Article Text

Abstract
Background: There is uncertainty about the most efficient model of emergency care. An attempt has been made to improve the process of emergency care in one hospital by developing an integrated model.
Methods: The medical admissions unit was relocated into the existing emergency department and came under the 4-hour target. Medical case records were redesigned to provide a common assessment document for all patients presenting as an emergency. Medical, surgical and paediatric short-stay wards were opened next to the emergency department. A clinical decision unit replaced the more traditional observation unit. The process of patient assessment was streamlined so that a patient requiring admission was fully clerked by the first attending doctor to a level suitable for registrar or consultant review. Patients were allocated directly to specialty on arrival. The effectiveness of this approach was measured with routine data over the same 3-month periods in 2005 and 2006.
Results: There was a 16.3% decrease in emergency medical admissions and a 3.9% decrease in emergency surgical admissions. The median length of stay for emergency medical patients was reduced from 7 to 5 days. The efficiency of the elective surgical services was also improved. Performance against the 4-hour target declined but was still acceptable. The number of bed days for admitted surgical and medical cases rose slightly. There was an increase in the number of medical outliers on surgical wards, a reduction in the number of incident forms and formal complaints and a reduction in income for the hospital.
Conclusions: Integrated emergency care has the ability to use spare capacity within emergency care. It offers significant advantages beyond the emergency department. However, improved efficiency in processing emergency patients placed the hospital at a financial disadvantage.
Statistics from Altmetric.com
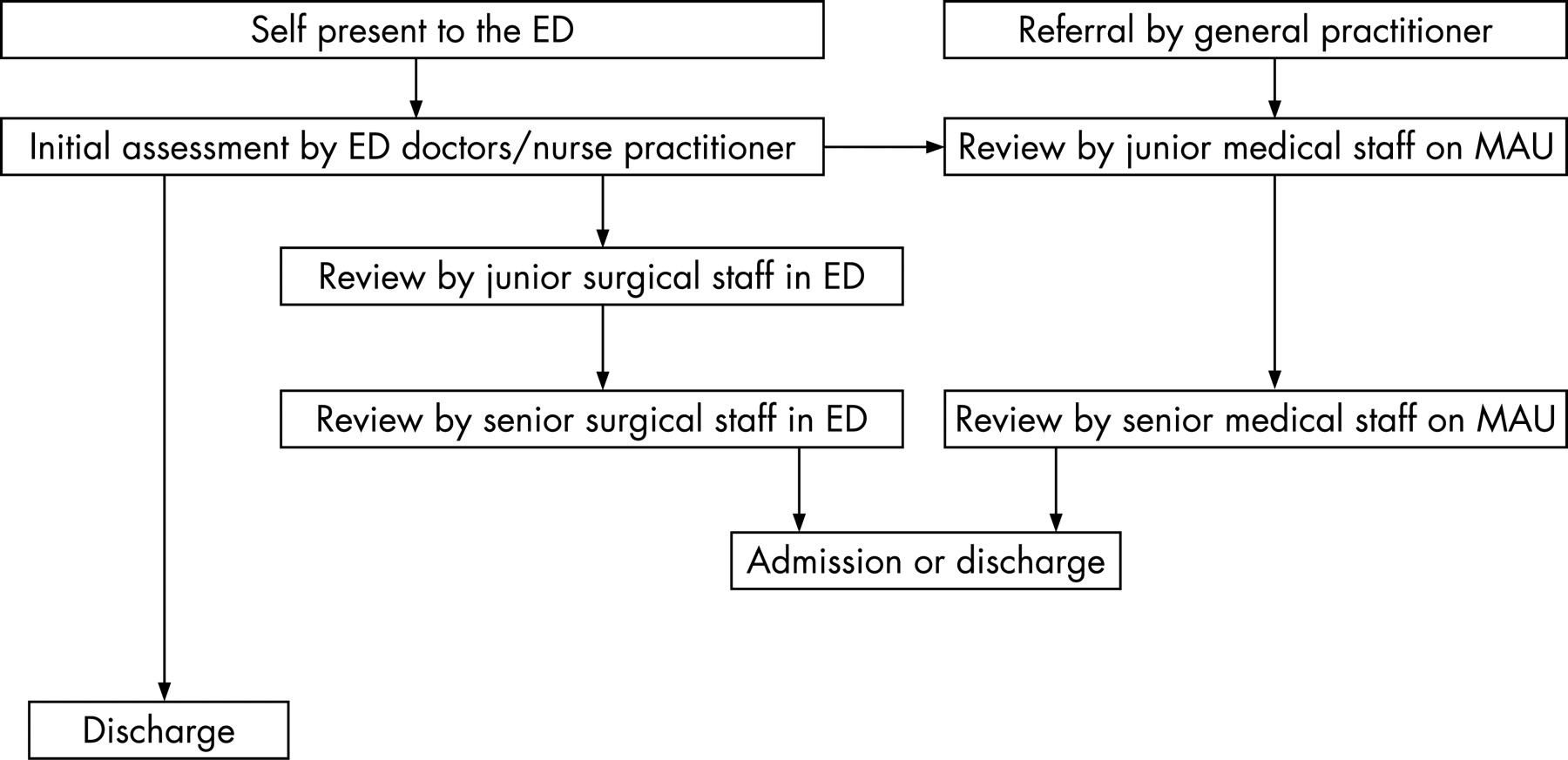
Emergency care is an imperfect system in the UK. The existing model is a consequence of emergent evolution rather than any planned system. The “traditional model” comprises the triage nurse and emergency department (ED) medical staff triaging patients to the appropriate specialty with variable levels of investigation and treatment. This model has much to commend it in terms of familiarity.
However, there are considerable inefficiencies and problems with this model of emergency care. Work through the Emergency Services Collaborative (ESC) highlighted problems with the processes of emergency care within our hospital. The major problem was that emergency patients were assessed in either the ED or the medical assessment unit (MAU) which were situated at opposite ends of the hospital, resulting in poor utilisation of resources, duplication of effort, inefficiency and unacceptable delays for patients.
Various strategies have been proposed to try and reduce time spent by patients in EDs. The 4-hour target (which requires that 98% of patients leave emergency departments in hospitals in England within 4 h of arrival) has improved patient processing, but there are concerns about the quality of patient care. Rapid streaming of ambulant cases is controversial but probably improves the overall response.1 The use of assessment and observation wards reduces inpatient length of stay and admissions to hospitals.2 3 The use of physician assistants reduces the length of time to key decision making in patients in emergency medicine departments.4 They provide phlebotomy, record ECGs, take arterial blood gases and can order radiographs for defined conditions before a patient is seen by a clinician.
We sought to improve the effectiveness of the hospital to deal with these issues by adopting an integrated medical model supported by four short-stay wards and personnel and process changes.
METHODS
Addenbrooke’s Hospital is a 1100-bed hospital providing all regional specialties except burns and cardiothoracic surgery. In 2005/6 there were 68 868 attendances to the ED and 10 748 attendances to the MAU. The development of the new Emergency Assessment Unit (EAU) required developments and changes in infrastructure, people and process. This whole process was supported by a major change implementation project.
Infrastructure
A substantial building programme provided a multimillion pound new EAU. The ED was enlarged significantly. The new building was sited behind the ED and comprised an eight-bed/eight-chair Clinical Decision Unit (CDU), a five-bed Children’s Observation Unit (COU), a 26-bed Surgical Short Stay Unit (SSSU) and a 26-bed Medical Short Stay Unit (MSSU) (fig 1). Within the main hospital, around 40 general medical beds were closed to provide staff and resources elsewhere. The SSSU ward was designed to accept all surgical specialty patients (orthopaedics, general surgery, plastics, maxillofacial and ear, nose and throat) that were expected to be discharged within 72 h.

Process
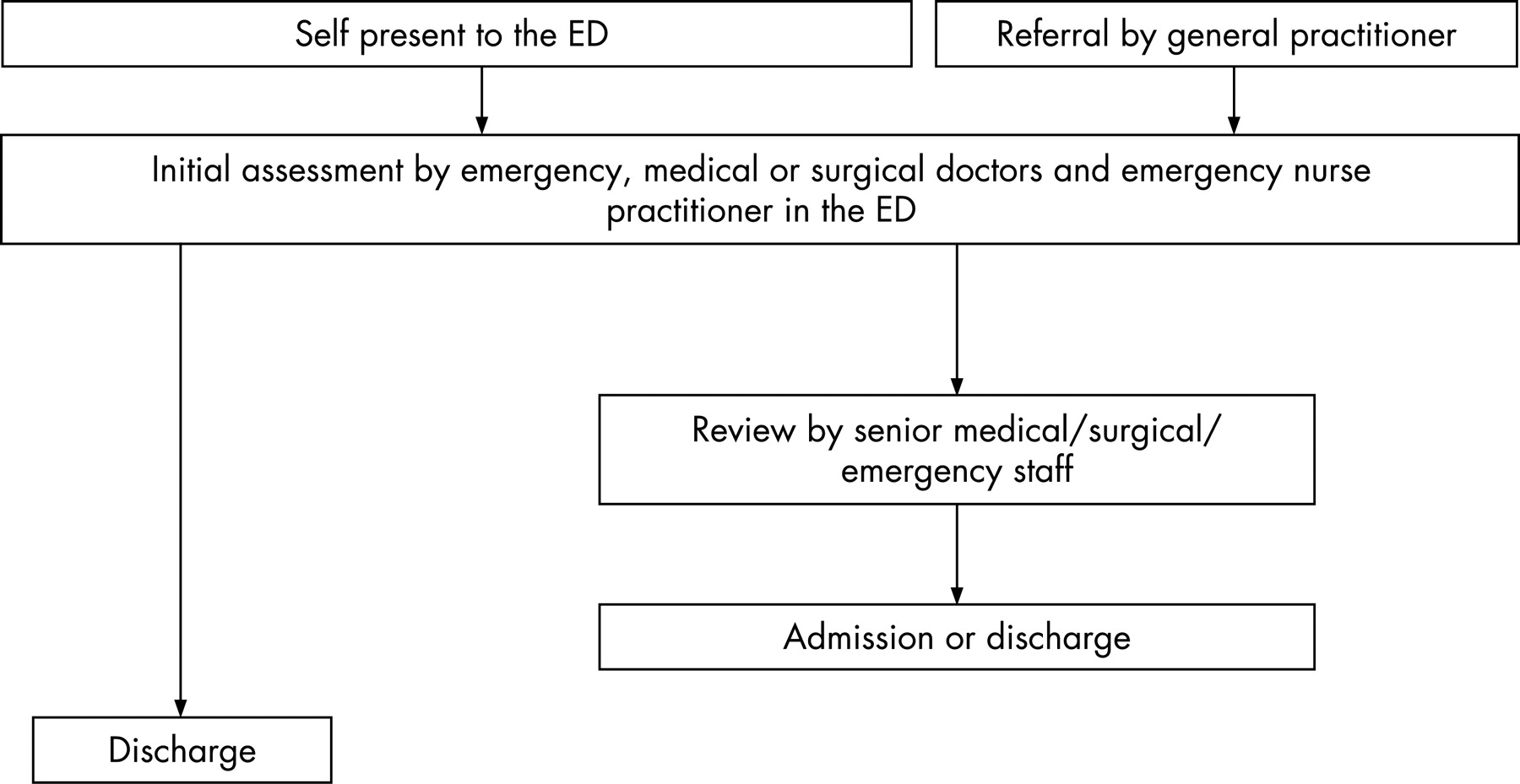
The admission documentation was changed so that all unplanned attendances and admissions to the hospital (except women in active labour) were recorded on a common case note, a new 8-page booklet. All unplanned admissions to the hospital were directed to the single door of the ED, except women in active labour (all the time) and women with obstetric and gynaecology problems (in office hours). Allocation to the most appropriate specialty and initiation of investigations was performed by the senior ED nurses with the support of physician assistants. Cases were directed immediately to the most appropriate specialty by the senior nursing staff. When a specialty was busy, support from other appropriate specialties was sought. For instance, if the ED staff were called to patients with multiple major trauma, the general and acute physicians would take the more obvious medical cases. Conversely, when the general and acute physicians were busy, the ED staff would support them by clerking in their patients. Close liaison between the general medical senior doctors and the senior ED staff aimed to identify those cases that could be investigated on the CDU such as patients with pleuritic chest pain. ED pathology requests were given priority and blood analysers were placed within the department, enabling the rapid availability of haemoglobin, urea and electrolytes, lactate, glucose levels and arterial blood gases.
The admission process was streamlined. A patient deemed to require admission was fully clerked by the first treating doctor (of whatever specialty) to the level suitable for secondary review by a senior doctor. This included providing written drug charts, ordering appropriate investigations, fluid charts and initiating treatment. There was also increased direct referral to tertiary level specialties. Service level agreements between all specialties with acute care responsibilities were made. These changes were implemented fully by the end of June 2006 (figs 2 and 3).


{kind=link}
{kind=link}
{kind=link}
People
The existing MAU was closed and an equivalent number of trolley spaces were opened in the ED. Doctors and nurses from the MAU were transferred to work in the ED. A new acute medicine service led by four consultants was introduced, supporting the general physicians and running the MSSU. Acute physicians have a relatively new role; they are responsible for the medical care of medical emergencies for up to 72 h.5 The roles of senior nursing staff were changed. A “flow nurse” role was generated to direct patients from the reception area to the most appropriate part of the ED. An EAU coordinator maintained real-time operational responsibility for the ED and movement of patients on from the department. There was significantly increased managerial support around the time of the EAU opening. Daily meetings led by an executive director and attended by senior representatives of all major specialties addressed any problems in the previous 24 h.
Outcome measures
The effectiveness and the quality of this approach were measured using routinely collected data. All outcome measures were taken between the second quarters of 2005 and 2006. We measured our performance against the 4-hour target. Bed capacity was measured using the number of medical patients on surgical wards and the hospital bed state at 09.00 hours, whether green (plenty of available bed capacity), amber, red or black (very little bed capacity). Admission rates for medical and surgical emergency admissions were compared. The number of elective surgical admissions cancelled was included. The median length of bed stay for surgical, paediatric and medical patients was compared for the two study periods. We also examined measures of quality of care—namely, incident reporting and formal complaints. The 28-day mortality and hospital standardised mortality days were compared. The numbers of new emergency attendances and case mix were analysed in an effort to exclude possible confounders. Changes seen locally were compared with national trends for emergency admissions.
Analysis of data
Statistical tests were performed with Stata Version 7. Statistical significance was assessed with the Mann-Whitney test for non-normally distributed continuous data and the χ2 test for categorical data. None of the continuous data was normally distributed.
We did not seek ethical approval since this was a service development and we were using routinely collected anonymous aggregate data.
RESULTS
The results are shown in tables 1 and 2. In the second quarter of 2006, 39.5% of GP referred patients were sent home from the ED. In the second quarter of 2005, all of these patients would have been admitted, if only for a few hours. Our non-elective admission rate per weighted 1000 population moved from the bottom quartile nationally into the second quartile. There was reduced capacity in the hospital. We recorded significant declines in the number of medical emergency admissions and shorter median lengths of stay for these patients. We admitted fewer surgical patients but the median length of stay was unchanged. There was no difference in the length of stay for paediatric emergency admissions. There appeared to be an increase in the efficiency of both elective and emergency surgical work. There was no significant change in paediatric emergency admissions. In the second quarter of 2005, five elective surgical operations were cancelled compared with two in the second quarter of 2006. There was no noticeable change in overall case mix (as defined by triage category) between the two quarters.
Our measures of quality show that the new process was associated with improvements (table 2). There were no high impact incident forms arising from the MAU or the ED during either study period.
DISCUSSION
We have integrated one hospital’s response to emergency care and found that it reduces the number of patients requiring admission to hospital. This effect is most apparent in the area of general medicine, but was also seen in surgical specialties. It seems that, by integrating all of the on-call specialties and making them work in the same place with a collective responsibility for workload, the number of admissions to hospital is reduced. Patients in the ED with conditions such as possible deep venous thrombosis or possible pulmonary embolism who can be sent home after early investigations are now counted as an “attendance”. Previously these cases would have been seen on the MAU and would have counted as an “admission”. However, the reduction in the number of surgical admissions cannot be explained by the attendance and admission difference described for medical patients because surgical patients referred by GPs have always been seen in our ED. We think it likely that senior ED doctors or senior surgical doctors are more prepared to make an earlier discharge decision on surgical patients, perhaps after a simple procedure. We were able to meet our 98% 4-hour target, but our performance against this suffered slightly. Bringing the general physicians under the constraints of the 4-hour target identified capacity problems and extra general medical staff were required in the evening.
There was a reduction in the median length of stay for admitted medical patients, despite the reduction in admissions. This is because short-stay wards are more efficient.3 5 This effect was less for surgical patients because their median length of stay was already very short. The median value is more valid as the data are highly skewed. Indeed, the increase in the mean values seen in this study reflects the increasing length of stay for long-stay patients.
There was an increase in the number of bed days for emergency medical and surgical patients. This implies that, although fewer patients are being admitted and the median length of stay is shorter, long-stay patients are staying even longer. We are uncertain of the cause of this but there are a number of possibilities. There have been some adverse changes in the local provision of community rehabilitation beds. Very elderly patients may not have gone directly to the most appropriate wards and this may have delayed discharges. The two populations may differ in terms of age and co-morbidity, although this seems unlikely.
We also found that the efficiency of the surgical unit was increased with more elective surgical patients being discharged within 1 day and fewer staying >1 day and >3 days. We think this is because the surgeons are able to manage their workload more effectively. Reduced numbers of admissions and length of stay were not seen in paediatrics, but the process changes have not been as marked in paediatrics as in other specialties and we think that paediatrics may have acted as a control.
Non-significant changes were seen in our measures of hospital mortality. There was a marked reduction in the number of incident forms and formal complaints arising from the ED. While these are imperfect tools for assessing the quality of care, the change suggests that the quality of care in the ED was improved. We feel that this is likely to result from a streamlined process and the ability to obtain earlier specialist opinions. The increase in medical outliers on surgical wards shows the effect of closing medical beds and is an area of concern; however, this did not reduce our elective activity or increase the number of surgical operations cancelled. The overall capacity of the hospital was less and this is indicated by the worsened bed state, as measured by the number of days on amber and red alerts and increased number of outliers. The number of patients not waiting and re-attending increased. These are usually low acuity patients and reflect the fact that the department is busier, with low acuity patients waiting longer. Adverse consequences are rare in patients who leave before treatment.6
The improved efficiency and reduced admissions has led to a decrease in income for the Primary Care Trust, since the hospital receives income from the Trust through a system known as “Payment by Results” and we treat patients more cheaply.
The role of the emergency physician was enhanced by this service design. After 1 year we found that ED doctors were seeing around 20% of the patients referred to general medicine by GPs, and that the general physicians were directly seeing around 20% of trolley-bound patients who arrived at the ED without a referral. Liaison between the general physicians and the ED aims to identify which patients can be rapidly investigated on the CDU. We also found that the general physicians are extremely grateful for the ready accessibility of the skills of the ED doctors—notably, in resuscitation, procedures, ultrasound and critical care.
There are limitations to this type of methodology and study. We did not use the conversion rate target as a measure of effectiveness. Our performance against this target has suffered because GP-referred patients have a higher rate of admission. Indeed, the Payment by Results system and a focus on conversion rates discourage our cheaper and safer system. We cannot be completely sure that the changes we saw were due to the interventions we put in place. We also cannot be sure which components of our complex intervention worked on which outcome measures. However, the data were collected without any overt bias. A confounding effect might be present in that there is an increasing demand for emergency health care and our population is older. The effect of this would be to lessen the strength of our findings.
Our approach seems to largely work for us. Clearly, local adaptation is necessary for different hospitals. Very few hospitals are of our size and have the range of our services on site. Whether the benefits that we have identified are transferable to smaller hospitals is not clear.
CONCLUSION
Combining all emergency care into one place has significant advantages in reducing admissions to hospital and the length of stay of admitted patients. It may be associated with a decrease in formal complaints and clinical incidents, but this system places a hospital at a financial disadvantage. The system needs testing in a range of settings to establish whether this is truly externally valid.
Footnotes
Competing interests: None.