deteriorates.
In keeping with the randomised controlled trials that have been carried out, it is suggested that standard medical therapy is given alongside any ventilatory support that is required in patients with ARF. This can be achieved by following local protocols.
The use of NIV and CPAP does not have to be continuous, and these modes of ventilatory assistance allow the patients to be able to eat, drink and communicate. Results from studies have shown varying lengths of time of ventilatory assistance received both over the first 24 h and the total duration of treatment. In general, studies have suggested that patients should receive as much NIV support in the first 24 h as possible before gradual weaning as symptoms begin to improve. However, some patients will show a clinical improvement much quicker than this, to a point where ventilatory support is no longer needed after just a few hours. Weaning may not be necessary for these patients.
Predictors of success and failure
Several studies have looked at the factors that may influence the success of NIV and CPAP in patients with ARF. Factors associated with success include a lower PAo2–Pao2 gradient7 initially and an improvement in pH8 9 and/or reduction in respiratory rate after 1 h.8 Factors correlated with failure include a high APACHE score,10 lower pH values and higher Paco2 values.10 11 In contrast to what might be expected, Mani et al found that an initial deterioration in Paco2 and pH in patients with severe hypercapnia and respiratory acidosis may not be related to treatment failure. This is provided that there is a clinical improvement of the patient and their respiratory distress.12
Sometimes failure cannot be predicted by patient characteristics before the implementation of NIV or CPAP. Rates of failure and complications of treatment other than those stated above are not well publicised and are often just noted as being lower than with invasive ventilation. Possible reasons for treatment failure and complications include (but are not limited to) poor tolerance and poorly fitting masks, soft tissue trauma from the masks and straps, gastric distension, aspiration and barotraumas.
Chronic obstructive pulmonary disease
Since the early 1990s, interest has been growing in the use of NIV and CPAP in patients with an acute exacerbation of COPD. These patients are usually suffering from acute hypercapnic respiratory failure and so are characteristically acidotic and have an increased Paco2 as well as being hypoxic. The aim of NIV and CPAP is to reverse these physiological abnormalities while relieving dyspnoea and avoiding intubation. Randomised controlled trials and other studies have evaluated the use of NIV in patients with an acute exacerbation of COPD, both on ITUs and general wards.
Studies carried out on ITUs have clearly shown that NIV reduces the rate of intubation.8 13 14 In trials conducted outside ITUs there have, however, been variable results. Plant et al (in the best designed and implemented randomised controlled trial) found a reduction in the need for intubation (from 27% to 15%) and in-hospital mortality (from 20% to 10%) with the use of NIV.15 A Cochrane review for studies both in and out of ITU found that NIV compared with standard therapy led to a 48% reduction in the relative risk of mortality (NNT = 10) and a reduction of approximately 60% in the relative risk of intubation (NNT = 4).16 Importantly, any potential benefit would be lost if the introduction of NIV led to a delay in intubation for patients with more severe exacerbations.
Balami et al investigated the use of bilevel positive pressure ventilation (BiPAP) in patients aged over 65 years and found similar success rates (79%) to other studies which tended to look at its use in younger patients.17 Scala et al studied the effects of co-morbidities on the outcome of NIV in patients with an acute exacerbation of COPD. As might be expected, they found that both acute and chronic co-morbidities led to poorer outcomes, especially if there was greater than one acute co-morbidity and especially if any were cardiac in origin.18
Mode of ventilation
Most studies to date have examined the use of NIV rather than CPAP, with no randomised controlled trials for the latter. For this reason and because randomised controlled trials for the use of NIV have shown a benefit, NIV would seem to be preferential to CPAP. Currently, there is no evidence to suggest that CPAP would be contraindicated in patients presenting with an acute exacerbation of COPD. BiPAP has been the method of NIV in most trials. Patients presenting with severe exacerbations of COPD may, however, become fatigued on CPAP and need to be monitored closely for worsening respiratory acidosis and CO2 retention. There may be a benefit in using proportional assist ventilation rather than pressure support ventilation,19 but more evidence is needed to support this.
Commencing treatment
There is no evidence for the best method for commencing NIV for an acute exacerbation of COPD. Protocols in studies have often begun with an inspiratory pressure of around 10 cm H2O, increasing to 20 cm H2O or to the maximum tolerated over the first hour. Expiratory pressures have usually been set at 2–4 cm H2O, but an EPAP of 4 cm H2O would be suggested for most patients to overcome intrinsic airway collapse. The fraction of inspired oxygen should be adjusted to maintain SpO2 at 90–92% unless the patient is known to have oxygen saturations chronically lower than this.
Cardiogenic pulmonary oedema
A meta-analysis study by Peter et al20 found that, in patients with acute cardiogenic pulmonary oedema (ACPO), CPAP offered a significant survival advantage over standard treatment (relative risk (RR) = 0.59 (95% confidence interval (CI) 0.38 to 0.90)). BiPAP does not appear to offer the same advantage. Both CPAP and BiPAP significantly decrease the need for intubation, with no significant difference between the two modes of ventilation (RR = 0.44 (95% CI 0.29 to 0.66) and 0.50 (95% CI 0.27 to 0.90), respectively).20 Contrary to results from an earlier trial,21 more recent studies, including one by Bellone et al,22 have not found an increased risk of acute myocardial infarction in patients receiving BiPAP rather than CPAP. Hubble et al looked at the use of CPAP in the prehospital setting (ie, early implementation of ventilatory support). In their non-randomised control trial they found a significant reduction in the rate of intubation between those receiving standard treatment and those receiving CPAP on top of standard treatment, with an absolute reduction from 28.12% to 6.66% (p = 0.001). Mortality was also reduced from 25% to 5.55% (p = 0.001).23 This study shows that early implementation of CPAP appears to be equally or more effective in patients with ACPO than later implementation, although no randomised controlled trials have specifically confirmed this.
Mode of ventilation
CPAP appears to be more effective than BiPAP in the treatment of ACPO and therefore should be used in preference. It is suggested that BiPAP should be reserved for those in whom CPAP is unsuccessful.6 Again, the fraction of inspired oxygen should be altered to maintain Spo2 at 85–90%. CPAP is normally given at 10 cm H2O, with or without titration to this level.
Other conditions where CPAP or NIV may be indicated
Chest trauma and flail chest
Two randomised controlled trials have shown advantages of using CPAP with regional analgesia in patients with flail chest compared with intubation.2 24 In a prospective observational study, Xirouchaki et al25 observed benefits when using NIV/CPAP in patients with blunt thoracic trauma. CPAP is currently recommended in patients with chest wall trauma if they remain hypoxic despite high flow oxygen and adequate analgesia.6 This recommendation has been strengthened by the more recent study by Gunduz et al.2 The lack of evidence supporting the use of NIV rather than CPAP in these patients means that it should not be a routine part of the treatment of patients with chest wall trauma. Because of an increased risk of pneumothorax in these patients, ventilatory support should be implemented on an ITU.6
Asthma
Currently there is a general lack of trials looking at the effect of NIV and CPAP in the treatment of exacerbations of asthma. Early results show potential for the use of these therapies (Meduri et al26 in a retrospective study and Soroksky et al27 in a randomised controlled trial both found BiPAP to be effective in the treatment of exacerbations of asthma). Despite this, it is suggested that they should not be used routinely until more is known about their safety and efficacy.6
Pneumonia
In a randomised controlled trial carried out by Confalonieri et al, NIV significantly reduced respiratory rate in the first 24 h in patients with community acquired pneumonia (CAP) where standard treatment did not. There was also a significant reduction in the requirement for intubation (50% vs 21%, p = 0.03) and mean (SD) number of days in the ITU (6 (2) vs 1.8 (0.7) days, p = 0.04). There was, however, no significant difference in hospital mortality.28 Patients with COPD and pneumonia are thought to benefit particularly from NIV. Case reports and case series have also supported the use of CPAP and NIV in patients with severe CAP,29 varicella pneumonia29 and CPAP in patients with Pneumocystis jiroveci pneumonia (also known as Pneumocystis carinii pneumonia or PCP).30
Others
NIV and CPAP have also been reported to have been useful in the management of respiratory failure associated with pulmonary embolism,31 hypothermia,32 malignancy,33 34 near drowning,35 myasthenia gravis,36 burns37 and acute respiratory distress syndrome.38 The usefulness and safety of CPAP and NIV has been questioned in chronic restrictive lung disease39 and Guillain-Barré syndrome.40
DISCUSSION
CPAP and NIV are safe and effective methods of assisting ventilation in patients with ARF. Traditionally, CPAP and NIV have been seen as treatments implemented by respiratory physicians. However, patients will benefit from early implementation of these therapies which therefore should also be available in emergency departments. Patients will benefit particularly from reduced intubation rates, along with the associated risks, and an overall reduction in mortality. Currently, there is good evidence to support the use of CPAP and NIV in CPO and acute exacerbations of COPD, but caution should be exercised for use in other conditions because there is less supporting evidence. Emergency physicians require training and education in the appropriate use of NIV.
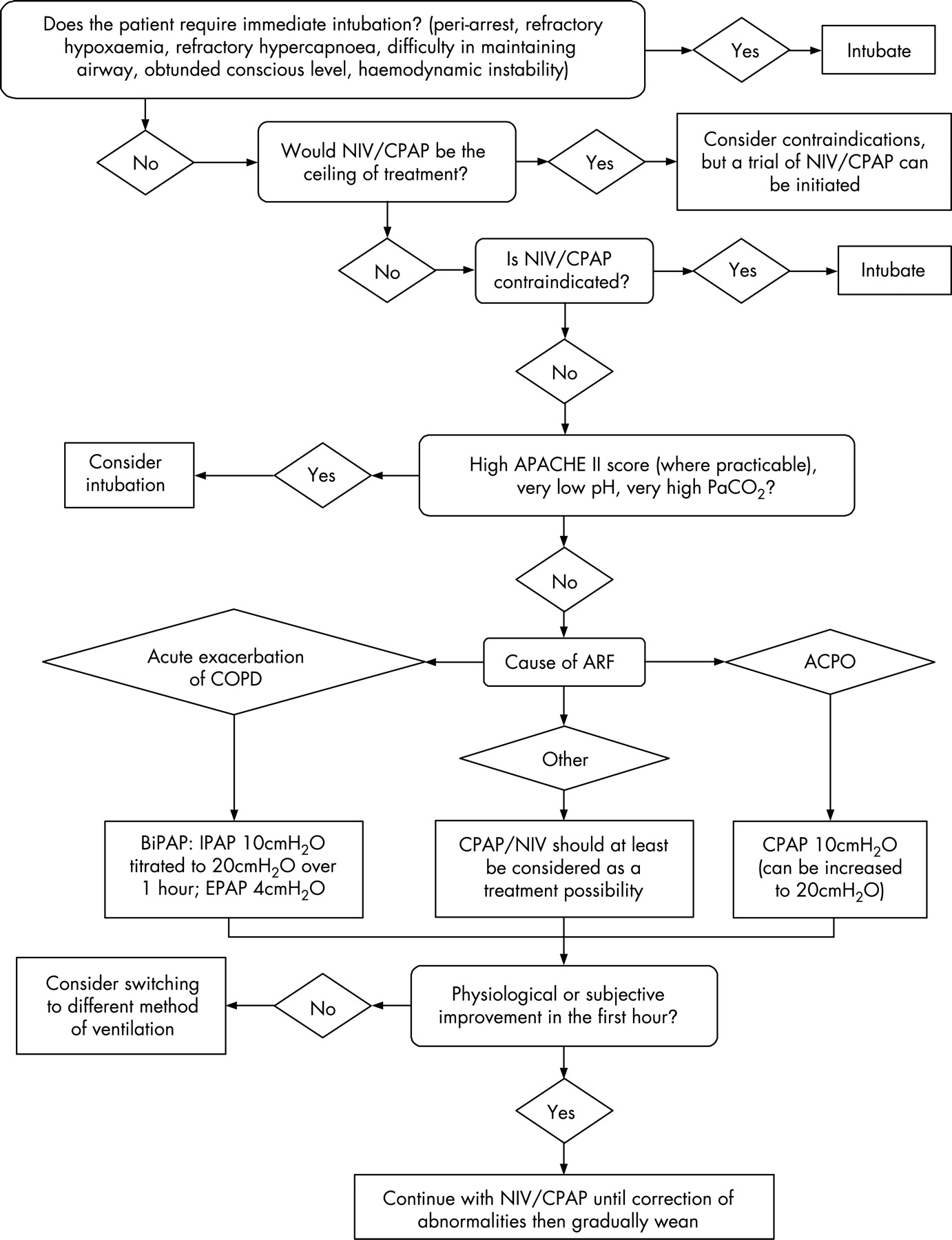
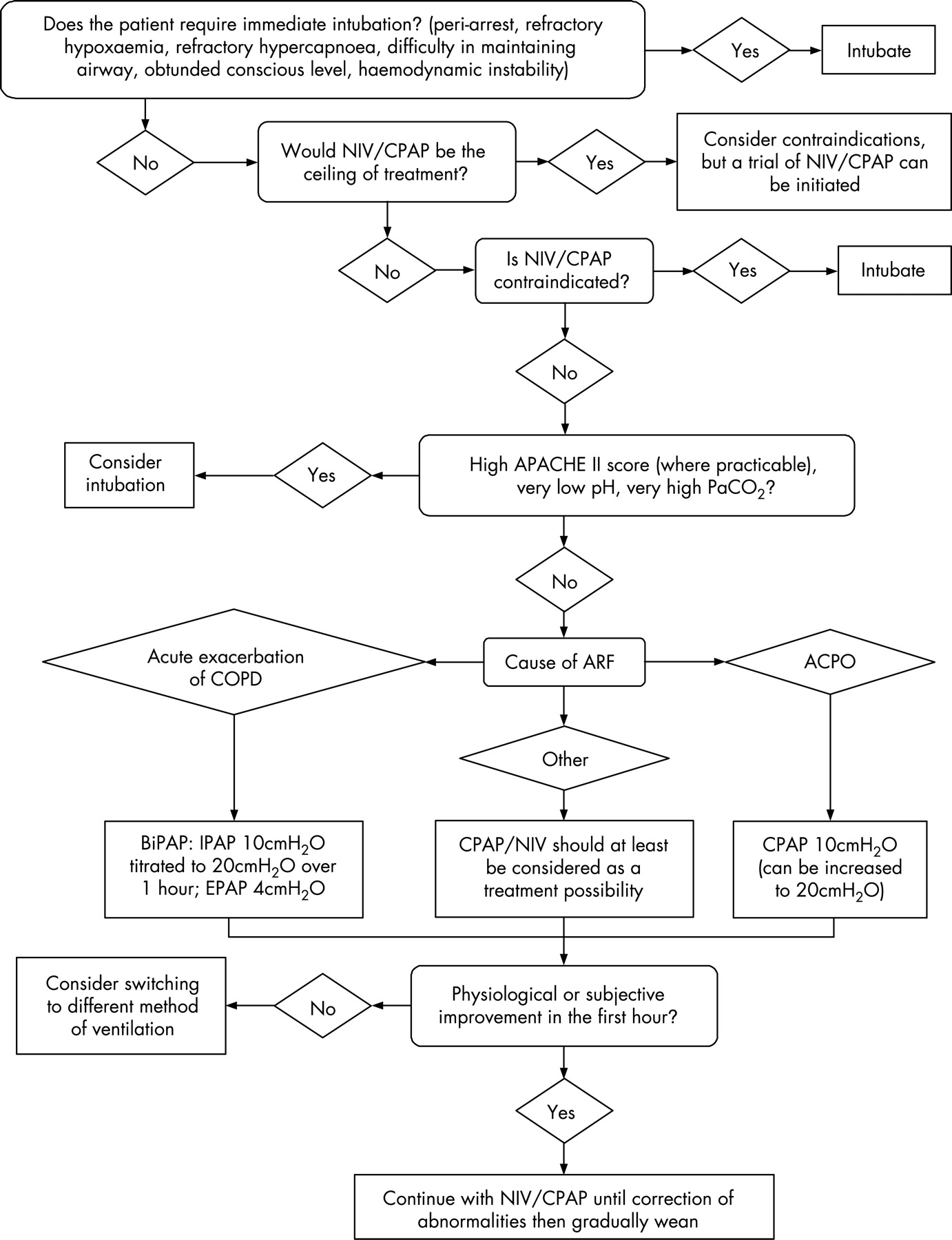
A validated evidence-based flow chart for use of NIV is presented in fig 1. This is offered as a starting point for emergency departments who wish to offer NIV to those patients who would most benefit from early implementation. We acknowledge that local guidance may influence some of the parameters and decision making.
{kind=link}
REFERENCES
Footnotes
Competing interests: None declared.
Linked Articles
- Primary survey