Article Text

Abstract
Introduction There is growing interest in the potential use of autologous fat grafting (AFG) for the purposes of breast reconstruction. However, concerns have been raised regarding the technique's clinical effectiveness, safety and interference with screening mammography. The objective of this systematic review was to determine the oncological, clinical, aesthetic and functional, patient reported, process and radiological outcomes for AFG.
Methods and analysis All original studies, including randomised controlled trials, cohorts studies, case–control studies, case series and case reports involving women undergoing breast reconstruction. All AFG techniques performed for the purposes of reconstruction in the postmastectomy or breast conserving surgery setting will be considered. Outcomes are defined within this protocol along; oncological, clinical, aesthetic and functional, patient reported, process and radiological domains. The search strategy has been devised to find papers about ‘fat grafting and breast reconstruction’ and is outlined within the body of this protocol. The full search strategy is outlined within the body of the protocol. The following electronic databases will be searched from 1 January 1986 to 6 June 2013: PubMed, MEDLINE, EMBASE, SCOPUS, CINAHL, PsycINFO, SciELO, The Cochrane Library, including the Cochrane Database of Systematic Reviews (CDSR), Cochrane Central Register of Controlled Trials (CENTRAL), Database of Abstracts of Reviews of Effect (DARE), the Cochrane Methodology Register, Health Technology Assessment Database, the NHS Economic Evaluation Databases and Cochrane Groups, ClinicalTrials.gov, Current Controlled Trials Database, the World Health Organisation (WHO) International Clinical Trials Registry Platform, UpToDate.com, NHS Evidence and the York Centre for Reviews and Dissemination. Grey literature searches will also be conducted as detailed in our review protocol. Eligibility assessment occurred in two stages, title and abstract screening and then full text assessment. Data were extracted and stored in a database with standardised extraction fields to facilitate easy and consistent data entry.
Ethics and dissemination This systematic review will be published in a peer-reviewed journal. It will also be presented at national and international conferences in the fields of plastic, reconstructive and aesthetic surgery and at more general surgical and methodological conferences. It will be disseminated electronically and in print. Brief reports of the review findings will be disseminated directly to the appropriate audiences of surgeons and societies through email and other modes of communication. Updates of the review will be conducted to inform and guide healthcare practice and policy.
Protocol Registration PROSPERO—National Institute of Health Research (NIHR) Prospective Register of Systematic Reviews (CRD42013005254)
- PLASTIC & RECONSTRUCTIVE SURGERY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Background
Breast cancer and reconstruction
Breast cancer is the most common cancer in the UK and is by far the most common cancer among women, where it accounts for 31% of all new cancer cases with a life-time incidence of 1 in 8.1 Approximately 50 000 women are diagnosed with breast cancer each year, 16 000 of whom undergo mastectomy and there are approximately 12 000 deaths from the disease.2 In the USA, the National Cancer Institute predicts 232 340 new cases and 39 620 deaths from breast cancer in 2013 with over 96 000 undergoing breast reconstruction following surgery.3 Surgical treatment options include mastectomy or breast conserving surgery (BCS), which is either quadrantectomy or lumpectomy plus axillary node dissection if nodal disease exists, often combined with radiotherapy (RT). Veronesi et al4 showed through a seminal randomised controlled trial beginning in 1973, comparing mastectomy with BCS, that long-term survival (after 20-year follow-up) was no different for those with tumours <2 cm in diameter. Hence, BCS has become the treatment of choice for this group.5 ,6
The mix of patients undergoing mastectomy or various forms of BCS leaves the reconstructive surgeon facing a variety of defects in the group of patients wanting reconstruction. There is a need for not just restoring volume but creating an aesthetically pleasing shape and also dealing with the aftermath of RT including pain, retraction, fibrosis, oedema, telangiectasia, atrophy as captured in the Late Effects Normal Tissue/Subjective Objective Management Analytic (LENT/SOMA) system for grading RT side effects.7 Reconstruction of the breast can occur either immediately postmastectomy or in a delayed setting several months or years later. Reconstructive options include implants or with autologous tissue as either a pedicled or free flap containing skin, fat and a variable amount of muscle harvested as a composite block of tissue. Existing reconstructive options are not without morbidity. Mioton et al8 reviewed over 13 000 breast reconstructions in the USA from 2006 to 2010 using the prospective and multicentre American College of Surgeons-National Surgical Quality Improvement Program (ACS-NSQIP) database. Autologous reconstructions (using mostly tissue from the abdomen or back) were performed in 25% of patients and implants were the reconstructive modality in 75%. Autologous reconstruction patients had higher rates of overall complications (12.5% vs 5.4%), wound infection (5.5% vs 3.5%), flap/prosthesis failure (3.1% vs 0.9%) and reoperation (9.6% vs 6.8%). There are of course general complications of major surgery and prolonged length of stay (3–5 days typically) such as deep vein thrombosis, pulmonary embolism, pneumonia and the need for blood transfusions.9
Implant-based reconstructions include complications, such as implant exposure/extrusion, rupture, deformation/distortion, rippling, migration and discontent among patients with implant animation and edge visibility. The placement of the implant itself can lead to reduced or absent sensation at the nipple in one in seven women.10 Furthermore, the body's natural reaction to a foreign body is to form a fibrous capsule around it as part of the healing process. This fibrous capsule shrinks over time (capsular contracture), which can lead to implant prominence, distortion of aesthetics (especially symmetry), increased palpability and pain.10 In its core study presentation to the Federal Drug Administration (FDA), Allergan's 10-year cumulative risk study found that 24.6% of patients who underwent implant-based reconstruction developed capsular contracture necessitating implant removal and/or replacement.11 Implanting foreign bodies to fill space and provide volume and shape is felt to be unnatural by some patients and underscores their refusal to proceed with implant-based reconstruction.12 Such reservations were reinforced during the silicone implant scandal in the 1990s and has not been helped by the more recent poly implant prothese (PIP) implant scandal13 and to a lesser extent the metal on metal hip replacement controversy.14
Another technique that has received much recent focus, is autologous fat grafting (AFG), where the patient's own fat is harvested using a liposuction technique, typically from the abdomen or thighs and then transplanted into the cavity left by removal of the gland postmastectomy or BCS. It holds the potential of reconstruction using nature's choice of filler—body fat, which is easily harvestable, often in good supply, where the donor site defect could be appreciated by patients with minimal scarring, no foreign body reaction and the potential for boosting skin trophicity and rejuvenation by combating the signs and symptoms of RT damage and aging, all performed as a day-case procedure.15 ,16
The history of fat grafting
In 1893, Neuber described the first reported case of autologous fat transfer for the purposes of reconstruction, implanting upper arm fat tissue to correct a depression in the face.17 In 1895, Czerny performed the first breast reconstruction when he transplanted a large lipoma from the dorsal flank to the breast.18 In the 1950s technical problems with harvesting and viability were brought into sharp focus when a study showed minimal graft survival 1 year post-transplantation.19 The corollary was that fat grafting fell out of favour at a time when synthetic implants were on the rise. The technique lay essentially dormant for a while but was revived in the early days of liposuction following Illouz's20 seminal paper describing the ability to remove fat cells from small port incisions using a cannula. Liposuction offered surgeons not just a method of body contouring but access to nature's own choice of filler—body fat through a low morbidity and safe approach that resulted in minimal scarring.
In 1987, Bircoll21 described the first reported case of harvesting fat using a liposuction technique with subsequent placement into the breasts using small syringes. This was performed in 1984 on a 20-year-old Caucasian woman who suffered a dog bite in the right thigh but who also had bilateral breast hypoplasia—with the harvested fat being used to treat both areas.21 Despite significant advances, obtaining consistently good aesthetic and reconstructive results for fat grafting to the breast remained challenging with complications such as cyst formation, fat necrosis and calcification relatively frequent compared with other body areas and volume maintenance being major hurdles.22 ,23 This has been put down to the technique not being well understood at the time with the many technical factors influencing graft take and maintenance not being appreciated.25
Controversy and prohibition of fat grafting
In 1987, following concerns that potential scarring and calcifications could mask the detection of breast cancer and that adipocytes might directly stimulate the formation of cancer, the American Society of Plastic and Reconstructive Surgeons (ASPRS) Ad Hoc Committee on New Procedures prohibited the use of AFG to the female breast through a position statement which stated
The committee is unanimous in deploring the use of autologous fat injection in breast augmentation.25
The advent of structural fat grafting
In the period that followed, Coleman26 developed the concept of structural fat grafting. The principle being that fat must be transplanted in small aliquots using multiple tunnels, in a multilayered and multidirectional way, formed by thin cannulas and syringes. This maximises the number of adipocytes in contact with the host tissue, optimising their chances of receiving sufficient nutrition and immobilisation to survive and become incorporated into the recipient site.27 Any fat that necroses, can cause an inflammatory reaction, with the sequelae of fibrosis and/or cystic formation plus or minus calcification and potential local infection.28 These principles are particularly important in the breast, where unlike the other anatomical areas, fat is being implanted into a loose and poorly vascularised space postmastectomy or BCS.26
A number of studies subsequently showed structural fat grafting to the breast to be efficacious.29––31 In 2009, the American Society of Plastic Surgeons (ASPS) Fat Grafting Task Force announced that fat grafting to the breast is not a strongly recommended procedure, as there is limited scientific data on safety and efficacy.23 They also stated that: “there appears to be no interference with breast cancer detection.”23
Growing knowledge on fat grafting
There has been much focus on how to boost fat graft survival including the development of centrifugation techniques for distilling the fat fraction from the harvested fluid (which will also contain blood residues in the precipitate and an oily supernatant composed of lysed cells and free triglycerides) and the understanding that adipose tissue is an endocrine organ with distinct circadian mechanisms and is rich in mesenchymal stem cells (MSCs).16 ,32 Such adipose-derived stem cells (ADSCs) can differentiate into a range of cells types (eg, chondrocytes, myocytes and osteoblasts) and secrete angiogenic factors such as vascular endothelial growth factor.32 ,33
ADSCs have now become the most studied adult stem cell and are thought to play a key role in the restorative, reconstructive and sustainable qualities of transferred fat.16 ,34––38
Current controversy and concerns
Pearl et al39 have cited concerns with respect to fat grafting into an area of previous malignant change. They highlighted basic science and animal studies which found that engrafted MSCs were less able to regulate growth patterns and how this could potentially lead to breast cancer recurrence.37 ,40 Wang et al41 have emphasised the role that adipose tissue may play in breast cancer progression and metastasis. Recent studies have shown that adipokine signalling may foster cancer initiation and progression with adipose tissue progenitors cooperating in breast cancer angiogenesis, growth and metastatic progression.42 There are also concerns about how AFG may lead to mammographic confusion with 16.7% of patients in one sample showing the subsequent development of clustered microcalcifications.43 The greatest concern thus comes in the use of AFG—which stimulates angiogenesis—to reconstruct what was a tumour bed that is, postmastectomy or BCS.
What have we learnt from prior systematic reviews?
The table below summarises previous systematic reviews assessing AFG to the breast.
The quality of the previous systematic reviews is assessed in table 1 below using the validated assessment tool ‘Assessment of Multiple Systematic Reviews (AMSTAR)’.44–46
Quality of prior systematic review according to AMSTAR
From table 2, it can be noted that two reviews do not state the years searched or only searched a narrow range of databases.23 ,49 All the reviews were restricted to the English language, which creates substantial language bias. All of these reviews suffer from significant heterogeneity across the included studies with cosmetic as well as reconstructive indications among populations with congenital and acquired defects or use of cointerventions such as simultaneous implant or flap-based procedures along with AFG.
Prior reviews of autologous fat grafting (AFG) to the breast
Many of the included studies did not report on patient satisfaction and those that did, did not use a standardised and validated instrument for such measurement. The follow-up periods were also highly variable, so the time point at which outcomes are measured is highly variable.
Why is it important to do this systematic review?
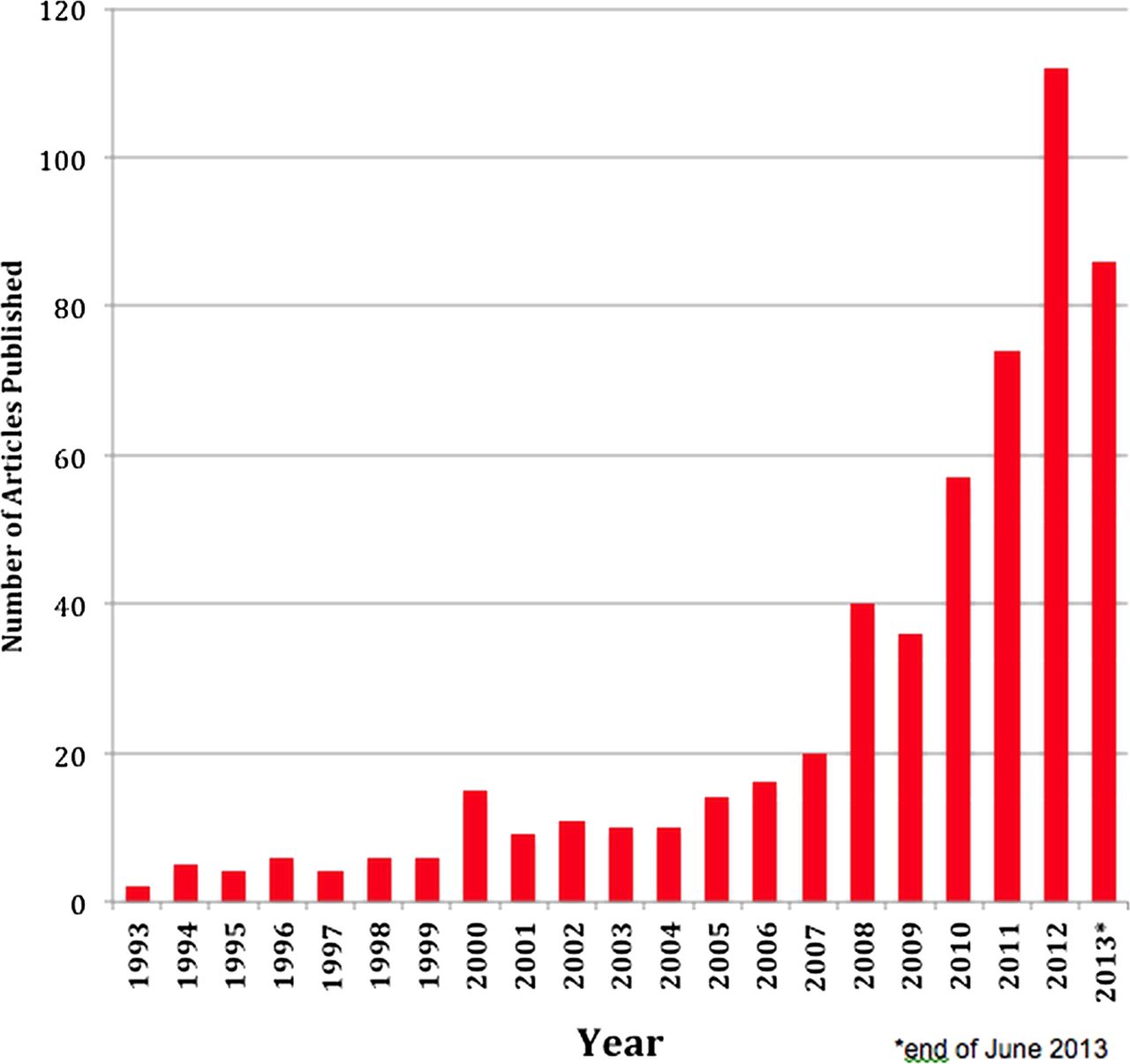
AFG is an active research front. A basic search using the database SCOPUS for ‘fat grafting’ reveals how research and interest in this area has increased in recent years (figure 1).

{kind=link}
Number of articles published per year and indexed by SCOPUS under the search term “fat grafting”.
Since the most recent systematic review looking at the use of AFG in breast reconstruction by Claro et al48 concluded its search in June 2011, there have been approximately 235 more articles published in this area. A new systematic review is needed to update our understanding of this rapidly evolving reconstructive technique and potentially answer the questions previous studies have.
Objectives
Our objective is to perform a comprehensive systematic review of AFG for the purposes of breast reconstruction with a particular focus on safety, efficacy and radiological outcomes.
Primary objectives
In the context of using AFG for breast reconstruction in women postmastectomy or post-BCS, we aim to determine its
-
Oncological outcomes
-
Clinical outcomes
-
Aesthetic and functional outcomes
-
Patient-reported outcomes
-
Process outcomes
-
Radiological outcomes
Secondary objectives
-
To determine optimal methods of fat harvesting, preparation and injection.
-
To determine the indications for the procedure.
-
To help refine patient selection for the procedure.
Methods
This review will be conducted in line with the recommendations specified in the Cochrane Handbook for Intervention Reviews V.5.1.0 and is AMSTAR compliant.50 It will be reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.51 This protocol has been developed a priori and registered on the National Institute of Health Research (NIHR) Prospective Register of Systematic Reviews PROSPERO CRD42013005254.52
Criteria for selecting studies for this review
The following inclusion and exclusion criteria were explicitly formulated to minimise heterogeneity and address the research questions asked.
Types of studies
All original studies, including randomised controlled trials, cohorts studies, case–control studies, case series and case reports. Hence, levels of evidence (LoE) 1–5 (excluding expert opinion) as defined by the Oxford Centre for Evidence-Based Medicine.53 Only articles which mentioned one or more of the outcomes of interest will be included. Unpublished trials and reports would be included if the methodology and data are accessible in written form.
Duplicate studies will be excluded as will; cost-effectiveness studies, those that did not contain an indication for the procedure, where original data is not reported such as review articles, editorials/discussions/commentaries, letters containing only viewpoints or purely technical descriptions.
Types of participants
Participants were women undergoing immediate or delayed breast reconstruction following a mastectomy, a quadrantectomy, wide local excision or a lumpectomy for the treatment of breast cancer. Male and transgender cases will be excluded.
Types of interventions
Autologous fat transfer techniques performed for the purposes of reconstruction following oncological surgery would be considered. We will include total breast reconstruction postmastectomy and BCS using AFG (primary reconstruction) and secondary reconstruction following initial reconstruction with implants or flaps. Studies involving cadaveric grafts or pedicled fat flaps will be excluded. Studies where fat grafting is used as a cointervention or simultaneously in combination with another reconstructive technique (such as implants or flaps) or used as a salvage procedure for failed reconstructions or used purely for nipple reconstruction will be excluded. Studies where fat grafting was used for the purposes of cosmetic breast augmentation or to reconstruct traumatic breast defects (such as breast amputations, ballistic or blast trauma or burns) will be excluded.
Types of comparators
Potential comparators include implant and flap-based reconstructions as well as no reconstruction at all.
Types of outcome measures
The outcomes of interest are defined along six distinct domains
-
Oncological outcomes: Defined as the incidence of new primary of recurrent breast cancer.
-
Clinical outcomes: Defined as the incidence of intraoperative and postoperative complications such as local infection, fat necrosis, oil cysts and palpable nodules. Complications will be graded using the validated Clavien-Dindo classification system, which assesses the therapeutic consequences of complications.54
-
Aesthetic and functional outcomes: Defined as clinician satisfaction with the results (subjective) as measured through questionnaire, visual analogue or other scale or Netscher score55 as well as more objective measures such as changes in LENT-SOMA score.7
-
Patient-reported outcomes: Defined as patient satisfaction with the procedure as measured by questionnaire, visual analogue or other scale or more formal instruments like BREAST-Q.56
-
Process outcomes: This refers to the number of sessions needed to achieve a satisfactory outcome, expressed as a mean together with a range for the group.
-
Radiological outcomes: Incidence of radiological abnormalities, such as calcific deposits, microcalcifications, cysts and other masses that may potentially interfere with mammographic screening.
Search methods for identification of studies
Electronic searches
Electronic databases will be searched from 1 January 1986 to 6 June 2013. The year 1986 was chosen as the start date by a multilingual information specialist with 8 years experience of searching Biomedical, Economic and Sociological databases, conducting approximately 80–100 literature searches per year: PubMed, MEDLINE, EMBASE, SCOPUS, CINAHL, PsycINFO, SciELO, The Cochrane Library including the Cochrane Database of Systematic Reviews (CDSR), Cochrane Central Register of Controlled Trials (CENTRAL), Database of Abstracts of Reviews of Effect (DARE), the Cochrane Methodology Register, Health Technology Assessment Database, the NHS Economic Evaluation Databases and Cochrane Groups, ClinicalTrials.gov, Current Controlled Trials Database, the World Health Organisation (WHO) International Clinical Trials Registry Platform, UpToDate.com, NHS Evidence and the York Centre for Reviews and Dissemination.
Search terms and keywords
The search strategy has been devised to find papers about ‘fat grafting and breast reconstruction’. A search will be conducted using appropriate keywords in the English language combined with Boolean logical operators typically as follows: lipostructuring OR lipotransfer OR lipomodelling OR lipomodeling [Title/Abstract] OR “adipose tissue/transplantation” [MeSH Terms] OR fat OR “autologous fat” OR “adipose tissue” OR “body fat” OR “tissue adipose” OR “fatty tissue” [Title/Abstract] OR “adipose tissue” [MeSH Terms] AND (autograft* OR autotransplant* OR graft* OR transplant OR transplantat* OR injection OR transfer OR lipofilling [Title/Abstract]) AND (mammoplast* OR mammaplast* [Title/Abstract]) OR “mammaplasty” [MeSH Terms]) OR (“breast reconstruction” OR “breast reconstructed” OR “breast augmentation” OR “breast enlargement” OR “breast surgery” [Title/Abstract]), adapted to the appropriate syntax of each database. In all databases free text and the relevant database thesaurus terms will be used. The thesaurus terms will be exploded to capture narrower terms.
Reports will not be excluded based on their publication status. The search will not be limited by language. Where a non-English language article is found, it will proceed to title and abstract screening (since the abstract will be in English). If the full paper is required to determine its eligibility for final inclusion, the authors of the manuscript will be contacted where possible to provide an English language version of their article or language translation will occur through a native speaker. If these options are not possible, Google Translate (Google, Mountain View, California, USA) will be used. Google translate is based on statistical machine translation and according to Google, looks for patterns in hundreds of millions of documents that have already been translated by human translators to determine what an appropriate translation should be.57 It has recently been recognised as an approach to minimise language bias in systematic reviews.58
Searching other resources
Grey literature searches will include conference proceedings from the ACS and ASPS Annual Congresses in 2012 and the European Plastic Surgery Research Council (EPSRC) Annual Meetings of 2012 and 2013 (to capture recent as yet unpublished studies). Other literature to be searched will include the Plastic Surgery textbook Grabb and Smith's Plastic Surgery—6th edition, a core text in the specialty.59 We will attempt to contact researchers who are active in this field for information about further published or unpublished studies. A link to the PROSPERO record for the protocol will also be distributed through Twitter using the lead author's account and a call for unpublished work made. In addition, references for all included papers and prior systematic reviews will be searched for any relevant studies that were not already captured through our search.
Identification and selection of studies
Studies identified through the electronic and manual searches will be listed with citation, titles and abstracts from all databases being populated into a Microsoft Excel 2011 database and duplicates excluded (Microsoft, Redmond, Washington, USA). The eligibility process will be conducted in two distinct stages
-
Titles and abstracts will be screened by two researchers acting independently. A final list will be agreed with discrepancies resolved by consensus. If any doubt about inclusion exists, the article will proceed to the next stage.
-
The full-text version of the articles passing title and abstract screening will be downloaded and further assessed for eligibility by two researchers acting independently. Discrepancies will be resolved by consensus. If this is not possible, one of the senior authors will be asked to make a judgement on the article.
Multiple reports of the same study will be linked together. Where required, correspondence with the relevant investigators would take place to clarify study eligibility and results or if the article was not readily accessible. Once final decisions on study inclusion had been made, the authors will proceed to data extraction.
Data extraction, collection and management
Data extraction will be performed independently by two researchers and then discrepancies will be resolved by consensus. If this is not possible, one of the senior authors will be asked to make a judgement on the data entered.
Extraction of data will occur by developing a database using Microsoft Excel 2011 (Microsoft, Redmond, Washington, USA) with standardised extraction fields where data can be inputted from each study in turn. The following data will be extracted.
-
Author names, countries and year of publication
-
Study design and LoE according to Oxford Centre for Evidence-based Medicine
-
Conflicts of interest and funding
-
Number of participants
-
Number of breasts treated
-
Age of participants expressed as mean or median with a range if provided
-
Previous oncology surgery—mastectomy, quadrantectomy, wide local excision or lumpectomy
-
Prior adjuvant RT
-
Previous breast reconstruction procedure(s)
-
Time interval between oncology surgery and fat grafting
-
Donor site(s) used
-
Technique—recipient site preparation, graft harvest, preparation and injection
-
Mean volume of fat injected per breast
-
Mean follow-up length
-
Loss to follow-up expressed as a percentage
-
Oncological, clinical, aesthetic, functional, patient reported, process and radiological outcomes as defined above
Assessment of study quality and bias in included studies
The extent to which the results from this systematic review can confidently be applied in practice depends in part on the methodological rigour with which contributing studies were conducted. The methodological quality of studies will be assessed using the Grading of Recommendation Assessment, Development and Evaluation (GRADE) system.61 ,62 GRADE offers four LoE quality: high, moderate, low and very low. Randomised trials begin as high-quality evidence, observational studies as low-quality evidence and case series and case reports as very low-quality evidence.
Quality may be downgraded as a result of following five domains
-
Limitations in study design or implementation (high risk of bias)
-
Inconsistency in results
-
Indirectness of evidence
-
Imprecision of estimates (wide CIs)
-
Publication bias
Quality may be upgraded because of three domains
-
A very large magnitude of effect
-
A dose-response gradient
-
All plausible biases would reduce an apparent treatment effect
For randomised controlled trials, we will extract whether clinically relevant outcomes are reported and compare trial protocols with subsequent publications where available. Key missing information across all study types such as complication rates and follow-up times will be documented and assessed.
Strategy for data synthesis and statistical analysis
Outcomes of interest will be tabulated and shown in descriptive or numeric form as appropriate and summarised. Using Review Manager V.5.2.6 (RevMan),62 an assessment of heterogeneity in comparative studies will be made.62 If high, meta-analysis will not be performed. Previous reviews have not conducted meta-analysis.47––49 ,61
Subgroup analysis
We will perform an additional analysis to separate total breast reconstructions using AFG postmastectomy, from its use to correct contour deformities postimplant, flap-based reconstructions or BCS alone.
Dissemination
This systematic review will evaluate the use of AFG for breast reconstruction. Hence it may influence the management of patients with breast cancer postmastectomy or BCS and the reconstructive options offered to them. Based on the results of this systematic review, independent analysis and recommendations will be made to clinicians, researchers, plastic surgical societies and policy makers. Authors of position statements and guidelines relating to AFG will be informed of the results directly. It will be published in the English language in a peer-reviewed journal and the authors will endeavour to respond to any commentary generated. It will also be presented at national and international conferences in the fields of Plastic, Reconstructive and Aesthetic Surgery and at more general surgical and methodological conferences. It will be disseminated electronically and in print to leading researchers in the field. Brief reports of the review findings will be disseminated directly to the appropriate audiences and societies through email and other modes of communication. Updates of the review could be conducted to inform and guide healthcare practice and policy should the need arise.
References
Footnotes
-
Contributors RAA contributed to concept and methods, writing and approving protocol. TG was involved in steerage on methodology, writing input and approving protocol. DPO contributed to concept, steerage on methodology, writing input and approving protocol.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors..
-
Competing interests None.
-
Ethics approval In line with guidance issued jointly by INVOLVE and the National Research Ethics Service (NRES), ethical approval is not needed for systematic reviews, even ones which involve patients and members of the public in a planning and advisory capacity. (INVOLVE. Patient and public involvement in research and research ethics committee review, 2009)
-
Provenance and peer review Not commissioned; externally peer reviewed.