Article Text

Abstract
Antimicrobial resistance is a global problem and is being addressed through national strategies to improve diagnostics, develop new antimicrobials and promote antimicrobial stewardship. A narrative review of the literature was undertaken to ascertain the value of C reactive protein (CRP) and procalcitonin, measurements to guide antibacterial prescribing in adult patients presenting to GP practices with symptoms of respiratory tract infection (RTI). Studies that were included were randomised controlled trials, controlled before and after studies, cohort studies and economic evaluations. Many studies demonstrated that the use of CRP tests in patients presenting with RTI symptoms reduces antibiotic prescribing by 23.3% to 36.16%. Procalcitonin is not currently available as a point-of-care testing (POCT), but has shown value for patients with RTI admitted to hospital. GPs and patients report a good acceptability for a CRP POCT and economic evaluations show cost-effectiveness of CRP POCT over existing RTI management in primary care. POCTs increase diagnostic precision for GPs in the better management of patients with RTI. CRP POCT can better target antibacterial prescribing by GPs and contribute to national antimicrobial resistance strategies. Health services need to develop ways to ensure funding is transferred in order for POCT to be implemented.
- Respiratory Infection
- Bacterial Infection
- Pneumonia
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Antimicrobial resistance (AMR) is a global healthcare and economic problem, and should be a priority for all the World's governments.1 The Director General of the WHO, Margaret Chan, has stated with respect to AMR that—‘No action today means no cure tomorrow’.2 The UK Chief Medical Officer has, likewise, repeatedly emphasised the threat of AMR3 and the recently published UK Strategy for AMR has three aims: 1 improving knowledge and understanding of AMR; 2 conserving and stewarding the effectiveness of existing treatments; and3 stimulating the development of new antibiotics, diagnostics and novel therapies.4 Substantial new or redeployed funding will be needed in order to deliver this strategy, as the amount spent on research in this area is relatively small.5 The UK public has recognised the importance of AMR by voting for the challenge of the Longitude Prize 2014 to be to create “a cheap, accurate, rapid and easy-to-use point-of-care diagnostic test for bacterial infections”.6 The aim is to find the test that will have the greatest impact globally on antibiotic resistance and the prize will be open until 2019. http://www.longitudeprize.org/challenge/antibiotics.
Community prescribing of antibacterial medication varies considerably across European countries and in general practice there are individual community and country-level associations in the prescribing of antibacterials—the prevalence of resistance underscoring the need to avoid unnecessary prescription many of which are for respiratory tract infections (RTIs) in the community.7 RTIs are the most frequent infections encountered in primary care and most people presenting to a GP with an acute uncomplicated RTI still receive an antibiotic prescription, with many doctors and patients believing that this is the ‘right thing’ to do.8 This is despite the facts (1) that most RTIs are viral, (2) that there is only limited evidence to support the use of antibiotics in acute bronchitis, sore throat, sinusitis and otitis media9–12 and (3) the evidence from systematic reviews and other studies suggests little, if any, benefit is achieved from the prescription of antibiotics, except in elderly patients at high risk of pneumonia.9 ,13–15 A recent study of GP prescribing in England found that the likelihood of GPs prescribing antibiotics for coughs and colds increased by 40% between 1999 and 2011, despite Government recommendations to reduce prescribing for illnesses largely caused by viruses.16 Clarity of diagnosis was questioned in a cross-sectional study, which showed there were considerable differences in GPs’ diagnosis of pneumonia between Denmark and Spain;17 moreover, there is evidence from diagnostic studies to show the poor accuracy of clinical diagnosis of pneumonia in general practice (with radiographic proof as reference standard).18–20
So, how can the prescribing of antibiotics for RTIs in primary care be made more appropriate? How might improvements in diagnostic testing promote this?
Point-of-care tests
Potentially, primary care prescribers can use point-of-care testing (POCTs) to inform their management of disease, especially if these tests can be performed within the duration of a patient visit, with results obtained within 5 min of taking the sample. If sufficiently sensitive and specific, these tests can offer objective precision to clinical assessment of the patient's signs and symptoms.
A recent survey of Dutch GPs reported the most common point-of-care tests currently used by family physicians were: blood glucose (96%), urine leucocytes or nitrite (96%), urine pregnancy (94%), haemoglobin (58%), and CRP (48%). The most commonly desired point-of-care tests were: D-dimer (70%), troponin (65%), brain natriuretic peptide (BNP; 62%), chlamydia (60%) and International Normalised Ratio (INR; 54%). Family practitioners expected point-of-care tests to have a positive effect on patient satisfaction (93%), diagnostic certainty (89%), antibiotics use (84%) and substitution to primary care (78%). They considered the proven effect on clinical management (46%), and the tests’ reliability (35%) to be important aspects of point-of-care tests. Respondents wanted point-of-care tests to help them diagnose acute conditions, such as acute thromboembolic disorders (D-dimers), cardiac disorders (troponin, BNP) and infections (CRP, chlamydia).21
However, are there any useful POCTs to help predict RTI in general practice and to reduce unnecessary antibiotic prescribing, as advocated in the UK AMR Strategy?
Narrative review
Aim
To consider whether POCTs improve antibacterial prescribing, whether they are acceptable for patients and GPs, and their cost-effectiveness for the National Health Service (NHS).
Design and setting
Narrative review of the literature on POCT and antibacterial use in RTI in a primary care setting.
Method
A literature search was undertaken to review the literature on biomarker Point-of-Care Tests (POCT) for adults presenting to GPs with symptoms of RTI in order to:
-
Determine whether POCTs can reduce antibacterial prescribing;
-
Ascertain the safety and acceptability of POCTs for patients and GPs;
-
Determine the cost-effectiveness of POCTs in an NHS setting;
Papers reviewed were in English, and published between 1995 and 2015.
Search terms were: CRP, C-reactive protein, biomarkers, procalcitonin, infections, antibiotics, antimicrobials, primary care, point of care testing, infection respiratory tract.
Databases searched were: EMBASE, Excerpta Medica (Ovid), Journals@Ovid Full Text (Ovid), PubMed, MEDLINE (Ovid).
Highwire Press, nature.com, ScienceDirect—All Content—V.4 (Elsevier), SpringerLink, Wiley Interscience Journals, NHS Evidence, The Cochrane Collaboration.
Results
The first search yielded 1022 references. This was further refined down to 76 references by focusing on systematic reviews, clinical trials and economic analyses in human adults, and in RTIs presenting in primary care. Excluded studies included laboratory studies, studies in children, duplications and non-systematic reviews.
The pivotal studies of randomised controlled trials, cluster randomised controlled trials, economic evaluations and systematic reviews are shown in table 1.
Studies that examine antibiotic prescribing for patients presenting with symptoms of RTI to GPs who use POCT biomarkers compared with normal care
Measurement of C reactive protein (CRP) and procalcitonin biomarkers have been advocated as additional tests to assist proper clinical examination, especially (1) where there is a high degree of diagnostic uncertainty, (2) for patients who are very worried and/or demanding an antibiotic, and (3) to differentiate the seriously ill from the non-seriously ill. Procalcitonin has greater sensitivity and specificity for distinguishing bacterial and viral infection in hospital settings, and multiple analyses point to its value in guiding hospital antibiotic use for patients with pneumonia, leading to reductions in antibiotic use without harm to patients.22 ,23 However, studies show that procalcitonin does not yet add sufficient value for decision-making in primary care,24–26 whereas CRP POCT appears better in correctly predicting the absence of radiographic pneumonia.24 Moreover, procalcitonin has not yet proven to be suitable for deployment as a POCT in general practice, having a turnaround time (depending on the system) of 18–30 min; CRP POCTs, by contrast, have a turnaround of <5 min, thus giving a result within the ambit of a standard NHS GP consultation.
CRP Background
CRP is a major acute-phase plasma protein which is produced in response to infection or tissue injury. It has Ca2+-dependent binding specificity for phosphocholine (PCh), a constituent of many bacterial and fungal polysaccharides, and of most biological cell membranes. The main biological function of CRP is determined by this ability to recognise pathogens and damaged host cells, and to mediate their elimination by recruiting the complement system along with phagocytic cells. PCh, the principal CRP ligand, is widely distributed in the teichoic acids, capsular carbohydrates, and lipopolysaccharides of bacteria and other microorganisms.27 CRP was discovered and named because of its reactivity with the PCh residues of Cpolysaccharide (PnC), the teichoic acid of Streptococcus pneumoniae.28 CRP is synthesised by the liver in response to factors released by macrophages and fat cells (adipocytes). Like many acute phase proteins, CRP is normally present at trace levels in serum, but increases rapidly and dramatically in response to a variety of infectious or inflammatory stimuli.29 Its levels typically are highest in patients with a bacterial infection and are lower in those with viral infection. Rapid tests for CRP were introduced into general practice about 20 years ago and are widely used as a diagnostic in the Netherlands and Nordic countries, mostly for RTI.30
CRP evidence
A recent Cochrane review concluded that a point-of-care biomarker (eg, CRP) to guide antibiotic treatment of acute respiratory infections (ARIs) in primary care can significantly reduce antibiotic use, figure 1.31 Studies included in the final analysis included randomised and cluster randomised controlled trials in England, Wales, the Netherlands, Poland, Spain, Belgium, Denmark and Russia to demonstrate that using CRP POCT in primary care can significantly reduce the initial prescribing rate of antibiotics. Reported reductions were 36.16% (37.6% vs 58.9%) in patients presenting with acute cough/lower respiratory tract infection, LRTI (including acute bronchitis, pneumonia and infectious exacerbations of chronic obstructive pulmonary disease (COPD) or asthma),30 31.25% (33% vs 48%) in upper and lower RTI,14 24.4% (59% vs 78%) in sinusitis,32 23.3% (43.4% vs 56.6%) in LRTI or rhinosinusitis33 and 6.5% (43% vs 46%) in respiratory infections.34 In an uncontrolled observational study, Swiss GPs who used CRP as part of a clinical assessment of patients presenting with acute cough were observed to prescribe antibiotics in 22% of consultations which is considerably lower than studies from other countries.35 These studies, together with systematic reviews, offer guidance on the value of measured levels of CRP as both positive and negative prognostic indicators of whether to administer antibiotics or not.36 ,37 Interpretive and prescribing criteria, have been developed from a consensus of collaborators in two consortia: the ‘Improving Management of Patients with Acute cough by C-Reactive Protein Point of Care Testing and Communication Training (IMPAC3T) Programme’ and the Genomics to Combat Resistance against Antibiotics in Community-acquired LRTI in Europe (GRACE) consortium.14 ,38 These groups propose:
-
CRP levels <20 mg/L—Self-limiting LRTI. Withhold antibiotics
-
CRP 21–50 mg/L—Most patients have self-limiting LRTI. Assessment of signs, symptoms, risk factors and CRP is important. Withhold antibiotics in most cases.
-
CRP 51–99 mg/L—Assessment of signs, symptoms, risk factors and CRP is crucial. Withhold antibiotics in the majority of cases and consider delayed antibiotics in the minority of cases.
-
CRP >100 mg/L.—Severe infection. Prescribe antibiotics14

Forest plots for randomised and cluster randomised controlled trials from Cochrane review Biomarkers as point-of-care tests to guide prescription of antibiotics in patients with acute respiratory infections in primary care.31
Similar criteria have been proposed by other groups, including the UK National Institute for Health and Care Excellence (NICE). These are given below and compared in table 2.
Criteria for management of RTIs in general practice with CRP POCT after proper clinical examination of the patient
Both general practitioners (GPs) and patients appear to find using the test acceptable, with one Dutch study showing CRP POCT to have little effect on GP workload in 50% of practices.39 Patients were satisfied to be provided with the results of a reassuringly low CRP POCT rather than receiving an antibiotic prescription.39–41 CRP testing has a role as an adjunct in effective communication with patients; clinicians and patients all recommend seeing the CRP in conjunction with the overall assessment and caution against over reliance on CRP results in isolation of clinical assessment.42 ,43 In elderly patients with bacterial infections, CRP POCT reportedly had a sensitivity of diagnosing bacterial infection of 80.7% and a specificity of 96%, with a positive predictive value 91.9% and negative predictive value 89.8%.44
While most of these results are promising, a few studies have sounded a note of caution, particularly on the ability of CRP to distinguish between bacterial and viral infection. One Dutch study of LRTIs found that a CRP >20 mg/L (OR 2.1–4.6), along with an erythrocyte sedimentation rate >50 (OR 2.3–3.3), were independent predictors for viral or bacterial LRTI, but could not delineate between these two aetiologies.45
Is withholding antibiotics based on CRP POCT safe?
In a Russian study of patients with acute cough/LRTI (including acute bronchitis, pneumonia and infectious exacerbations of COPD or asthma), participants were randomised by GPs to normal care or to care informed by a CRP POCT. As well as a significant reduction in antibiotic prescribing, the referral rate for chest radiography was significantly lower in the intervention group (55.4%) as compared to the control group (76%; p=0.004).30 Another Dutch study showed that GPs’ use of CRP POCT significantly reduced antibiotic prescribing for LRTIs, without compromising patients’ recovery and satisfaction with care.40 This study also enhanced general consultation skills and showed that proper discussion of the test results with the patient offered an important contribution to better antibiotic stewardship.
While near patient tests can add diagnostic precision to a standard clinical examination, these are not 100% reliable.24 Any strategy reducing antibiotic use may have rare adverse consequences due to untreated infection. Use of the test is not a substitute for a proper clinical examination and ‘safety net’ advice for those not recovering as expected.
Economic evaluations of CRP POCTs
In an observational study of the presentation, management, and outcomes of patients with acute cough and LRTI in primary care settings in the Netherlands, the total mean cost per patient in the ‘usual care’ group was €35.96, with antibiotics prescribed to 68% of patients; €37.58 per patient managed by GPs using CRP POCT (antibiotic prescribing, 39%); €25.61 per patient managed by GPs trained in enhanced communication skills (antibiotic prescribing 33%); and €37.78 per inpatient managed by GPs using both interventions (antibiotic prescribing, 23%). It is less clear how such outcomes translate between national healthcare systems varying in consultation format, and in the choice and cost of the particular antibiotics prescribed.46 In a primary care study undertaken in Norway and Sweden, CRP POCT testing was associated with non-significant reductions in antibiotic prescribing (p=0.078) and increased cost (p=0.092). Despite this, CRP POCT was also associated with a cost per quality-adjusted life year (QALY) gain of £9391. At a Willingness-to-Pay threshold of £30 000 per QALY gained, there is a 70% probability of CRP POCT being cost-effective.47
Finally, in a modelling study undertaken in England, 3 models of CRP POCT use for patients presenting with RTI symptoms were subjected to Markov analysis: GP plus CRP, Practice nurse plus CRP POCT and GP plus CRP POCT and communication training. All these models were found to be more cost-effective than not using any CRP POCT.48
Limitations of study
These include, the heterogeneity of presenting conditions of patients for both upper and lower RTIs in the studies evaluated and the different healthcare systems that provide primary care services in different countries. However, these limitations are somewhat ameliorated by the designs of the studies selected—randomised controlled and cluster randomised controlled trials.
Clinical guidelines for use of CRP in RTI investigation for GPs
National Institute of Health and Care Excellence
Current draft clinical guidelines for pneumonia from the NICE propose a number of actions to help GPs to manage patients who present with symptoms of RTI.49 These include:
Consider a point-of-care C-reactive protein test for patients presenting with lower respiratory tract infection in primary care if it is not clear after clinical assessment whether antibiotics should be prescribed. Use the results of the C-reactive protein test to guide antibiotic prescribing as follows:
Do not routinely offer antibiotic therapy if the C-reactive protein concentration is less than 20 mg/L.
Consider a delayed antibiotic prescription (a prescription for use at a later date if symptoms worsen) if the C-reactive protein concentration is between 20 mg/L and 100 mg/L.
Offer antibiotic therapy if the C-reactive protein concentration is greater than 100 mg/L.
These NICE guidelines were developed following a systematic review and meta-analysis of the clinical and cost-effective published evidence from randomised controlled trials. The stratification differs from the advice of the IMPAC3T and GRACE consortia (above) only in not subdividing the patients with CRP concentrations between 20 and 100 mg/L.
Public Health England
Current guidance from Public Health England offers strategies for the management of acute upper and lower RTIs in general practice, including community-acquired pneumonia.50 This guidance is expected to be updated in line with the NICE guidance, given above, including the use of CRP as a biomarker.
European guidance
The European Respiratory Society has produced Guidelines for the management of adult lower RTI which include the recommendation:
In patients with a suspected pneumonia, a test for serum-level of C-reactive protein (CRP) can be done. A CRP level of <20 mg/L at presentation, with symptoms for >24 h, makes the presence of pneumonia highly unlikely, a level of >100 mg/L makes pneumonia likely.51
Table 2 compares the CRP-guided management of RTI based on the various slightly differing sets of guideline criteria outlined above.
Which countries use CRP POCT as a prognostic tool in general practice?
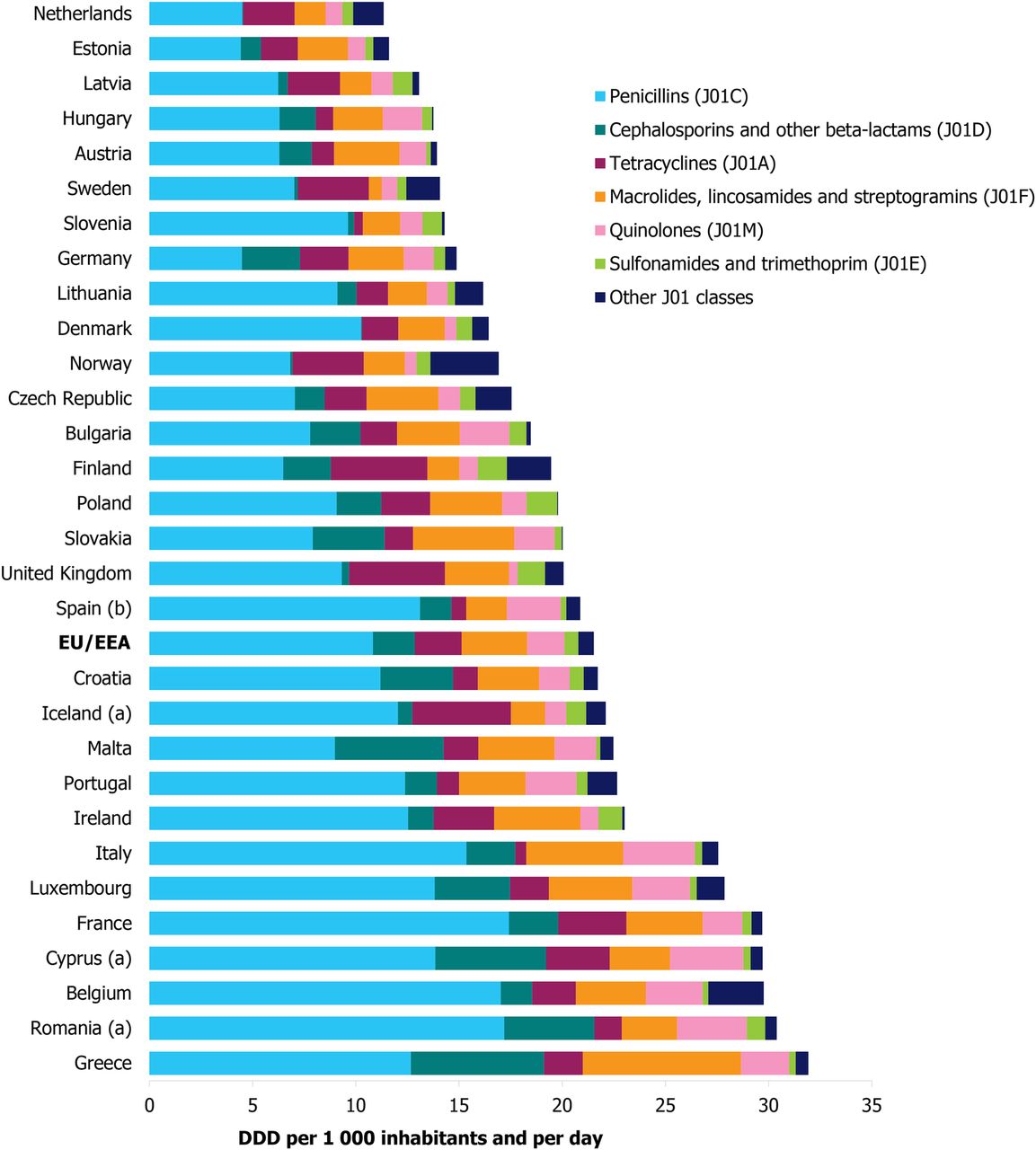
Countries that use CRP POCT widely include: Denmark, Norway, Sweden, Germany, the Netherlands, Switzerland and Finland; countries that use CRP POCT to some extent include: Estonia, Slovenia, Latvia, Czech Republic, Hungary and Austria.52 Interestingly, most of these countries have lower systemic antibacterial consumption in the community than does the UK.53 The Netherlands has particularly addressed antimicrobial stewardship in primary care, and has one of the lowest ambulatory antibiotic prescribing rates for humans in Europe53 (figure 2). Its national guidelines (NHG Guidelines)54 resemble those of GRACE and IMPACT, and the draft NICE guidance, summarised in table 2.

{kind=link}
{kind=link}
Consumption of antibacterials for systemic use (ATC group J01) at anatomical therapeutic chemical (ATC) group level 3 in the community, European Union/European Economic Area countries, 2012, expressed as defined daily dose (DDD) per 1000 inhabitants and per day. From European Centre for Disease Prevention and Control.53
Making comparisons between countries is not complete without considering how different countries pay for POCTs. In the UK, GPs would have to meet the additional costs of CRP POCT in order to encourage uptake of this technology; the alternative funding mechanisms would need to be identified, for instance, by using ‘enhanced service’ contracting arrangements.
Conclusion
There is considerable and accumulating evidence that measurements of CRP and procalcitonin are both clinically valuable and cost-effective diagnostics. Procalcitonin is not currently available as a POCT but has shown value in patients admitted to hospital with RTI. CRP POCT offers GPs a simple test that can be performed within 5 min and this helps to distinguish whether community patients with RTI need antibiotics or not. The test is acceptable to both patients and GPs, and the consequential reduction in the prescribing of antibiotics will contribute to global strategies in promoting the better stewardship of antimicrobials.
References
Footnotes
-
Contributors All authors have contributed to this paper.
-
Funding This study was supported through an educational grant from Alere International.
-
Competing interests JC chaired the Antimicrobial Stewardship Subgroup of the Department of Health Advisory Committee on Antimicrobial Resistance and Healthcare Associated Infection (travel expenses only), and has chaired, presented and received honoraria at meetings supported by Astellas, Cubist, Alere and HHI. DML is partly self-employed and consults for numerous pharmaceutical and diagnostic companies, including Achaogen, Adenium, Allecra, Astellas, AstraZeneca, Bayer, Basilea, bioMerieux, bioVersys, Cubist, Curetis, GSK, Longitude, Merck, Meiji Seika, Pfizer, Roche, Tetraphase, VenatoRx and Wockhardt; he holds grants from AstraZeneca, Basilea, Cubist, Meiji Seika, Merck and VenatoRx; has received lecture honoraria or travel reimbursement from AstraZeneca, Curetis, GSK, J&J, Leo, Meiji, Merck, Novartis, Pfizer and Tetraphase, and holds shares in Dechra, GSK, Merck and Pfizer, collectively amounting to <10% of portfolio value.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.