Article Text

Abstract
Objective To investigate the association between ambient air pollution and stroke morbidity in different subgroups and seasons.
Methods We performed a time-series analysis based on generalised linear models to study the short-term exposure–response relationships between air pollution and stroke hospitalisations, and conducted subgroup analyses to identify possible sensitive populations.
Results For every 10 µg/m3 increase in the concentration of air pollutants, across lag 0–3 days, the relative risk of stroke hospitalisation was 1.029 (95% CI 1.013 to 1.045) for PM2.5, 1.054 (95% CI 1.031 to 1.077) for NO2 and 1.012 (95% CI 1.002 to 1.022) for O3. Subgroup analyses showed that statistically significant associations were found in both men and women, middle-aged and older populations, and both cerebral infarction and intracerebral haemorrhage. The seasonal analyses showed that statistically significant associations were found only in the winter.
Conclusions Our study indicates that short-term exposure to PM2.5, NO2 and O3 may induce stroke morbidity, and the government should take actions to mitigate air pollution and protect sensitive populations.
- epidemiology
- public health
- stroke medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study investigated the association between air pollution and subtypes of stroke morbidity.
This study included more than 67 000 cases, ensuring high statistical power.
The modification effects of different demographic characteristics and seasons were explored.
Being a single-city study limited the generalisation of the findings.
Associations between air pollution and stroke hospitalisations did not prove causality.
Introduction
Stroke is one of the leading causes of disability-adjusted life years (DALYs) and mortality, accounting for approximately 132 million DALYs and 6.2 million deaths globally in 2017.1 2 It is also the leading cause of long-term adult disability and the leading cause of death in China; 20.19% of total deaths were caused by stroke in 2017,3 4 and the age-standardised incidence and mortality rates were 246.8 and 114.8 per 100 000 person-years, respectively.5 Well-known risk factors of stroke include history of hypertension, current smoking status and alcohol intake.6
With the deterioration of global air quality, concerns have been raised about the relationship between ambient air pollution and stroke. According to the Global Burden of Disease, approximately 12.75% of stroke cases in China in 2017 were linked to air pollution.3 Possible mechanisms linking ambient air pollution to stroke include inflammation, oxidative stress, atherosclerosis and autonomic dysregulation.7 To date, most of the relevant epidemiological studies have focused on stroke mortality instead of morbidity,8 9 but it should be noted that morbidity is more indicative of the early stages of stroke; early prevention of stroke has an important public health significance. Studies that examined the relationship between ambient air pollution and stroke morbidity obtained inconsistent results, and most of them studied the association over a full year but failed to consider the seasonal differences in pollutant concentration and their health effects.10–12
In this study, a time-series analysis was conducted to investigate the association between ambient air pollution and stroke morbidity in different seasons; we also researched possible sensitive populations by conducting subgroup analyses by sex, age group, education level and stroke subtypes.
Materials and methods
Study area
Shenzhen is located within the Pearl River Delta, China, is 1 degree south of the Tropic of Cancer and has a permanent population of approximately 12.5 million people.13 Because of the Siberian anticyclone, it has a warm and humid subtropical climate. Six kinds of air pollutants, including ozone (O3), fine particulate matter (PM2.5), nitrogen dioxide (NO2), inhalable particulate matter (PM10), sulfur dioxide (SO2) and carbon monoxide, are monitored in Shenzhen, and the main ambient air pollutants are O3, PM2.5 and NO2.
Data collection
Stroke data containing 67 078 cases from 1 January 2014 to 31 December 2016 were collected from the Shenzhen Centre for Chronic Disease Control. Sixty-nine hospitals from 10 administrative districts reported their stroke case information (including patient age and sex, clinical diagnosis and classification, onset date, diagnosis date and major risk factors) to the Shenzhen Centre for Chronic Disease Control. All the cases were coded according to the WHO's International Classification of Diseases, 10th Revision, ranging from I60 to I64: (1) subarachnoid haemorrhage, which was coded as I60; (2) intracerebral haemorrhage (ICH), which was coded as I61; (3) other non-traumatic intracranial haemorrhage, which was coded as I62; (4) cerebral infarction (CBI), which was coded as I63; and (5) stroke not specified as haemorrhage or infarction, which was coded as I64. All cases were diagnosed in the hospital with CT, MRI or neurological examination. In the subgroup analysis for stroke subtypes, we focused on ICH and CBI, which accounted for 94.8% of all stroke cases.
Hourly concentrations of O3, PM2.5 and NO2 were obtained from the National Urban Air Quality Real-time Publishing Platform (http://106.37.208.233:20035/). The daily mean concentrations for each air pollutant were averaged from all the 11 fixed-site air pollution monitoring stations in Shenzhen.14 Daily meteorological data were obtained from the National Meteorological Data Sharing Platform (http://data.cma.cn/), including the daily mean, maximum and minimum temperatures, the mean relative humidity, the mean wind speed and the mean atmospheric pressure.
Statistical modelling
This time-series analysis adopted generalised linear Poisson models to estimate the association between air pollutants and stroke hospitalisations.15 The daily mean concentrations of air pollutant (PM2.5, NO2 or O3) were the independent variables, and the number of daily hospital admissions for stroke was the dependent variable. Meteorological variables (ie, temperature, relative humidity and air pressure), long-term trends and seasonal patterns, as well as day of the week, were used as adjustment variables. The influence of other pollutants was examined in two-pollutant models.
Considering the possible delayed and/or cumulative effects of air pollution on stroke morbidity, we created cross-basis matrix for air pollutants, within the framework of distributed lag linear model.16 The selection of lag days was justified by the polynomial lag models.
The model to represent the relationship between the daily mean concentration of air pollutants and hospital admissions for stroke is as follows:

Here,  indicates the expected number of hospital admissions for stroke on day t;
indicates the expected number of hospital admissions for stroke on day t;  is the cross-basis matrix of the air pollutants (PM2.5, NO2 or O3), with β as the corresponding vector of coefficients; and
is the cross-basis matrix of the air pollutants (PM2.5, NO2 or O3), with β as the corresponding vector of coefficients; and  is the natural cubic spline function.
is the natural cubic spline function.  is a dummy variable for the day of week. We used 7 df per year for the time trend (
is a dummy variable for the day of week. We used 7 df per year for the time trend ( ), 3 df for the previous 14 days' moving average temperature (
), 3 df for the previous 14 days' moving average temperature ( )17 18 and 3 df for both the relative humidity (
)17 18 and 3 df for both the relative humidity ( ) and the air pressure (
) and the air pressure ( ) on day t; the choice of df for each variable was based on the Akaike Information Criterion for quasi-Poisson models.
) on day t; the choice of df for each variable was based on the Akaike Information Criterion for quasi-Poisson models.
Subgroup analyses were conducted for different sexes, age groups (<40, 40–64 and ≥65 years), education levels (primary school or below, junior high school, high school or above) and stroke subtypes (CBI and ICH). When comparing seasonal differences, we defined spring as the period from 1 March to 31 May, summer as the period from 1 June to 31 August, autumn as the period from 1 September to 30 November and winter as the period from 1 December to 28 February of the next year. The differences among the effect estimates between different subgroups were tested via the Z-test.19 Sensitivity analyses were performed by adjusting the df values of  and
and  , as well as the number of lags considered for the air pollutant. All results were reported as relative risks (RRs) and 95% CIs of hospital admissions for stroke for every 10 µg/m3 increase in air pollutant exposure, and two-tailed p<0.05 was considered statistically significant. Main analyses were performed using the ‘dlnm’ and ‘splines’ packages in R V.3.5.1.
, as well as the number of lags considered for the air pollutant. All results were reported as relative risks (RRs) and 95% CIs of hospital admissions for stroke for every 10 µg/m3 increase in air pollutant exposure, and two-tailed p<0.05 was considered statistically significant. Main analyses were performed using the ‘dlnm’ and ‘splines’ packages in R V.3.5.1.
Patient and public involvement
This study belongs to ecological research and does not reveal any personal information; patients or the public were not involved in the design, conduct, reporting or dissemination of our research. Therefore, patients did not have to be asked for informed consent.
Results
Data description
In total, during 2014–2016, 67 078 hospital admissions for stroke were recorded, of which 77.8% were first-time cases, and 61.9% were men. Patients aged 40–64 years accounted for 49.3% of the total, and 44.7% were older (age ≥65 years old). In total, 27.7% of the cases had an education level of primary school or below; 39.8% completed junior high school; and 32.5% had a high school education or higher. Among the subtypes of stroke, CBI and ICH accounted for 52 168 (77.8%) and 11 415 (17.0%), respectively. The other three subtypes accounted for approximately 5% of the total (table 1).
Summary statistics of stroke hospitalisations in Shenzhen
On average, there were approximately 61 hospital admissions for stroke per day during our study period, and the 24 hours mean concentrations of PM2.5, NO2 and O3 were 30.1, 33.2 and 56.9 µg/m3, respectively. The daily mean temperature was 23.5°C; the mean relative humidity was 74.7%; and the daily mean air pressure was 1005.7 hPa (table 2). In general, the pollutant concentrations of PM2.5 and NO2 were higher in winter than in other seasons (online supplementary table S1). Correlations between air pollutants and meteorological factors are in table 3.
Supplemental material
Distribution of daily air pollution concentrations, meteorological factors and stroke hospitalisations in Shenzhen
Spearman’s rank coefficients between daily mean air pollutants and meteorological variables
Regression analysis
When the lag length was set as 7 days, the results showed that the lag effect mainly lasted for 3 days (online supplementary figure S1). Therefore, we used 3 days as the lag length in later analyses. Positive associations and lag effects were observed between stroke morbidity and air pollution. The cumulative effect of a 10 µg/m3 increase in PM2.5 concentrations across lag 0–3 days corresponded to a 2.9% (95% CI 1.3% to 4.5%) increase in daily stroke hospitalisations; it was a 5.4% (95% CI 3.1% to 7.7%) increase in the case of NO2, and a 1.2% (95% CI 0.2% to 2.2%) increase for O3.
Table 4 showed that, for PM2.5, an association was found in both men and women, populations older than 40 years old and people with education levels of junior high school and above, and the CBI stroke subtype. For NO2, the association was consistently significant in both men and women, populations in all age groups and all education levels, and subtypes CBI and ICH. For O3, the association was significant in women, the middle-aged population, populations with an education level of junior high school and the CBI stroke subtype. The associations occurred mainly in the winter. Comparing the effect estimates between different subgroups, we found none of the differences to be statistically significant.
RRs (95% CI) of stroke hospitalisations for every 10 µg/m3 increase in ambient PM2.5, NO2 and O3 in the single-pollutant model, across lag 0–3 days
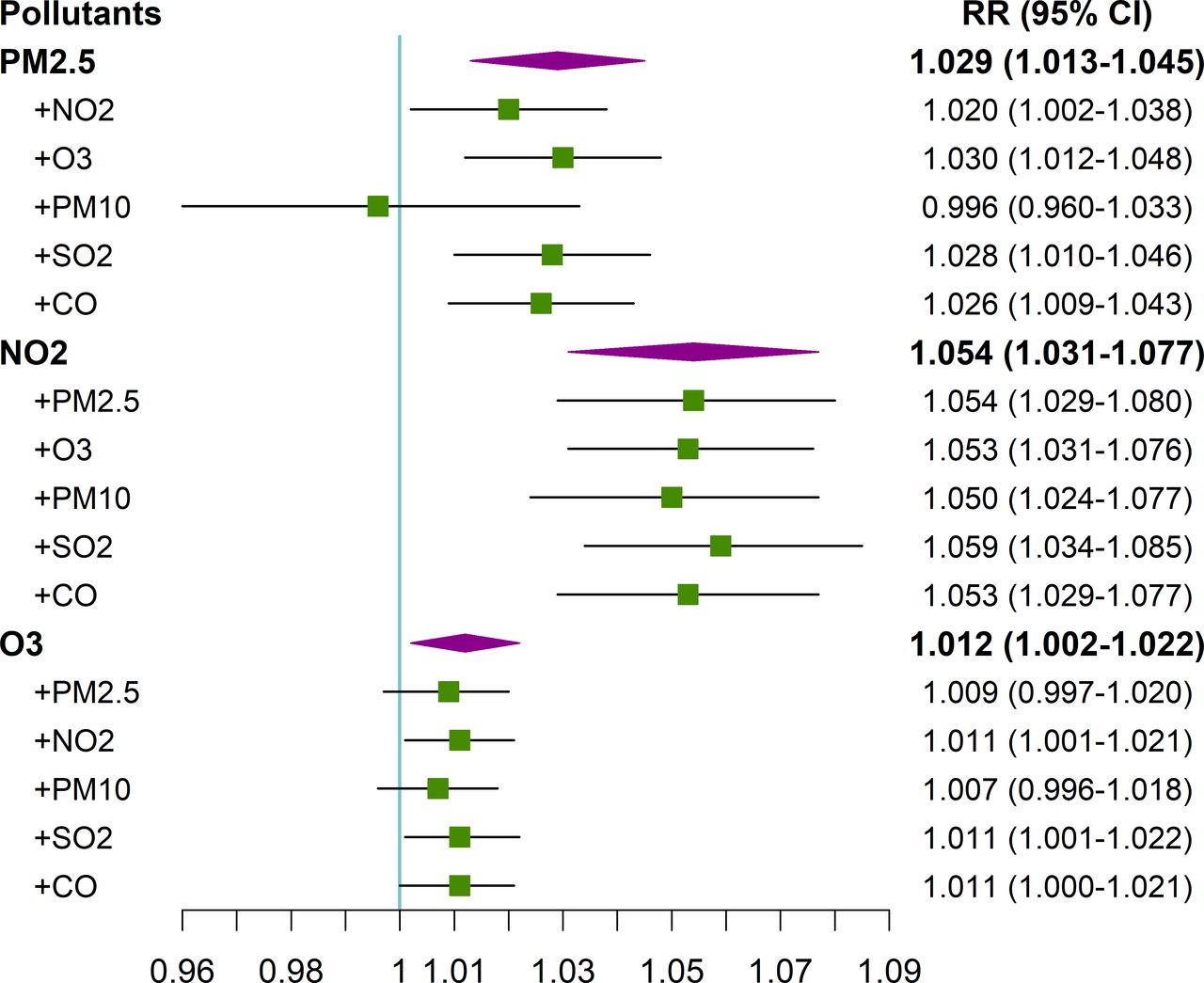
For the two-pollutant model (figure 1), the results did not vary substantially compared with those in the single-pollutant models, especially for NO2. The results were stable after adjusting the df values of  and
and  , as well as the number of lags considered for the air pollutant in the model, indicating the stability of the estimated effects (online supplementary tables S2 and S3).
, as well as the number of lags considered for the air pollutant in the model, indicating the stability of the estimated effects (online supplementary tables S2 and S3).
{kind=link}
RRs (95% CI) of stroke hospitalisations for every 10 µg/m3 increase in ambient PM2.5, NO2 and O3 in the two-pollutant model, across lag 0–3 days. CO, carbon monoxide; NO2, nitrogen dioxide; O3, ozone; PM10, inhalable particulate matter; PM2.5, fine particulate matter; RR, relative risk; SO2, sulfur dioxide.
Discussion
In this study, a positive association was found between the daily stroke hospitalisations and the concentration of ambient PM2.5. Previous studies showed inconsistent results when exploring the short-term associations between PM2.5 and stroke morbidity. Some studies observed a non-significant association, while other studies found a significant positive association.10 20 For example, a 2014 meta-analysis of nonfatal strokes found an RR of 0.7%–0.8% for short-term effects per 10 µg/m3 PM2.5.21 Exposure to particulate matter increases inflammation, antioxidant activity and circulating blood platelet activation, and decreases vascular endothelial functions and enzyme activity, the latter of which may increase peripheral thrombosis and blood clotting.22–24 Furthermore, compared with PM10, PM2.5 has a smaller size and larger surface area and can carry more harmful substances and penetrate deep into the human body,25 finally inducing a stroke.
We found that daily stroke hospitalisations increased by 5.4% for every 10 µg/m3 increase of NO2. These results are similar to those of previous studies, but some of the previous studies obtained different effect estimates.26–28 For example, a study in Wuhan, China, showed a 2.9% increase in stroke hospitalisations per 10 µg/m3 increase in NO2 in the cold season, which was smaller than the result (9.5%) from our study.29 Evidence has shown that NO2 is related to plasma fibrinogen30 and is also correlated with PM2.5, which leads to increased coagulability through the release of cytokines.28 Gaseous NO2 can also be mixed with water to form acid aerosols after inhalation, which damages health through a series of oxidation mechanisms.31
The study found that the RR of stroke associated with an increase in the level of air pollution from the first to the third quartile was slightly higher for NO2 than for PM2.5. Previous studies showed similar results14 32; gaseous pollutants appeared to have a stronger effect on stroke mortality,33 34 and some studies indicated that, after adjusting for other pollutants, only NO2 showed consistent results with a single-pollutant model.35 36 Concern has been raised that the observed health effects associated with NO2 might be a result of exposure to traffic-related emissions or fine particles.37
A weak positive association between O3 and hospital admissions for stroke was found in our study. Previous studies exploring this relationship showed different results. For example, a 10-year study conducted in France showed a significant positive relationship between O3 exposure and ischaemic stroke in men over 40 years of age, and the result was observed for a 1‐day lag (OR 1.133, 95% CI 1.052 to 1.220).38 In the USA, where air pollution levels are low, the incidence of CBI/transient ischaemic attack was also associated with O3 exposure.39 However, there was no statistically significant association found between O3 pollution and the incidence of stroke in South Carolina and Nueces County, Texas.40 41 Some studies even showed a significant or non-significant negative association between O3 and CBI.42 43 The mechanisms linking O3 and stroke need to be further studied.
The associations were found in both men and women; no clear trends were found across age groups and education levels. We found that the associations between air pollution and stroke morbidity had no statistically significant differences between different age groups. Similar results have been found in some previous studies.14 44 Elderly people may spend more time indoors, and they are likely to wear masks when air pollution is severe; thus, their individual exposure may be less.45 On the other hand, Tian et al found that the associations between air pollution and stroke morbidity were stronger in the elderly.32 Therefore, the modification effect of age on the associations between air pollution and stroke morbidity needs further study. In addition, vascular risk factors, such as hypertension and hyperlipidaemia, may also modify these associations, which needs to be addressed in future research.
The seasonal analyses showed that statistically significant associations between ambient air pollutant concentrations and hospital admissions for stroke were only found in the winter; Dong et al also found that the harmful effects of NO2 and SO2 were more robust in the cold season.14 One possible reason for this result is that the air pollution concentrations in Shenzhen are higher in winter than in summer (online supplementary table S1). The substances carried by particles may vary between seasons, which would influence the effect.
Our study found that PM2.5, NO2 and O3 were related to hospitalisations for CBI but found different results for ICH. Similarly, previous studies showed consistent associations between CBI and air pollution, while the association between ICH was more variable and had a higher imprecision.46 One reason is that the prevalence of ICH was much lower than CBI. In our study, 77.8% of stroke hospitalisations were for CBI, and ICH only accounted for 17.0% of stroke hospitalisations. Therefore, the risk estimates for ICH were more imprecise, and the CI of the RR for ICH was wider. Another reason may be the differential mechanisms linking air pollution exposure to CBI and ICH. PM2.5 exposure is conducive to atherosclerosis and the oxidative stress of the heart. These conditions may upregulate visfatin, reduce heart rate variability and induce CD36-dependent 7-ketocholesterol, which accumulate in macrophages.47–50 All of these factors are more likely to induce CBI than ICH.
There are several limitations in this study. First, the air pollution data from fixed-site monitoring stations may not be representative of average population exposure. For example, the air pollution concentrations near the main roads with heavy traffic were often higher than those near the parks with few vehicles, and the air pollution monitoring stations were usually located far away from the main roads with heavy traffic. Second, it is difficult to completely eliminate the possibility of ecological fallacy in time-series studies, and we cannot provide absolute risks in this study. Moreover, the associations observed in the present study cannot prove causality.
Conclusions
PM2.5, NO2 and O3 may induce stroke morbidity, especially in the winter. All three air pollutants were associated with higher risks of hospital admission due to CBI, the most prevalent stroke subtype in the study location. The government should take actions to address air pollution issues and develop warning systems for sensitive populations during high-risk periods.
References
Footnotes
YG and XX contributed equally.
Contributors The study was conceived and designed by JB, JP and YG; XX and YG conducted statistical analysis and drafted the manuscript; LL, HZ, and SD contributed to data collection and processing; YX and ZL helped in study management and the interpretation of the results; JB, JP and CH reviewed the manuscript for important intellectual content. All authors read and approved the final version.
Funding This study was supported by grants from National Key R&D Program of China (2018YFA0606200), Shenzhen Science and Technology Project (grant number JCYJ20170303104937484), Sanming Project of Medicine in Shenzhen (grant number SZSM201911015) and China Postdoctoral Science Foundation (grant number 2017M612827).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval The institutional review board at the School of Public Health, Sun Yat-sen University, approved the study protocol (number 2019-029) with a waiver of informed consent. Data were analysed at the aggregate level. All patients were anonymous, and no patient privacy were revealed.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No additional data are available.