Article Text

Abstract
Introduction Disruption of care during transition from child and adolescent mental health services (CAMHS) to adult mental health services may adversely affect the health and well-being of service users. The MILESTONE (Managing the Link and Strengthening Transition from Child to Adult Mental Healthcare) study evaluates the longitudinal course and outcomes of adolescents approaching the transition boundary (TB) of their CAMHS and determines the effectiveness of the model of managed transition in improving outcomes, compared with usual care.
Methods and analysis This is a cohort study with a nested cluster randomised controlled trial. Recruited CAMHS have been randomised to provide either (1) managed transition using the Transition Readiness and Appropriateness Measure score summary as a decision aid, or (2) usual care for young people reaching the TB. Participants are young people within 1 year of reaching the TB of their CAMHS in eight European countries; one parent/carer and a CAMHS clinician for each recruited young person; and adult mental health clinician or other community-based care provider, if young person transitions. The primary outcome is Health of the Nation Outcome Scale for Children and Adolescents (HoNOSCA) measuring health and social functioning at 15 months postintervention. The secondary outcomes include mental health, quality of life, transition experience and healthcare usage assessed at 9, 15 and 24 months postintervention. With a mean cluster size of 21, a total of 840 participants randomised in a 1:2 intervention to control are required, providing 89% power to detect a difference in HoNOSCA score of 0.30 SD. The addition of 210 recruits for the cohort study ensures sufficient power for studying predictors, resulting in 1050 participants and an approximate 1:3 randomisation.
Ethics and dissemination The study protocol was approved by the UK National Research Ethics Service (15/WM/0052) and equivalent ethics boards in participating countries. Results will be reported at conferences, in peer-reviewed publications and to all relevant stakeholder groups.
Trial registration number ISRCTN83240263; NCT03013595 (pre-results).
- mental health
- child and adolescent mental health services
- transition
- health services research
- cluster randomised controlled trial
- longitudinal cohort study
- youth mental health
- Europe
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- mental health
- child and adolescent mental health services
- transition
- health services research
- cluster randomised controlled trial
- longitudinal cohort study
- youth mental health
- Europe
Strengths and limitations of this study
This is the first ever methodologically robust trial to test whether a decision support and assessment tool can improve the mental health and social outcomes and functioning of transition-age young people receiving care at child and adolescent mental health services.
A large, prospectively identified and robustly evaluated cohort of young people across several European countries with diverse healthcare systems is taking part in the study.
The cost-effectiveness of the intervention and research-related changes in health systems in terms of both expenditure and related health outcomes will be evaluated.
There is a strong patient and public involvement at all stages of the study.
Due to the nature of the intervention, it is not possible for clinicians or assessors to be blind to the allocation of clusters or of the service users within these clusters.
Introduction
The MILESTONE (Managing the Link and Strengthening Transition from Child to Adult Mental Healthcare) study focuses on the period when young people attending child and adolescent mental health services (CAMHS) need to move on, or ‘transition’ to, an adult mental health service (AMHS), if they still require ongoing care.
Adolescence is a high-risk period for psychological morbidity, and young adulthood is the period during which most of the serious mental disorders that disable or cause death in adult life have their onset.1–4 The National Comorbidity Survey Replication in the USA found that 75% of people with a mental disorder have an age of onset younger than 24 years, and 50% have an onset before 16.5 However, only a small proportion of young people with mental health problems approaching adulthood, less than one in six, access services or receive appropriate care.6
There is international concern about young people who get ‘lost’ during their move from CAMHS to AMHS,7–15 and transition-related discontinuity of care is a major socioeconomic and societal challenge. In the UK, almost half of the service users reaching the transition boundary of their CAMHS do not go on to receive adult care.7 16 The Transition from CAMHS to Adult Mental Health Services (TRACK) study found that less than 5% of patients undergoing CAMHS to AMHS transition experience continuity of care.17 There is also a concern that despite recognition of ongoing mental health need, few young people are referred, with fewer than one-third in one study.18 Continuity of care is hampered by a multitude of reasons, including differences between adult and child models of care; differing referral criteria; lack of a planned, purposeful and needs-based assessment of those who reach the boundary; communication and information transfer problems between services caused partly by different beliefs, attitudes, mutual misperceptions and lack of understanding of different service structures; lack of shared protocols/manuals for transition; lack of shared client planning between child and adult systems; young people’s level of maturity and understanding; and adolescent and/or family resistance to transition.19–21 Furthermore, transition may differ widely across different regions and countries due to lack of or different procedures.
Problems at the CAMHS–AMHS interface are accentuated by the fact that young people are simultaneously negotiating developmental and situational transitions, such as changes in housing and relationships and moving on to adult roles.8 17 A lack of information about possible options, planning that takes too long and where no one professional takes charge to ensure decisions are acted on, compound the problem.22 Those who slip through the care net are likely to present to adult services at a subsequent time, with more severe and enduring mental health problems.23–25 Disruption of care during transition adversely affects the health, well-being and potential of this vulnerable group,26–31 and negative transition experiences adversely impact the young person’s future engagement with mental health services.32
Intervening at the level of transition represents one of the most important ways we can facilitate recovery and mental health promotion and mental illness prevention in adulthood. Ensuring sustained treatment through the transitional period is very likely to be cost-effective, since the presence of mental illness during childhood leads to 10 times higher costs during adulthood.33–35 However, there is currently no evidence for any effective model of appropriate transitional mental healthcare or any interventions to reduce these individual and societal costs.36
Transitional care
Ideally, transition to adult mental health services (AMHS) should be a planned, orderly, purposeful and patient-centred process that ensures continuity of care, optimises health, minimises adverse events and ensures that the young person attains his/her maximum potential.37–41 Good transitional care starts with preparing a service user to leave the child-centred healthcare setting and ends when that person is received in, and properly engaged with, the adult provider or an appropriate alternative, or is discharged from care in a planned and managed fashion.42 43
European research on transition from CAMHS to AMHS is sparse, with little information available on the quality of transition and transition experiences in different European Union (EU) countries in relation to long-term mental health outcomes. The organisation of CAMHS in the member states varies, including the age at which young people are transitioned to adult services, size and complexity, sources of funding, and service provision and care. There is some evidence though that transition is a problem across all EU states.44–46
Barriers to good transition have been mapped,16 17 but the evidence of interventions for improving transitional care is scant. A recent systematic review of CAMHS to AMHS transition identified only three initiatives, all in the USA,20 including a case management model, a transition support model and an outpatient transition programme. Although all three programmes showed improved clinical and social outcomes for those with facilitated transition, none of these was a randomised trial and each model was deeply rooted within its own particular and specific healthcare context. There is no consensus as to who can be discharged on reaching the CAMHS transitional boundary, who should receive transitional care and how this care should be delivered. Furthermore, it is not clear what outcomes should be measured to assess clinical and cost-effectiveness of the model, what the outcomes of those who fall through the care gap are, and what the individual, organisational and societal costs of poor, inadequate or inappropriate transition are. A recent National Institute for Health and Care Excellence (NICE) review on transition from child to adult care across all specialties found that there was no robust evidence on models of transitional care.36
In the absence of a planned, purposeful and needs-based assessment of those who reach the boundary, clinical judgement on transition can be influenced by misperceptions of other services, time and resource constraints, poor communication between CAMHS and AMHS, and poor adherence to existing policies.19 Research has confirmed several information-gathering biases in unstructured clinical judgements, such as diagnostic biases, confirmation biases, ignoring conflicting information, and assumptions based on patient and service background.47 A recent study found that feeding back structured assessment results to clinicians led to improved clinical decision making.47
Ideally all young people who reach a transition boundary would be assessed in a structured and standardised way to determine ongoing need for care. Those who need such care would make a transition to adult services in a planned and managed manner ensuring continuity of care across all domains. Those without ongoing need would be appropriately discharged. Despite the intuitive simplicity and clinical importance of such a structured decision process, a transition model incorporating this approach with regard to mentally ill patients has not been evaluated or reported in research or health practice literature, although its need has been articulated.11 14
The MILESTONE project
The 5-year MILESTONE project (February 2014–January 2019) aims to improve the understanding of, and strengthen, CAMHS–AMHS transitional care across different healthcare systems in the EU. In a series of work packages, it will (1) map current services and transitional policies across the EU; (2) develop and validate transition-specific outcome measures; (3) conduct a longitudinal cohort study of transition processes and outcomes across eight EU countries; (4) develop and test, in a cluster randomised trial, the clinical and cost-effectiveness of an innovative transitional care model; (5) create clinical, organisational, policy and ethics guidelines for improving care and outcomes for transition age youth; and (6) develop and implement training packages for clinicians across the EU. This paper presents the protocol (V.2.2) for the work packages dealing with the longitudinal cohort study, the cluster randomised controlled trial (cRCT) and the economic evaluation of the trial, which combined constitutes the MILESTONE study.
MILESTONE model of managed transition
The model of transitional care we have developed consists of an evidence-based decision-making process and managed transition, incorporating key principles of continuity of care: adequate information transfer, appropriate joint working, therapeutic and relational continuity, and engagement with adult services.48 49 The model of managed transition can be seen as one of the cornerstones of a planned and purposeful transition process and can lead to more effective joint working between services. It addresses the need to involve young people and parent/carers in the planning process, tailor transition support to individual needs, identify barriers to smooth transition and act on these, plan transition in a timely fashion, produce a succinct medical summary of the service user, and improve information transfer and communication with adult providers.36 The model includes the following:
The establishment and/or confirmation of shared understanding of criteria for good-quality transitional care at the CAMHS–AMHS interface, and managed ending of care, taking into account clinicians’ prior knowledge of good-quality transition.
Systematic identification of all young people under CAMHS care who reach the transition boundary for their service.
Structured and standardised assessment of their mental health and social care needs using a bespoke Transition Readiness and Appropriateness Measure (TRAM), completed by the young person, their parent/carer if available and CAMHS clinician prior to, ideally 6 months before, the transition boundary.
Feedback of TRAM results from all parties in a short, clearly presented report to relevant clinicians in CAMHS, allowing clinicians to identify areas in which attention should be focused to ease a young person’s path to transition.
Using the findings from the TRAM report to focus communication with service users and carers on issues surrounding end of care at CAMHS and potential transition to AMHS or other community-based service.
Incorporation of critical information by clinician to young person’s care or transition plan, and designing goals for critical items that are achievable.
Sending the TRAM findings, along with a referral letter, to the new adult service, if a referral to AMHS is made.
Structured and regular follow-up of all young people using the Transition Related Outcome Measure (TROM) to assess whether those who needed care were appropriately engaged with adult services and those who had been discharged or referred to other services had no unmet needs following cessation of care.
TRAM and TROM
The TRAM, a decision support and assessment tool, uses the HealthTrackerTM platform. The measure, together with the linked findings report, have been designed to help the clinician identify (1) high-risk, high-need cases for whom transition to AMHS is advisable and appropriate, (2) those who can be appropriately discharged in a planned manner from CAMHS to a general practitioner (GP), or (3) transitioned to another community-based service (such as social services, voluntary sector or other non-statutory agencies). Obviously, the clinicians will need to take their local service provision into account when making the decisions. The TROM provides information on outcomes post-transition, and on the transition process and experience.
The TRAM and TROM were developed using existing literature, expert input and focus groups on developing and validating Patient Reported Outcome Measures50 51; MILESTONE’s group of young advisors also reviewed the scales and helped identify areas of duplication or unclear terms. The scales have been translated into Croatian, Dutch, Flemish, French, German and Italian languages, and provide a summary of all factors necessary to consider (including symptoms, functioning, risk and need for care) when making a transition decision and when assessing the outcomes of a transition. There are versions for young people pre- or post-transition, parents/carers and clinicians at CAMHS and AMHS, which can be completed online, via the HealthTrackerTM platform (https://www.healthtracker.co.uk), a web-based portal allowing measures to be completed remotely that has been used in other EU’s Seventh Framework Programme for Research and Technological Development (FP7)projects.52
The TRAM and TROM contain 20 questions common to both scales for all participants; eight additional questions are relevant only to the clinician and nine only to the young person and parent/carer versions. All participant versions of TRAM contain 15 additional questions that are not in TROM, yet to allow comparison of results over time, most of the domains present in TRAM are also present in TROM, with versions for AMHS and CAMHS clinicians and different follow-up time points (available from the corresponding author upon request).
The construct validity, content validity, inter-rater validity, test–retest validity and sensitivity to change of TRAM and TROM were assessed in a substudy between June 2015 and April 2016.
The ‘TRAM score summary report’ presents the scores from the young person, parent/carer and clinician for each item, with graphs visualising differences or similarities in scoring. The report contains items that are relevant to the clinician’s transition decision (symptoms, risk factors and disruption experienced by the young person) and those that can facilitate a smooth transition. It displays all information in a user-friendly, relevant and accessible format, helping identify young people requiring further care and allowing key facts to be easily transferred to care plans and referrals. It should complement a much more comprehensive evaluation, with the ultimate decision about transition being the outcome of a process involving key stakeholders.
The TRAM will be optimised on the HealthTrackerTM platform based on decision-making algorithms derived from the study. If appropriately funded, this will be made available to serve as the platform for optimisation of transitions to adult mental health in the EU.
Aims and objectives
The overall aim of the nested cRCT is to determine the effectiveness and cost-effectiveness of the model of managed transition in improving the health and social outcomes of young people, and their transition to adult roles, as compared with treatment as usual, in eight participating EU countries. The specific objectives are the following:
To test the hypothesis that the implementation of the model of managed transition in CAMHS at the transition boundary improves the mental health and social outcomes of young people and their transition to adult roles when they move on from CAMHS, as compared with usual care.
To conduct an economic evaluation of the model of managed transition compared with usual care.
To explore the views and experiences of health professionals and young people concerning the intervention.
The prospective cohort study will delineate the transition journey of a large number of young people across eight EU countries. The aims are the following:
To evaluate the mental health, quality of life and functioning of young people who attend CAMHS and reach the CAMHS/AMHS transition boundary;
To evaluate the longitudinal course of mental health, social and adult functioning outcomes of young people who reach the CAMHS/AMHS transition boundary and transition into young adulthood;
To compare the outcomes in those young people who transition with those who do not transition to AMHS (ie, remain in CAMHS, are discharged or referred to other care).
Methods and analysis
Study design and management
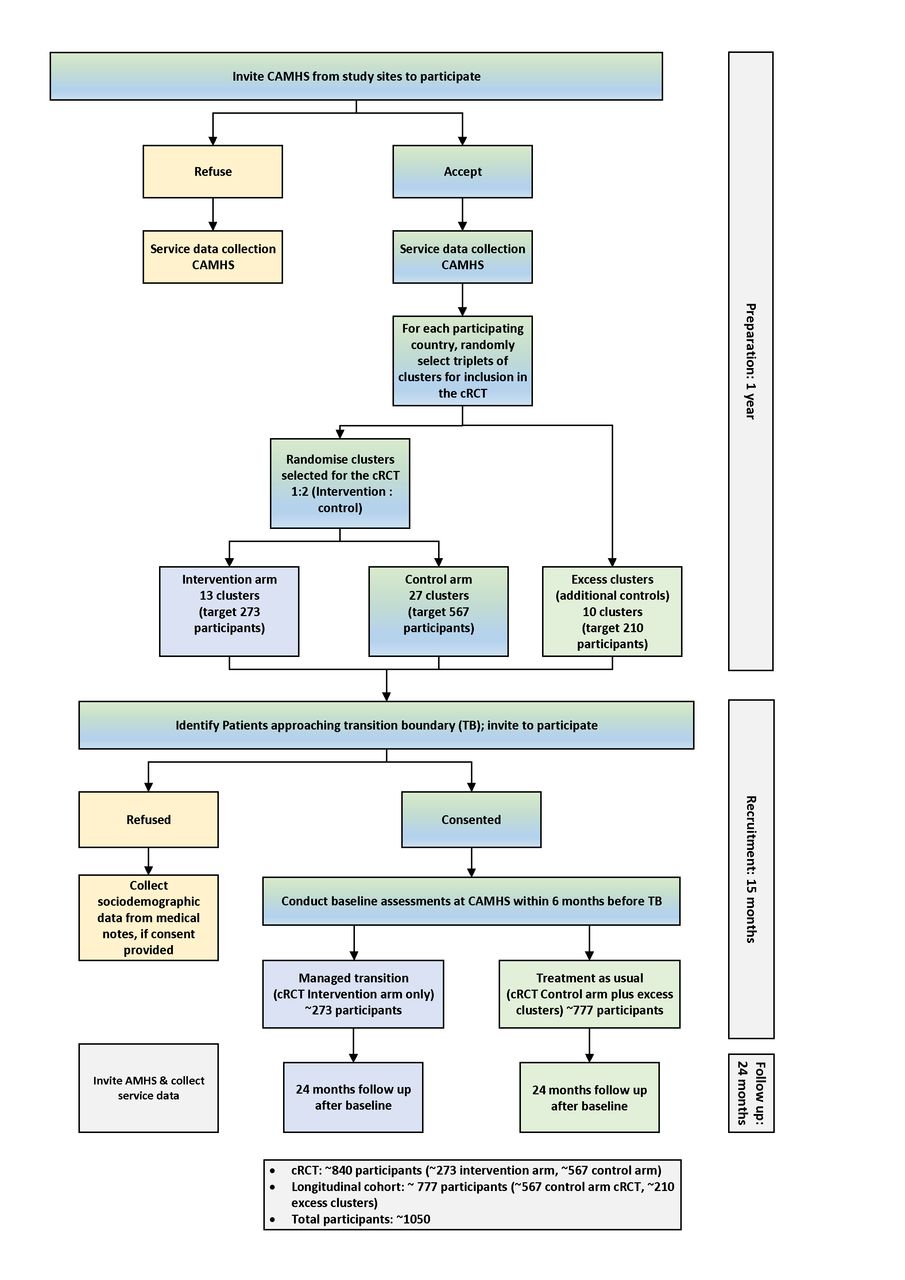
A large cohort of young people approaching the CAMHS–AMHS transition boundary in eight EU countries will be recruited and a nested cRCT in a randomly selected subset of clusters (CAMHS) will be implemented. The study design is a modification of the Cohort Multiple Randomised Controlled Trial,53 by virtue of allocation to the intervention by cluster randomisation, with each distinct CAMHS comprising a cluster. The control arm clusters from the cRCT together with additional excess clusters form the longitudinal cohort study, with a follow-up period of 24 months. The cRCT is a superiority trial; the aim is to show that managed transition is superior to usual care in improving patient-reported outcomes. Usual care varies by CAMHS and may or may not include transitioning planning. The primary outcome endpoint is 15 months. The study flow diagram is presented in figure 1. All arms of the study undergo the same data collection. The trial has economic and qualitative components, addressing objectives 2 and 3, respectively. Detailed Statistical Analysis Plans have been developed for both the cRCT and longitudinal cohort study. Final versions will be signed off prior to commencement of the analysis and made available on the study website.
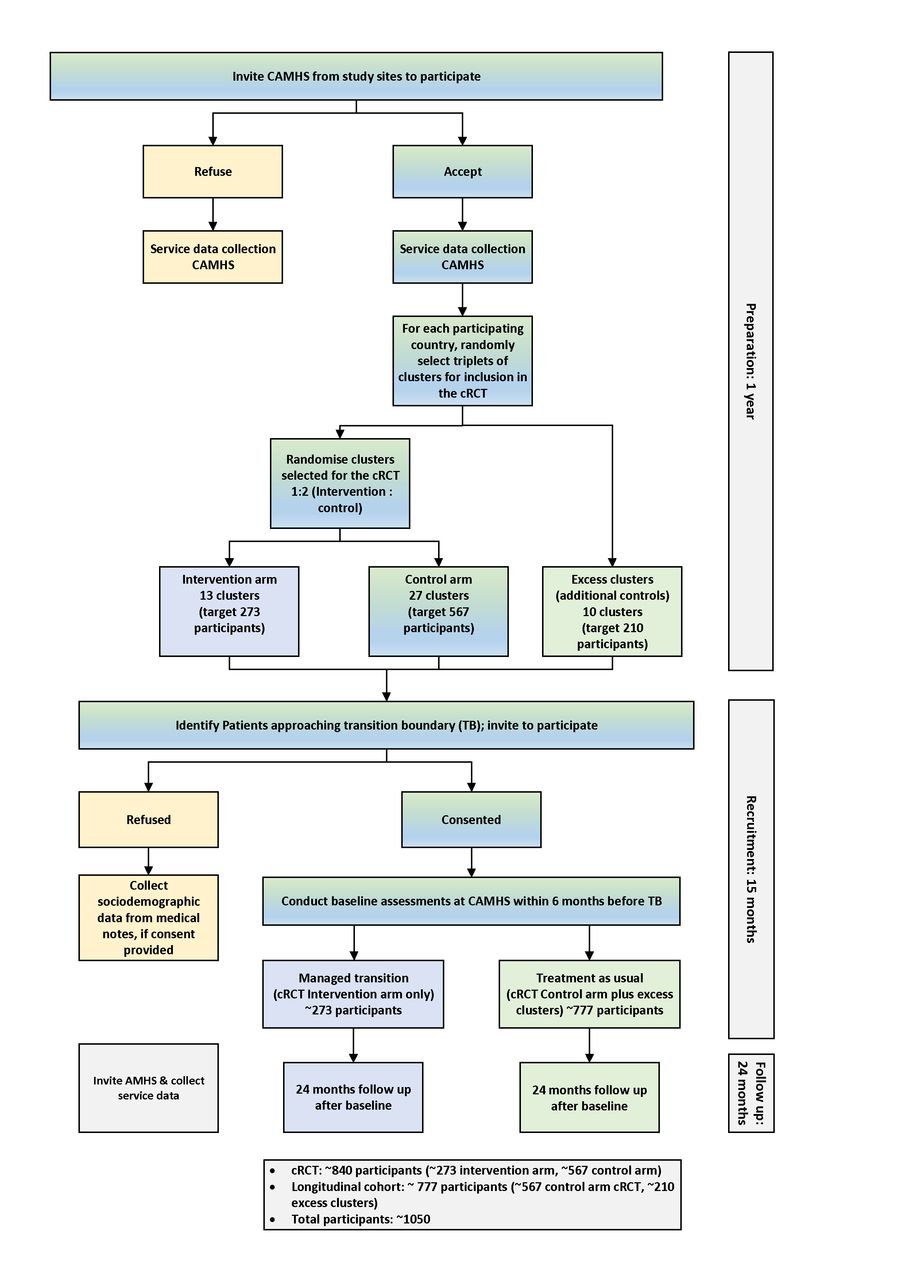
MILESTONE study flow diagram. AMHS, adult mental health services; CAMHS, child and adolescent mental health services; cRCT, cluster randomised controlled trial; MILESTONE, Managing the Link and Strengthening Transition from Child to Adult Mental Healthcare.
The study is sponsored by the University of Warwick and coordinated from the research office in the Mental Health and Wellbeing unit, Warwick Medical School, with Quality Assurance and Statistics from Warwick Clinical Trials Unit. The study coordinator is responsible for the day-to-day coordination and the chief investigator (CI) for clinical aspects. The study is managed by a trial management group (TMG), including work package leaders (ie, country leads), and supported by MILESTONE research staff. The TMG speaks monthly by telephone conference chaired by the CI. The study conduct and progress are overseen by the independent MILESTONE Scientific, Clinical and Ethical Advisory Board (SCEAB) comprising five international experts and four patient and public involvement (PPI) representatives. The SCEAB members are invited to the annual general meetings in order to monitor the progress of work, to assess the scientific quality and to give feedback to the Consortium members, but without a right to vote. The SCEAB will also review the main governance and any ethical issues that might require greater attention.
MILESTONE has strong PPI embedded throughout the project; young advisors, some with experience of transition in mental health services, provided feedback on the protocol and study documents, and designed the intervention leaflet. Their ongoing role includes attending and contributing to project steering committee meetings, developing other promotional materials, and advising on recruitment and the engagement of young people. The first five PPI representatives have been from the UK; in the third year, service users from other participating countries will be involved.
Setting and site selection
The study is currently running in Belgium, Croatia, France, Germany, Ireland, Italy, the Netherlands, and the UK. Recruitment of participants is underway in 52 CAMHS clusters that fit the inclusion criteria below (October 2015–December 2016, with last inclusions in January 2017). Face-to-face meetings with clinical and managerial leads were arranged at those sites that expressed an interest and the study was explained in detail. Signed site agreements or equivalent were obtained from participating sites prior to the start of the study. The majority of sites received no funding from the EU grant (no 602442) for taking part in the study. However, two German recruiting sites received payments under subcontract to facilitate recruitment.
In most countries, other than the UK, there is no umbrella organisation to facilitate collaboration between AMHS and CAMHS. Furthermore, a single CAMHS may be linked with numerous AMHS (inpatient services, clinics, teams and individuals), making it difficult for AMHS clinicians to be engaged from the start, particularly given our limited resources. Also, we were not able to predict which AMHS would be involved, as this is dependent on transition decisions.
Cluster-level eligibility criteria
For a CAMHS to be eligible, it had to be a service delivering medical and psychosocial interventions for children and adolescents with mental health problems and disorders, and/or neuropsychiatric/developmental disorders (eg, emotional/neurotic disorders; eating disorders; hyperkinetic disorder/attention deficit hyperactivity disorder; autism spectrum disorders); community-based, or provide outpatient or inpatient care; publicly or privately funded; have a formal upper age limit (the transition boundary) for providing care to young people; and be responsible for transfer of care to an adult service for those who reach the transition boundary. Forensic services and highly specialised national services, which cater to rare/unusual disorders and/or serve a national population, such as specialist clinics for rare metabolic disorders or long-term residential care for severe autism, were excluded. Eligible services could vary in size and complexity, ranging from single psychiatrists or psychologists (eg, Germany) or circumscribed teams, to services with multiple teams and localities offering multidisciplinary care (eg, UK).
Baseline service-level data collection
Baseline service data were collected from the CAMHS manager or leading CAMHS clinician at all recruited CAMHS in the year preceding recruitment of study participants. The questionnaire covered (1) size (number of staff), structure and function of CAMHS; (2) transition boundary of the service (ie, age at expected transition); (3) the number and type of AMHS that operate within the CAMHS catchment area; (4) current transition policy and practice; and (5) size of the catchment population. This information was used to establish the organisational structure of CAMHS and identify potential crossover and/or movement of staff between teams or units so that distinct units (clusters) could be identified. If one or more CAMHS teams share the same core clinicians, then these were classified as one cluster, becoming the unit of allocation.
The data revealed that the CAMHS–AMHS transition boundary for most countries was 18 years, that is, the age of majority. In the UK, Belgium and France, there was more variation, the boundary ranging from 15 to 18 years. We also discovered that some services in Belgium, France, the Netherlands and Germany adopt a more flexible approach to the boundary, and in these situations we agreed a nominal boundary (18 years), which reflects the age at which transitions most commonly occur and, in most instances, is also the official transition boundary.
On leaving CAMHS care, young people may be referred on to AMHS or another community-based service (eg, social services, voluntary sector or other non-statutory agencies offering support and therapeutic interventions for mental health needs), or discharged back to their GP. AMHS and community-based services will be invited to participate in the study, and service-level data will be collected once they are recruited.
Randomisation
As several countries only had three CAMHS clusters, this fixed the randomisation ratio at 1:2 and the randomisation was conducted in a two-stage process: First, randomly selected triplets of clusters within each country were identified for inclusion in the cRCT. These three clusters were further randomised in a 1:2 ratio between intervention and control arms. The excess clusters (those not selected during the first stage for the cRCT) were used for the cohort study only to enhance numbers. Overall, this two-stage process equates approximately to a randomisation ratio of 1:3. All randomisations were conducted by the trial statistician using the statistical software Stata V.14.54
The CAMHS were informed of their allocation after randomisation. The study personnel were also aware of the allocation as they are involved in delivering the intervention and assessing outcomes. The young people and their parents/carers, who are recruited after randomisation, are informed of their allocation after they have consented to the study, yet only if they ask about this specifically.55
Participant eligibility and recruitment
Young people
Individual recruitment targets were set for each CAMHS (cluster), based on local capacity, but with the constraint that in the cRCT there should be on average 21 participants per cluster. Databases of all participating CAMHS are scrutinised by CAMHS personnel to identify all young people approaching the service’s transition boundary and meeting the inclusion criteria over a 15-month recruitment period (between October 2015 and December 2016).
Young people are eligible if (1) their age is within 1 year of reaching the transition boundary of their CAMHS during the trial recruitment period and, in exceptional cases, not more than 3 months older than the transition boundary, if a decision about transition has not yet been made; (2) they have a mental disorder defined by the Diagnostic and Statistical Manuals of Mental Disorders, DSM-IV-TR (4th edition text revision), or DSM-5 (5th edition), or the International Statistical Classification of Diseases and Related Health Problems 10th and 11th revisions (ICD 10/11), or they are under the regular care of CAMHS (attended at least one appointment, if not yet diagnosed); (3) they have an IQ ≥70 as ascertained by previous standardised assessment or diagnosed by clinician, or no indication of intellectual impairment; and (4) they provide valid written informed consent, or assent, if below the legal age of consent (in England this age is 16, in all other participating countries 18). They are ineligible if they (1) are younger than a year before the transition boundary of their CAMHS; (2) have a more severe intellectual impairment (IQ <70), as ascertained by previous standardised assessment or diagnosed by clinician—if no data on intellectual functioning are available (because it has never been assessed), then care coordinators are asked to make a clinical judgement on intellectual impairment before baseline assessment takes place; (3) are not able to (or expected not to be able to) complete the questionnaires due to severe physical disabilities or language problems, even with assistance from family members or a research assistant; (4) are service users in a secure forensic institution; or (5) do not provide valid written informed consent, or assent, if below the legal age of consent.
At each site, the clinicians of eligible young people advise the research team of the ability/capacity of the young person to give informed, voluntary consent or assent. Young people are introduced to the study (as appropriate, taking local ethical/legal conditions and best practice into consideration) either by (1) a clinician or care coordinator, who provides a study leaflet and/or briefing sheet and seeks consent for the individual to be contacted by a MILESTONE research assistant using a signed contact form; (2) a letter signed by their care coordinator or clinician outlining the purpose of the study followed by a phone call by a CAMHS personnel if no response is received; or (3) posters and/or leaflets displayed in the participating CAMHS sites, with contact details of the research team.
All young people who agree to be approached by a MILESTONE researcher are individually contacted and provided with further information about the study; interested individuals are asked to sign a study consent form. Young people who are below the legal age of consent are asked for their assent and signed consent is obtained from a parent/carer (or, in some countries, parents/carers, according to national medical ethics requirements).
A compensatory inclusion process has been factored in; if one country is unable to meet its recruitment target, another country is allowed to over-recruit.
Parents/carers
The information provided to young people includes separate information and consent forms for their parents/carers. After signing up to the study, the young person is asked to name his/her primary caregiver, whom he/she would like to be involved. For young people under the legal age of consent, the parent/carer has to be the legal guardian of the young person. The aim is to engage the same parent/carer throughout the whole study period. If the latter is not possible, then the aim is to involve another parent/carer. If the young person does not live with his/her biological parent/s, then his/her carer is involved. A carer may be the legal guardian or a partner or an older adult sibling, or another individual living with and/or providing regular support to the young person.
The parent/carer is eligible if the young person consents to parent/carer participation and he/she provides a valid written informed consent. A parent/carer is ineligible if he/she does not live with and/or provide regular support to the young person, and/or is not able to (or expected not to be able to) complete the questionnaires due to severe physical disabilities or language problems, even with assistance from family members or a research assistant.
Young people who do not wish their parent/carer to be approached to participate in the study have their wishes respected, regardless of their own capacity to consent. If a parent/carer is unwilling to participate, their wishes are respected.
Clinicians/care providers
Clinicians/care providers are contacted and provided with separate information sheets and consent forms. They are eligible if they are responsible for the main care for the young person at CAMHS (and AMHS or other relevant service provider, if referral is made) and provide a valid written informed consent.
Intervention
The CAMHS in the intervention arm receive information on good-quality managed transition and feedback from the TRAM assessment in the form of a TRAM score summary report for each participating young person.
Information provision at CAMHS
A special meeting is held between MILESTONE personnel and participating CAMHS in the intervention arm prior to service user recruitment to establish clinicians’ existing knowledge and current practice of transition, and to discuss optimal transition, using TRAM as a decision support tool, and managed ending of care. Each meeting follows a prescribed structure. Additionally, written information on good-quality transitional care is provided to all clinicians in the intervention arm CAMHS teams. This consists of presentation handouts and a leaflet on good-quality transition designed by our young project advisors.
Feedback of TRAM results
The aim is to conduct the TRAM assessment approximately 6 months prior to the transition boundary. The TRAM findings (TRAM score summary report) are fed back to clinicians soon after the young person, parent/carer and CAMHS clinician have completed the baseline assessments.
The TRAM results are communicated to the CAMHS clinician in a secure fashion via an email, attaching the TRAM score summary report (which contains no identifiable information), and an offer is made to explain the findings at a face-to-face meeting. If no response is received, the email is followed up once only with a telephone call.
The CAMHS clinician is encouraged to communicate the TRAM findings to the young person and parent/carer, and incorporate critical information to young person’s care or transition plan, and design goals for critical items that are achievable.
The CAMHS clinician decides whether or not to refer the young person to adult services.
If a referral is made, the CAMHS clinician is asked, if appropriate and with relevant permissions, to send the TRAM score summary report along with the referral letter to the new adult service.
The AMHS clinician or other care provider is offered a chance to discuss the TRAM findings with an appropriate member of the MILESTONE research team.
The aim of the TRAM score summary report is to support clinicians in their decision making regarding transition, communication with stakeholders and planning of the transition process. A flow chart of the study intervention is depicted in figure 2.

{kind=link}
{kind=link}
Flow chart of study intervention (feedback of TRAM results) and follow-up assessments with young person. AMHS, adult mental health services; CAMHS, child and adolescent mental health services; P/C, parent/carer; RA, research assistant; TRAM, Transition Readiness and Appropriateness Measure; YP, young people.
The control arm
Young people, parent/carers and clinicians in the control arm complete the same baseline assessments, but the latter do not receive any additional training or feedback of TRAM scores, that is, continue providing usual care, which may or may not include transition planning.
Outcome measures
Primary outcome measure
The primary outcome measure is the clinician-rated Health of the Nation Outcome Scale for Children and Adolescents (HoNOSCA),56 which has 15 items scored on a scale of 0–4, and covers the severity of the behaviour, impairments, symptoms and social functioning of children and young people with mental health problems. The clinical usefulness of the HoNOSCA has been validated and its sensitivity to change confirmed.57 58
Although the HoNOSCA is intended as a measure that is completed by a clinician who is also responsible for treatment of the client, the measure can also be completed by a mental healthcare professional not involved in the treatment using semistructured interview.59 In our study the measure is completed by a trained MILESTONE research assistant by interviewing the young person and taking into account all other available sources of information (parent/carer, relevant clinician and the medical records) to ensure accuracy of data.
To ensure consistency and comparability, HoNOSCA is used throughout (rather than switching to HoNOS at age 18 years). The primary outcome endpoint for the cRCT is 15 months.
Secondary outcome measures
The secondary outcome measures are as indicated in table 1. Apart from the TROM, two others were developed specifically for the MILESTONE study.
Outcome measures
The Ethics of Transitioning questionnaire was developed based on the themes raised by a systematic literature review and focus groups and addresses the following research question: ‘What are the ethical challenges of ensuring delivery of transitional care to those who need it most against the risk of pathologising transient and self-limiting distress and dysfunction, which may be normal during adolescence?’ It contains seven items rated on a 5-point Likert scale, with one version to be completed prior to, and another after, transitioning.
The Life Events questionnaire is a dichotomous 13-item scale that is appropriate for both young people and adults, and focuses on significant life events, such as accidents, deaths in the family and separation of parents/carers.
Data collection
Data collection is the same in the intervention, control and cohort arms of the study.
Baseline data
Table 2 highlights the number of contacts with the participants, the time points of the various assessments, and the type of data to be collected from the young person, parent/carer and clinician.
Study assessments for participants (transition scenario)
The baseline assessment (T1) is undertaken after consent/assent has been given but before the delivery of the intervention, within 6 months before the transition boundary of the service or, in exceptional cases, within 12 months before or 3 months after the boundary (eg, if transitions regularly happen earlier in a service or a decision about transition has not yet been made). Young people and their parents/carers are assessed at the clinic, or at an alternative location suitable for the young person, with both semistructured interview (sociodemographic and personal information, and HoNOSCA) and online assessment. The sociodemographic and personal information questionnaire for young people and parent/carers collects general information about the young person and family, and the care the young person receives. The questionnaire covers also medical history and additional variables previously shown to contribute to continuity of mental health problems (eg, history of mental health problems and alcohol or drug abuse by parents). The last online assessment of T1 is the structured sections of the Development and Well-Being Assessment (DAWBA),60 61 which obtains information on mental health. Information from the assessment with the young person and parent/carer will be combined with a computer algorithm that provides an estimate of the probability of a certain individual diagnosis. Information on clinical diagnosis is obtained from the clinician.
The length of the baseline assessment (young people) is approximately 1.5–2 hours. The participant can take a short break in between the online measures, and if required, complete them over multiple sessions. The research assistant is available to assist if there are any difficulties. The baseline assessment (T1) should be completed before the end of the recruitment period.
Follow-up data
Outcomes are measured 9 months (T2), 15 months (T3) and 24 months (T4) after T1. The aim is to complete measures at T2 and T3 via telephone and online assessment, and at T4 via face-to-face contact with young people and their parents/carers, within a month (±) of the calculated assessment time point (table 2). Assessments with CAMHS or AMHS clinicians (or other service provider), which are dependent on transition status, follow the same schedule.
Evaluation of the intervention and experiences of young people regarding services
The views and experiences of CAMHS clinicians in the intervention arm are captured using a semistructured questionnaire. All clinicians are approached and those willing to engage are interviewed over the telephone or face to face.
A subsample of young people taking part in the study will be invited to take part in focus groups at T4 from three participating countries: Ireland, UK and Croatia. The purpose of the focus groups will be to explore their experiences of leaving CAMHS, transition to AMHS if applicable and views of mental health services, the aim being to establish whether young people have better health, educational and social outcomes, better quality of life, and satisfaction with services if they (1) have experienced a managed transition from child to adult services at the transitional boundary or (2) have experienced usual care (ie, their transition to adult services, or their discharge from services, is via the usual procedure of their CAMHS clinic). It is hoped that, as part of MILESTONE’s PPI activity, some of the young advisors, or other young people trained in facilitation skills by some of the research sites, may cofacilitate these focus groups.
Three audio-recorded focus groups will be held in each country with 9–12 young people in each group. Recruitment will be from the study participants with purposive sampling to include some young people who (1) did not transition to adult services, (2) who transitioned to adult services via usual care and (3) who experienced managed transition.
Sample size
Assuming an average cluster size of 15 participants, an allocation ratio of 2:1 (control:intervention), a coefficient of variation of cluster size of 0.4 (cluster sizes ranging from approximately 5 to 30), and an intracluster correlation coefficient of 0.01, with 600 participants (195 intervention arm (13 clusters), 405 control arm (27 clusters)), the cRCT has 89% power to detect a difference of 0.30 SD in the primary outcome measure (HoNOSCA). To allow for 30% dropout, the required average cluster size is 21 participants. Thus, for the cRCT the target sample size is 840 participants in total (273 intervention—13 clusters of size 21; 567 control—27 clusters of size 21). The randomisation was stratified by country, with the number and size of clusters dictated by local capacity. Excess clusters (those not required for the cRCT) were allocated to the control arm and will be used in the analysis of the cohort study only to enhance numbers for sufficient power to study predictors for the longitudinal course and outcome of mental health during transition. There are 10 such excess clusters (average size 21 before dropouts). The recruitment target for the cohort study is therefore 777 participants (567 from the control arm of the cRCT plus 210), and the total recruitment target is 1050 (840 plus 210).
Retention of study participants
To ensure that contact is not lost with any members of the study population during the follow-up period and that data are as complete as possible, MILESTONE has paid considerable attention to its engagement and retention strategies, drawing extensively on the advice and experiences of its young advisors to create a special ‘Bonding Plan’. Participants may be contacted using several methods of communication (post/phone/email); contact details of all participants, including GP and CAMHS clinician details, are recorded in a ‘keeping in touch’ form; data are collected in several different ways (face to face, online, phone); and each contact, or contact attempt, made with participants is recorded in a bespoke contact log. There are multiple contact points between study assessments, where the participants can advise of any changes to their contact details. The Bonding Plan activities vary by country, taking local ethical and cultural requirements into consideration. Items include thank you cards, newsletters, gift vouchers and a chance to win a prize in a lottery. The value of gift vouchers provided after assessments range from £10 to £20 or similar equivalent in euros. In Italy and Croatia, the research ethics committees did not allow providing any gifts after the individual assessment time points. Reasonable travel expenses are reimbursed for young people and their parents/carers.
Losses to follow-up
Due to the characteristics of the study population group (young people, highly mobile, in the process of moving on to higher education, training or work), we have allowed for a 30% dropout rate.
Withdrawal of young people from the study
All participants remain in the study and follow-up data are sought unless consent for participation in data collection is explicitly withdrawn.
Data analysis
Detailed Statistical Analysis Plans, which include specific methods of analysis for each outcome variable, have been developed individually for both studies, and final versions will be reviewed and approved by the TMG and made available on the study website (http://www.milestone-transitionstudy.eu/).
Sensitivity analyses using multiple imputation will be conducted to explore the potential impact of missing data.
Cluster randomised controlled trial
Basic descriptive methods will be used to present the data on study participants, trial conduct, clinical outcomes and safety (in total and for each study group separately). The primary outcome will be HoNOSCA score at T3, and we will test the hypothesis that there is no difference in this between the managed transition and standard care arms over the study period using a multilevel model with random effects to account for clustering and repeated measures, and adjustment for design factors (country and size of service). Where appropriate, a similar approach will be applied to the analysis of secondary outcomes. All analyses will be on an intention-to-treat (ITT) basis.
Cohort study
Baseline, longitudinal course and outcome data at T4 will be analysed. Trajectories of mental health, subjective need for care and quality of life will be determined using mixed growth models and related to whether transitions from CAMHS to AMHS took place.
Data will be analysed to predict and characterise those with higher primary and secondary outcome scores. Functional, clinical and quality of life outcomes will be assessed in those CAMHS users who transition with those who do not transition to AMHS.
Economic evaluation
Health economic data collection
To conduct the economic evaluation of the trial, information on healthcare usage, social care usage/social costs and intervention costs will be captured. Additionally, participant health-related quality of life (HRQL) and HoNOSCA score will be recorded.
Resource use data collection
Health and social care resource utilisation for both trial arms will be estimated using the MILESTONE-specific Client Service Receipt Inventory (CSRI), which draws on a CSRI used previously to estimate mental healthcare costs in the UK,62 but has been substantially revised for use in MILESTONE. It includes questions regarding healthcare usage, and relating to social and judicial resource use, and these questions are tailored for each participating country to reflect local services. Young people complete the measure at all four time points. For the purpose of economic evaluation, a questionnaire on the burden and impact of TRAM will be completed by all clinicians within the cRCT. This will assess how much extra burden is placed on staff involved within the transition process due to the intervention compared with usual care.
The intervention costs associated with managed transition include the cost of implementing, as well as the delivery of the intervention. Questionnaires have been distributed to researchers in each country to ascertain the resources required to set up the intervention, while Excel logbooks capture the time spent by clinicians completing the TRAM. Likewise, the time spent by the University of Warwick preparing the TRAM report is logged within an Excel database, and clinician questionnaires will be used to capture the impact of the intervention on resource use.
Outcomes for economic evaluation
The two primary outcomes for the economic evaluation are quality-adjusted life years (QALYs) and HoNOSCA score.56 57 HRQL will be measured using the EuroQol health questionnaire (EQ-5D-5L),63 and index scores64 will be applied to calculate QALYs to determine the impact of the intervention on HRQL. Changes in QALYs and HoNOSCA score between the two trial arms will be examined in conjunction with the costs to examine the cost-effectiveness of the intervention on mental health.
Economic evaluation: analysis
General principles of the economic analysis
Intention to treat: As recommended by best practice,65 an ITT framework will be adopted. For each individual within the trial, the analysis will be conducted according to which arm they were randomised.
Perspective: The base-case analysis will adopt a healthcare and personal social services perspective in accordance with NICE recommendations.65 Given the widespread acknowledgement of the wider costs of poor mental health,66 a societal perspective will be adopted as a secondary analysis. Societal costs will include social care, productivity and criminal justice system contacts.
Time horizon: The base-case analysis will be a trial-based analysis and therefore consider just the years followed up within the trial. Given the complexity of the trial, the potential for long-term decision modelling and extrapolation will be informed by a systematic review of the methods used within existing mental health literature. Long-run extrapolation will therefore be considered in light of this.
Discounting: As recommended by NICE,65 all costs and outcomes that occur after the first year of the trial will be discounted at 3.5%.
Missing data: 67 Should missing data be prevalent, the health economics analysis will address missing data through the use of multiple imputation.67
Clustering: The hierarchical nature of the data needs to be addressed within multiple imputation procedures and within the analysis framework. To do this, random effects approaches will be used.68
Uncertainty: The uncertainty around the results will be assessed through sensitivity analyses and the generation of cost-effectiveness acceptability curves.69
Calculating costs for economic evaluation
Data on staff time and other resources in the transition process will be obtained at each location, and costed using appropriate sources of unit cost data (eg, for the UK, standard unit cost sources include the National Health Service (NHS) reference costs and the Unit Costs of Health and Social Care report published annually by the Personal Social Services Research Unit at the University of Kent). This will result in location-specific estimates of the direct costs involved in implementing the managed transition process.
Outcomes for economic evaluation
The primary economic analysis will be a cost utility analysis. The EQ-5D-5L measure allows the calculation of QALYs. These will be calculated for each young person within the trial using the trapezium rule to calculate the area under the curve. An underlying assumption of this methodology is that there is a linear line between each utility value at each follow-up. When analysing incremental QALYs between trial arms, it is important to adjust for baseline differences in utility70 and to account for the hierarchical nature of the outcome data.68 The base-case analysis of effectiveness will therefore use methods that incorporate a random-effects regression model controlling for baseline health status and accounting for clustering.68 EQ-5D-5L tariffs for each participating country, where available, will be used to allow for country-specific economic analyses. The cost-effectiveness of the intervention over the duration of the trial will be examined, and decision uncertainty assessed using probabilistic sensitivity analysis and scenario analysis.
Data management
Online data collection
All measures apart from DAWBA are completed using HealthTrackerTM, which allows measures to be completed remotely using developmentally appropriate interfaces. It also enables participants to skip modules if they do not score on screening questions for that module, thereby reducing the time needed for completion. Each questionnaire has been optimised for the screen, based on feedback from service users and providers. HealthTrackerTM automatically generates random participant (service user, parent and clinician) ID numbers and passwords when the participant is entered onto the system. HealthTrackerTM stores participants’ month and year of birth. All other data are anonymised.
The DAWBA is completed using the website http://dawba.net and anonymised scores (identified and linked using the unique DAWBA ID) are transferred to a bespoke form on the HealthTracker system. A secure database developed at Warwick Medical School stores information that is not collected by HealthTrackerTM. This includes participant name, unique study ID, HealthTracker and DAWBA IDs, contact details, information linking participants (eg, young person to CAMHS clinician) and service-level information. This database is maintained locally at sites with access password-controlled and strictly limited to MILESTONE personnel to ensure confidentiality. No personally identifiable information relating to participants leaves the local site. Only the unique identifiers, linking information (using identifiers) and service-level data are shared with Warwick Medical School.
Paper copies of measures are only used as a last resort, or if preferred by the participant. All MILESTONE researchers have received training on the HealthTrackerTM platform and other systems for data collection prior to the study beginning.
Data transfer
All transfers of study data are informed by and comply with the European Parliament and the Council of Europe’s Directive 95/46/EC on protection of individuals with reference to the handling of personal data and on the free flow of such information between EU countries.
To ensure the security and integrity of data during such transfer, an appropriate documented standard procedure has been established and will befollowed without exception. Any study data that are to be transferred between research sites are anonymised prior to transfer.
Data storage
All essential documentation and trial records are stored by Warwick Medical School and participating local sites in conformance with the applicable regulatory requirements with access to stored information restricted to authorised personnel.
Data access and quality assurance
In all partner countries, local research ethics committee requirements and national and EU law underpin the collection, recording, sharing and secure storage of person identifiable data.
Personal information about potential and enrolled participants is collected, shared and maintained in a manner that protects their confidentiality before, during and after the trial. All researchers working on the MILESTONE study are experienced in undertaking research in a way that maintains the privacy and confidentiality of study participants but which balances these demands against the need to ensure that participants are not at risk. Names or addresses of participants are not disclosed to anyone other than the staff involved in running the trial.
Data are only accessible by authorised personnel and made available to relevant bodies for audit purposes only.
At the end of the MILESTONE project, analysis data sets will be made available following University of Warwick’s Research Data Management Policy, which ensures that data produced through the university’s research activities are registered, stored, made accessible for use and reuse as appropriate, managed over time and/or disposed of, according to legal, ethical, funder requirements and good practice (http://www2.warwick.ac.uk/services/rss/researchgovernance_ethics/research_code_of_practice/datacollection_retention/research_data_mgt_policy/).
Archiving
Data from this study will be retained intact in an appropriate format and storage facility for a minimum of 10 years in the UK in line with the Medical Research Council’s guidelines on Personal Information in Medical Research; other countries will follow their relevant guidelines (http://www.mrc.ac.uk/documents/pdf/personal-information-in-medical-research/).
Monitoring
UK sites are monitored by Warwick Medical School. Monitoring includes compliance to the protocol, quality of data collection and storage of documentation, and requires monitors to have access to relevant participant notes/charts and trial documentation. Each overseas party is responsible for monitoring its sites according to local procedures.
Adverse event management
A young person experiencing adverse events as a direct consequence of the intervention is unlikely, as the intervention is aimed at the clinician. At each study assessment, the young person is asked whether any adverse events (bad or unfavourable medical occurrence) have occurred since the last time point. This includes events from the first trial-related activity after the participant has signed the consent form until the endpoint of the trial as defined in the protocol. Any worsening of concomitant illness or new illness is recorded as adverse events at each visit. If the event is classified as a serious adverse event (SAE), an SAE form is completed and the principal investigators of each country report all SAEs immediately to the trial coordinating centre at Warwick Medical School. The trial CI determines whether SAEs require reporting to the trial sponsor or SCEAB.
Ethics and dissemination
Ethics and research and development governance
The study has been approved by the National Research Ethics Service in the UK (West Midlands—South Birmingham Research Ethics Committee, Ref no 15/WM/0052) and by the research ethics committees of all partaking countries. Regional and site-specific approvals have been obtained from NHS Research and Development offices in the UK and from other similar bodies in the other countries. The study is registered with the International Standard Registered Clinical/soCial sTudy Number (ISRCTN) registry (ISRCTN83240263) (http://www.isrctn.com/ISRCTN83240263?q=MILESTONE&filters=&sort=&offset=3&totalResults=21&page=1&pageSize=10&searchType=basic-search) and ClinicalTrials.com (NCT03013595) (https://clinicaltrials.gov/ct2/show/NCT03013595?term=NCT03013595&rank=1).
The ethical conduct of the study is monitored throughout by the MILESTONE ethics work package.
Service users
We are involving a potentially vulnerable population in research: adolescent mental health service users, most of whom are over the age of 16, but in areas where the transition boundary is 16 years (some parts of England) or 16.5 years (some parts of France) they are 15 years of age. In England, the legal age of consent is 16, whilst in all other participating countries it is 18.
Despite best efforts, vulnerable people, either by virtue of being young and/or with mental health difficulties, are often omitted from research studies because of concerns regarding informed consent.71 72 The researchers in this study acknowledge these concerns and risks but also recognise the importance of including individuals with enduring mental health difficulties in the study to better inform practice. The Council of Europe strongly promotes the participation of children in decisions affecting them.73 Young people also have rights as service users to expect appropriate and good-quality services.
The participant information sheets and consent/assent forms make explicit the voluntary nature of young people’s involvement. Even if the parent/carer gives consent but a young person refuses, that young person is not included in the study. The young person’s consent is sought before follow-up assessments (verbal consent for telephone interviews), consent being implicit when they log on to give responses online. The forms also seek permission to delay data collection until a later point should a young person become unwell or due to some other pressing circumstances, as long as transition does not take place in the meantime. The forms explain the various safeguards in place, namely to liaise with a young person’s clinician and/or family, if required, and the resulting impact on confidentiality.
In order to minimise any distress to young people taking part in face-to-face interviews, wherever possible these are organised at a time and place convenient to the young person when there are familiar staff or a parent/carer on hand to offer support should a young person become upset during any data collection processes.
In the event that during an assessmenta MILESTONE researcher identifies any situation where a young person is thought to be at risk of abuse or neglect, or the young person discloses information that raises concern about theirsafety, then a detailed risk management plan is followed, which stipulates that the child protection policies and procedures applicable to that country are adhered to. This is likely to involve close liaison by the researcher and the MILESTONE lead for that study site, with the young person’s clinician and/or the nominated child protection leads within the mental health service attended by the young person. Also, young people consenting to the study are asked to nominate and provide contact details fora health/care professional (eg, GP or CAMHS clinician) who can be contacted should any adverse event arise. This safeguard is made explicit in the study information leaflets, and at all data collection time points.
Training
All research assistants have participated in training sessions addressing good clinical practice, transition practices, rating procedures, compliance, TRAM feedback, and communication with young people, families and clinicians. A special focus of the training has been the primary outcome measure, the clinician-rated HoNOSCA, completed by research assistants. The training has included ratings and discussions of clinical vignettes and how to conduct the HoNOSCA interview.74 The study has been presented to all participating CAMHS teams and additional meetings have been held to implement the specific transition procedures in the intervention clusters.
Dissemination
The MILESTONE project has a work package that focuses on dissemination. Partnerships and networks with target bodies will be strategically developed to support both short-term and long-term dissemination of the MILESTONE study and other project findings. External dissemination will target the scientific community, but also the general public, lay and patients’ associations, healthcare authorities and caregivers, scientific societies and professional boards, students, policy makers, and the pharmaceutical industry. Particular attention will be paid to the information needs of the various target audiences, ensuring that they are addressed in the appropriate language and format.
The results of the MILESTONE study will first be made available to the clinicians of partaking CAMHS and AMHS , and then to the scientific community at large via publications in scientific journals, presentations at meetings, the MILESTONE website (http://milestone-transitionstudy.eu), press releases and leaflets.
Conclusion
The continuity of adolescent psychopathology into adulthood means that transition to AMHS is necessary for many. However, there are real gaps in mental healthcare provision at this crucial stage, and those who experience transition frequently describe it as disruptive. The MILESTONE study is the first ever methodologically robust trial to test whether a decision support and assessment tool, the TRAM, can improve the mental health and social outcomes and functioning of transition age young people receiving CAMHS care. Young people in eight European countries are partaking in the trial and their longitudinal course of mental health, social and adult functioning outcomes are evaluated as part of a prospective cohort study. The MILESTONE study has crucial input from young advisors, some with experience of transition in mental health services. Overall, this is an ambitious and challenging study which will provide a timely and valuable insight into an under-researched population.
Acknowledgments
We are very grateful for the CAMHS and AMHS services and research teams who are collaborating in this study in the eight European countries. We also extend thanks to all the participating service users and their parents/carers. We are also grateful to the members of the MILESTONE Scientific Clinical and Ethical Advisory Board (SCEAB)—Norman Sartorius, Pat McGorry, Maryann Davis, Mario Maj and Adriana Mihai—and to Tanveer Sandhu and Philippa Coleman for reviewing the protocol. We would also like to thank the members of the wider MILESTONE Consortium for their contribution. We extend a special thanks to Andrea Wohner, our project manager based at Concentris Research Management, Fürstenfeldbruck, Germany, for excellent project management and delivery.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.
- 76.
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.
- 85.
- 86.
- 87.
- 88.
Footnotes
Contributors SS is the chief investigator who conceived the original study design and obtained funding, together with AM, GDG, PS, JM, FM, DP-O, ST, US, TF, CS, MP, DW, FCV and GCD. HT is the study coordinator who prepared the first draft and subsequent versions of the protocol and this manuscript, and is joint first author with SS. JW and AC contributed to the manuscript. JW is the senior trial statistician who led the calculation of the sample size; JG will undertake the statistical analysis under her direction. JM designed the health economic component, and AC will undertake the health economics analysis under his direction. CD is the quality assurance manager. PT, SG, GS, LA, FR, SA, LOH and ND are research assistants and helped set up the study in their countries and gain local ethical approvals. The UK young advisors, AT, AW, CG and LW, reviewed the proposed study scales (including the likely time required for completion, to assess for possible burden on study participants), participated in the design of the intervention leaflet and reviewed all study information material before submission to ethics. All authors critically reviewed the protocol and the manuscript, and gave approval for the publication.
Funding The MILESTONE project has received funding from the European Union’s Seventh Framework Programme for research, technological development and demonstration under grant agreement no 602442. This paper reflects only the authors’ views, and the European Union is not liable for any use that may be made of the information contained therein. The funding body has had no role in the study design, in the writing of the protocol or in the decision to submit the paper for publication.
Competing interests PS is the director and shareholder of HealthTracker. FCV publishes the Dutch translations of ASEBA, from which he receives remuneration.
Ethics approval NRES Committee West Midlands—South Birmingham.
Provenance and peer review Not commissioned; externally peer reviewed.
Collaborators Rebecca Appleton, Jude Taylor (University of Warwick, UK); Alessandro Ferrari, Elisa Gheza, Cecilia Ferrari, Laura Rivolta, Flavia Levi, Maria Cataldo, Lidia Manenti, Giorgia Morini, Adriana Pastore, Cecilia Toselli, Pamela Varvara (Saint John of God Clinical Research Center, Italy); Ilyas Sagar-Ouriaghli, Natalie Heaney, Jatinder Singh (Kings College London, UK); Virginie Maurice, Véronique Humbertclaude (Centre Hospitalier Universitaire de Montpellier, France); Larissa van Bodegom, Mathilde Overbeek (Yulius Academy, Netherlands); Ulrike Schulze, Jörg M Fegert, Melanie Saam, Ulrike Breuninger, Renate Schepker, Michele Noterdaeme (University of Ulm, Germany); Gaëlle Hendrickx (Katholieke Universiteit Leuven, Belgium); Aleksandra Gronostaj (University College Dublin, Republic of Ireland); (University Hospital Split, Croatia); Kate Lievesley, Federico Fiori (HealthTrackerLtd, UK); (Erasmus Medical Centre, Netherlands); Andrea Wohner (concentris research management GmbH, Germany).