Article Text

Abstract
Objective Hospitalisations for ambulatory care-sensitive conditions (ACSCs), a group of chronic and acute illnesses considered not to require inpatient treatment if timely and appropriate ambulatory care is received, and early rehospitalisations are common and costly. We sought to determine whether individuals with depression are at increased risk of hospitalisations for ACSCs, and rehospitalisation for the same or another ACSC, within 30 days.
Design National, population-based cohort study.
Setting Denmark.
Participants 5 049 353 individuals ≥18 years of age between 1 January 2005 and 31 December 2013.
Measurements Depression was ascertained via psychiatrist diagnoses in the Danish Psychiatric Central Register or antidepressant prescription redemption from the Danish National Prescription Registry. Hospitalisations for ACSCs and rehospitalisations within 30 days were identified using the Danish National Patient Register.
Results Overall, individuals with depression were 2.35 times more likely to be hospitalised for an ACSC (95% CI 2.32 to 2.37) versus those without depression after adjusting for age, sex and calendar period, and 1.45 times more likely after adjusting for socioeconomic factors, comorbidities and primary care utilisation (95% CI 1.43 to 1.46). After adjusting for ACSC-predisposing comorbidity, depression was associated with significantly greater risk of hospitalisations for all chronic (eg, angina, diabetes complications, congestive heart failure exacerbation) and acute ACSCs (eg, pneumonia) compared to those without depression. Compared to those without depression, persons with depression were 1.21 times more likely to be rehospitalised within 30 days for the same ACSC (95% CI 1.18 to 1.24) and 1.19 times more likely to be rehospitalised within 30 days for a different ACSC (95% CI 1.15 to 1.23).
Conclusions Individuals with depression are at increased risk of hospitalisations for ACSCs, and once discharged are at elevated risk of rehospitalisations within 30 days for ACSCs.
- PRIMARY CARE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
A strength of our study is that we followed a nationwide, population-based cohort with nearly no loss to follow-up.
Our use of data from a country with a national healthcare system with universal access to healthcare and a relatively homogeneous population may impact generalisability to other countries with more ethnically diverse populations and different healthcare settings.
Although we lack data on potential mediators of an association between depression and ambulatory care-sensitive condition (ACSC)-related hospitalisations such as health-risk behaviours (eg, smoking, sedentary lifestyle), previous studies that controlled for health-risk behaviours found that the association between depression and greater risk for ACSC-related hospitalisations was independent of these factors.
Our data lacks the degree of detail required to determine if adequate treatment for depression could moderate the adverse outcomes seen here.
Introduction
Hospitalisations for chronic illnesses and their sequelae are a major contributor to rising healthcare costs in Western societies.1 In the USA, an estimated 10% of all hospitalisations may be preventable,2 such as those for ambulatory care-sensitive conditions (ACSCs), a set of chronic (eg, diabetes with complications, congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD) exacerbation) and acute illnesses (eg, bacterial pneumonia, urinary tract infection (UTI)) considered not to require inpatient treatment if patients receive timely and appropriate ambulatory care.3 Hospitalisations for ACSCs have been estimated to cost US$31.9 billion and £1.4 billion in the UK annually.4 ,5 Moreover, early rehospitalisations, some of which may be due to ACSCs, are common and costly to health systems.6 With the advent of accountable care organisations in the USA and other efforts to improve healthcare delivery worldwide, health systems are increasingly trying to prevent hospitalisations for ACSCs and early rehospitalisations in an effort to reduce healthcare spending.7–9
Depression is highly prevalent worldwide,10 and is independently associated with more chronic disease sequelae,11 greater healthcare costs12 and increased mortality.13 Importantly, depression is amenable to treatment and could be a potentially modifiable risk factor for ACSC-related hospitalisations. Depression may increase hospitalisations for ACSCs through factors such as reduced adherence to chronic disease treatments and reduced self-care.14 While prior studies have found higher risk of hospitalisations for ACSCs and/or early rehospitalisations among persons with depression, they have been limited to single centre,15 ,16 specific chronic disease populations,17 geographically defined health systems,16 ,17 and older adults.18 Furthermore, previous research on depression and risk of rehospitalisations within 30 days has not focused on potentially preventable rehospitalisations,15 ,16 ,18 ,19 such as rehospitalisations within 30 days for an ACSC, an outcome that is arguably of particular importance to health systems and health policymakers. Also, it remains unknown whether depressed individuals are at greater risk of ACSC-related hospitalisations and rehospitalisations simply because they are more likely to have underlying chronic diseases.20 ,21
Utilising data from a population-based cohort of 5 million Danish adults, we sought to determine if individuals with depression, defined by a clinical diagnosis and/or receiving antidepressant treatment, are at increased risk of hospitalisations for ACSCs after adjusting for demographics, socioeconomic factors, comorbidities (ACSC-predisposing and non-ACSC-predisposing comorbidities), and primary care utilisations. Further, we examined whether persons with depression who have been hospitalised for an ACSC are at greater risk of rehospitalisation for the same, or another ACSC, within 30 days. We hypothesised that depression would be independently associated with increased risk of hospitalisations for ACSCs as well as rehospitalisations within 30 days for either the same or a different ACSC.
Methods
Population
We conducted a population-based cohort study of all adults ≥18 years of age, alive and residing in Denmark at least 1 day between 1 January 2005 and 31 December 2013. The cohort was constructed using data from the Danish Civil Registration System,22 which includes data on sex, date of birth, vital status and emigration since 1 January 1968. In the register, Danish residents are each assigned a unique personal identification number which links to person-level data.22
Primary independent variable
Our primary independent variable of interest was depression as identified by either psychiatric diagnosis or filling at least one antidepressant prescription. Depression was treated as a time-dependent variable (ie, an individual without a recorded depression diagnosis or antidepressant prescription redemption at baseline could be diagnosed with depression or redeem an antidepressant prescription during the follow-up period, moving from the ‘unexposed’ to the ‘exposed’ group). Information on psychiatric diagnoses was obtained from the Danish Psychiatric Central Register23 (see online supplementary appendix 1), which includes diagnostic information on all psychiatric hospitalisations from 1969 onwards and outpatient specialty mental health visits from 1995 onwards.23 Prescription fills for antidepressants (ie, selective serotonin re-uptake inhibitors, monoamine oxidase inhibitors, and other non-tricyclic (TCA) antidepressants, see online supplementary appendix 1) were identified using the Danish National Prescription Registry.24 This register includes data on all prescriptions dispensed at Danish pharmacies since 1995, including purchase date and classification of drugs according to the Anatomical Therapeutic Chemical Classification.25 We excluded TCA prescriptions from our depression definition because of their frequent use for insomnia and/or pain. We also excluded bupropion or trazodone prescriptions since neither was approved for treating depression in Denmark during the study period. Individuals with schizophrenia, schizoaffective disorders or bipolar disorder were censored at date of diagnosis (see online supplementary appendix 2) and excluded from analyses.
Outcomes of interest
Our primary outcome of interest was hospitalisation for 1 of 12 ACSCs as defined by the Agency for Healthcare Research and Quality (AHRQ) (see online supplementary appendix 3).2 Register-based diagnoses were based on the Danish version of the International Classification of Diseases, 8th Revision (ICD-8) prior to 31 December 1993.26 From 1 January 1994 onwards, the Danish version of the ICD-1027 was used. Since the AHRQ-defined ACSCs were originally derived using ICD-9 diagnoses, we included eight AHRQ-defined ACSCs (ie, angina without concomitant cardiovascular procedures, COPD exacerbation, CHF exacerbation, diabetes with short-term complications, diabetes with long-term complications, uncontrolled diabetes, hypertension (HTN) and appendicitis with perforation) that were translated into ICD-10 diagnosis codes and validated in a previous study.28 We also included four AHRQ-defined ACSCs (ie, bacterial pneumonia, diabetes-related lower extremity amputations, UTIs and adult asthma exacerbations) based on ICD-10 codes used in prior Danish register-based studies.29–32 We further divided ACSCs into five ‘chronic’ ACSCs (ie, angina, CHF exacerbation, HTN, diabetes related, COPD/adult asthma exacerbation) and three ‘acute’ ACSCs (ie, appendicitis with perforation, pneumonia and UTI). We used the Danish National Patient Register,33 which contains information on all medical hospitalisations since 1 January 1977 and outpatient visits since 1 January 1995,33 to obtain information on hospitalisations with principal discharge diagnoses for ACSCs occurring between 1 January 2005 and 31 December 2013. If a discharge was followed by an admission within 1 day, it was considered a transfer and counted as one admission only. We excluded hospitalisations with secondary obstetric diagnoses (ICD-10 codes: O00.0-O99.9).
Our secondary outcome of interest was rehospitalisation for an ACSC within 30 days of discharge from the initial ACSC-related hospitalisation. We counted rehospitalisations that were for the same ACSC, or for a different ACSC, using data from the Danish National Patient Register.
Socioeconomic factors, comorbid medical conditions and substance abuse disorders
Information on marital/partnered status and education was obtained from Statistics Denmark and the Danish Educational Registers, respectively (see online supplementary appendix 4).34 ,35 We categorised marital/partnered status as living with a partner (ie, married, registered partnership or cohabitation) or living alone (ie, living without a partner, including widows/widowers). We classified maximum educational level attained into the following three categories based on the United Nations Educational, Scientific and Cultural Organisation's International Standard Classification of Education: low (<10 years), middle (10–15 years) and high (>15 years).36
For the five chronic ACSCs, we defined ACSC-predisposing medical comorbidity specific for each ACSC in question (see online supplementary appendix 5). Information on ACSC-predisposing medical comorbidity and non-ACSC predisposing medical comorbidity was obtained from the Danish National Patient Register and based on Charlson comorbidity index (CCI) categories37 (see online supplementary appendix 6) (eg, myocardial infarction as ACSC-predisposing medical comorbidity for angina hospitalisation, etc), with two exceptions. Diabetes diagnoses were obtained from the Danish National Diabetes Register between 1 January 1990 and 31 December 2013 (see online supplementary appendix 7).38 Chronic pulmonary disease was identified as either a diagnosis based on the CCI category obtained from the Danish National Patient Register or ≥2 prescription redemptions within a 6-month period for medications treating obstructive airway diseases (see online supplementary appendix 8) as obtained from the Danish National Prescription Registry. Non-ACSC predisposing medical comorbidity included all remaining CCI diagnostic categories. We did not define ACSC-predisposing medical comorbidity for the three acute ACSCs.
Data on substance abuse (excluding tobacco abuse) was obtained from the Danish Psychiatric Central Register or the Danish National Patient Register (see online supplementary appendix 9).
Primary care utilisation
We obtained information on daytime face-to-face visits with primary care physicians (PCPs) or other primary care staff from the Danish National Health Service Register,39 which has been collecting primary care administrative data since 1 January 1990. To reduce the chances of including a primary care visit that directly resulted in an ACSC-related hospitalisation, we constructed a time-dependent variable counting the number of primary care visits from 10 to 375 days before any given day. We categorised primary care visits into three equally sized categories of low, medium or high utilisation based on observed frequencies (ie, 0–2, 3–9 or ≥10 visits).
Statistical analysis
We compared individuals with depression to those without depression using Poisson regression models in order to estimate incidence rate ratios (IRRs) of hospitalisations for ACSCs and subsequent rehospitalisation within 30 days for an ACSC. We estimated corresponding 95% CIs using cluster robust variance estimation to account for interperson correlation and dichotomy of rehospitalisation. In these analyses, our outcomes of interest were a count of the number of hospitalisations for ACSCs. Age and calendar period were adjusted for using 2-year and 1-year age and time bands, respectively. All variables (including depression status), except sex, were treated as time-dependent. Individuals contributed at-risk time from 1 January 2005 or from their 18th birthday, whichever came last, in different time bands based on the different covariate combinations they enter with during follow-up. Within each of these combinations, we counted the number of ACSC-related hospitalisations. These methods allowed us to count only ACSC-related hospitalisations that occurred after registration of a depression diagnosis and/or redemption of an antidepressant prescription. Censoring occurred at date of death, emigration, date of bipolar disorder or schizophrenia diagnosis, or on 31 December 2013, whichever came first.
For each ACSC-related hospitalisation outcome, we fitted five risk models, adjusting sequentially for demographics (ie, age, sex and calendar period), socioeconomic factors (ie, marital/partnered status and education), ACSC-predisposing medical comorbidity (with each comorbid condition entered individually), other comorbidities (ie, non-ACSC-predisposing medical comorbidity entered individually and substance abuse) and primary care utilisation. All model covariates were chosen a priori based on prior studies identifying their potential associations with both depression and healthcare utilisation outcomes.12 ,16 ,17 ,40 To address missing data on education, we conducted multiple imputation using five imputed data sets according to methods developed by Rubin.41
We performed two pre-specified subanalyses. First, we examined whether the association between depression and risk of ACSC-related hospitalisations was modified by age. To do so, we repeated our Poisson regressions stratified by three age categories: ≤40, 41–64 and ≥65 years. Second, we examined the associated risk of hospitalisations for chronic and acute ACSCs based on time since depression diagnosis in models adjusted for demographics.
In order to determine if an association between depression and risk of hospitalisations for ACSCs was impacted by our depression definition, we performed a prespecified sensitivity analysis in which we repeated our regressions using three different depression definitions: antidepressant prescription alone, outpatient psychiatric visit-based diagnosis alone or psychiatric hospitalisation for depression.
We fitted three models examining risk of rehospitalisation within 30 days for an ACSC. The first model was adjusted for demographics, the second included adjustment for socioeconomic factors and the third for medical and substance abuse comorbidities. Our outcome of interest in these models was time to rehospitalisation for an ACSC within 30 days of discharge from the initial ACSC-related hospitalisation. Individuals were at risk of the outcome on the day of discharge from their ACSC-related hospitalisation. All variables in these analyses excluding sex were treated as time-dependent.
We used two-sided significance tests for all analyses with statistical significance set at p<0.05. Analyses were performed using STATA V.13 (Stata Corporation, College Station, Texas, USA).
Results
We followed a cohort of 5 049 353 individuals for a total of 38 674 363 person-years at risk, including 1 319 896 (26.1%) persons diagnosed with depression or who had redeemed an antidepressant prescription during the study period. Of those with depression, 1 182 495 (89.6%) cases were from antidepressant prescription fills while 137 401 (10.4%) cases were diagnosed by mental health specialists in outpatient or inpatient contacts. The mean age at initially registered depression diagnosis was 49.1 (SD=19.2) years.
Table 1 displays the characteristics of our cohort by depression status. During the 9-year follow-up period, we identified 1 255 640 hospitalisations for ACSCs, including 542 184 (43.2%) among persons with depression. There were 71.4 ACSC-related hospitalisations per 1000 person-years among those with depression versus 23.0 per 1000 person-years among those without depression during the study period.
Study cohort characteristics
Compared to those without depression, the IRR for individuals with depression having any ACSC-related hospitalisation was 2.35 (95% CI 2.32 to 2.37) after adjusting for demographics. This association remained robust after adjusting for socioeconomic factors, and decreased though remained significant after adjusting for possible mediators including comorbidities and PCP visits during the previous year (table 2).
The risk of hospitalisations for ACSCs associated with depression compared to individuals without depression
In comparison to persons without depression, depression was associated with increased risk of hospitalisations for all of the chronic ACSCs even after adjusting for specific chronic ACSC-predisposing medical comorbidity (table 2), particularly for hospitalisations for angina (IRR=1.77; 95% CI 1.73 to 1.81), COPD/asthma exacerbations (IRR=1.88; 95% CI 1.84 to 1.93) and diabetes-related hospitalisations (IRR=1.83; 95% CI 1.77 to 1.89). Although these results were attenuated by adjusting for additional comorbidity and PCP visits during the previous year, depression remained independently associated with increased risk of hospitalisations for all chronic ACSCs, especially for hospitalisations for COPD/asthma exacerbations (IRR=1.61; 95% CI 1.57 to 1.65), and diabetes-related hospitalisations (IRR=1.69; 95% CI 1.63 to 1.75) (table 2).
Similarly, depression was associated with increased risk of hospitalisations for all three acute ACSCs even after adjusting for medical and substance abuse comorbidities (appendicitis with perforation: IRR+1.26, 95% CI 1.21 to 1.33; pneumonia: IRR+1.55, 95% CI 1.53 to 1.56; UTI: 1.74, 95% CI 1.71 to 1.77). These associations remained significant after adjusting for PCP visits during the preceding year.
When we stratified by age categories, we found that the association between depression and risk of hospitalisations for ACSCs was especially potent for individuals aged 40 years or younger (IRR 2.06; 1.98 to 2.13). Depression was also independently associated with increased risk of hospitalisations for ACSCs among middle-aged and older adults (table 3).
The effect of age on the association of depression with risk of hospitalisation for an ambulatory care-sensitive condition
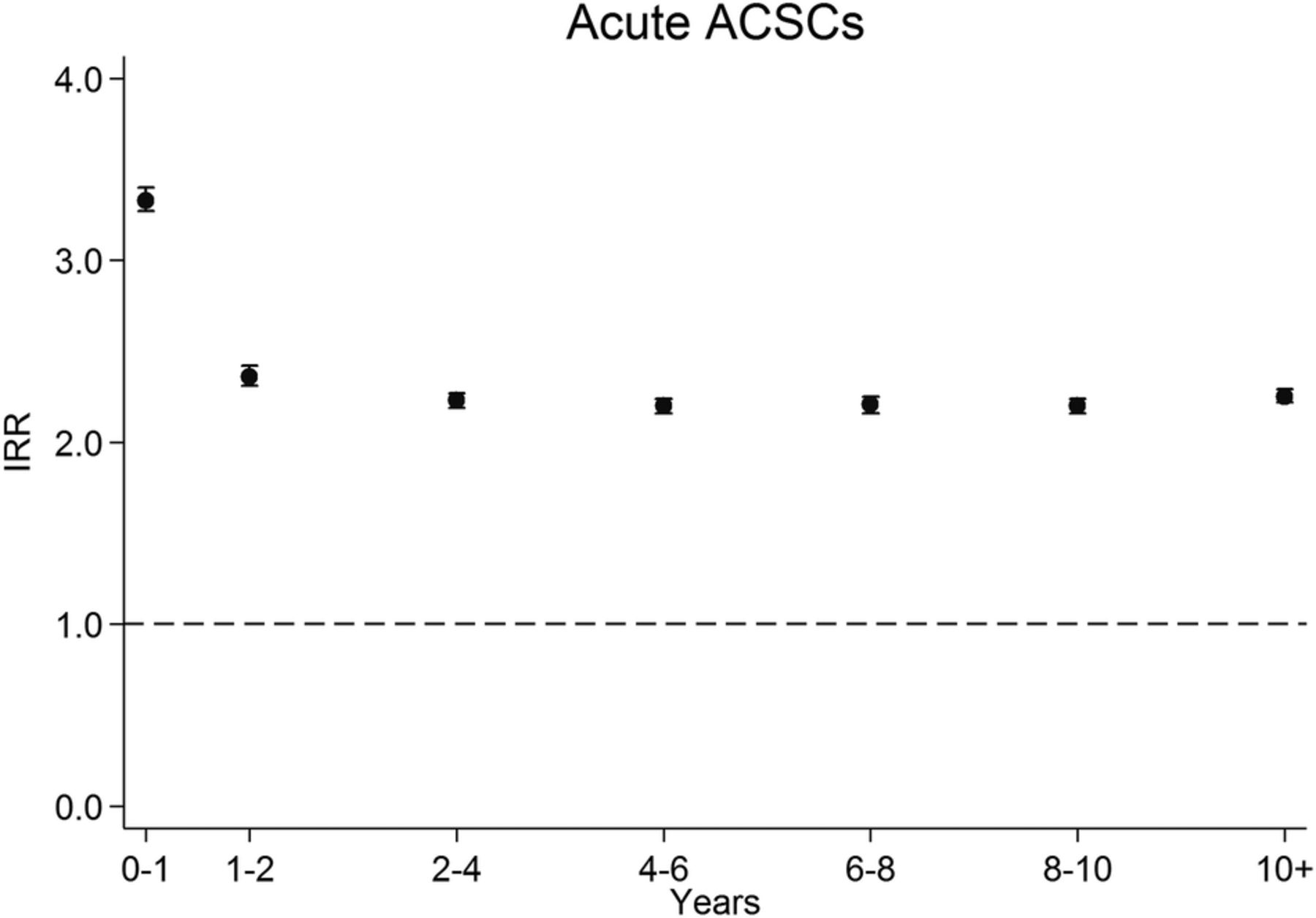
In the first year after depression diagnosis, the associated risk of hospitalisation for a chronic ACSC was nearly three times greater than those without depression (IRR 2.89; 95% CI 2.83 to 2.96) (figure 1). The associated risk remained nearly 2.4 times greater than for those without depression (IRR 2.39, 95% CI 2.34 to 2.43) 10 or more years after depression diagnosis. During the first year after depression diagnosis, the associated risk of hospitalisation for an acute ACSC was 3 1/3 times greater than for those without depression (IRR 3.33, 95% CI 3.27 to 3.40), and the associated risk remained 2¼ times higher at ≥10 years after depression diagnosis (IRR 2.25; 95% CI 2.22 to 2.29) (figure 2).

Risk of hospitalisation for a chronic ACSC by time since (ACSC, ambulatory care-sensitive condition; IRR, incidence rate ratio).
{kind=link}
{kind=link}
Risk of hospitalisation for an ACSC by time since (ACSC, ambulatory care-sensitive condition; IRR, incidence rate ratio).
In our sensitivity analysis in which we examined whether our results regarding risk of hospitalisation for any ACSC were impacted by depression definition, we found that depression defined by antidepressant prescription alone (IRR 2.31; 95% CI 2.28 to 2.33), outpatient psychiatric visit-based diagnosis alone (IRR 2.66; 95% CI 2.56 to 2.77) or psychiatric hospitalisation for depression (IRR 2.69; 95% CI 2.62 to 2.77) were all associated increased risk of hospitalisation for an ACSC after adjusting for demographics. These associations remained significant after adjusting for socioeconomic factors, comorbidities and PCP visits in the previous year (antidepressant prescription alone: IRR 1.44, 95% CI 1.43 to 1.45; outpatient psychiatric visit-based diagnosis: IRR 1.54, 95% CI 1.48 to 1.60; psychiatric hospitalisation for depression: IRR 1.50, 95% CI 1.46 to 1.54).
Approximately 6.8% of all ACSC-related hospitalisations during the follow-up period were followed by an ACSC-related rehospitalisation within 30 days, of which 73% were for the same ACSC and 27% were for a different ACSC. Of the 85 046 ACSC-related rehospitalisations within 30 days, 42 791 (50.3%) were among those with depression. Compared to those without depression, depression was associated with 1.36 times greater risk of rehospitalisation within 30 days for the same ACSC (95% CI 1.32 to 1.39) and 1.44 times greater risk of rehospitalisation within 30 days for a different ACSC (95% CI 1.39 to 1.49) after adjusting for age, sex and calendar period (table 4). After adjusting for socioeconomic factors and comorbidities, while attenuated, depression remained independently associated with greater risk of rehospitalisation within 30 days for the same ACSC (IRR 1.21; 95% CI 1.18 to 1.24) or another ACSC (IRR 1.19; 95% CI 1.15 to 1.23).
The risk of rehospitalisation within 30 days for the same or another ACSC among those with depression compared to individuals without depression
Discussion
In this nationwide, population-based longitudinal study of over 5 million individuals, we found that depression was independently associated with higher risk of hospitalisations for both chronic and acute ACSCs and that the associated risk remained high for at least 10 years. To the best of our knowledge, the present study is the first to show that depression was associated with higher risk of rehospitalisation for the same or another ACSC within 30 days of an ACSC-related hospitalisation. Importantly, we identified that the associated risk of hospitalisations for ACSCs was greater among persons with depression even when we adjusted for the higher prevalence of predisposing chronic diseases in this population.
An increased risk of hospitalisation and subsequent rehospitalisation for an ACSC among depressed individuals is troubling in light of evidence that some ACSC-related hospitalisations may have negative effects on long-term functioning, cognition and mental health.42 Depression in-and-of-itself is known to increase the risk of cognitive decline and functional impairment,43 ,44 both of which increase the risk of ACSC-related hospitalisations.18 ,45 Therefore, depressed individuals could be especially at risk for a vicious cycle of hospitalisations, rehospitalisations and rapid decline.
This study has important implications for development of interventions to prevent costly ACSC-related hospitalisations and rehospitalisations. A potential explanation for our findings is that depressed individuals may not receive timely and/or appropriate ambulatory care for chronic diseases such as diabetes or cardiovascular disease as well as acute diseases such as pneumonia or UTIs. Yet, we found that depression was independently associated with increased risk of hospitalisations for these conditions even in a country, Denmark, with universal access to primary care. Therefore, it could be reasonable to conclude that simply increasing access to primary care may not ameliorate these problems. This interpretation is supported by recent studies evaluating the impact of healthcare reform in Massachusetts that found improving access to care was not associated with reductions in ACSC-related hospitalisations or rehospitalisations within 30 days among high-risk populations.46 ,47
If expanding access to primary care by itself is insufficient to prevent hospitalisations for ACSCs among at-risk populations such as those with depression, then additional research is needed to identify cost-effective interventions that could reduce these potentially preventable events. One possibility is through ongoing efforts to integrate psychiatric care into primary care and other ambulatory care medical settings. Collaborative care for depression and comorbid conditions in primary care settings has been proven effective and cost-effective,48–53 and its cost-effectiveness is in part due to reductions in hospitalisations for comorbid medical conditions.54 Further studies of sufficient duration and size are needed to determine if collaborative care could prevent ACSC-related hospitalisations among individuals with depression. More research is also needed to ascertain if integrating aspects of collaborative care into existing interventions focusing on improving transitional care from the hospital back to primary care55 ,56 could prevent early rehospitalisations for ACSCs. Such research would be of particular interest to accountable care organisations and health policymakers aiming to reduce healthcare costs while simultaneously improving patient outcomes and overall quality of care.
Our study has several strengths and limitations. We followed a nationwide, population-based cohort with nearly no loss to follow-up. However, our use of data from a country with a national healthcare system with universal access to healthcare and a relatively homogeneous population may impact generalisability. Yet, these factors may enhance internal validity by decreasing the degree socioeconomic factors play in healthcare-seeking behaviour, and potentially suggest that our estimates may be overly conservative. Further, our depression definition was based on a combination of psychiatric diagnoses and antidepressant prescription records, potentially introducing selection bias since patients with more severe depression are more likely to be prescribed antidepressants and/or referred to psychiatrists,57 ,58 and is further exacerbated by inability to capture depressed individuals who have not sought treatment.59 However, our sensitivity analysis examining different depression definitions did not yield differing results, and our primary depression definition has been used in prior related research.43
While we lack the data on potential mediators of an association between depression and ACSC-related hospitalisations such as health-risk behaviours (eg, smoking, sedentary lifestyle), previous studies in this area that controlled for health-risk behaviours found that the association between depression and greater risk for ACSC-related hospitalisations was independent of these factors.17 ,18 Our data lacks the degree of detail required to determine if adequate treatment for depression could moderate the adverse outcomes seen here. Also, the registers lack detail to sufficiently ascertain illness severity, so we cannot fully exclude the possibility that our findings reflect when compared to the general population, depressed individuals may present with higher acuity of medical illnesses and a greater burden of comorbidity, necessitating hospitalisation for optimal treatment.
In conclusion, in a nationwide study in Denmark, we found that compared to individuals without depression, depression was associated with increased risk of hospitalisations for ACSCs. Furthermore, once hospitalised for an ACSC, depression was associated with greater risk of rehospitalisation within 30 days for the same, or another, ACSC. Further research that clarifies the mechanisms linking depression and ACSC-related hospitalisations, and that develops interventions that prevent ACSC-related hospitalisations in persons with depression, is needed given the burden that recurrent hospitalisations places on individuals and society.
Acknowledgments
The authors thank the late Wayne Katon, MD (1950–2015), for his support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Funding This work was supported by an unrestricted grant (grant number R155-2012-11 280) from the Lundbeck Foundation.
Competing interests None declared.
Ethics approval The Danish Data Protection Agency and the Danish Health and Medicine Authority.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.