Article Text

Abstract
Introduction Low anterior resection syndrome (LARS) is described as disordered bowel function after rectal resection that leads to a detriment in quality of life, and affects the majority of individuals following restorative proctectomy for rectal cancer. The management of LARS includes personalised troubleshooting and effective self-management behaviours. Thus, affected individuals need to be well informed and appropriately engaged in their own LARS management. This manuscript describes the development of a LARS patient-centred programme (LPCP) and the study protocol for its evaluation in a randomised controlled trial.
Methods and analysis This will be a multicentre, randomised, assessor-blind, parallel-groups, pragmatic trial evaluating the impact of an LPCP, consisting of an informational booklet, patient diaries and nurse support, on patient-reported outcomes after restorative proctectomy for rectal cancer. The informational booklet was developed by a multidisciplinary LARS team, and was vetted in a focus group and semistructured interviews involving patients, caregivers, and healthcare professionals. The primary outcome will be global quality of life (QoL), as measured by the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire—Core 30 (QLQ-C30), at 6 months after surgery. The treatment effect on global QoL will be modelled using generalised estimating equations. Secondary outcomes include symptom change, patient activation, bowel function measures, emotional distress, knowledge about LARS and satisfaction with the LPCP.
Ethics and dissemination The Research Ethics Committee (REC) at the Integrated Health and Social Services Network for West-Central Montreal (health network responsible for the Jewish General Hospital) is the overseeing REC for all Quebec sites. They have granted ethical approval (MP-05-2019-1628) for all Quebec hospitals (Jewish General Hospital, McGill University Health Center, CHU de Quebec) and have granted full authorisation to begin research at the Jewish General Hospital. Patient recruitment will not begin at the other Quebec sites until inter-institutional contracts are finalised and feasibility/authorisation for research is granted by their respective REC. The results of this study will be presented at national and international conferences, and a manuscript with results will be submitted for publication in a high-impact peer-reviewed journal.
Trial registration number NCT03828318; Pre-results.
- colorectal surgery
- gastrointestinal tumours
- epidemiology
- adult gastroenterology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This will be the first randomised controlled trial evaluating a supportive intervention for patients with low anterior resection syndrome (LARS).
This study will collect longitudinal data on patient-reported outcomes following restorative proctectomy, and will report on the natural evolution of several important outcome measures over the first postoperative year.
The informational booklet used in the trial underwent a rigorous pretrial assessment and was revised into its final format based on feedback obtained in focus groups involving patients, caregivers and healthcare professionals.
As with any longitudinal study, there is a risk for attrition throughout the study period, which could be a source of bias in the final results.
Management in the standard care group will vary by institution; however, none of the participating institutions have a formal LARS programme for rectal cancer survivors.
Introduction
Restorative proctectomy is increasingly performed for rectal cancer as surgeons continue to push the limits of sphincter preservation.1 2 However, despite avoiding a permanent ostomy, many individuals are left with significant bowel dysfunction after sphincter-sparing surgery. Low anterior resection syndrome (LARS) encompasses a series of negative bowel symptoms, such as frequency, urgency, incontinence and clustering of bowel movements,3 that can affect 70%–90% of patients following restorative proctectomy.4 5 Although symptoms may improve somewhat in the first 1–2 years after surgery, long-term bowel dysfunction often remains in more than 70% of patients and major dysfunction in over 50%.6–8 As such, LARS remains a significant concern for rectal cancer survivors and their significant others, as increased severity correlates with worse perceived global health status and quality of life (QoL).5 8 9
Currently, there is no well-established treatment strategy for LARS, and management is both empirical and symptom-based.4 LARS is usually managed with a combination of lifestyle, pharmacological, and at times, interventional strategies, with mixed success. Due to the individual nature of each patient’s cluster of symptoms, much of the care requires personalised troubleshooting and self-management behaviours to improve bowel symptoms and QoL.4 These behaviours include understanding one’s own symptoms, knowing how to use and dose stool bulking agents and anti-diarrhoeal medications, performing pelvic floor exercises, adhering to dietary recommendations, proper perianal skin management and preparing ahead of social engagements. Thus, individuals need to be well informed, motivated and engaged in their own LARS management to take better control over their bowel function and achieve optimal outcomes.
Among individuals undergoing rectal resection with a permanent ostomy (eg, abdominoperineal resection), there is evidence that supportive and informational interventions improve QoL, ostomy proficiency, self-efficacy and knowledge.10–12 However, evidence regarding the impact of such interventions in patients who undergo restorative proctectomy is lacking, despite the latter operation being far more frequently performed.1 When provided with the means to better understand and control important aspects of their bowel function, patients may be more likely to experience positive improvements in self-reported outcomes. In a recent review comparing long-term patient-reported outcomes after ostomy or sphincter-sparing surgery for low rectal cancer, the authors concluded that interventions geared towards patients without ostomies warrant further attention.13
This paper describes a study protocol for a randomised controlled trial (RCT) investigating the impact of a LARS patient-centred programme (LPCP) on patient-reported outcomes after restorative proctectomy for rectal cancer. Furthermore, qualitative data are presented that were gathered through a focus group assembling individuals with LARS and their caregivers, and through semistructured interviews with rectal cancer healthcare professionals, as a joint effort to develop the LPCP.
Methods and analysis
Phase 1: study protocol for proposed RCT
The study protocol was written in accordance with the Standard Protocol Items: Recommendations for Interventional Trials statement.14
Objectives
The overall objective of this study is to evaluate the effects of an LPCP on patient-reported outcome measures (PROMs) after restorative proctectomy for rectal cancer. Specifically, our primary objective is to evaluate the extent to which an LPCP improves global QoL, as measured by the European Organisation for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire—Core 30 (QLQ-C30), at 6 months after surgery in comparison to standard care. Secondary objectives include the effects of an LPCP on symptom change, patient activation, bowel function, emotional distress, patient knowledge and satisfaction with LARS care.
Participants and setting
This multicentre RCT involves participants from multiple institutions across North America with high-volume colorectal surgery or surgical oncology practices. Patients who have undergone restorative proctectomy for neoplastic disease (benign or malignant) located in the rectum (0–15 cm from the anal verge) with a diverting ostomy and who are scheduled for ostomy closure are eligible for inclusion. Patients will be recruited approximately 1 month prior to ostomy closure by their individual surgeon, who will go through the informed consent process with them. Exclusion criteria include: (1) active chemotherapy or radiotherapy treatment at the time of consent; (2) major colonic resection in addition to proctectomy; (3) inability to be contacted by telephone; (4) inability to read and comprehend English or French and (5) inability to provide clear and informed consent. The study is estimated to be open from November 2019 to November 2022.
Randomisation
Consecutive participants will be randomised in a 1:1 ratio into one of two groups: (1) LPCP or (2) standard care. Block randomisation with randomly varying block sizes will be performed to ensure an equal number of participants in each group. Randomisation will also be stratified by participating institution. An online centralised computer-generated randomisation sequence will be used to ensure allocation concealment.
LARS patient-centred programme
The LPCP consists of an informational booklet, patient diaries and nursing support made available only to patients randomised to the intervention group.
Informational booklet and patient diaries
The goals of the booklet are to inform individuals with rectal cancer about postoperative bowel dysfunction, manage expectations, and review the different treatment strategies. Prior to developing the booklet, our team conducted a systematic review of online health information for LARS to assess the readability, suitability, quality, accuracy and content of materials currently available to patients.15 We concluded that the current body of health information for patients with LARS is suboptimal. In particular, no patient material was written at the American Medical Association-recommended sixth grade reading level, there was little use of headings, summaries and illustrations to accompany the text, and important content was missing. We then set out to develop our own informational booklet, drawing on the important elements emphasised in each assessment tool used in the systematic review. After developing the first draft of the booklet, patients, caregivers and healthcare professionals provided feedback to improve the booklet into its current format. The booklet was then translated into French and underwent a similar evaluation process. A more thorough description of the booklet’s development process can be found below (see the Phase 2 section).
The booklet will be introduced to patients at the time of study recruitment (before ostomy closure). Participants will be instructed to read through the booklet at least once prior to their ostomy closure operation and will be encouraged to consult it as much as needed thereafter. In addition to the informational booklet, participants will receive bowel symptom, diet and loperamide diaries and will be instructed to use them whenever experiencing any symptoms of bowel dysfunction, and for 2 weeks prior to each scheduled nurse phone call (see the Nursing support section). The goal of these diaries is to assist participants in recognising the underlying patterns related to their symptoms so that they can optimise their self-management.
Nursing support
Nursing support will be centralised from one institution and made available to participants in the intervention group, by telephone and email. The study nurse (bilingual in English and French) has expertise in rectal cancer management and postoperative bowel dysfunction. She will briefly review the booklet content with participants by telephone at the beginning of the study (prior to ostomy closure) and answer related questions. Postoperatively, the nurse will have scheduled telephone calls with participants at 1 month, 3 months, 6 months, 9 months and 12 months, to provide support and periodically review their completed diaries for troubleshooting. Lastly, she will be available to speak with participants in between scheduled calls, either by phone or by email.
Standard care group
Participants randomised to the standard care group will not have access to either the informational booklet nor nursing support. Instead, they will only receive a paper copy (and/or instructions for online access) of the Colorectal Cancer Association of Canada module on ‘Living with Colorectal Cancer’. The standard care group will also receive the usual care for LARS information and counselling that is routinely made available at their hospital, with participating hospitals asked to provide a description of what constitutes ‘standard care’ for LARS. Due to the expected heterogeneity in institutional LARS practices, participating institutions will be accounted for in the final statistical model in addition to stratified randomisation by institution. Participants in the standard care group will be told that they can have access to the informational booklet when the study is complete.
Data collection
Baseline demographics, medical comorbidities and disease and treatment characteristics will be obtained from chart review, including known predictors of bowel dysfunction (eg, tumour height, neoadjuvant radiotherapy, type of proctectomy (total vs partial mesorectal excision), reconstruction technique (straight anastomosis vs neorectal reservoir) and anastomotic leak after proctectomy). The remaining data will be gathered from self-reported questionnaires at study time-points throughout the 12-month study period.
Outcomes
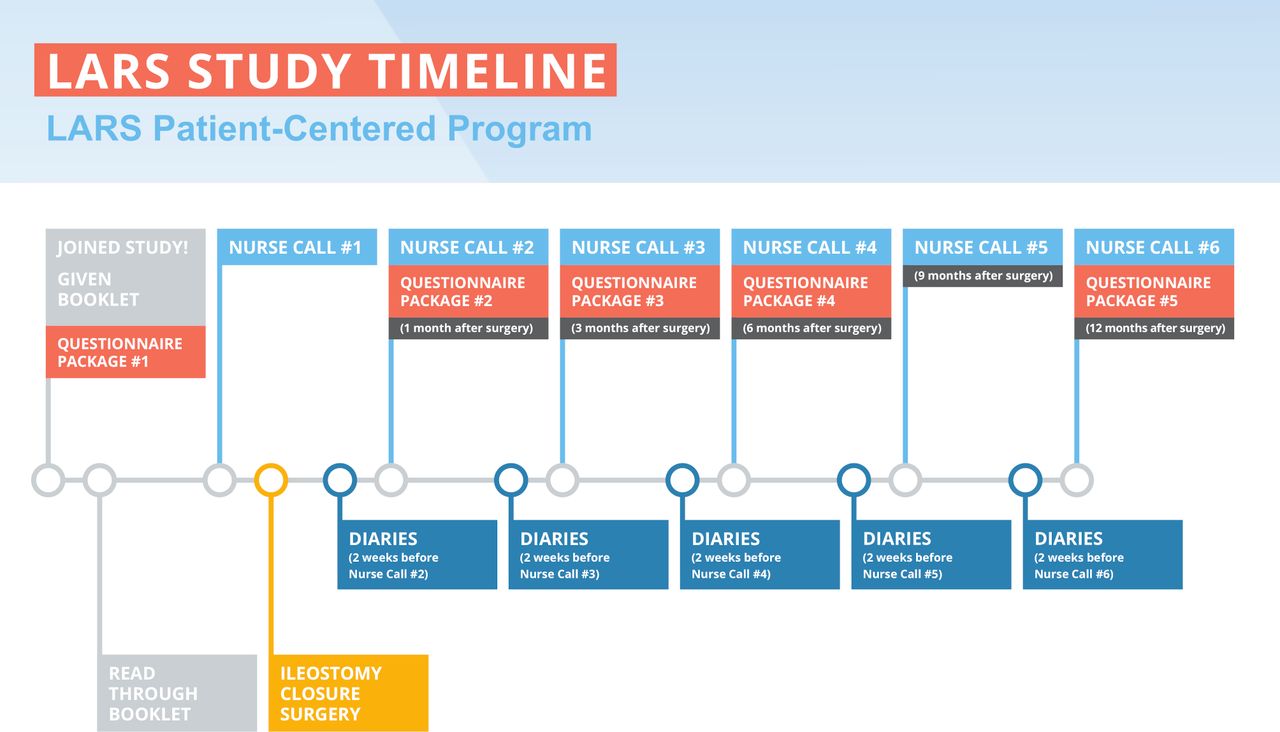
Outcomes will be measured with the use of various PROMs and recorded into an online registry (REDCap 9.1.9 - (c) 2020 Vanderbilt University) by a blinded assessor. PROMs captured at the same time-point will be completed as a single package. The schedule for all PROMs can be found in table 1. The PROM package for each time-point (available in both English and French) will either be mailed to participants, disseminated via email or completed over the phone, depending on participants’ preferences. Participants will receive email and telephone reminders for incomplete questionnaires. The study timeline for both groups can be found in figures 1 and 2. The following outcomes and PROMs will be collected:

Study timeline for patients in the LARS patient-centred programme. LARS, low anterior resection syndrome.

{kind=link}
{kind=link}
Study timeline for patients in the standard care group. LARS, low anterior resection syndrome.
Schedule of patient-reported outcome measures
Quality of life
QoL will be measured using the EORTC-QLQ-C30, a self-reported questionnaire developed to assess QoL for patients living with or beyond cancer. It consists of 30 items, which aggregate into 1 global QoL scale, 5 functional scales, 3 symptom scales and 6 single items. The EORTC-QLQ-C30 has been well validated in individuals with rectal cancer and correlates significantly with LARS severity.5 8 9
Symptom changes
The Measure Your Medical Outcome Profile (MYMOP2) is a patient-centred measure that assesses changes over time in a specific symptom identified as most bothersome to the patient.16 17 The patient also identifies a daily activity that is being restricted or prevented by the symptom. Both the symptom and the activity are scored using a 6-point Likert-type scale in the last week.
Patient activation
Patient activation measures the degree of knowledge, skills and confidence for self-management of healthcare.18 In patients with chronic medical conditions, patient activation is associated with increased adherence to medication and decreased healthcare resource utilisation.19 We believe that the LPCP may increase patient activation, which may ultimately translate into increased patient engagement in their LARS healthcare.
The Patient Activation Measure-13 (PAM-13) is a 13-item questionnaire. Responses are based on a Likert scale ranging from ‘disagree strongly’ to ‘agree strongly,’ and the final score is a transformation ranging from 0 to 100 according to a conversion formula provided by the developers. Activation is then categorised into 1 of 4 groups based on their transformed score: level 1, ‘overwhelmed and not ready to take an active role’ (≤47.0); level 2, ‘realise they have a role to play, but lack the knowledge and confidence’ (47.1–55.1); level 3, ‘beginning to take action, but still lack confidence’ (55.2–72.4) and level 4, ‘can manage their healthcare, but may struggle to maintain the behaviours’ (≥72.5).
Bowel function
Bowel function will be measured postoperatively using three validated tools/questions. The LARS Score is a five-item tool aimed at symptoms of bowel dysfunction, with each question weighted differently according to the perceived importance by patients. The scores of the five questions sum to 42 points. The LARS Score allows the categorization of patients as having major (30–42 points), minor (21–29 points) or no LARS (0–20 points). The Cleveland Clinic Florida/Wexner Faecal Incontinence Score (WFIS) is a five-item tool aimed at measuring the frequency of incontinence to gas and liquid or solid stools, and its consequences (pad wearing and lifestyle alterations). Each question ranges from 0 (never) to 4 (always) and the total score is measured out of 20. Lastly, each participant will be asked a single, validated, bowel-related QoL question: ‘Overall, how much does your bowel function affect your quality of life?’ Responses categorise respondents into 1 of 3 grades: ‘not at all’ (no impairment); ‘very little’ (minor impairment); ‘somewhat’ or ‘a lot’ (major impairment). Bowel-related QoL is significantly correlated with both the LARS Score and general QoL as per previous studies.9
Emotional distress
Many patients with LARS describe emotional distress, anxiety and isolation (see the Phase 2 section). The LPCP is designed to alleviate some of the distress associated with LARS, and may provide hope that symptoms can be optimally managed.
Emotional distress will be measured using the Hospital Anxiety and Depression Scale, which has been validated in colorectal cancer survivors.20 21 It includes seven items aimed at assessing depression and seven items for anxiety. Each item is scored 0–3, and is based on frequency of symptoms. The total score is out of 21, and individuals can be categorised as ‘normal’ (0–7), ‘borderline abnormal’ (8-10), or ‘abnormal’; that is, depressed or anxious (11–21).
Knowledge
Given that the LPCP is partly an informational intervention, knowledge related to LARS will be measured using a short, investigator-generated multiple-choice questionnaire. The items reflect key concepts in aetiology/risk factors and management of LARS. We believe that improving LARS knowledge will further improve patient activation and engagement in LARS healthcare, which may lead to improvements in QoL and possibly bowel function.
Satisfaction
Satisfaction related to LARS care received throughout the study period (information and support) will be assessed in both groups using a short, investigator-generated, 2-item questionnaire. Responses will be recorded using a 5-point Likert scale, ranging from ‘not satisfied’ (1) to ‘very satisfied’ (5).
Statistical analysis
Descriptive analyses will include means with SD, medians with ranges or frequencies with proportions, where appropriate. Continuous outcomes will be compared using a t-test or Wilcoxon rank-sum test and categorical outcomes using χ2 tests. The treatment effect on global QoL and bowel function will be modelled using generalised estimating equations (GEEs).22 This method accounts for (1) the within-subject correlation between responses at different time-points and (2) possible clustering of responses among patients from the same hospital. GEE models also make use of all the available data, so that patients can contribute to the model if they have data available for any single time-point. An appropriate correlation structure will be chosen using the quasi-likelihood information criterion. The effect size, SE and 95% CI for the estimate of the treatment effect at 6 months will be reported. For the remaining secondary outcomes, pairwise comparisons will be performed at various time-points.
Power analysis and sample size calculations
The primary outcome of the study is global QoL at 6 months, as measured by the EORTC QLQ-C30. Based on the largest available cohort of patients with QoL data who have undergone restorative proctectomy for rectal cancer and who are ostomy-free, mean global QoL score is assumed to be 77 (maximum possible score is 100) with an SD of 19.9 According to the consensus guidelines on the use of the EORTC QLQ-C30 to power an RCT, a mean difference in global QoL of 10 points (small-medium treatment effect) is the most appropriate expected effect-size for interventions aimed to improve QoL in cancer patients.23 Thus, with an α=0.05 and power=0.80, we estimate that 45 participants are required in each arm of our study. Given the risk for attrition over the 6 month study period, the adjusted final sample size accounting for a 30% attrition rate is 64 participants in each arm (128 patients in total).
Phase 2: development of informational booklet
The first draft of the informational booklet was developed by a multidisciplinary team of healthcare professionals who care for patients with rectal cancer. The initiative was co-led by a general surgery resident (RG) and a colorectal surgery attending (MB), and included a senior colorectal cancer oncology pivot nurse, pelvic physiotherapist and members of the McGill University Patient Education Office. The booklet was designed to review important information regarding the epidemiology, symptomatology and management of LARS. The booklet was written at a sixth-grade reading level, which is recommended by the American Medical Association for any patient material,24 and included original illustrations designed by our team.
An Institutional Review Board-approved qualitative study was subsequently undertaken to evaluate the booklet. A single focus group with rectal cancer patients and their caregivers, as well as individual semi-structured telephone interviews with healthcare professionals, were conducted.
Participants for the focus group were recruited from individual colorectal surgeons practicing at a single institution. The focus group included 12 participants (6 patients and their caregivers/partners) and followed a semi-structured interview guide (online supplementary file 1). Each patient was a minimum of 6 months removed from ileostomy closure (if diverted) or proctectomy. Participants’ characteristics are reported in table 2. Each participant/caregiver was given two copies of the informational booklet and allowed 3 weeks to review the booklet and generate their own thoughts. The purpose of the focus group was to obtain feedback regarding the first draft of the booklet, to better understand participants’ current/past experiences with LARS, and to incorporate changes into the booklet to better meet the informational needs of rectal cancer survivors. The focus group was audio-recorded and transcribed, and data were analysed using the grounded theory.25 26 The constant comparative method was applied; data from participants were coded based on emerging patterns, concepts and themes to generate theory, which was then analysed and categorised accordingly so that descriptive statements could be formed.27 The principal findings from the thematic analysis of the focus group are displayed in table 3. Patients and their caregivers described the emotional difficulties of living with LARS and the general lack of support and preparation they received from their healthcare team. They unanimously supported the development and dissemination of the booklet, reporting that it would have had a major impact on their outlook and knowledge regarding LARS in their first year after surgery. Some of the feedback included more emphasis to be placed on expectation management and emotional support, and they asked for more detail regarding enema use. They also requested a list of healthcare providers who could support them in their LARS care, and more examples for foods which may activate their LARS.
Supplemental material
Characteristics of patient participants in focus group (caregivers not included)
Principal findings from thematic analysis of focus group with patients and caregivers
Healthcare professionals from multiple institutions across North America were invited to review the booklet as well. In total, 10 healthcare professionals comprised of seven colorectal surgeons and three nurses in gastrointestinal oncology, and each was interviewed using a semi-structured interview guide (online supplementary file 2). Characteristics of the healthcare professionals are reported in table 4. Similar to patient participants, each healthcare professional was given one copy of the informational booklet and allowed 3 weeks to review the booklet and generate their own thoughts. The focus of these interviews was largely on content and management strategies; to ensure that our booklet would be as comprehensive and inclusive as possible. Furthermore, healthcare professionals were asked about the layout and structure, clinical applicability and other means of improving the booklet. Similar to the focus group, the interviews were recorded, and the same methods were used for data analysis. The principal findings from the interviews are displayed in table 5. Healthcare professionals felt that the booklet was accurate and comprehensive, and that it would complement the role of a clinician/nurse in supporting patients with LARS. Several interviewees recommended additional medications and illustrations, but did not feel the layout or structure needed to be further revised. Small changes in language were recommended as well (eg, ‘stoma’ instead of ‘bag’—most healthcare professionals felt that patients understand the meaning of stoma).
Supplemental material
Characteristics of Interviewed healthcare professionals
Principal findings from thematic analysis of semi-structured interviews with healthcare professionals
Based on the results of this qualitative study, the informational booklet was modified into its final format. The booklet was then professionally translated into French language, and underwent a similar evaluation process with French-speaking patient volunteers.
Patient and public involvement
Patients were involved in the development of the informational booklet to be used as part of the LPCP. Patients and the public were not involved in the design of the study; however, the outcomes proposed in this study are specifically designed to assess participants’ experience with LARS and the LPCP. The authors would also like to thank Dr’s Steven D. Wexner, Patricia Sylla, Mitchell Bernstein, as well as Holly Bonnette and Tracy Chornopyski, for their contributions.
Ethics and dissemination
The Research Ethics Committee (REC) at the Integrated Health and Social Services Network for West-Central Montreal (health network responsible for the Jewish General Hospital) is the overseeing REC for all Quebec sites. They have granted ethical approval (MP-05-2019-1628) for all Quebec hospitals (Jewish General Hospital, McGill University Health Center, CHU de Quebec) and have granted full authorisation to begin research at the Jewish General Hospital. Patient recruitment will not begin at the other Quebec sites until inter-institutional contracts are finalised and feasibility/authorisation for research is granted by their respective REC. The English-language patient consent is presented as online supplementary file 3.
Supplemental material
The results of this study will be presented at national and international meetings, and a manuscript will be submitted for publication in a high-impact peer-reviewed journal. We anticipate that the findings will inform the development of future rectal cancer survivorship programmes with a focus on bowel dysfunction, in an effort to improve the long-term QoL of individuals with rectal cancer.
References
Footnotes
Contributors All authors contributed to the design of the study. RG, CGL, JP, LGB, ASL, NM, JF, GG, C-AV and MB participated in qualitative data acquisition. RG, CGL, JFFJ, SRB, and MB contributed to the data analysis plan. RG, JP, LGB, ASL, NM, JF, GG, C-AV and MB were involved in obtaining ethical approval. RG and MB prepared the first draft of the manuscript. All authors contributed to, and approved, the final version of the manuscript.
Funding This work is supported by a McGill University Rossy Cancer Network Cancer Quality and Innovation research grant and a Canadian Society of Colon and Rectal Surgeons research grant.
Competing interests ASL receives travel stipends from Merck and Servier, and is on the advisory committee of Novadaq. JFFJ received a research grant from Merck and fees for consulting from Shionogi.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.