Article Text

Abstract
Introduction Severe sepsis and septic shock (SS) are time-critical medical emergencies that affect millions of people in the world. Earlier administration of antibiotics has been shown to reduce mortality from SS; however, the initiation of early resuscitation requires recognition that a patient may have sepsis. Early warning scores (EWS) are broadly used to detect patient deterioration, but to date have not been evaluated to detect patients at risk for SS. The purpose of our study was to look at the relationship between the initial national EWS (NEWS) in the emergency department (ED) and the diagnosis of SS.
Methods We performed a retrospective, single-centre, observational study in the ED of an urban university hospital with an annual attendance of 140 000 patients. We aimed to include 500 consecutive non-trauma adult patients presenting to the ED with Manchester Triage System (MTS) category 1–3. The final diagnosis was taken from either the ED medical records or the hospital discharge summary. For all NEWS, the sensitivity and specificity to detect patients with SS was calculated.
Results A total of 500 patients were included, 27 patients (5.4%) met the criteria for SS. The area under the curve (AUC) for NEWS to identify patient at risk for SS is 0.89 (95% CI 0.84 to 0.94). A NEWS of 3 or more at ED triage has a sensitivity of 92.6% (95% CI 74.2% to 98.7%) and a specificity of 77% (95% CI 72.8% to 80.6%) to detect patients at risk for SS at ED triage.
Conclusions A NEWS of 3 or more at ED triage may be the trigger to systematically screen the patient for SS, which may ultimately lead to early recognition and treatment.
- infection
- resuscitation
- emergency department management
- diagnosis
- bacterial
Statistics from Altmetric.com
Key messages
What is already known on this subject?
A standardised national early warning score (NEWS) has been introduced in the UK for early detection of patient deterioration. While NEWS on arrival to the emergency department (ED) has been shown to correlate with adverse outcome in patients with septic shock, its use in detecting septic shock on arrival has not been studied.
What this study adds?
In this retrospective, single-centre study in a high volume ED in London, a NEWS of 3 predicted patients at risk of septic shock with a sensitivity of 92% and specificity of 77%. The NEWS score could potentially be used as a trigger for early detection and treatment of septic shock.
Introduction
Severe sepsis and septic shock (SS) are time-critical medical emergencies that, every year, affect millions of people in the world and kill an estimated 37 000 people in the UK.1 ,2 A recent analysis of a hospital cohort consisting of almost 500 000 patients in the USA revealed that sepsis contributes to 1 in every 2–3 deaths and most of these patients had sepsis at the time of admission to hospital.3
Earlier administration of antibiotics has been shown to reduce mortality from septic shock, and the Surviving Sepsis Campaign advocates the early administration of antibiotics in all patients with SS.4–7 However, the initiation of early resuscitation requires recognition that a patient may have SS. Because of the ambiguous nature of its manifestation and non-specific symptoms, the diagnosis of SS in the emergency department (ED) remains challenging.8 Different scoring systems have been developed and evaluated for patients presenting to the ED with sepsis, but the studies looked at the prognostic value of the scores rather than validating their use for early detection and recognition of patients with SS.9–14
Early warning scores (EWS) are broadly used as track and trigger systems to allow early detection of patient deterioration.15 ,16 A standardised national EWS (NEWS) has been introduced for use in the NHS in the UK.17 Corfield et al14 evaluated the use of NEWS in patients with sepsis in the ED and revealed an association between increased NEWS on arrival and adverse outcome (intensive care unit referral and mortality).
To our knowledge, no study has yet evaluated the ability of NEWS to detect patients at risk for SS in the ED. Therefore, the purpose of our study was to look at the relationship between initial NEWS in the ED and a diagnosis of SS. We hypothesised that patients with SS would have an elevated NEWS, and this would alert ED staff to the potential for those patients to have SS and therefore to screen them for SS.
Methods
Design and study population
We performed a retrospective, single-centre, observational study in the ED of an urban university hospital with an annual attendance of approximately 140 000 patients. The ED is a tertiary centre for hyperacute stroke, acute myocardial infarction, cardiac arrest and major trauma.
Given that we did not know the prevalence of SS in our population, and we did not know the sensitivity of NEWS to identify SS, we were unable to accurately calculate a sample size. Therefore, we performed a data extraction of all patients ≥16 years old presenting to the ED and triage category 1–3 according to the Manchester Triage System (MTS) until we had a patient population of 500. The MTS is widely used throughout the UK and consists of five categories with 1 (‘immediate’) to 5 (‘non-urgent’).18 Patient details were identified using specific search criteria on the local ED information technology (IT) system (Ascribe Symphony), and their medical records were reviewed.
Patients were excluded if they had a presenting complaint of trauma, or if trauma was consequent to a medical complaint (eg, twisted ankle after collapse). We also excluded patients with MTS 4 and 5 because these patients were unlikely to have a full set of observations and blood tests. Further, we excluded patients where parameters to calculate the NEWS were missing, and if the patient presented with sepsis, but it was impossible to determine if the patient had SS as per the criteria in table 1.
Definitions
Data collection
Baseline characteristics, observation parameters and blood results (INR, white cell count, platelets, creatinine, bilirubin and lactate) were obtained from the patient's ED medical records, the hospital electronic patient record system, the inpatient medical records and the hospital discharge summary. The final diagnosis was taken from either the ED medical records or the hospital discharge summary.
Definitions
Systemic inflammatory response syndrome (SIRS), sepsis and severe sepsis were defined according to the most recent Surviving Sepsis Campaign guidelines, see table 1.5 ,19
The NEWS is based on a scoring system consisting of six physiological parameters: RR, oxygen saturation or requirement, temperature, systolic BP, pulse rate and level of consciousness. The NEWS in our study was calculated for each patient using the initially documented observation parameters in the ED of each patient using the toolkit endorsed by the Royal College of Physicians.17 See detailed information in table 1.
Statistical analysis
All analyses were performed using SPSS V.22.0 for Windows 8.1. The ability of the NEWS to identify severely septic patients was evaluated by plotting the sensitivity (true positives) against 1-specificity (false positives) using receiver operating characteristic (ROC) curves. The associated ROC area under the curve (AUC) was calculated to evaluate the overall performance of NEWS.
Ethics
The study was discussed with the local research and development department who deemed it exempt from ethical review.
Results
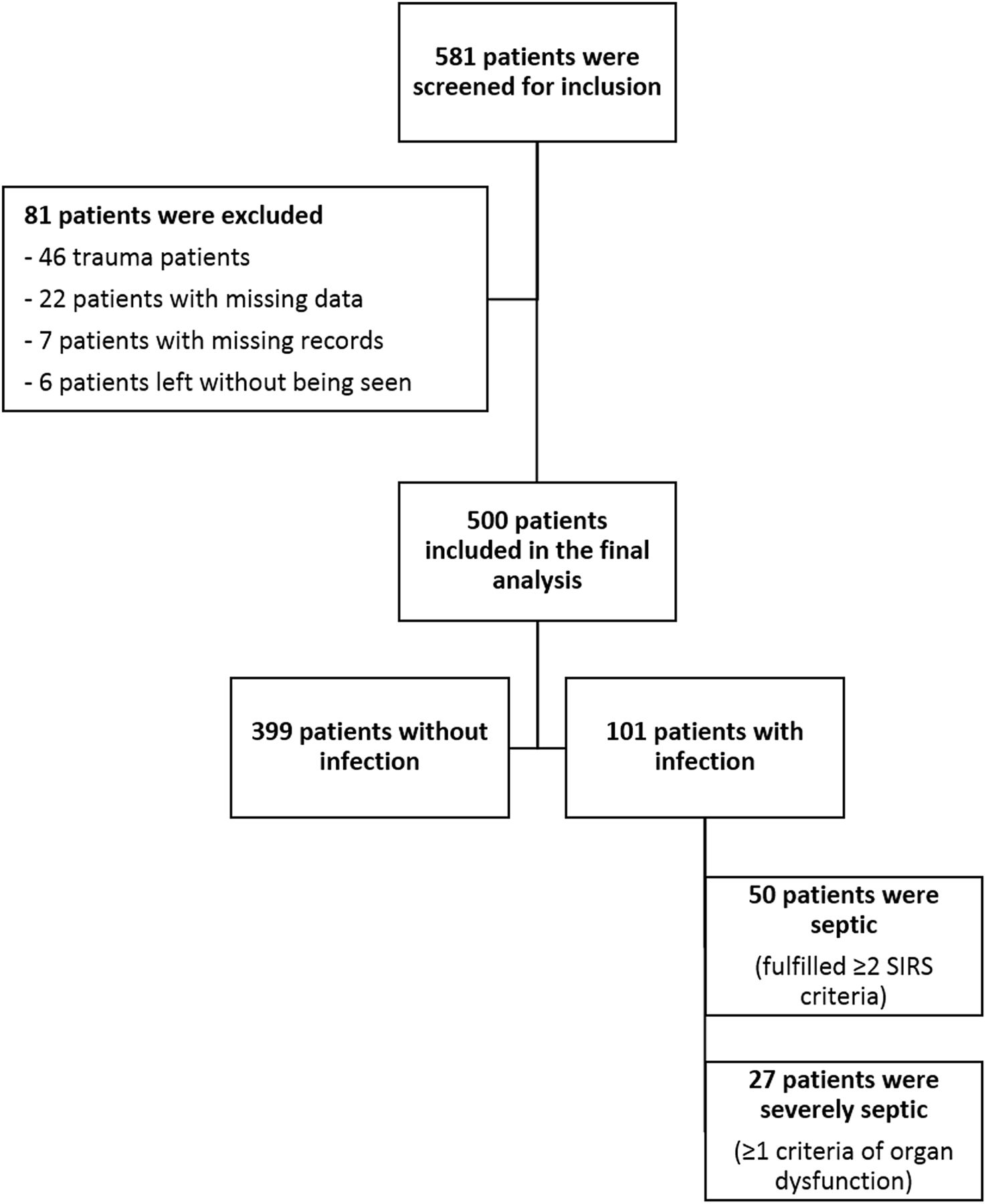
From 21 July 2013 until 26 July 2013, a total of 581 patients were screened for inclusion, of which 500 patients were included in the final analysis, see figure 1. Of the 500 analysed patients, the median age was 47 years (IQR 31/68), and 259 patients were female. The prevalence of sepsis was 9.8% (50 patients), and 5.4% (27 patients) met the criteria for SS; see table 2 for the baseline characteristics. The AUC for NEWS to identify patients at risk for SS is 0.89 (95% CI 0.84 to 0.94). A NEWS of 3 or more performed with the best ability to detect patients with SS with a sensitivity of 92.6% (95% CI 74.2% to 98.7%) and a specificity of 77% (95% CI 72.8% to 80.6%), see table 3 and figure 2. The positive predictive value is 18.7% (95% CI 12.7% to 26.5%), and the negative predictive value is 99.5% (95% CI 97.8% to 99.9%).
Patient population baseline characteristics

Flowchart describing patient inclusion. SIRS, systemic inflammatory response syndrome.
NEWS receiver operating characteristic (ROC) curve for severe sepsis and septic shock (SS)

{kind=link}
{kind=link}
National early warning score (NEWS) receiver operating characteristic curve for severe sepsis and septic shock.
Discussion
A survey among doctors and nurses in US EDs in 2007 revealed that one of the top-ranked barriers to implementing early resuscitation is the identification of patients with SS.20 Consensus guidelines recommend immediate diagnostic testing for all patients with SIRS criteria and suspected infection, but a recent study revealed that SIRS is common in the ED, and its lack of specificity for an infectious condition limits its utility as a sepsis screen.7 ,21 Additionally, blood results (namely the white cell count) are needed to assess for the SIRS criteria, which, depending on local ED circumstances, can take up to an hour or more. Most importantly, it also implies awareness at the time of ED triage of the possibility that the patient may have SS.
Physiological observations are routinely performed and are readily available on most patients at the time of ED triage, especially in patients with MTS 1–3. Furthermore, an EWS, such as the NEWS, is sometimes calculated as part of the initial patient assessment at triage. Using the NEWS at ED triage to identify patients who could potentially have SS would, therefore, not require an additional step in the patient's pathway in the ED.
The results of our derivation study show that the prevalence of SS in the ED is relatively low (5.4%). Therefore, screening all non-trauma adult patients with a MTS of 1–3 would be time-consuming for such a low return. Our retrospective analysis indicates that the NEWS may be an important intermediate step to detect patients at ED triage at risk of SS. From our results, a NEWS of 3 or more provided a good level of sensitivity (92.6%) with the least detriment to specificity (77.0%). We favoured sensitivity over specificity because the presentation of SS to the ED can be subtle. Given that NEWS is a measure of physiological derangement, those patients with a high NEWS may be more easily visible as unwell, and recognition of their illness is likely to be sooner. Therefore, screening for SS based on a sensitive tool may allow for earlier recognition of patients with more subtle presentations and allow consequent earlier instigation of treatment.
In practice, if we had only screened adult non-trauma patients with MTS 1–3 and NEWS ≥3 for sepsis, we would have performed a total of 134 sepsis screens and detected 25 patients with SS. However, we would have missed two patients with SS, both of whom had a NEWS of 2. Had we increased the threshold for sepsis screen to NEWS ≥4, we would have screened 84 patients, detecting 20, but missing 7. Therefore, by increasing the threshold for sepsis screen based on the value of NEWS, fewer patients will need to be screened for sepsis at triage, but more patients with SS will be missed at this early stage.
While there is a trigger to perform an ECG in all patients presenting to the ED with chest pain for the early recognition of ST-elevation myocardial infarction, there is no such trigger for early diagnosis of SS. A NEWS of 3 or more may be such a trigger to systematically screen for SS and look specifically for signs of infection, obtain an early serum lactate and, where appropriate, start fluid resuscitation and antibiotic therapy.
Limitations
There are some limitations to this study, and therefore, the results should be interpreted with caution. Our sample size was too low, and therefore, it is possible that a NEWS of 3 as the optimal threshold to perform a screen for SS may be a chance finding and would need to be tested in a new, adequately large dataset.
This was a retrospective review of patient records, and the original data were obtained and recorded for purposes other than this study. It is, therefore, possible that not all information was entered correctly, and 20 patients were excluded due to missing data. Additionally, all of the patients screened and eventually included for analysis presented to the same ED over a 5-day period, and therefore, our results may lack generalisability. Also, we analysed patients who presented in July, and the prevalence of SS may vary at different times of the year, which could alter the results.
Conclusion
A NEWS of 3 or more at ED triage may be the trigger to systematically screen the patient for SS, which may ultimately lead to early recognition and treatment.
We recommend that a prospective study be performed to confirm the association between NEWS, MTS (all categories) and the final diagnosis of SS. An accurate sample size for this study can now be calculated using the sensitivity and prevalence herein derived. An important addition to such a study could be the timings of the administration of antibiotics to those patients with SS to determine whether earlier detection of SS at triage will have positive practical implications for patients.
References
Footnotes
Contributors JWK, NB, RS and MT contributed substantially to the conception and design of the work and the acquisition. ASM, NB, RS and JWK contributed to the analysis and interpretation of the data. JWK, ASM, MT, RP, RS, NB and EG drafted the work or revised it critically for important intellectual content. All authors have given their final approval of the version published.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.