Article Text

Abstract
Objectives To identify the determinants of antenatal care (ANC) utilisation in sub-Saharan Africa.
Design Systematic review.
Data sources Databases searched were PubMed, OVID, EMBASE, CINAHL and Web of Science.
Eligibility criteria Primary studies reporting on determinants of ANC utilisation following multivariate analysis, conducted in sub-Saharan Africa and published in English language between 2008 and 2018.
Data extraction and synthesis A data extraction form was used to extract the following information: name of first author, year of publication, study location, study design, study subjects, sample size and determinants. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist for reporting a systematic review or meta-analysis protocol was used to guide the screening and eligibility of the studies. The Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies was used to assess the quality of the studies while the Andersen framework was used to report findings.
Results 74 studies that met the inclusion criteria were fully assessed. Most studies identified socioeconomic status, urban residence, older/increasing age, low parity, being educated and having an educated partner, being employed, being married and Christian religion as predictors of ANC attendance and timeliness. Awareness of danger signs, timing and adequate number of antenatal visits, exposure to mass media and good attitude towards ANC utilisation made attendance and initiation of ANC in first trimester more likely. Having an unplanned pregnancy, previous pregnancy complications, poor autonomy, lack of husband’s support, increased distance to health facility, not having health insurance and high cost of services negatively impacted the overall uptake, timing and frequency of antenatal visits.
Conclusion A variety of predisposing, enabling and need factors affect ANC utilisation in sub-Saharan Africa. Intersectoral collaboration to promote female education and empowerment, improve geographical access and strengthened implementation of ANC policies with active community participation are recommended.
- antenatal care
- prenatal care
- utilisation
- determinants
- sub-Saharan Africa
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study involved a large number of studies that covered a wide and geographically important subregion of Africa.
This study accessed several databases and used recent publications (≤10 years old).
This review provides evidence on the role of social determinants of health in antenatal care (ANC) utilisation and the importance of intersectoral collaboration in improving ANC utilisation.
This review excluded publications in French language which may limit the representativeness and generalisability of the findings to some settings.
Introduction
Globally, pregnancy and childbirth are significant events for women and their families even though they represent a period of heightened vulnerability for both women and their unborn babies.1 Every day, preventable causes related to pregnancy and childbirth lead to the deaths of over 800 women with 99% of these maternal deaths occurring in low and lower middle-income countries. Although by 2015, maternal mortality had decreased by over 40% from the 1990 levels, maternal mortality levels have continued to remain unacceptably high in sub-Saharan Africa (SSA).2 3 Inadequate access to quality antenatal care (ANC) contributes significantly to these preventable maternal deaths.4
As part of reproductive healthcare, ANC presents a unique and lifesaving opportunity for health promotion, disease prevention, early diagnosis and treatment of illnesses in pregnancy using evidence-based practices.5 To ensure optimum care, the WHO previously recommended that every pregnant woman should have a minimum of four ANC visits throughout the pregnancy with the first visit occurring in the first trimester of pregnancy.6 7 However in 2016, WHO revised its recommended minimum number of ANC visits from four to eight contacts following recent evidence that increased number of contacts between a pregnant woman and a skilled health provider reduced perinatal mortality and improved women’s experience of care. Early ANC initiation in the first trimester of pregnancy and receiving the required services is emphasised in the revised guideline.5 In spite of this, global reports in 2017 showed that only three in five women attended at least four antenatal visits. In regions with the highest rates of maternal mortality, such as SSA, only 52% of women received at least four ANC visits.8
ANC promotes the health of pregnant women and has been found to reduce the risk of adverse pregnancy outcomes, perinatal and infant mortality and morbidity.9–12 It also encourages skilled birth attendance for delivery and postnatal care as women who attend ANC are more likely to use these services than the non-attenders.13–18 Studies have used a variety of indicators to assess ANC use. This includes at least one visit, at least four visits, trimester timing of ANC visits, services received during ANC visits and care provider type visited, however the quantity of contacts remains commonly used.19 Recently, indicators to enable the progressive realisation of maternal health targets have been proposed especially for low and middle-income country contexts like countries in SSA.19 The Andersen framework is a behavioural model that describes the social, individual and health system determinants affecting access to healthcare services. Several studies have employed this model in identifying the factors affecting ANC utilisation.20–27
Various studies have assessed factors affecting ANC utilisation in SSA countries,28–35 but none has systematically summarised such studies in SSA. A review conducted over 10 years ago examined factors affecting the use of ANC in low and middle-income countries, however this review only contained seven studies from Africa and did not include recently published studies from SSA.36 The aim of this review was to systematically identify the factors associated with the utilisation of ANC in SSA.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist for reporting a systematic review or meta-analysis protocol37 was used in screening studies for eligibility (see online supplementary file 1).
Supplemental material
Search strategy
A systematic review of published quantitative literature was conducted between October 2018 and April 2019 to capture studies published in the last 10 years (2008–2018). The databases searched were PubMed, OVID, EMBASE, CINAHL and Web of Science. Other databases searched were Google Scholar and African Journal Online. The search terms used include: antenatal, prenatal, maternal health, maternal care, maternal health services, utilisation, factors, determinants, predictors, Africa. The search strategy and results are provided in online supplementary file 2.
Supplemental material
Inclusion criteria
Studies were eligible for inclusion if they were quantitative (primary or secondary data used) reporting on factors associated with ANC utilisation following multivariate analysis, conducted in SSA and published between 2008 and 2018. ANC utilisation in this review refers to attendance of at least one and at least four ANC visits and booking visit within the first trimester of pregnancy. Various study designs (longitudinal, cohort, case–control, cross-sectional and experimental) were eligible for inclusion if they assessed the predictors of ANC utilisation.
Exclusion criteria
This review excluded articles and studies published before 2008 and written in any language other than English. Studies that used measures other than the WHO recommendation for ANC were excluded. Review articles, case reports, case studies and simple descriptive studies without regression analyses were excluded. At the level of titles, titles that did not address ANC and maternal health/health services utilisation were excluded. At the abstracts stage, studies that did not report factors associated with ANC and qualitative studies were excluded. Full-text quantitative studies that did not report on the determinants of ANC utilisation after multivariable regression analysis such as studies that assessed the predictors of utilisation skilled birth attendance and postnatal care were excluded. Full-text publications that did not employ the WHO definitions for ANC and qualitative were also excluded
Data extraction
A data extraction form was developed and reviewed by all reviewers. Screening of titles and abstracts and the full texts was carried out independently by two of the review authors (INOA and ICA). Any disagreements were resolved through discussion and consensus between the two review authors or with the help of the third author (OBE). Mendeley reference manager was used to keep track of references. Data were extracted for each paper using standardised forms with the following domains: the name of first author and year of publication, study location and setting, study design, study subjects and sample size and factors/determinants. Figure 1 shows the article selection and inclusion process.
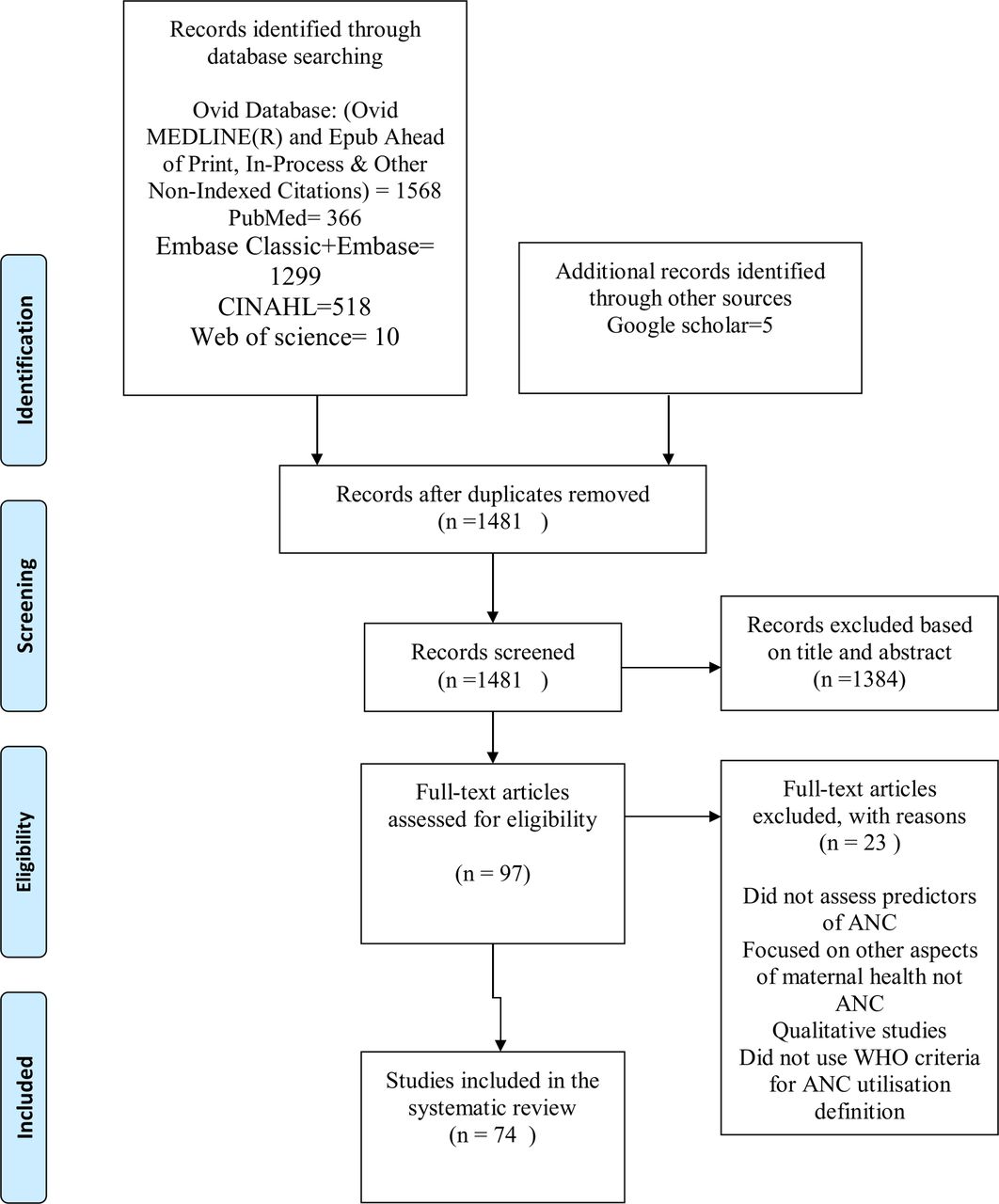
{kind=link}
Selection and inclusion process for articles included in the review. ANC, antenatal care.
Quality appraisal
Quality assessment of the studies included in this review was carried out by the main reviewer in consultation with the other authors. The Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies was used to assess the quality of the studies. This quality assessment tool has been used in other systematic reviews38 39 (see online supplementary file 3). The tool consists of 14 questions assessing different aspects of a study including but not limited to definition of objectives, study population, sampling strategy, sample size and statistical analyses. To appraise a study, each question is scored as Yes (1) or No (0), and others (CD, cannot determine; NA, not applicable and NR, not reported). All the studies included in this review were assessed for quality using the appropriate criteria based on study design. Elements of the criteria which did not apply to a particular study were marked as not applicable.
Supplemental material
All the studies fulfilled the quality criteria except for six studies9 40–44 that did not report on sample size.
Patient and public involvement
It was not appropriate or possible to involve patients or the public in this work
Results
Study selection
The search yielded 3248 studies. The initial search identified a total of 3243 articles from the main databases and five articles from Google Scholar. After removal of duplicates, 1481 articles remained. Using title and abstracts, we first screened the identified articles and excluded 1384 articles based on the agreed inclusion criteria with the other three authors. The studies were excluded because they were irrelevant to the study, conducted outside SSA and were purely descriptive. A total of 97 full-text studies were assessed for eligibility and 23 articles were further excluded after reading the full text because they did not assess predictors of ANC, did not use the WHO definitions for ANC, were focused on other aspects of maternal health not specific to ANC and were qualitative studies. The four reviewers agreed on the inclusion of 74 studies in the final review.
The 74 studies included were from 23 SSA countries. East Africa had the highest number of studies included in this review. Countries with the most studies were Ethiopia (24), Nigeria (15), Kenya (5) and Ghana (5). Most studies were cross-sectional surveys and secondary data analyses (table 1). Table 2 contains the determinants of ANC utilisation classified as overall uptake of ANC (at least one ANC visit), frequency (at least four ANC visits) and initiation of ANC in first trimester. Table 3 contains the summary of the determinants of ANC utilisation by regions in Africa. The characteristics and summary of findings of the articles included in the review are presented in online supplementary file 4 tables 1 and 2. The summary measure used by various studies was mostly the OR.
Supplemental material
Summary of articles included in the review by regions
Determinants of ANC uptake, frequency and timing
Determinants of ANC utilisation by regions in sub-Saharan Africa
The study findings were presented using the Andersen framework for the utilisation of health services.45 The Andersen framework is a health behaviour model used to assess the factors affecting health services utilisation. The model proposes three main determinants that influence the use of health services, including predisposing, enabling and need factors. These represent the preillness sociocultural characteristics, access-related factors and immediate cause/problems that generate a need for the use of health services, respectively. The predisposing factors include age, gender, marital status, family size, social status, education and race; enabling factors include family income, health insurance, distance, social relationships, service availability, and health facility characteristics (waiting time, availability of health providers) and need factors include symptoms or perceived illness. Under each main category (according to the Andersen framework), each determinant of ANC utilisation was presented with studies on its effect on overall uptake of ANC (at least one ANC visit), frequency (at least four ANC visits) and initiation of ANC in first trimester highlighted as applicable.
Predisposing factors
Maternal age
Overall uptake of ANC (at least one ANC visit)
Seven studies reported the effect of age on at least one ANC visit. Four of the studies showed that older/increasing age was a predictor of ANC utilisation.46–49 Two of the studies conducted in Ethiopia found that younger age at first pregnancy was a predictor of ANC use as women aged less than or equal to 20 years at the time of first pregnancy were nearly three times more likely to use ANC services than whose age at first pregnancy was more than 20 years.50 51 Also, in one of the studies, Nigerian women aged less than 20 years were more likely to use ANC than their older counterparts23 (table 2).
Frequency of ANC (at least four ANC visits)
Nine studies found that maternal age significantly influenced the frequency of ANC visits. Eight of the studies found that older women were more likely to have at least four ANC visits compared with their younger counterparts.30 34 43 49 52–55 One of the studies found that increasing maternal age was associated with less than four ANC visits in Ethiopia33 (table 2).
Maternal education
Overall uptake of ANC (at least one ANC visit)
In 19 studies, the relationship between maternal education and overall uptake of ANC was reported. The lack of formal education and lower educational levels were predictors of poor ANC use among women in these studies in 19 of the studies.9 25 46 47 49–51 53 58–68 However, one of the studies found that more educated women were less likely to use ANC from skilled medical providers23 (table 2).
Frequency of ANC (at least four ANC visits)
In 14 studies, maternal education was a predictor of frequency of ANC. In all the studies, the odds of attending at least four ANC visits was more in women who had higher educational levels15 24 25 27 29 30 49 53 54 64 67 69–71 (table 2).
Timing of first antenatal visit (gestational age <12 weeks)
Six studies documented the relationship between maternal education and timing of initiating ANC. Five studies found that educated women were likely to book early for ANC.24 56 57 70 72 Only one of the studies found that more educated women were less likely to use ANC from skilled medical providers23 (table 2).
Husband/partner’s education
Overall uptake of ANC (at least one ANC visit)
Only one study conducted in Ethiopia found that the higher the educational status of the husbands, the more likely the woman will attend at least one ANC visit63 (table 2).
Frequency of ANC (at least four ANC visits)
Six studies reported on the influence of husband/partner’s education on ANC use. Women whose husbands/partners had some education were more likely to access ANC services than those with less educated husbands/partners22 30 41 63 73 74 (table 2).
Maternal occupation/employment status
Overall uptake of ANC (at least one ANC visit)
Seven studies documented the impact of occupation/employment status on uptake of ANC. In six of the studies, women who were employed and those who had a working status were found to be more likely to use ANC than the unemployed/not working.47 48 62 67 75 76 Women who were farmers were more likely to use ANC in one of the studies59 (table 2).
Frequency of ANC (at least four ANC visits)
Women who were employed were more likely to use ANC up to four times compared with their unemployed counterparts in six of the studies.29 30 73 74 77 In another study, there was a higher odds of inadequacy in ANC visits among women who engaged in sales/business, agriculture, skilled manual and other jobs when compared with women who currently do not work33 (table 2).
Timing of first antenatal visit (gestational age <12 weeks)
Unemployed women were less likely to initiate ANC early in pregnancy in one study.57 In another study carried out in Ethiopia, women who were engaged in agricultural occupation were more likely to have delayed initiation of ANC.33 In Rwandan communities with higher employment rate among men, women were more likely to have received care early in the pregnancy76 (table 2).
Husband/partner’s occupation
Maternal religion
Overall uptake of ANC (at least one ANC visit)
Two studies found that Christian women were more likely to use ANC services compared with non-Christians (traditional African religion and Muslims).75 78 In another study, orthodox Christians used ANC more than the Protestants and Catholics group.48
Marital status and family type
Overall uptake of ANC (at least one ANC visit)
Three of the studies assessed the effect of marital status on using ANC once in the course of pregnancy. These studies showed that married women were more likely to use ANC than the never married/currently unmarried.79 80 One of the studies employed a composite index (adequate ANC) comprising at least one, four ANC visits, ANC by skilled professional and number of services received.79 In another of the studies, never and formerly married women were more likely to use skilled ANC attendants63 (table 2).
Parity/birth order and household size
Overall uptake of ANC (at least one ANC visit)
Five studies found that women with high parity or large household sizes were less likely to attend at least one ANC visit.46 47 49 60 61 Women whose pregnancy was for the first time were more likely to use ANC services at least once during their pregnancy.51 In one other study, mothers with high parity were more likely to use ANC than those with low parity83 (table 2).
Frequency of ANC (at least four ANC visits)
In six of the studies, women with high parity or large household sizes had significant reduction in attainment of at least four ANC contacts in the course of pregnancy15 30 40 42 70 77 (table 2).
Timing of first antenatal visit (gestational age <12 weeks)
Five studies reported that low parity/null parity was a predictor of early booking while having many children led to delayed ANC initiation.57 67 81 82 84 85 However, one of the studies showed that women who had given birth at least once were less likely to seek prenatal care in the first trimester78 (table 2).
Ethnicity
Knowledge of pregnancy/exposure to media
Overall uptake of ANC (at least one ANC visit)
In two studies, awareness of danger signs of pregnancy, timing and recommended number of ANC visits was a predictor of at least one ANC.58 83 Exposure to mass media has also increased the odds of attending at least one ANC visit48 58 75 86 (table 2).
Frequency of ANC (at least four ANC visits)
Five of the studies showed that women exposed to mass media were more likely to use ANC services and promptly compared with those who were not22 30 54 64 77 (table 2).
Timing of first antenatal visit (gestational age <12 weeks)
A study conducted in Nigeria found that women who had been exposed to three media channels (radio, television and newspaper/magazine) were more likely to initiate ANC in the first trimester compared with those who were less exposed to the media.72 Another study showed that women who lacked information on correct time of booking were more likely to book late for ANC87 (table 2).
Attitude and perception towards ANC
Overall uptake of ANC (at least one ANC visit)
Women who considered pregnancy a risky event were more likely to use ANC than those who considered it risk free46 (table 2).
Enabling factors
Household wealth/socioeconomic status
Overall uptake of ANC (at least one ANC visit)
Nine studies showed high socioeconomic level positively influenced attendance of at least one ANC visit.51 60 63 65–67 71 80 88
Frequency of ANC (at least four ANC visits)
In 14 studies, women of high socioeconomic status (SES) attended at least four ANC visits more than those in the lower socioeconomic/wealth strata15 25 27 29 30 32 41 54 64 69 77 89–91 (table 2).
Place of residence/geographical location
Overall uptake of ANC (at least one ANC visit)
Eight studies reported the role of place of residence (urban/rural) on attendance to at least one ANC clinic. In all the studies, rural dwellers were reported to be less likely to attend at least one ANC visit.15 33 35 59 64 73 90 91 Living in communities where a government health facility was situated increased the odds of attending at least one ANC visit.78 Three studies reported increased likelihood of attending at least one ANC visit based on residence in specified geographical regions/locations within the countries where the studies were conducted62 66 80 (table 2).
Frequency of ANC (at least four ANC visits)
In six of the studies, residing in the rural area made attending at least four ANC visits more likely than residing in the urban area.46 48 49 51 63 80 One study showed that women residing in communities with a government health facility providing ANC services were more likely to have four ANC visits44 (table 2).
In eight studies, residing in a particular geographic region increased the likelihood of achieving at least four ANC visits during pregnancy.22 25 27 30 44 53 54 80 This varied by the different regional and zonal categories within each country (table 2).
Timing of first antenatal visit (gestational age <12 weeks)
Rural dwellers were more likely to present late for ANC (in second and third trimesters) in four of the studies included in this review33 72 78 92 (table 2).
Distance from the health facility
Overall uptake of ANC (at least one ANC visit)
In three studies, increased distance to ANC services negatively impacted the uptake of at least one ANC visit.46 61 68 In one study, Kenyan women who lived close to the dispensary were more likely to have at least one ANC visit, however among those women with at least one visit, the number of ANC visits increased as the distance from the dispensary increased.9 Another study also found that for each 10 km increase in distance from a health facility, the odds of a woman receiving different ANC services decreased by a quarter.93 In one of the studies, having a Women’ Health Development Team within a 2 km radius from the nearest health facility increased the likelihood of at least one skilled ANC utilisation.86 Access to health services was associated with attending at least one ANC visit in another study48 (table 2).
Health insurance/user-fee exemption
Overall uptake of ANC (at least one ANC visit)
One of the studies found that women who were insured were more likely to attend at least one ANC visit.94 In another study, the proportion of women who made at least one ANC visit during pregnancy increased significantly following user-fee exemption95 (table 2).
Involvement in decision-making/autonomy
Frequency of ANC (at least four ANC visits)
Women who made decisions jointly with their husbands or partners were significantly more likely to have four or more antenatal visits compared with women whose husbands or partners made decisions alone.29 30 87 Another study conducted in Eritrea and Ethiopia showed that women who were involved in major household decisions such as large purchases were more likely to use ANC at least four times73 (table 2).
Husband/partner’s approval and support, social support
Overall uptake of ANC (at least one ANC visit)
Women whose husbands have positive attitude towards ANC were more likely to use ANC than women whose husbands had negative attitude towards ANC.46
Women who had their husband/partner’s approval/permission to attend ANC were more likely to use ANC services compared with those without support from their husbands50 58 97 (table 2).
Frequency of ANC (at least four ANC visits)
Women who did not experience physical intimate partner violence during the year preceding survey were more likely to have four ANC visits.44 In another study, women who had the father of their child present in their lives were more likely to use ANC services.98 Women who lacked social support were more likely to underuse ANC services compared with those with social support52 (table 2).
Quality/content of ANC services
Overall uptake of ANC (at least one ANC visit)
In one of the studies, women who received advice on ANC from health workers were more likely to attend ANC at least once in pregnancy97 (table 2).
Frequency of ANC (at least four ANC visits)
High cost of services was associated with decreased ANC use.53 In one of the studies, having an ANC at a private hospital was a predictor of delayed initiation of ANC, but in another, it increased the likelihood of receiving adequate ANC compared with those clients using public health facilities.24 81 The level of antenatal service provision (measured as the availability of key functions, screening tests, skilled health workers and opening times) affected the quality of ANC received. Using ANC at facilities that provide a wide range of ANC services was associated with an increase in the odds of receiving the complete ANC services given in the clinic and attending ANC.93 Visits by health extension workers during pregnancy increased ANC attendance in one of the studies99 (table 2).
Need factors
Pregnancy wantedness and planning
Overall uptake of ANC (at least one ANC visit)
Nine studies found that women with planned pregnancies were more likely to attend at least one ANC than those with unplanned pregnancies46 47 50 55 58 71 83 85 100 (table 2).
Frequency of ANC (at least four ANC visits)
Attending at least four ANC visits was positively influenced by pregnancy planning and wantedness as seen in two studies.41 55 Conversely, in six studies, women with mistimed or unwanted/unplanned pregnancies were unlikely to attend at least four ANC visits13 53 78 81 98 100 (table 2).
Previous/current health and pregnancy experiences
Overall uptake of ANC (at least one ANC visit)
Pregnancy complications, illnesses and stillbirths in previous pregnancies were found to reduce the odds of attending at least one ANC visit in two studies50 55 (table 2).
Frequency of ANC (at least four ANC visits)
Women whose pregnancy was confirmed by missed period rather than urine test were more likely to delay booking ANC visit.87 Women who attended ANC in the first trimester were more likely to attend up to four ANC visits89 (table 2).
Timing of first antenatal visit (gestational age <12 weeks)
Women who had negative experiences in previous pregnancies were less likely to attend the booking ANC visit in first trimester.84 Women who had an early initiation of ANC in a previous pregnancy were more likely to book early for ANC in the subsequent pregnancy56 (table 2).
Discussion
This study reviewed the predictors of ANC utilisation in SSA. Although the studies included in this review used different study designs, most were cross-sectional studies and secondary data analyses of national surveys. The determinants of ANC utilisation identified in this review include predisposing factors (such as age, education, religion, husband/partner’s education, maternal occupation/employment status, husband/partner’s occupation, parity), enabling factors (such as income status, place of residence, distance from the health facility, health insurance, involvement in decision-making, quality/content of ANC services) and need factors (wantedness of pregnancy, previous pregnancy experiences).
In this review, higher educational attainment for women and their husband/partner was a predisposing factor that increased overall attendance, frequency and timeliness of ANC visits in majority of the studies. These studies found that being educated increases the odds of the number and timeliness of ANC visits. This could be explained as educated women tend to be more financially independent, employed and better informed on the importance of ANC to the mother and baby.101 Similarly, studies have found that educated women and those with educated partners were more likely to use antenatal services and also initiate this within the first trimester of pregnancy.36 102 103 Poor educational status has been identified as a major cause of heath inequality in ANC coverage.104 This finding highlights the need to collaborate with the educational sector to promote both female and male school enrolment and completion.
Studies in this review showed that women with a working status (employed) were found to be more likely to attend at least one and at least four ANC visits than the unemployed/not working. Being employed also increased the odds of early initiation of ANC. Employment status is closely related to income and educational status as educated women tend to be employed and consequently earn income. Beyond being a source of funds for sponsoring ANC use, employment can also increase women’s exposure and access to information on ANC, thus further promoting utilisation. Women empowerment programmes and provision of employment opportunities sensitive to maternal health considerations should be encouraged in order to promote uptake of ANC services.105
As a predisposing factor, the role of high parity in reducing the odds of ANC attendance and initiation could have been because women who have had previous pregnancies may consider themselves ‘experienced’ and used to the routine care offered during ANC and so delay ANC initiation and number of ANC contacts made.106 Timely initiation of the first ANC visit provides a critical opportunity for health promotion, disease prevention and curative care for women and their unborn children. More efforts are needed to optimise the uptake of first ANC visit in the first trimester of pregnancy.107 Also, decreased use of ANC among high-parity women could be due to the less time available for ANC attendance due to the care of children, inadequate resources in the family and negative experiences with ANC from previous pregnancies.36
Among the predisposing factors, increasing/older maternal age increased attendance to at least one and four ANC visits in most of the studies that assessed its relationship with ANC utilisation. A few studies however found that younger women attended ANC clinics more than older ones. Also, younger women were more likely to attend the first ANC visit in the first trimester of pregnancy. The higher odds of early trimester booking visits in these studies may have been due to the relative childbearing inexperience (low parity) as they may be newly weds or adolescents and therefore be more likely to seek out ANC earlier than their older counterparts due to ignorance/limited knowledge of pregnancy. Confounding effect of by parity on age may also have affected the relationship between age and ANC use as low parity was associated with early ANC booking and increased number of ANC contacts in the studies reviewed.15 30 40 42 47 49 60 61 70 73 77 Younger women have been found to initiate ANC early in a similar review.108 109 In contrast, age was not significantly associated with the utilisation of ANC in a review of factors affecting ANC in Ethiopia.103
Most of the studies showed that being married conferred a protective effect on ANC utilisation as a predisposing factor. Married women were more likely to attend ANC and less likely to delay initiation of ANC visits when compared with their unmarried counterparts. This could be due to the psychosocial and financial support received from their husbands, planning/desirability of their pregnancy and the societal acceptability and support of their pregnant state when compared with their unmarried counterparts.106 Some studies included in this review showed that women who enjoyed support from their husbands and other social support were more likely to use ANC. This suggests and reinforces the importance of including married men in programmes that are designed to improve ANC uptake as male involvement has been proven beneficial to maternal health.110 However, one of the studies in this review found higher odds of using skilled ANC attendants among currently unmarried women.63 One possible explanation for this is that unmarried women are sole decision makers, making them empowered to seek and use ANC.
Our findings suggest that SES was one of the enabling factors reported to influence ANC utilisation across many studies as high SES increased the uptake of at least one and at least four ANC visits and the early initiation of ANC. Poverty is a known deterrent to healthcare utilisation in SSA and women of low-wealth status may be unable to afford the medical and non-medical costs associated with using ANC.111 112 Thus, because of lack of financial access, such women may not attend ANC at all, limit the number of ANC visits or even initiate ANC late in pregnancy. The effect of SES on ANC use has been documented in other studies.36 113–115 Although free/subsidised maternal health services are offered in some African countries, women still pay out of pocket for some direct medical costs such as laboratory investigation and non-medical costs for transport. These costs pose financial barriers to using ANC services by pregnant women.116 117 Further reflecting the role of the woman’s ability to fund ANC on utilisation, early initiation and attending ANC for at least four times were reduced in women who did not have health insurance. Women have peculiar maternal-related health needs (such as pregnancy and childbirth), thus making them use health services such as ANC, however they are oftentimes less willing and able to pay for insurance compared with men because of their low-income status and financial dependence.118 119 Consequently, ANC and other maternal health services should be provided free (under mandatory social health insurance) or at subsidised rates with exemptions in order to improve the utilisation of these services and in turn reduce maternal morbidity and mortality. This review did not identify cultural/local beliefs as a determinant of ANC utilisation in contrast with findings from a similar review conducted in low and middle-income countries where women were declined from using ANC services due to fear of witchcraft attacks following blood sample collection for laboratory investigation.36 It is possible that women are getting more enlightened and as such not holding on to such beliefs.
As part of the enabling factors, rural residence negatively impacted on attendance and timing of the first ANC visit. The interplay between the peculiar characteristics of rural areas such as sparse distribution of health services and development, poor educational and employment status of residents and poor access to mass media could explain this. Similar findings on the effect of rural residence on ANC use have been documented in other studies.36 103 108 To improve ANC utilisation in rural areas, community-wide sensitisation on ANC, provision of basic amenities and redistribution of health services are recommended. Likewise, long travel distance between a woman’s place of residence and the health facility providing ANC services was associated with a lower odds of ANC utilisation. Walking or travelling long distances could be difficult for pregnant women in addition to travel-related costs and these may discourage them from using ANC services. This negative effect of long distance on the utilisation of ANC and the continuum of maternal healthcare services has been documented in other studies.120
Involvement in decision-making on major household decisions and ANC was one of the enabling factors that exerted a positive effect on attaining adequate and timely ANC visits. Many patriarchal communities exist in SSA in which women lack autonomy and cannot decide to seek ANC without approval from their husbands largely because of financial dependence and cultural norms.121 Autonomy and involvement of women in decision-making have been found to increase the utilisation of maternal health services.103 109 122
The findings from this review suggest as part of the need factors, women whose pregnancies were planned and desired were significantly more likely to use ANC services at least once and at least four times compared with those with unplanned/undesired pregnancies. This agrees with findings from other studies.36 103 In order to encourage ANC use, more needs to be done to increase uptake of family planning by securing only desired pregnancies.
Strengths and limitations
This study involved a large number of studies that covered a wide and geographically important subregion of Africa. The review accessed several databases and used recent publications (≤10 years old). It provides evidence on the variety of determinants across different sectors affecting ANC utilisation and the importance of intersectoral collaboration in improving ANC utilisation.
The contextual differences in study settings and outcome measures used could affect the interpretation and meaning of the results. However, some determinants showed similarities and differences within and between countries. This review excluded publications in French language and this may limit the representativeness and generalisability of the findings to some settings.
Conclusion
Based on this review, a variety of factors affect ANC utilisation in SSA. These factors include the predisposing, enabling and need factors with the poor, uneducated, unmarried, uninsured, rural dwellers, multiparous, poorly knowledgeable, those living far from health facilities and unsupported by their husbands/partners less likely to use ANC services. These factors also demonstrate the importance of multistakeholder intersectoral collaboration in mitigating poor ANC utilisation in SSA. Thus, ministries of labour/employment, education, rural development, women affairs, finance, community and religious leaders need to collaborate with the ministry of health to achieve universal ANC coverage. Examples would include health-in-all policies, joint stakeholder policy, planning and implementation review meetings, capacity development for policymakers on intersectoral cohabitation secondments and having desk officers represent related ministries (sectors above) in the ministry of health. An example of the implementation will be the educational sector encouraging enrolment in schools while the health sector participates in curriculum development to include basic information on care in pregnancy (ANC inclusive). The ministries of works, labour and employment can lay their part by road construction to improve access to health facilities especially in rural underdeveloped areas, subsidised transport for pregnant women, provision of regular electricity to enable access to electronic media and provision of job and empowerment opportunities for women. The finance ministry can partner to provide loans, grants, conditional cash transfers and other forms of financial empowerment to women. Strengthened implementation of ANC policies with active community participation is also recommended.
Acknowledgments
We acknowledge the Alliance for Health Policy and Health Systems (WHO) for providing mentorship support and funding the publication of this article under the publication mentorship programme for women in Health Policy and Health Systems (HPSR). We are grateful to John Ataguba for providing mentorship to this work. We also acknowledge the technical assistance received from the African Institute for Health Policy and Health Systems, Ebonyi State University, Abakaliki.
References
Footnotes
Contributors INO: study of conceptualisation and design, data extraction, analysis and interpretation of results, manuscript drafting and approval of the final manuscript for publication. ICA, OBE: study design, data extraction, manuscript drafting and approval of the final manuscript for publication. CJU: study design, analysis and interpretation of results, manuscript drafting and approval of the final manuscript for publication.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.