Article Text

Abstract
Introduction Neither the pathophysiology nor an effective treatment for heart failure with preserved ejection fraction (HFpEF) has been elucidated to date. The purpose of this ongoing study is to elucidate the pathophysiology and prognostic factors for patients with HFpEF admitted to participating institutes. We also aim to obtain insights into the development of new diagnostic and treatment methods by analysing patient background factors, clinical data and follow-up information.
Methods and analysis This study is a prospective, multicentre, observational study of patients aged ≥20 years admitted due to acute decompensated heart failure with preserved left ventricular ejection fraction (≥50%) and elevated N-terminal-pro brain natriuretic peptide (NT-proBNP) (≥400 pg/mL). The study began in June 2016, with the participation of Osaka University Hospital and 31 affiliated facilities. We will collect data on history in detail, accompanying diseases, quality of life, frailty score, medication history, and laboratory and echocardiographic data. We will follow-up each patient for 5 years, and collect outcome data on mortality, cause of death, and the number and cause of hospitalisation. The target number of registered cases is 1500 cases in 5 years.
Ethics and dissemination The protocol was approved by the Institutional Review Board (IRB) of Osaka University Hospital on 24 February 2016 (ID: 15471), and by the IRBs of the all participating facilities. The findings will be disseminated through peer-reviewed publications and conference presentations.
- heart failure
- cardiology
- cardiac epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The Prospective, Multicenter, Observational Study on the Prognosis of Heart Failure with Preserved Ejection Fraction study has very detailed clinical, echocardiographic and laboratory data at multiple time points.
A wide-range of heart failure with preserved ejection fraction patients will be enrolled and classified using detailed data.
Long-term outcome data for 5 years, and data on exercise capacity, sympathetic imaging, quality of life (QOL) score, sleeping status and mental condition will be collected.
Outcome data will be collected through the National Vital Statistics to ensure a high follow-up rate.
All of the participating hospitals are located in a single region of Japan, which may cause some bias in patient background.
Introduction
The number of heart failure cases in developed countries is rapidly increasing due to the increasing number of elderly people.1 In particular, a dramatic increase in cases of heart failure with preserved ejection fraction (HFpEF), a disease that accounts for about half of patients with congestive heart failure, is a substantial public health problem in aged societies. However, despite the many previous studies, an effective treatment for HFpEF patients backed by valid evidence has yet to emerge. β-blockers, ACE inhibitors, mineralocorticoid receptor antagonists and angiotensin receptor-neprilysin inhibitors improve the prognosis of patients with heart failure with reduced ejection fraction (HFrEF), but do not show efficacy in patients with HFpEF.2–5 The lack of an effective treatment may be largely because researchers have been unable to categorise the phenotypes of HFpEF patients due to the heterogeneity and complexity of the pathogenesis of HFpEF itself, which includes not only myocardial diastolic dysfunction but also valvular dysfunction, vascular stiffening, renal dysfunction and other comorbidities.6 To classify the heterogeneous phenotypes of HFpEF patients, detailed and comprehensive data from a large number of HFpEF patients is needed.
Several cohort studies of HFpEF patients have been reported in recent years.7–11 However, these studies have not been able to sufficiently clarify the pathogenesis of HFpEF. In addition, recent reports indicate that Japanese HFpEF patients are much older and less obese, and show a higher frequency of complication by atrial fibrillation than patients in western countries,10 11 suggesting the need for a specific database of Japanese HFpEF patients.
To overcome these issues, we designed a Prospective, Multicenter, Observational Study on the Prognosis of HFpEF (PURSUIT-HFpEF study). The PURSUIT-HFpEF study will collect detailed data from more than 1500 hospitalised HFpEF patients with 5-year prognosis data. The study will enrol a wide range of HFpEF patients with few exclusion criteria, and collect detailed data on admission, at discharge and at 1 year after discharge to enable precise understanding of ‘real world’ HFpEF patients. Our strategy is to enrol heterogeneous and wide range of HFpEF patients with broad inclusion criteria and classify them using detailed clinical data. We also aim to collect mortality and cause of death data that is as complete as possible using the National Vital Statistics, which includes reports of death among all Japanese people. This study will add important data to aid in the pathophysiological classification of HFpEF, the establishment of prognostic factors and consequences of current treatments, and lead to the development of effective treatments specific for HFpEF patients. This paper describes details of the rationale and design of the PURSUIT-HFpEF study.
Methods and analysis
Design of PURSUIT-HFpEF study
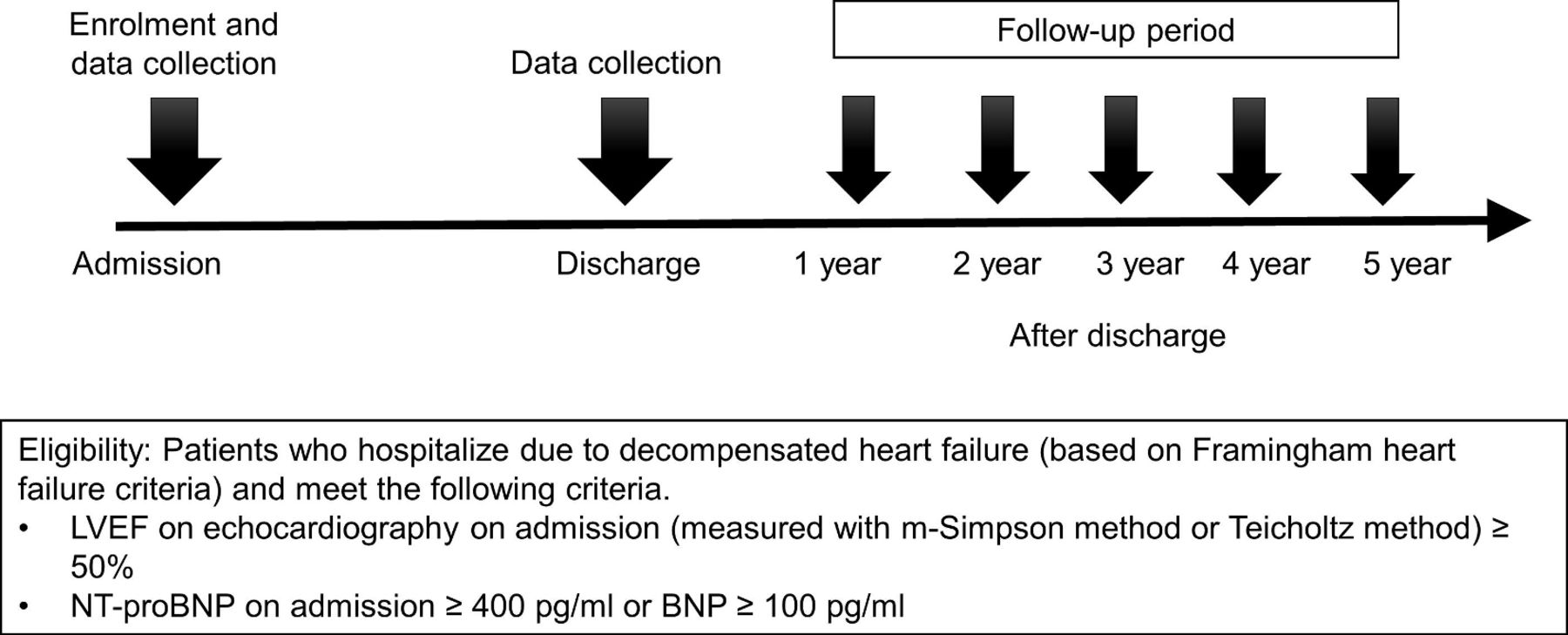
The PURSUIT-HFpEF study is being conducted under a prospective, multicentre, observational design in which 31 collaborating hospitals (1 university hospital, 30 regional core centres) in the Osaka region of Japan will collect demographic, clinical and outcome data from patients hospitalised due to congestive HFpEF (UMIN ID: UMIN000021831). The study began in June 2016. This study complies with the Declaration of Helsinki, and the study protocol was approved by the ethics committee of each participating hospital. Briefly, patients hospitalised due to the diagnosis of decompensated congestive heart failure who meet the inclusion criteria but not the exclusion criteria (box 1) will be prospectively registered and followed for 5 years (figure 1). Patients who agree to receive follow-up will provide written informed consent.
Inclusion and exclusion criteria
Patients admitted due to decompensated heart failure (based on the Framingham heart failure criteria) who meet the criteria below.
Left ventricular ejection fraction ≥50% as measured using the modified Simpson method or Teichholz method in transthoracic echocardiography (TTE) on admission.
Brain natriuretic peptide (BNP) ≥100 pg/mL or N-terminal-pro BNP ≥400 pg/mL by laboratory test on admission.
Exclusion criteria
Patients with severe aortic stenosis, aortic regurgitation, mitral stenosis or mitral regurgitation due to structural changes in valves detected using TTE on admission.
Patients aged under 20 years old.
Patients with acute coronary syndrome on admission.
Patients with poor life expectancy within 6 months due to non-cardiac diseases.
Patients who had previously undergone heart transplantation.
Patients considered ineligible for the study by the attending physician.
{kind=link}
Overview of the Prospective, Multicenter, Observational Study on the Prognosis of Heart Failure with Preserved Ejection Fraction study. BNP, brain natriuretic peptide; LVEF, left ventricular ejection fraction; NT-proBNP, N-terminal-pro BNP.
Eligibility criteria
We will enrol patients hospitalised with the diagnosis of decompensated heart failure based on the Framingham criteria and who meet the criteria of left ventricular ejection fraction (LVEF) ≥50% in transthoracic echocardiography (TTE) and brain natriuretic peptide (BNP) ≥100 pg/mL or N terminal-proBNP (NT-proBNP) ≥400 pg/mL on admission. Heart failure is defined as a clinical syndrome that results from structural or functional impairment of ventricular filling or ejection of blood.12 The Framingham criteria are widely used diagnostic criteria for congestive heart failure proposed by McKee et al.13 Major criteria include physician-assessment of neck-vein distension, rales, S3 gallop, venous pressure >16 cm of water, hepatojugular reflux and weight loss of 4.5 kg in 5 days due to diuretic therapy. Minor criteria are ankle oedema, night cough, dyspnoea on exertion, hepatomegaly, tachycardia and weight loss. ‘Definite congestive heart failure’ is defined as having at least two major criteria, or one major criteria and two minor criteria. We defined the cut-off value of LVEF for HFpEF as ≥50% according to the corresponding guideline.12 On admission, while either BNP or NT-proBNP is acceptable as an inclusion criterion, confirmation of NT-proBNP level will be mandatory in this study. Electrochemiluminescence immunoassay developed by Roche Diagnostics will be recommended for the measurement of NT-proBNP.
We will exclude patients with severe aortic stenosis, aortic regurgitation, mitral stenosis or mitral regurgitation due to structural changes in valves detected by TTE on admission. We will also exclude patients aged under 20 years, those with acute coronary syndrome on admission, life expectancy of less than 6 months due to prognosis for non-cardiac diseases, previous heart transplantation, and those judged ineligible for the study by the attending physician (box 1). We will not exclude patients with haemodialysis or bradycardia, consistent with our focus on studying real-world HFpEF patients. Regarding patients on haemodialysis, we consider that we can ensure the accuracy of HFpEF diagnosis in these patients owing to our requirement for not only BNP level but also a diagnosis of heart failure by a cardiologist. Patients with secondary cardiomyopathies such as amyloidosis or Fabry disease may also be enrolled; however, we will collect the final diagnosis of underlying cardiac disease which caused HFpEF, and this will enable the exclusion of specific cardiac conditions from the analysis if necessary.
Data collection
Research cardiologists and specialised research nurses will record patient data during hospital stays and designated visits after discharge. Data collection will be performed using an electronic data capture system integrated into the electronic medical records developed at Osaka University.14 In-hospital data will be entered into the system and transferred to the data collection centre via a secure internet connection for processing and analysis. Collaborating hospitals will be encouraged to enrol consecutive patients with heart failure with preserved ejection fraction irrespective of treatment.
Blood samples will be obtained at admission, before discharge and 1 year after discharge. Oral medications will be evaluated at admission and before discharge. The Six-Minute Walk Test will be administered before discharge.
In-hospital data will be collected on admission and at discharge. ‘On admission’ is defined as the period between admission and approximately 48 hours after admission, and ‘at discharge’ as the period between approximately 48 hours after admission and 30 days after discharge. In this study, we consider ‘at discharge’ to be a stable phase. Contrary to the timing of admission, the timing of recovery from the acute decompensated phase to the stable phase and discharge varies markedly, depending on the severity of the worsening of heart failure on admission. Some patients may recover to the stable phase very early after admission, and leave the hospital within 3 or 4 days after admission and then be followed at outpatient clinics. We will collect data ‘at discharge’ for these patients either during hospitalisation or at outpatient clinics. Accordingly, we define a broad range of times as ‘at discharge’. Investigators are required to collect as much data as possible at discharge when patients are stable.
Patient demographics
We will collect data on age, sex, height, weight, body mass index, blood pressure (systolic, diastolic), heart rate, peripheral capillary oxygen saturation (SpO2; room air), activities of daily living using the Clinical Frailty Scale,15 history of hospitalisation for heart failure, New York Heart Association class, Nohria-Stevenson class,16 clinical scenario class17 and matched Framingham criteria.13 SpO2 in room air will be measured only when patients can tolerate room air.
Data on comorbidities including atrial fibrillation, hypertension, diabetes mellitus, dyslipidaemia, smoking, alcohol consumption, hyperuricaemia, chronic obstructive pulmonary disease and chronic kidney disease, history of hospitalisation for heart failure, prior myocardial infarction, prior stroke and malignant diseases will also be collected. We will assess quality of life using the 5-Level EuroQol 5 Dimension (EQ-5D-5L),18 19 sleep quality using the Pittsburgh Sleep Quality Index (PSQI)20 21 and depression using the Self-rating Depression Scale (SDS)22 before and 1 year after discharge. EQ-5D-5L, PSQI and SDS will be performed in a self-reported manner.
Medication and therapeutics
We will collect data on the use of catecholamines, carperitides, vasodilators, antiplatelets, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, calcium channel blockers, β-blockers, α-blockers, diuretics, mineralocorticoid receptor antagonists, anticoagulants, antiarrhythmic drugs, statins, glucose-lowering drugs and uric acid-lowering drugs on admission, at discharge and 1 year after discharge. In addition, implementation of oxygen inhalation, respirator use and intubation during hospitalisation will be reported.
Laboratory data, echocardiography examination and other tests
Laboratory data will be obtained on admission, before discharge, and 1 year after discharge. Laboratory data include complete blood count and serum chemistry. Serum chemistry includes renal and liver tests, and tests for electrolytes. Transthoracic echocardiographic parameters will be obtained immediately after admission, before discharge, and 1 year after discharge. We will measure LVEF by either the Teichholz or modified Simpson method on admission, and by both at discharge and 1 year after discharge. Measuring LVEF only by Teichholz method will be allowed because of the difficulty of performing the modified Simpson method in acute settings. We will obtain data on cardiac chamber size and function, Doppler measurements and tissue Doppler measurements.
We will also collect data on standard 12-lead ECG and chest X-ray on admission, before discharge and at designated annual visits after discharge.
123I MIBG cardiac scintigraphy
Although it is well known that sympathetic nerve activity plays an important role in the pathogenesis of HFrEF, its role in HFpEF remains to be elucidated. 123I MIBG cardiac scintigraphy will be performed at discharge or soon after discharge at designated facilities. All patients will receive 111 MBq (3 mCi) of iodine-123-MIBG (Fuji Film Toyama Chemical, Tokyo, Japan) after an overnight fast and subsequently undergo planar imaging of the anterior thorax using a nuclear camera equipped with low-energy, general-purpose collimators. The scan at the early phase will be obtained at 15–20 min after injection, and that at the late phase at 3 hours after the early phase. Image processing will be performed locally at each institution. The heart-to-mediastinum ratio (HMR) on early and late images and the washout rate will be assessed using a standardised method for automatic setting of the region of interest (ROI).23 24 The software used to set the automatic ROI includes cross-calibration of HMR among hospitals to normalise differences due to variations in the types of collimator used. The algorithm is based on phantom studies conducted in all participating hospitals, and converts the HMR obtained from a low-energy type collimator to a value comparable to that obtained using a medium-energy type collimator. The washout rate will be calculated based on background correction and decay correction.
Cardiac catheterisation test
Right-sided and left-sided heart catheterisation tests will be performed at the discretion of the attending physician. Haemodynamic data on right atrial pressure, right ventricular end-diastolic pressure, main pulmonary artery pressure and coronary angiographic data will be recorded.
Follow-up schedule
Enrolled patients will be followed up at out-patient clinics at least once a year, and outcome data during the period from the previous visit will be collected. Outcome events include cardiogenic death, non-cardiogenic death and readmission due to cardiogenic or non-cardiogenic causes. The primary outcome of this study is all-cause mortality. However, since this study is explorative and observational, we will also set a primary endpoint in each analysis according to the aim of the analysis. Follow-up will be performed either by direct contact or telephone interview with patients. For patients whose survival information cannot be determined by these means, the data of National Vital Statistics of Japan will be used under the permission of the Ministry of Health, Labour and Welfare in accordance with the Statistics Act in Japan. The National Vital Statistics includes all death records in Japan reported by prefectural public health centres.
Study organisation
Osaka Cardiovascular Conference
The Osaka Cardiovascular Conference (OCVC) consists of cardiologists belonging to the Osaka University Graduate School of Medicine or one of 30 affiliated hospitals in Osaka, Japan. The OCVC was launched in 2014 to investigate clinical questions in the cardiovascular field.
The PURSUIT-HFpEF study is being conducted by the OCVC and its collaborators, which form the OCVC-Heart Failure Investigators. A total of 1500 study cases are expected to be registered in 5 years, with 300 cases registered per year. This study started enrolment in April 2016, will stop enrolment in March 2021 and will continue until March 2026 to allow the completion of follow-up for all patients.
Statistical considerations
Considering the explorative and observational nature of the current study, no formal sample size will be calculated. We will enrol all consecutive patients who fulfil the criteria among those admitted to participating facilities. We roughly surveyed the number of past patients who would have fulfilled criteria in each participating facility, and derived a number of about 300 patients per 1 year. Continuous data will be expressed as mean±SD or median with IQR for all variables collected from the entire population or specific subgroups. Categorical variables will be reported as percentages. Specific analyses including multivariable regression models will be used to explore the relationships between baseline covariates and predefined post-baseline endpoints, as appropriate. We will perform Kaplan-Meier analysis for survival analysis, and univariate and multivariate Cox regression analyses for calculation of unadjusted and adjusted HRs. In addition, details of method of analysis will be provided for each analysis. Handling of missing values will be decided based on the type and frequency of missing values. A p value <0.05 will be considered statistically significant.
Patient and public involvement
We will not involve patients or the public in the development, design, conduct or reporting of the study. The research results will be disseminated through publications or social media.
Ethics and dissemination
The study protocol has been approved by the Institutional Review Board of all participating facilities. namely Kansai Rosai Hospital Institutional Review Board, Kawachi General Hospital Ethics Committee, Osaka Rosai Hospital Ethics Committee, Higashiosaka City Medical Center Institutional Review Board, Osaka Prefectural Hospital Organization Osaka General Medical Center Institutional Review Board, Hyogo Prefectural Nishinomiya Hospital Ethics Committee, Ikeda Municipal Hospital Ethics Committee, Kawanishi City Hospital Institutional Review Board, Rinku General Medical Center Ethics Committee, Saiseikai Senri Hospital Ethics Committee, Yao Municipal Hospital Institutional Review Board, Kawasaki Hospital Ethics Committee, Minoh City Hospital Ethics Committee, National Hospital Organization Osaka National Hospital Second Institutional Review Board, Kano General Hospital Ethics Committee, Osaka International Cancer Institute Institutional Review Board, Toyonaka Municipal Hospital Ethics Committee, Kinan Hospital Ethics Committee, Japan Community Health Care Organization Osaka Hospital Ethics Committee, Kobe Ekisaikai Hospital Ethics Committee, Sakurabashi Watanabe Hospital Ethics Committee, Sumitomo Hospital Research Ethics Committee, Suita Municipal Hospital Institutional Review Board, Kinki Central Hospital Ethics Committee, Osaka Police Hospital Institutional Review Board, Japan Community Health Care Organization Hoshigaoka Medical Center Institutional Review Board, National Hospital Organization Osaka Minami Medical Center Institutional Review Board, Japan Community Health Care Organization Osaka Minato Central Hospital Ethics Committee, Amagasaki Chuo Hospital Ethics Committee, Otemae Hospital Institutional Review Board and Osaka University Hospital Clinical Research Review Committee.
We will present analysed data at domestic and international medical conferences, and will publish them as scientific papers in peer-reviewed journals.
Discussion
In this study, we will enrol a wide range of HFpEF patients diagnosed with definite heart failure using the Framingham criteria, and collect their detailed clinical data and long-term prognosis data. Our study will have distinct features compared with previous studies that will enable the conduct of in-depth analysis and elucidation of the characteristics and pathophysiology of HFpEF.
A number of previous studies have attempted to elucidate the pathophysiology of HFpEF, which is known to be very complex and heterogeneous.6 The Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF) registry is a large scale registry of 48 612 patients hospitalised for HF, including 10 072 patients with LVEF >50%, and contains comprehensive data from both admission and discharge, and outcome data at 60 and 90 days after enrolment.7 The Acute Decompensated Heart Failure National Registry (ADHERE) is the largest database, containing more than 100 000 patients with heart failure, including 26 322 patients with LVEF ≥50%. This database examines almost 80 variables and in-hospital outcomes, and therefore seems relatively less comprehensive than the former two studies.8 While OPTIMIZE-HF7 and ADHERE8 examined very large sample sizes of >10 000 patients and obtained prognosis data, data items related to clinical tests were limited, and prognosis data were limited to short-term outcomes (in-hospital or 60–90 days after discharge). Further, ADHERE had a retrospective study design. The Enhanced Feedback for Effective Cardiac Treatment study is another cohort study that enrolled HFpEF patients with LVEF ≥50% and obtained 1-year prognosis data.9 However, sample size was relatively limited (880 patients) and the study design was retrospective, as in the case with ADHERE. The Japanese CArdiac REgistry in CHF-CARDiology (JCARE-CARD) is a prospective observational study which enrolled 2675 patients hospitalised with heart failure, including 429 patients with LVEF ≥50%, and contains data from both admission and discharge, as well as outcome data at 1 year after admission.10 Recently, the Japanese Heart Failure Syndrome with Preserved Ejection Fraction (JASPER) registry reported the characteristics and 2-year prognosis of 535 patients with HFpEF, with detailed echocardiographic and laboratory data.11 JCARE-CARD and JASPER are prospective studies conducted in Japan, which have obtained long-term follow-up data. JCARE-CARD included not only HFpEF patients but also HFrEF patients, which enabled comparisons between these patients. JASPER obtained detailed clinical, echocardiographic and laboratory data, which enabled in-depth analysis of patient characteristics and pathophysiology. A possible limitation of these two studies is the sample size (JCARE-CARD: 401 cases, JASPER: 535 cases). Most recently, the ASIAN-HF group reported detailed characteristics, echocardiographic data and outcomes of an international registry of 1204 HFpEF patients from 11 Asian regions.25 The VIP-HF study is an ongoing prospective registry of 250 HFpEF patients designed to evaluate the incidence of ventricular arrhythmias in HFpEF using an implantable loop recorder (NCT01989299). This study also aims phenotyping of this disease, using comprehensive laboratory testing, echocardiography, cardiac MRI, bone scintigraphy for cardiac amyloidosis, and the Six-Minute Walk Test, and may produce very important findings, particularly regarding cardiac pathophysiologies in HFpEF. Our present PURSUIT-HFpEF study will have a relatively large sample size (target patient number >1500), and very detailed clinical, echocardiographic and laboratory data on admission, at discharge and 1 year after discharge. In addition, our study will collect long-term outcome data for 5 years, and data on exercise capacity (Six-Minute Walk Test), sympathetic imaging (123I-MIBG scintigraphy), QOL score (EQ-5D-5L), frailty (the Clinical Frailty Scale (CFS)), sleeping status (PSQI) and mental condition (SDS test). Data regarding not only cardiac conditions but also extracardiac conditions will be obtained in this study. Therefore, our study will comprise a more comprehensive database of HFpEF patients than previous studies. The broad inclusion criteria and few exclusion criteria will enable the inclusion of ‘real-world’ HFpEF patients. Detailed data items regarding both cardiac and extracardiac abnormalities will be useful to classify real-world, heterogeneous HFpEF patients. These characteristics of our study are expected to allow for a more detailed characterisation and elucidation of HFpEF.
In this study, we will sequentially collect echocardiographic and laboratory data at admission, discharge and follow-up, which may be another distinctive feature of this study. OPTIMIZE-HF obtained data both at admission and discharge, but not at follow-up, and data items on echocardiography are very limited.26 JCARE-CARD collected echocardiographic data and laboratory data only on admission.27 In JASPER, laboratory test data were obtained both at admission and discharge, but echocardiography data was obtained only once.11 Therefore, the sequential collection of both echocardiography and laboratory data in our study is unique, and will be useful for clarifying details of the time course of changes in HFpEF patients and the effects of changes in extracardiac and cardiac conditions during hospitalisation or after discharge on prognosis, which are not well known.
We will collect the outcome data through direct contact or telephone interview with patients or their family members, and also through the National Vital Statistics. Potential limitations of prospective observational studies in clinical settings are missing outcome data due to loss to follow-up, and the lack of determination of cause of death in patients who died out of hospital. Because HFpEF patients are generally elderly, loss to follow-up due to discontinuation of clinic visits is a frequent concern. The National Vital Statistics in Japan collects the data on all death records that occur in Japan. This includes the date and cause of death as diagnosed by physicians, and has been used in community-based epidemiological research.28 29 This database would clarify the survival and cause of death of patients who cannot be followed up in the past clinical studies.
There are several limitations to the design of the PURSUIT-HFpEF study. First, all of the participating hospitals are located in a single region of Japan, which may cause some bias in patient background. Second, the sample size is limited compared with previous large scale studies.8 26 Therefore, detailed classification of HFpEF patients may be limited. Third, because the treatment and care of patients will be performed at the discretion of the attending physicians, caution is needed when interpreting the analysed data. Fourth, because evaluation of imaging data (eg, echocardiography, electrocardiography, MIBG scintigraphy) and blood samples will be performed locally without validation of inter-institutional variation, we cannot exclude the potential for measurement bias among facilities or investigators. Fifth, since no structural or functional alterations on echocardiography are needed for enrolment, this may result in inclusion of patients who do not qualify or are generally not accepted as having HFpEF. In addition, patients with recovered LVEF who previously had reduced LVEF will not be excluded due to technical difficulties in this study, despite the fact that these patients have a distinct prognosis to those with HFpEF. Finally, this study will include only patients admitted due to decompensated heart failure, and not patients who have not been admitted. Therefore, it is possible that our study population is a relatively sick cohort.
In conclusion, we have begun a PURSUIT-HFpEF. This study will enrol a wide range of patients diagnosed with HFpEF and collect detailed information at multiple time points after enrolment. It is therefore expected to produce a detailed sequential database of HFpEF patients to date. Statistical analysis of the obtained data is expected to lead to elucidation of the pathophysiology of HFpEF in the ‘real world’ and the development of evidence for appropriate interventions for patients with HFpEF.
Acknowledgments
We thank Hiroyuki Kurakami and Tomomi Yamada for their statistical support, Nagisa Yoshioka, Kyoko Tatsumi, Satomi Kishimoto, Noriko Murakami and Sugako Mitsuoka for their excellent assistance with data collection. This article was supported by the Advanced Clinical Epidemiology Investigator’s Research Project in Osaka University Graduate School of Medicine.
References
Footnotes
SS and SH are joint first authors.
Collaborators The OCVC-Heart Failure Investigators. Chair: Yasushi Sakata, Department of Cardiovascular Medicine, Osaka University Graduate School of Medicine, 2-2 Yamada-oka, Suita 565-0871, Japan. Secretariats: Shungo Hikoso (Chief), Daisaku Nakatani, Hiroya Mizuno, Shinichiro Suna, Katsuki Okada, Tomoharu Dohi, Takayuki Kojima, Akihiro Sunaga, Hirota Kida, and Oeun Bolrathanak, Department of Cardiovascular Medicine, Osaka University Graduate School of Medicine, Suita, Japan. Investigators: Shunsuke Tamaki and Masatake Fukunami, Osaka General Medical Center, Osaka, Japan; Takaharu Hayashi and Yoshiharu Higuchi, Osaka Police Hospital, Osaka, Japan; Masaharu Masuda, Mitsutoshi Asai, and Toshiaki Mano, Kansai Rosai Hospital, Amagasaki, Japan; Hisakazu Fuji, Kobe Ekisaikai Hospital, Kobe, Japan; Daisaku Masuda, Yoshihiro Takeda, Yoshiyuki Nagai, and Shizuya Yamashita, Rinku General Medical Center, Izumisano, Japan; Masami Sairyo, Yusuke Nakagawa and Shuichi Nozaki, Kawanishi City Hospital, Kawanishi, Japan; Haruhiko Abe, Yasunori Ueda, and Yukihiro Koretsune, National Hospital Organization Osaka National Hospital, Osaka, Japan; Kunihiko Nagai, Ikeda Municipal Hospital, Ikeda, Japan; Masamichi Yano, Masami Nishino, and Jun Tanouchi, Osaka Rosai Hospital, Sakai, Japan; Yoh Arita and Shinji Hasegawa, Japan Community Health Care Organization Osaka Hospital, Osaka, Japan; Takamaru Ishizu, Minoru Ichikawa and Yuzuru Takano Higashiosaka City Medical Center, Higashiosaka, Japan; Eisai Rin, Kawachi General Hospital, Higashiosaka, Japan; Tetsuya Watanabe and Shiro Hoshida, Yao Municipal Hospital, Yao, Japan; Masahiro Izumi, Kinki Central Hospital, Itami, Japan; Hiroyoshi Yamamoto and Hiroyasu Kato, Japan Community Health Care Organization, Osaka Minato Central Hospital, Osaka, Japan; Kazuhiro Nakatani and Hisatoyo Hiraoka, Sumitomo Hospital, Osaka, Japan; Mayu Nishio and Keiji Hirooka, Saiseikai Senri Hospital, Suita, Japan; Takahiro Yoshimura and Yoshinori Yasuoka, National Hospital Organization Osaka Minami Medical Center, Kawachinagano, Japan; Akihiro Tani, Kano General Hospital, Osaka, Japan; Yasushi Okumoto and Hideharu Akagi, Kinan Hospital, Tanabe, Japan; Yasunaka Makino, Hyogo Prefectural Nishinomiya Hospital, Nishinomiya, Japan; Toshinari Ohnishi and Katsuomi Iwakura, Sakurabashi Watanabe Hospital, Osaka, Japan; Nagahiro Nishikawa and Yoshiyuki Kijima, Japan Community Health Care Organization, Hoshigaoka Medical Center, Hirakata, Japan; Takashi Kitao and Hideyuki Kanai, Minoh City Hospital, Minoh, Japan; Wataru Shioyama and Masashi Fujita, Osaka International Cancer Institute, Osaka, Japan; Koichiro Harada, Suita Municipal Hospital, Suita, Japan; Masahiro Kumada and Osamu Nakagawa, Toyonaka Municipal Hospital, Toyonaka, Japan; Ryo Araki and Takayuki Yamada, Otemae Hospital, Osaka, Japan; Takao Maruyama, Kawasaki Hospital, Kobe, Japan; Fusako Sera, Kei Nakamoto, Hidetaka Kioka, Tomohito Ohtani, and Shirou Manabe, Osaka University Graduate School of Medicine, Suita, Japan.
Contributors YS conceived the study. SS, SH, TY, MU, YY, AN, TD, DN and YS drafted the original protocol. AN, TT, YM contributed to developing an original data collecting system. TK, KO, DN and HI played a major role in the establishment of an outcome survey system using National Vital Statistics. SS, SH, AN, TK, HK, OB, AS, TK, TD, KO, HM, DN and YS participated in refining the protocol. All authors participated in drafting this manuscript, and have read and approved the final manuscript.
Funding This work was funded by JSPS KAKENHI Grant Number JP 17K09496 and AMED under Grant Number JP16lk1010013. This work was funded by Roche Diagnostics K.K. and Fuji Film Toyama Chemical.
Competing interests SS has received personal fees from Nihon Medi-Physics and FUJIFILM Toyama Chemical. SH has received personal fees from Daiichi Sankyo Company, Bayer, Astellas Pharma, Pfizer Pharmaceuticals and Boehringer Ingelheim Japan, and grants from Roche Diagnostics, FUJIFILM Toyama Chemical and Actelion Pharmaceuticals. AN has received personal fees from AstraZeneca and Otsuka Pharmaceutical. YM has a leadership position and stock of MKS, and has received a grant from MKS. HM has received personal fees from Daiichi Sankyo Company, Kowa Company, Bayer and Pfizer Pharmaceuticals, and a grant from Terumo. DN has received a personal fee from Daiichi Sankyo Company. YS has received personal fees from Otsuka Pharmaceutical, Ono Pharmaceutical, Daiichi Sankyo Company, Mitsubishi Tanabe Pharma Corporation and Actelion Pharmaceuticals, and grants from Roche Diagnostic, FUJIFILM Toyama Chemical, Abbott Medical Japan, Otsuka Pharmaceutical, Daiichi Sankyo Company, Mitsubishi Tanabe Pharma Corporation and Biotronik.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.