Article Text

Abstract
Objective To identify, understand and explain potential risk and protective factors that may influence individual and physician group performance, by accessing the experiential knowledge of physician-assessors at three medical regulatory authorities (MRAs) in Canada.
Design Qualitative analysis of physician-assessors’ interview transcripts. Telephone or in-person interviews were audio-recorded on consent, and transcribed verbatim. Interview questions related to four topics: Definition/discussion of what makes a ‘high-quality physician;’ factors for individual physician performance; factors for group physician performance; and recommendations on how to support high-quality medical practice. A grounded-theory approach was used to analyse the data.
Setting Three provinces (Alberta, Manitoba, Ontario) in Canada.
Participants Twenty-three (11 female, 12 male) physician-assessors from three MRAs in Canada (the College of Physicians & Surgeons of Alberta, the College of Physicians and Surgeons of Manitoba and the College of Physicians and Surgeons of Ontario).
Results Participants outlined various protective factors for individual physician performance, including: being engaged in continuous quality improvement; having a support network of colleagues; working in a defined scope of practice; maintaining engagement in medicine; receiving regular feedback; and maintaining work-life balance. Individual risk factors included being money-oriented; having a high-volume practice; and practising in isolation. Group protective factors incorporated having regular communication among the group; effective collaboration; a shared philosophy of care; a diversity of physician perspectives; and appropriate practice management procedures. Group risk factors included: a lack of or ineffective communication/collaboration among the group; a group that doesn’t empower change; or having one disruptive or ‘risky’ physician in the group.
Conclusions This is the first qualitative inquiry to explore the experiential knowledge of physician-assessors related to physician performance. By understanding the risk and support factors for both individual physicians and groups, MRAs will be better-equipped to tailor physician assessments and limited resources to support competence and enhance physician performance.
- qualitative research
- clinical governance
- quality in health care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Our study is the first known qualitative inquiry to explore the risk and support factors of individual and group physician performance.
This is the first qualitative study undertaken by and using shared resources from multiple medical regulatory authorities in Canada.
This work forms one component of a pan-Canadian initiative tasked with building the evidence base on risk and support factors of physician performance.
This study was among the first to explore the risk and support factors of physician group practices, an area becoming increasingly important with the movement in healthcare settings towards team-based practices and assessments.
Study participants’ experiences and opinions may not be generalisable to or representative of all physician-assessors, in Canada or internationally.
Introduction
Although most Canadian citizens who access healthcare services receive competent and safe care, medical regulators and other physician organisations are charged with developing a robust system of continuing competence for physicians in practice. This system supports the maintenance of competence for safe care as well as the identification of physicians who may be providing low-quality, unsafe care.1 2 Risk factors for poor performance have been studied in the published literature generating evidence about the individual, organisational and systems level factors that may hinder performance. Studies have also examined support factors that may promote high-quality practices.
An evidence synthesis in 20151 examined 17 primary studies looking at risk and support factors for quality clinical practices across three performance outcomes: complaints, disciplinary action and prescribing and testing errors. This synthesis, along with other published work, highlights several risk factors that are consistent predictors of poor performance across a variety of outcomes: gender,2–4 age4–6 and performance on medical examinations have consistently been shown to be risk factors of poor performance; workload,7 8 practising in a solo environment,9 and practice specialty3 10 have been studied less frequently but seem to pose some risk to poor performance; and being an internationally-trained medical graduate is inconsistently related to performance.10 11 A recent (2017) scoping review of literature regarding risk and support factors of competence for healthcare professionals12 revealed that the top four risk factors discussed in medicine were transitions in practice, being an international medical graduate, lack of clinical exposure and age. Studies on support factors primarily examined the role of continuing education participation and key features of educational programming on performance.
While the evidence base on risk and support factors of physician performance is growing steadily,13 there remains a scarcity of information on why identified factors may hinder or support practice and how identified factors may interact. This dearth can be largely explained by the methodological approaches used to study risk and support factors to date; most of the published literature13 14 uses epidemiological and/or quantitative research approaches which do not shed light on why a factor might be a factor. While undeniably valuable, these approaches are also constrained by the availability of data that can be included in epidemiological models (eg, gender and age are consistently studied because they are relatively easy to include).
The relationship between physician competence and performance is important to consider when evaluating the evidence that has been produced to date. In the Cambridge Model from Rethans et al,15 competence is a necessary—but not sufficient—condition for high-quality physician performance. Competence refers to how physicians perform in ‘controlled representations of practice’ such as a written or physical examination; the competence a physician obtains on completing undergraduate medical school and residency training, and passing appropriate qualifying medical licensure examinations. Performance, on the other hand, is a broader term that represents how physicians perform on a daily basis, acknowledging that practice is multidimensional and impacted by many factors. While much work has explored methods of assessing physician competence, assessment methods of physician performance is lagging.16 Assessing physician performance requires consideration of the dynamic interaction of individual and contextual factors that impact how an individual applies their attitudes, knowledge and skills.16 An understanding of risk and support factors of performance helps to inform such assessment initiatives.
Globally, medical regulatory authorities (MRAs) are charged with licensing physicians and developing quality assurance programmes to fulfil the mandate of public protection.17 Quality assurance and quality improvement programmes are designed to highlight areas for physician practice improvement. In collaboration with system partners, such programming is intended to contribute to ensuring that physicians remain competent throughout their careers. Canadian MRAs, in collaboration with other physician organisations (The Pan Canadian Initiative consists of: the College of Family Physicians Canada, the Canadian Medical Protective Association, the Federation of Medical Regulatory Authorities of Canada, the Medical Council of Canada and the Royal College of Physicians and Surgeons of Canada), have embarked on a national research agenda to identify, explore and understand risk and support factors of physician performance. Knowledge of the individual, organisational and systems-level factors that protect and hinder physician performance will be used to develop a robust system that promotes high-quality medical practices. Various individual and organisational or system factors, and the effect of such factors on physician performance, are increasingly being investigated by MRAs, in both Canada and internationally.18–20
This current research is a component of a pan-Canadian initiative tasked with building the evidence base on risk and support factors of physician performance. The aim of this study is to address a gap in the literature by investigating the experiential knowledge of physician assessors who regularly assess physician performance on behalf of MRAs. Perspectives of experienced assessors regarding risk and support factors will be explored for both individual and group performance with a particular attention to why a factor may be a factor and interactions among factors. The firsthand wisdom of these assessors can provide key insights into the contextual factors that impact medical practice that quantitative data alone cannot describe.21 In addition, such experiential knowledge may reveal factors which are inherently difficult to study using traditional empirical methods and therefore may be lacking in the published literature.21 22 Gaining a comprehensive understanding of the experiential knowledge of physician assessors is essential to improve the collective understanding of factors that influence the quality of physician performance. Such knowledge will be used to identify potential strategies to support and protect high-quality medical practice and physician performance in Canada and internationally.
Methods
A pan-Canadian research team comprised of a senior research associate with experience in qualitative health research projects and methodologies (NK) and a senior medical advisor (NA) from the province of Alberta, Canada; a senior researcher (WY) and a research associate (KH) from the province of Ontario, Canada, was assembled in 2016 for this project.
Participant selection was completed primarily through convenience sampling in Alberta and Manitoba, and purposive sampling in Ontario. A total of 23 individual physician-assessors were invited to participate from Alberta, 3 from Manitoba and 13 from Ontario. Using a constructivist grounded-theory approach, semistructured interviews were held with 13 physician-assessors from the College of Physicians & Surgeons of Alberta (CPSA), 2 from the College of Physicians and Surgeons of Manitoba (CPSM) and 8 from the College of Physicians and Surgeons of Ontario (CPSO).23 Participants were provided with a study background/information sheet and a consent form that was signed and sent back to the research team prior to their interview.
Eleven out of the 23 participants were female. Collectively, participants had experience conducting assessments in family medicine, rural general practice, addictions/chronic pain medicine, walk-in or episodic clinic care, emergency medicine, rheumatology, dermatology, anaesthesiology, surgery, psychiatry and General Practitioner (GP)-psychotherapy. The 23 interviews were conducted by NK between April 2016 and February 2017 via telephone or in-person whenever possible. Interviews lasted no longer than 60 min, and were audio-recorded on consent and transcribed verbatim. Twenty-two of the 23 participants agreed to be audio-recorded; one assessor refused but still participated in the interview.
Interviews focused on four topic areas (see online supplementary appendix for complete interview guide):
Definition/discussion of what makes a ‘high-quality physician’.
Risk and protective factors of individual physician performance.
Risk and protective factors of groups or clinic performance.
Recommendations or suggestions on how to support or protect high-quality medical practice.
Supplemental material
A grounded-theory approach was used to analyse the data, meaning that findings were generated inductively from the data (participant interviews).23 24 Interviewer notes and transcripts were imported into NVivo 11 Pro qualitative data analysis software to assist NK with coding and grouping into appropriate themes. NK, KH and WY reviewed several transcripts concurrently and held bi-weekly teleconferences (February 2017–May 2017) to discuss and review common themes, and resolve any discordance. NK and KH reviewed all transcripts, going back and forth from the original transcripts to the iterative coding chart and ‘grounding’ the emergent themes in the data.23 To ensure rigour—or ‘credibility,’ as more appropriately defined in grounded theory research24—researchers attempted to bracket preconceptions regarding what makes a ‘high-quality’ physician and what potential risk and/or protective factors might be. Interviews, research team meetings, notes and memos were documented to ensure auditability.
Patient and public involvement
Patients (and/or the public) were not involved in the development of the research question(s), the design of the study, recruitment and conduct of the study.
Results
An exploration of the experiential knowledge of physician-assessors generated insight into the following four categories:
Skills and attributes of high-quality physicians.
Risk and protective factors of individual physician performance.
Risk and protective factors of group performance.
Contextual factors that influence individual and group performance.
These categories interact with each other to influence physician performance and patient care (see figure 1). The factors within each category (see table 1) are detailed below, supported by anecdotes and excerpts from participant interviews.

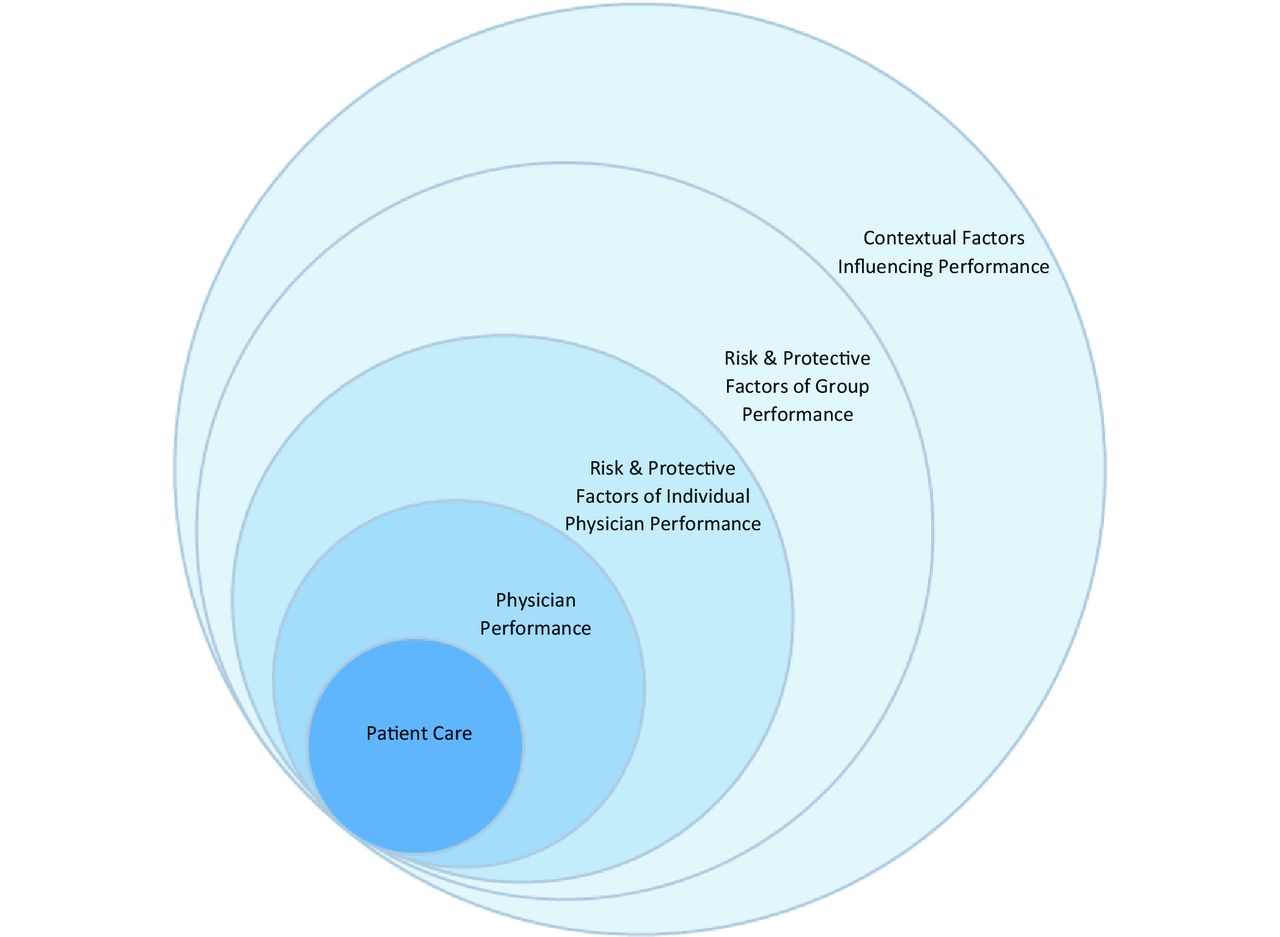{kind=link}
Model of the interaction of factors affecting patient care, as identified by experienced physician assessors.
Factors of physician performance as identified by physician assessors
Skills and attributes of high-quality physicians
Assessors’ perceptions of the skills and attributes of high-quality physicians were grouped into four key areas: clinical, administrative, interpersonal and personal (see table 1). While all were perceived as important components of high-quality performance, participants almost universally stated that a physician’s personal attributes, specifically their level of engagement and intrinsic motivation, were most critical. Participants spoke of physicians who were in medicine for the ‘right reasons’, who truly cared about patients as human beings and who were ‘emotionally engaged in healthcare’. This was considered central to high-quality performance, influencing the maintenance of most other skills and attributes.
"A high-quality doctor is somebody who really wants to be a physician not because they want to make a lot of money, but because they really enjoy the practice of medicine."
Conversely, many participants stated that at-risk physicians are those who don’t ‘care’ about their practice but are, rather, ‘money-oriented.’ Being extrinsically motivated was seen as a critical detractive quality, primarily because it can lead to high volume practices, rushed patient visits and the potential for medical errors and low-quality patient interactions.
"The most significant risk factor is a money orientation. If somebody’s primary goal is volume and quick throughput, it’s very difficult to actually have an environment that will foster good quality care."
Although such personal attributes are often not directly observable, assessors described using administrative practices and office environments as indicators of whether a physician ‘cares’ about their practice and their patients. For example, engagement is often evident in diligent record keeping, efficient office management, and clean and pleasant waiting rooms, while disengagement and extrinsic motivation can be inferred from high volume practices, scanty record keeping and poorly maintained offices.
"The most important point is that they care about what they are doing. I see those qualities in measurable things: appointments are booked so that they have time to spend with patients, to talk to them. Care is well-documented and follow-up is arranged."
By observing administrative practices, and determining if the physician ‘cares’, participants stated that they are able to form impressions about the quality of the practice. In this way, assessors seem to use a physician’s level of engagement as a global measure of how protected the entire practice will be.
Protective and risk factors of individual physician performance
Assessors outlined a number of factors that may support or detract from individual physician performance (see table 1). Continuous quality improvement (CQI) was perceived as central to supporting one’s practice. This included participating in continuing professional development (CPD), staying current with literature and guidelines, seeking out feedback proactively and acquiring new skills and knowledge as needed to serve one’s evolving patient population. Relatedly, maintaining engagement in medicine—fostering a continued sense of curiosity and interest in solving clinical problems and serving patients—was identified as a critical protective factor. Additionally, having a colleague support network for asking questions and receiving regular feedback from, was seen as essential for supporting one’s practice and stimulating ongoing professional development:
"Interactivity is very, very important. It’s really hard for a physician to keep growing and keep moving forward without that external feedback. There is something very special about having other professionals who are meeting the same challenges that you are meeting, and to have the ability to discuss them in a safe way."
Physicians who manage their practice scope and volume were thought to be protected: working in a defined scope may make it easier to stay abreast of relevant guidelines and maintaining a moderate patient volume can both reduce the risk of patient errors and foster work-life balance, preventing burn out and fatigue. Conversely, participants noted that physicians with high patient volumes tend to rush through patient interactions and have insufficient time to think critically:
"It is very easy, in the middle of an influenza epidemic, to be working so quickly with many patients that you may not realise one of them has encephalitis; and that if you had a bit more time and weren’t so rushed, the bells would go off. That is a huge risk."
Not staying current with medical knowledge, having a limited colleague network or feedback opportunities and becoming disengaged were seen as detractive of physician performance. Participants spoke of physicians who had ‘gotten in a rut’, who had lost their interest in seeking out new trends in medicine or who were no longer ‘curious’:
"An awful lot of physicians run into trouble when they have lost their sense of curiosity, or they never had it in the first place, and things are done by rote. When things are done by rote without being curious as to the underpinnings, mistakes are made."
Some factors could be either supportive or detractive depending on the circumstances. The use of electronic medical records (EMRs) can support good record keeping and patient management, but only if the system is user-friendly and the physician is already proficient at record-keeping. Otherwise, EMRs can be risky as they may interfere with workflow and detract from patient interaction. In this sense, EMRs were seen as a ‘facilitating’ factor: they might enhance a good practice but may not support an already at-risk one.
Being an international medical graduate (IMG) was also perceived as either a support or risk factor, depending on a physician’s level of colleague support and professional integration. IMGs can often speak languages other than English or French and can relate to multicultural patient populations within Canada which support high-quality patient care:
"Patients will gravitate to a doctor they feel comfortable with, often who speaks their language, who comes from a similar cultural background. For a multicultural population, I see it as overall advantageous and beneficial for our healthcare system."
However, IMGs who are newcomers to Canada may not have a network of colleagues to support one’s practice. Professional isolation is itself a risk factor, and may be exacerbated for IMGs who may be unaware of ‘taken for granted’ norms. Some noted that there are also personal and contextual factors that interact with being an IMG: one participant recounted instances of female IMGs becoming isolated because they felt disempowered to ask for assistance; others noted that IMGs can get ‘trapped’ in isolated practices or high volume clinics as they are often recruited to underserviced areas.
Increased physician age was identified as potentially risky, as it may correlate with declining mental capabilities, fatigue, not staying up-to-date or being resistant to change, factors that can be exacerbated when paired with lack of insight, disengagement or professional isolation. However, older physicians often have the benefit of wisdom, knowledge and experience which can be protected by insight (specifically, knowing when to restrict/reduce practice), maintaining engagement in medicine or having a network of colleagues to provide regular feedback. The interaction between age and other factors was therefore evident.
"If I see an elderly physician who works in isolation in a small community, I know there is a much higher chance that there are going to be issues."
Protective and risk factors of group performance
The supportive or detractive factors of group performance fell into four themes: communication, collaboration, philosophy of care and practice composition (see table 1). High-quality group practices maintain open and honest communication among group members, foster a collaborative environment for shared patient care and have a unified philosophy of serving patients. Such practices have regular meetings about cases and practice management, maintain a culture of trust and ‘reciprocal co-mentoring’ where physicians can learn from each other and work towards a cohesive patient care approach, ultimately optimising patient care. Participants noted that working in a group is often protective in and of itself, but only if the group communicates effectively, collaborates well and has a unified approach to serving patients; in the absence of these factors, being in a group may not necessarily be protective.
"To have a high-functioning group, you have to have a group of physicians who get along well, who are collegial, who respect one another, who have a similar outlook, a similar philosophy."
Groups who do not communicate and collaborate with each other, and do not have a shared approach to patient care may be at risk, as they tend to operate as adjacent solo practices rather than cohesive teams. Participants noted that groups need a shared philosophy of care in order for the group to thrive. Groups formed solely for financial reasons may put themselves at risk of ineffective team functioning.
Interviewees indicated that practice composition can also influence performance. Groups with a dedicated medical director or someone who takes leadership in the group are often supported, as these leaders tend to oversee the practice, address issues as they arise, facilitate change management, assign accountability where required and drive the Continuous Quality Improvement (CQI) of the practice. Having diversity of physicians within a group practice (eg, differing backgrounds, training, experiences and ages) can also be supportive, as patient care is often enhanced when multiple perspectives are considered. Diversity, however, was only seen as protective if there is effective collaboration among the group and a shared philosophy of care underlying physicians’ diverse perspectives.
"Working together, interacting with another doctor, you have the benefit of a younger physician who may have just learnt something new in training; versus an older doctor’s wisdom. Then the patient is getting the benefit of several different minds with perhaps different clinical backgrounds."
Multidisciplinary groups are also often supported in providing high-quality patient care. Conversely, an over-reliance on other health professionals could be risky, as it might encourage physicians to take short cuts or create gaps in care if role boundaries are unclear. Groups that do not empower change may also be at risk as they can prevent physicians from improving on ineffective group practices. Lastly, group practices can be put at risk when there is one ‘risky’ physician within a group; one physician who does not collaborate well or who provides low-quality care affects the entire group when patient care is shared.
Contextual factors
Contextual or system-level factors that influence physician performance were also identified: community culture, colleague supports, episodic care clinics, resources and payment models (see table 1). Participants noted that the culture within a hospital or healthcare community, specifically the extent to which collaboration is emphasised, can influence physician performance. A collaborative culture can support all health professionals within a given environment, allowing for ‘virtual’ or ‘extended’ teams that protect practices and enhance patient care. Some assessors noted that academic hospitals tend to foster these cultures due to the nature of trainees asking questions and requiring collaborative input. Workplaces that have strong connections to the community, and that have a collaborative culture among all health professionals in a geographic area, are also often supported. Conversely, solo practices or practices within communities that do not foster collaboration may be at risk.
Assessors noted that while a community culture can influence individual physician performance, individual physicians can also affect the culture of a community, highlighting the reciprocal nature of the factors:
"When you get a disruptive physician in a group, it really is a big risk factor for the whole group. Not only the group but the whole community as well, it becomes a whole culture… And when you try to change how the practice functions, you have a lot of hurdles to overcome… it is not just that group that’s affected. Particularly in small towns, it is the whole culture."
Episodic care or ‘walk-in’ clinics were identified as risky, as they tend to have high patient volumes, short patient encounters and often do not foster a culture of accountability for patient care. One participant noted that chain clinics may be protected as they tend to have standard operating procedures that facilitate accountability and ensure the quality and continuity of care.
"Episodic care is really problematic… the main reason for that is they do not set themselves up to be accountable. No one’s going to review anything after the fact… I think it sets up that expectation that the patient is not expecting to be called back."
Assessors stated that resource constraints can cause tension for physicians and may lead physicians to take short cuts which can hinder patient care. Fee-for-service payment models can also detract from high-quality care as they tend to encourage high volume practices and short patient encounters, and also tend to perpetuate extrinsic motivation in medicine, which is a key detractive quality of physician performance.
"If they change the payment structure, if they pay physicians the same way they pay teachers and office workers and every other civil servant, you’d beat out a lot of people who go into [medicine] for the money."
Alternative payment structures to fee-for-service were seen as protective of high-quality care as they allow for longer, more mindful patient interactions and they support physician wellness by reducing time and resource pressures.
Discussion
This study explored the experiential knowledge of physician assessors regarding the skills and attributes of high-quality physicians, and the risk and support factors of individual and group performance. While some research has attempted to identify and describe factors influencing medical performance,1 3–23 this work expands on previous efforts by identifying new factors, contextualising previously studied factors and highlighting potential interactions between factors.
Some factors described in this study have been previously discussed in the literature, such as the influence of CQI and Continuous Professional Development (CPD) on physician performance.25–28 Other factors were unique, such as the importance of a physician’s personal attributes (eg, level of engagement/intrinsic motivation) in fostering high-quality performance and patient care. Our results suggest that personal attributes, or intra-personal skills, are distinct from current frameworks of physician competence (eg, CanMEDS)12 29 and that these personal attributes are vital for supporting performance over time. This aligns with the perspective in medical education that intra-personal skills are an important component of humanistic care in medicine,30 but that humanism is often absent in the education and assessment of physicians.31 The evolution towards observable, measurable competencies in medical education has de-emphasised humanistic qualities in much of medical curricula.31 However, our results propose that such qualities are imperative for high-quality performance and should not be dismissed because they are not directly observable.
Engagement at an individual level was perceived as vital for supporting quality patient care, and the act of maintaining professional engagement and ‘curiosity’ in medicine was seen as essential in protecting one’s practice over time. Engagement was also paralleled in group practices, with assessors noting that groups with a ‘common mission’ of serving patients are best supported. At the same time, extrinsic motivation was identified as a critical detractive quality at both the individual and group level, leading to low-quality patient care and obstructing effective team functioning. Physician disengagement was also seen as risky as it can detract from patient care, impede motivation for CQI and potentially impact the entire culture of a healthcare community.
In addition to identifying new factors of performance, this research also provides more nuanced information about some commonly studied factors. For example, although age is an oft-cited risk factor of physician performance,1 12 our results suggest that older physicians who maintain engagement in medicine and have opportunities for feedback may be protected. IMGs are also often cited as being at risk, but our findings suggest that this may be not because of inadequacies of training but because they lack a colleague network, suggesting that these physicians may be supported through coordinated communities of practice. Additionally, while group practices are widely considered protective, our findings suggest that such practices may only be supported if the groups communicate regularly, collaborate effectively and maintain a shared philosophy of patient-centred care.
Collectively, these findings reinforce the complexity of physician performance and the multitude of individual, organisational and contextual factors that can interact with each other to influence performance. Our results demonstrate that a physician’s personal skills and attributes, the composition and dynamics of their group practice, and the culture and context within which they work can all support or detract from their ability to provide quality patient care. These findings align with the dynamic understanding of physician performance described in the Cambridge Model15 and elsewhere26 wherein performance is conceptualised as multidimensional and influenced by many factors. Our findings also support the growing understanding that assessing physician performance is a much more complicated and dynamic process than simply assessing individual characteristics.15–17 32
The results of this study have practical implications for how MRAs can better support physicians in practice. This information could be used to educate physicians on risk and protective factors, encouraging physicians to reduce risks and seek out supports where possible. Assessors suggested that MRAs could publish examples of high-quality, well-protected practices to demonstrate how others may adopt similar supportive strategies. They may also share trends about common risks based on aggregated performance data. MRAs could also use knowledge of the factors to directly assist physicians in protecting their practices. For example, given the importance of colleague support and feedback, they could coordinate peer networks or communities of practice for physicians, particularly IMGs and those in rural or isolated regions.
MRAs could also use knowledge of risk and support factors to more appropriately allocate assessment and educational resources. Ageing or isolated physicians may benefit from focused assessment and feedback about one’s practice while high-volume practices may need strategies to ensure that patient care is not being compromised. MRAs may also tailor their assessment approaches to provide more contextually appropriate assessments for a given physician. Assessing individual characteristics places total accountability for performance on the individual physician, whereas assessments ought to consider the dynamic nature of factors contributing to physician performance within a system of healthcare delivery.17 The growing body of literature on the complexity of physician performance assessment,15 33 and the evolving nature of physician group practice34 suggest that MRAs should enhance assessment methods to include these dynamics. By doing this, MRAs will be better able to promote physician practice improvement to enhance population and public health.1 35
Lastly, MRAs may consider innovative ways of assessing the nuances of physician performance. While many factors remain difficult to measure directly, assessors indicated that they use physicians’ administrative practices to gauge the degree to which a physician ‘cares’ about their practice and their patients, then use this as a surrogate measure of how supported the entire practice will be. This may suggest that certain measurable factors, such as record keeping, may be valuable proxies of the personal qualities that support high-quality care.
Strengths and limitations
This is the first known study to qualitatively explore the risk and support factors of physician performance. The use of qualitative methodology facilitated the identification of factors that cannot easily be ascertained, described or measured through predominantly quantitative means.36 The use of experiential knowledge was particularly valuable as it allowed information about physician performance and assessment to be generated from those most closely involved.37 The assessors in this study have collectively assessed thousands of individual and group physician practices across a variety of practice settings throughout their careers, providing a rich source of data for our inquiry.
This study provides insight into why certain factors might influence physician performance, and how said factors may interact with each other. It sheds light on how assessors use these factors when assessing physicians, using observable means to form impressions of the unobservable. This study was among the first to explore the risk and support factors of group practices, an area that will become increasingly important with the movement towards team-based practices and assessments.34
A limitation of this work is that we cannot comment on the extent to which the identified factors may affect practice outcomes. Further research is warranted to test these factors in order to determine their relationship with physician performance, patient care and related health outcomes. Also, although we did not find any substantial differences in responses across specialties or regions represented in this study, we recognise that these results may not be applicable to all physicians across Canada and internationally.12
Conclusion
This research contributes to a pan-Canadian initiative aimed at understanding the risk and support factors of physician performance. By exploring the experiential knowledge of physician assessors, this study provides an in-depth understanding of the factors that support and detract from individual and group practices. Assessors defined a high-quality physician as someone who is engaged in their career and who is intrinsically motivated to serve patients. They also identified many factors influencing individual and group practices which can be further explored, validated and used to understand the complexities of physician performance. This research adds to the growing knowledge base of risk and protective factors of performance and may help to assess, educate and support physicians in practice. Most notably, this research provides rich contextual information about risk and support factors based on a wealth of experiential knowledge, and offers a more nuanced understanding of physician performance.
References
Footnotes
Contributors NAK conceptualised and designed the study, conducted all interviews (collected the data), carried out the initial data analysis, drafted the initial manuscript, critically reviewed the manuscript, approved the final manuscript as submitted and has agreed to be accountable for all aspects of the study in ensuring that questions related to the accuracy or integrity of any part of the study are appropriately investigated and resolved. KH and WY conceptualised and designed the study, carried out data analysis, critically reviewed the manuscript, approved the final manuscript as submitted and has agreed to be accountable for all aspects of the study in ensuring that questions related to the accuracy or integrity of any part of the study are appropriately investigated and resolved. NA conceptualised and designed the study, critically reviewed the manuscript, approved the final manuscript as submitted and has agreed to be accountable for all aspects of the study in ensuring that questions related to the accuracy or integrity of any part of the study are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Ethics approval This study was approved by the joint Health Research Ethics Board at the University of Alberta.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement As per the study ethics approval from the University of Alberta Research Ethics Board, additional unpublished data from the study (interview audio files, interview transcripts) are kept in a secured, locked location. Any electronic files are encrypted on the research team’s computers and will be destroyed after a period of 5 years from when the data was collected (e.g., destroyed in 2022). Only the research team has access to the data via secured servers at the College of Physicians & Surgeons of Alberta in Edmonton,Alberta, Canada and the College of Physicians and Surgeons of Ontario in Toronto, Ontario, Canada.
Patient consent for publication Not required.