Article Text

Abstract
Introduction Geriatric assessment and management is recommended for older adults with cancer referred for chemotherapy but no randomised controlled trial has been completed of this intervention in the oncology setting.
Trial design A two-group parallel single blind multi-centre randomised trial with a companion trial-based economic evaluation from both payer and societal perspectives with process evaluation.
Participants A total of 350 participants aged 70+, diagnosed with a solid tumour, lymphoma or myeloma, referred for first/second line chemotherapy, who speak English/French, have an Eastern Collaborative Oncology Group Performance Status 0–2 will be recruited. All participants will be followed for 12 months.
Intervention Geriatric assessment and management for 6 months. The control group will receive usual oncologic care. All participants will receive a monthly healthy ageing booklet for 6 months.
Objective To study the clinical and cost-effectiveness of geriatric assessment and management in optimising outcomes compared with usual oncology care.
Randomisation Participants will be allocated to one of the two arms in a 1:1 ratio. The randomisation will be stratified by centre and treatment intent (palliative vs other).
Outcome Quality of life.
Secondary outcomes (1) Cost-effectiveness, (2) functional status, (3) number of geriatric issues successfully addressed, (4) grades3–5 treatment toxicity, (5) healthcare use, (6) satisfaction, (7) cancer treatment plan modification and (8) overall survival.
Planned analysis For the primary outcome we will use a pattern mixture model using an intent-to-treat approach (at 3, 6 and12 months). We will conduct a cost-utility analysis alongside this clinical trial. For secondary outcomes 2–4, we will use a variety of methods.
Ethics and dissemination Our study has been approved by all required REBs. We will disseminate our findings to stakeholders locally, nationally and internationally and by publishing the findings.
Trial registration number NCT03154671.
- randomized controlled trial
- geriatric oncology
- comprehensive geriatric assessment
- frail elderly
- cost-effectiveness analyses
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- randomized controlled trial
- geriatric oncology
- comprehensive geriatric assessment
- frail elderly
- cost-effectiveness analyses
Strengths and limitations of this study
This study will be a large multicentre randomised phase III trial studying geriatric assessment and management for older adults referred for chemotherapy and includes a cost-effectiveness analysis.
Our primary endpoint of quality of life is an important patient-reported outcome that is recommended for trials with older adults.
We will conduct a process evaluation to understand the fidelity of the intervention implementation in the different centres and how this greater diversity impacted the implementation and effect of the intervention.
Our process evaluation of intervention fidelity will only be possible if the different study centres recruit sufficient numbers to compare the different modes of intervention delivery.
A potential limitation is selection bias with recruitment primarily at selected tertiary cancer centres.
Introduction
Over 60% of Canadians diagnosed with and over 70% of those dying of cancer are aged >65.1 Due to ageing of the population, the proportion aged 65+ is expected to increase to 27% by 2050 and cancer incidence will increase by 40% by 20301. With older age, the risk of treatment complications may rise. However, there is a lack of evidence on how to best treat older adults with cancer as this population has been severely under-represented in clinical trials. As patients age, their health and function can vary significantly, resulting in an increasingly heterogeneous population2 for whom age is not a reliable marker of health.3 Research has shown that for the majority of older adults, the most important reason to undergo treatment is preservation or improvement of quality of life.4 Physicians often find it challenging to select the best cancer treatment when older adults have other diseases in addition to cancer that impact life expectancy, quality of life and treatment tolerability.5
To help clinicians and patients select appropriate treatment and identify health and functional status issues that may affect cancer treatment delivery, the US National Comprehensive Cancer Network (NCCN),6 the International Society of Geriatric Oncology (SIOG),3 the American Society for Clinical Oncology (ASCO)7 and the European Organisation for the Research and Treatment of Cancer (EORTC)8 have all recommended a Comprehensive Geriatric Assessment (CGA) for patients aged 70 years and older for whom chemotherapy is considered.
A CGA is a multidimensional, interdisciplinary diagnostic process focusing on determining an older person’s medical, psychosocial and functional capability in order to develop a coordinated and integrated plan for treatment and long-term follow-up.9 The CGA process comprises five consecutive steps and is the main principle of modern geriatric medicine9:
Identifying who can benefit from CGA.
Completing the CGA.
Developing the care plan based on CGA.
Implementing the care plan.
Provision of follow-up and adjustment of the care plan with repeated CGA.
A CGA identifies issues that can interfere with cancer treatment delivery and includes a care plan (the intervention) to address the identified issues in the CGA. This is hypothesised to improve patient outcomes such as quality of life and functional status.3
Canada and most other countries have not implemented CGA into routine clinical care because of lack of robust evidence that it improves oncological and patient outcomes. Kenis et al 10 conducted the largest non-randomised controlled trial (RCT) to date and showed that 52% of 1115 patients aged 70+ who received a CGA had previously undetected geriatric problems such as cognitive impairment, poor nutritional status and depression. Interventions were recommended for 77% of patients.11 Findings from our and other systematic reviews of CGA indicate that cancer treatment plans were changed in 30%–39% of all patients after CGA.12 13 A small cohort study compared patients who underwent a CGA to usual oncology care; CGA was associated with a higher chance of completing treatment as planned; there was a 10% reduction in grades 3–4 toxicity in the intervention group.14
Several reviews of CGA in diverse in- and outpatient populations showed conflicting findings with no RCT incorporating CGA with geriatric management completed in oncology.12 15 16 It was tested with a very different patient population (in the geriatric medicine setting more older adults have cognitive and functional impairments compared with oncology setting). Although the literature has shown the approach is feasible in the oncology setting,12 15 there is currently no evidence available on the clinical and cost-effectiveness of this approach in improving patient reported outcomes such as quality of life in the oncology setting.
Our team consisting of oncology, geriatric and health economics experts previously completed a randomised phase II study and based on the positive results of the intervention on the quality of life a larger study is warranted and adjustments to the design for the current study were made based on feedback from clinicians, patients and feasibility data17 (eg, monthly interviews instead of mail surveys every 3 months, and more frequent contact with intervention team).
Primary objective
To determine the clinical effectiveness of the intervention (at 6 and 12 months) on maintaining/improving quality of life in older adults aged >70 years referred for first/second line chemotherapy compared with usual oncology care.
Secondary objectives
To determine the effectiveness of the intervention compared with usual oncology care with regards to:
Cost-effectiveness.
Maintaining/improving functional status.
Number of geriatric issues successfully addressed.
Development of grades 3–5 chemotherapy toxicity).
Unscheduled healthcare utilisation.
Patient and provider satisfaction.
Cancer treatment plan modification.
Overall survival (OS).
To examine intervention fidelity by healthcare setting.
Intervention theory
The intervention improves quality of life by targeting three main challenges in the care of older adults:
Untimely detection of health/functional issues, which are risk factors for unsuccessful cancer treatments.
Older adults’ lack of autonomy/participation in their care process.
Inadequate coordination of care.
We hypothesise that the CGA will identify health and functional issues that were previously unknown to the oncology team. This may result in changes in the treatment plan and thus prevent both over- and under-treatment, which theoretically may alter outcomes such as quality of life and OS. Two systematic reviews of inpatient geriatric assessment,15 16 showed this intervention improved survival at 6, 8 and 12 months. However, most studies included in the review excluded ambulatory cancer/oncology patients as well as those with limited life expectancy and included more patients with functional and cognitive impairments. Thus, the survival benefits may be different in cancer patients. In this study, we will examine OS as a secondary outcome. The intervention team will coordinate care with the oncology team, primary care team and external providers. Most of the RCTs have been conducted many years ago and none included a cost-effectiveness analysis. Thus, there is no information about the cost-effectiveness of this intervention in the ambulatory setting.
Methods and analysis
Study design
A multicentre two-group parallel group, outcome assessor blinded RCT (figure 1) will be conducted. A cost-effectiveness analysis will be done alongside the RCT using a payer and societal perspective to study the cost-effectiveness of this intervention compared with usual care.
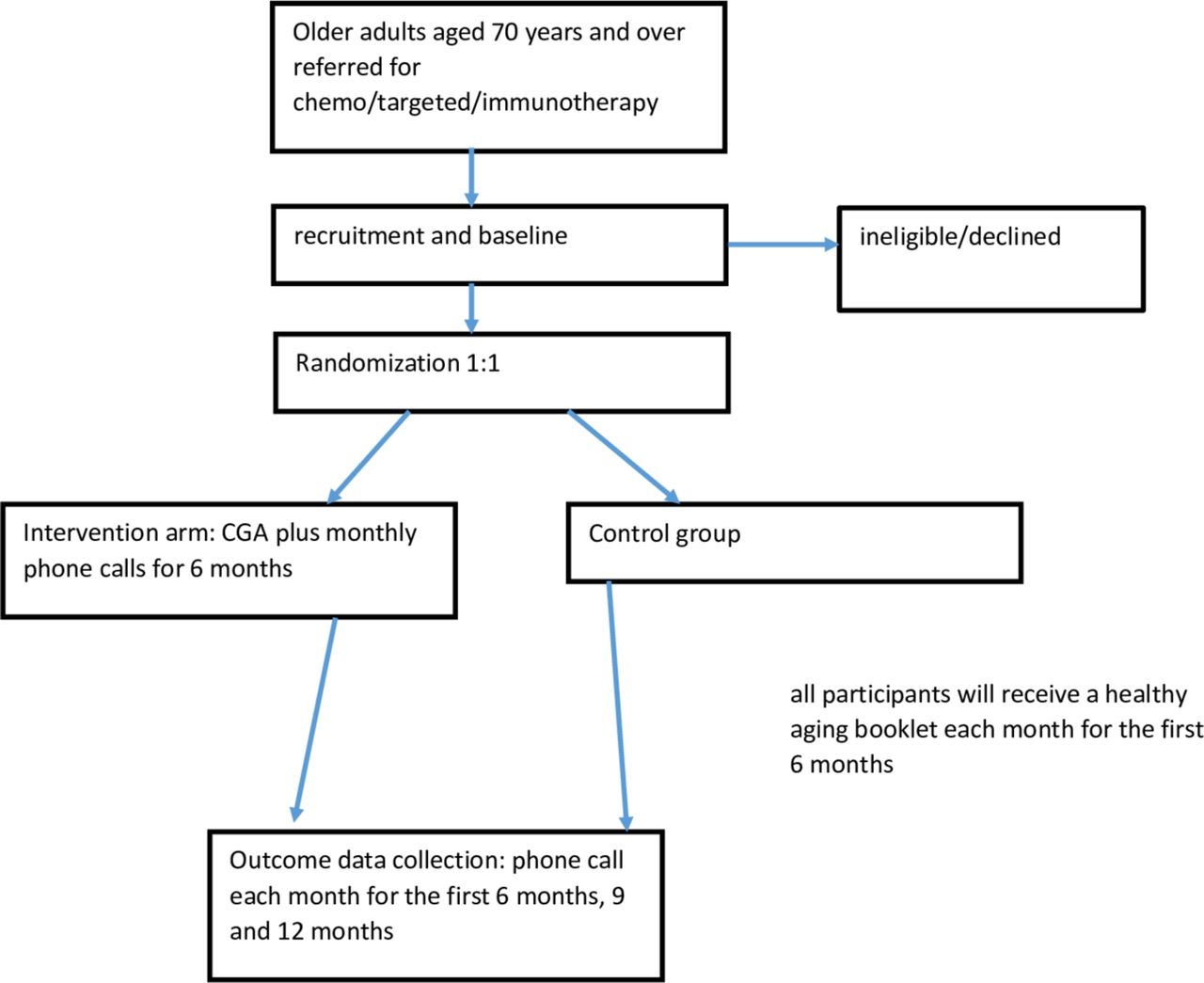
{kind=link}
Study overview. CGA, Comprehensive Geriatric Assessment.
Study centres
Princess Margaret Cancer Centre, Mount Sinai Hospital, Odette Cancer Centre, Toronto; the Ottawa Hospital Cancer Centre, Ottawa; the R.S. McLaughlin Durham Regional Cancer Centre, Oshawa, Ontario; the Segal Cancer Centre, Jewish General Hospital, Montreal, St. Mary’s Hospital, Montreal, Quebec and the Fraser Valley Cancer Centre Surrey in collaboration with the Royal Columbian Hospital, New Westminster, British Columbia. Over 30% of patients at each study centre are age 70 years or older.
Randomisation
We will use the randomisation module in REDCap (https://projectredcap.org/), which is 24 hours accessible, to randomly allocate participants to the intervention or control group in a 1:1 ratio. We will use stratified randomisation (curative/adjuvant vs palliative treatment intent and by study centre) to ensure balanced groups in each centre. Randomisation will occur after the baseline assessment is completed.
Blinding
Although neither clinicians nor patients can be blinded to treatment allocation, the outcome assessors will be blinded. The independent statistician conducting the clinical effectiveness outcomes will also be blinded to group allocation.
Inclusion criteria
In this study to select participants who can benefit from the CGA, inclusion criteria are age 70 years and over who are being considered for chemotherapy as in agreement with the SIOG3 and ASCO geriatric oncology guidelines.7
Patients aged 70+ with any solid tumour (excluding pancreatic) or lymphoma/myeloma referred for first/second line adjuvant/curative or palliative chemotherapy in the ambulatory setting (cannot have received more than one cycle at the time of consent).
Able to speak English/French.
Physician-estimated life expectancy >6 months.
Eastern Collaborative Oncology Group (ECOG) Performance Score 0–2 (indicating participants are ambulatory and able to complete all self-care activities).
Able to give informed consent.
Exclusion criteria
Being followed by a palliative care physician on recruitment.
Already participating in another psychosocial/educational intervention study (participation in a new therapeutic treatment study is allowed).
Having seen a geriatrician (in community or hospital) in the previous 12 months.
Intervention
Geriatric assessment
Participants randomised to the experimental group will receive usual cancer care from the cancer specialist PLUS CGA and management by the geriatric oncology team (a registered nurse [RN] and geriatrician).
Our standardised CGA protocol (see table 1) is based on our previous phase II trial, the clinical experience of the existing clinical geriatric oncology teams and expert guidelines/reviews.3 6 12
Overview of Comprehensive Geriatric Assessment domains, tools and relevance to cancer treatment
The CGA includes sociodemographic information, functional status (consisting of Basic Activities of Daily Living [ADL]),18 Instrumental Activities of Daily Living (IADL),19 and the 1-item ECOG-Performance Status20), comorbidities (the Charlson Comorbidity Index),21 history of falls (Cancer and Ageing Group Chemotherapy Toxicity Risk Tool item),22 a medication review3 and seven frailty markers (weight loss,23 fatigue (one item from Edmonton Symptom Assessment system-revised),24 grip strength (handheld dynamometer),23 cognition(Mini-Cog),25 mobility (Short Physical Performance Battery),26 physical activity,27 and mood (Patient Health Questionnaire—nine items).28 Furthermore, we will include the Geriatric Risk G8 screening tool,29 pain (one item from Edmonton System Assessment system-revised),24 vision and hearing (Cancer and Ageing Research Group Chemotherapy Toxicity Risk Tool items),22 vitals and the Cancer and Ageing Research Group chemotherapy toxicity risk score.22
Based on our experiences, this CGA takes approximately 45–60 min which is acceptable and feasible in older adults.12 In our phase II study, all participants were able to complete the CGA in one visit. The CGA will be completed at baseline; components may be repeated during follow-up if deemed necessary by the intervention team.
Geriatric management
The standardised geriatric management protocol (see table 2) is based on clinical experience of the Princess Margaret Cancer Centre/Jewish General Hospital team, evidence-based practice and the NCCN Older Adult Oncology Guideline6 and the CGA guided care expert consensus document.30 Based on the CGA results, predefined evidence-based interventions described in table 2 that are deemed necessary by the intervention team together with the participant will be implemented and this includes referrals to other allied healthcare team members such as dieticians, social workers and occupational therapists. For the two hospitals who do not have a geriatrician on site (Lakeridge Hospital in Oshawa and the Ottawa Hospital Cancer Centre), the nurse who conducted the CGA will discuss with the geriatric team at the Princess Margaret Cancer Hospital to develop the care plan using the telephone/the Ontario Telehealth System. As the older population is the most heterogeneous of any age group in terms of health, functioning and comorbidities, interventions will be targeted based on need rather than a one-size-fits-all approach and will take into account the priorities of older adults and their family which might not always be identical to those of the healthcare team.
Intervention protocol based on team experience, National Comprehensive Cancer Network older adult, International Society of Geriatric Oncology and expert consensus guideline
Overview outcome data collection at each point in time
After the visit in which the CGA has been conducted and the care plan has been developed, the RN from the intervention team will follow the patient with at least monthly using telephone calls for 6 months to evaluate the care plan developed on the basis of the CGA, assess changes in health and identify if clinical follow-up with the geriatricians is needed. The nurse will consult with the geriatrician for any new issues arising during the follow-up (eg, new fall) to manage the issue. Clinical follow-up appointments to repeat the CGA will be arranged as needed to address any new geriatric issues that arise during treatment. We will record which recommendations the participant implemented and which not and the reasons for that for the process evaluation.
The CGA results and recommendations will be communicated to the oncologist and primary care team within two business days allowing them to use the CGA information for treatment decision-making. Each intervention team will communicate the results to the participant’s family doctor based on the normal procedures used at their hospital. The intervention teams will implement all recommendations as much as possible by themselves to enhance adherence to the recommendations.
Based on the literature, approximately 30%–40% of treatment decisions may change resulting in increases and decreases in intensity.12 13 Previous research has also shown that 5%–23% of patients may be offered best supportive care instead of chemotherapy based on the CGA.31 With our inclusion criteria of a life expectancy of six or greater months, we anticipate that most patients may thus benefit from chemotherapy treatment. Patients who receive best supportive care will remain in the study and outcomes will be collected for the follow-up period. In the statistical analyses, we will adjust the analyses for the receipt of chemotherapy or not. For the secondary outcome treatment toxicity, those who received no chemotherapy will be excluded from the analyses.
Description of usual care
Participants allocated to the control group will have access to standard care provided by their oncologist. All study participants will receive a monthly healthy ageing booklet that will address a different topic each month (coping with cancer, nutrition, exercise, fall prevention and home safety, medication use) to enhance engagement of participants with the study and thus increase retention.32 The passive provision of mailed health education booklets has been shown to increase motivation to change health but has no impact on health behaviour outcomes33 and has been used in the usual care arms of numerous recent RCTs with older adults.34 35 These pamphlets are currently available in many hospitals and in the community.
Risks to the safety of trial participants
This intervention is standard of care in the geriatric medicine setting and there are minimal risks of our study intervention for trial participants.
Contamination
While we will capture how many participants in each arm consult with a geriatrician outside the study during the study period, in all cities where we will recruit participants the average waiting time for a geriatric consult ranges between 3–4 months (British Columbia) and 4–6 months (Ontario and Quebec); thus, we expect that contamination will be low. Most family doctors do not routinely use GA in their clinical practice and thus we expect a low contamination rate and this will be captured in our healthcare diary. We will offer the intervention to the control group after 6 months for interested participants.
Outcomes
Outcomes will be assessed at baseline (see table 3 for Overview data collection), then monthly by telephone for the first 6 months, and then at 9 and 12 months by telephone, in person or by mail survey to accommodate that older adults may have different sensory problems/dexterity/literacy skills impacting the data collection (eg, hearing problems limiting telephone interviews and preferring in person interviews, vision problems limiting self-completion and thus the research assistant can help complete it in person with them at a hospital visit). The data will be entered during the interview in the REDCap system (https://projectredcap.org/). The healthcare use cost data will be collected through a prospective diary that participants will be asked to return by mail at 3, 6, 9 and 12 months.
Our primary effectiveness analysis for primary and secondary outcomes will take place at 3 months (short-term effectiveness as our intervention is hypothesised to help patients during cancer treatment delivery), and our secondary analysis at 6 months (intermediate effectiveness). At 6 months, many patients with cancer have completed their cancer treatments. Our final analysis will take place at 12 months to determine the long-term impact of the intervention. The statistical model will incorporate all the data collected from all the multiple time points to be able to model the potential non-linear relationship of our quality of life outcome for each of the three effectiveness analyses.
Primary outcome
Quality of life will be measured with the EORTC Quality of Life-Core 30 item version (QLQ-C30 Questionnaire),36 which is a psychometrically valid cancer-specific quality of life instrument. We will use the global quality of life scale. This outcome is clinically relevant for older adults,37 plays a major role in their decision to accept chemotherapy,38 and is recommended as an end point in trials by the EORTC and SIOG.39
Secondary outcomes
Cost-effectiveness will be determined alongside the clinical trial following standard guidelines.40 We will use two methods to collect data needed for the cost-effectiveness analyses: (a) EuroQol-5 dimensions with five levels (EQ-5D-5L)41: the EQ-5D-5L is a well-validated, widely used, generic instrument that measures patient utilities across 5 dimensions of health; (b) patient costs: resource utilisation, out-of-pocket costs and productivity costs will be estimated using a patient cost diary42 that Drs Alibhai and Krahn have used in prior studies, and that will be adapted for this study.43 The intervention team will keep a record about the time spend for the clinical contacts to calculate the intervention costs.
Functional status using the Older American Resources and Services IADL questionnaire19.
The number of geriatric issues successfully addressed for participants in intervention group.
Grades 3–5 chemotherapy treatment toxicity using the Common Terminology Criteria for Adverse Events v4.0344 and treatment completion rate (number of cycles received) will be abstracted from the medical chart (provider record).
Unscheduled hospitalisation and emergency department visits, and visits to the family physician abstracted from patient diary and medical chart.
Patient and provider satisfaction using surveys (patients) and interviews (providers).
Cancer treatment plan modification (brief survey filled out by oncologist).
Overall survival at 6 and 12 months (charts).
Intervention fidelity by healthcare setting (see Section 10).
Data on the cancer diagnosis, and treatment received during the 12 month period will be retrieved from the medical chart.
Sample size
Using the clinical minimally important difference of 10 points on the EORTC QLQ C30 global quality of life scale,45 a sample size of 350 is needed to provide 80% power, with alpha set at 0.05, to detect significant clinically meaningful change in quality of life scores, assuming a 20% attrition rate. This sample size will also give us 80% power to examine the cost-effectiveness of this intervention.46 Recruitment began in March 2018 and is estimated to take 12 months.
Statistical analyses
Baseline characteristics will be summarised for each group using descriptive statistics. Baseline differences will be evaluated using independent t tests for continuous and χ2 tests for categorical variables. Any potential confounding variables that display clinically important differences between the groups (eg, frailty level as measured with Geriatric Risk G8 screening tool, comorbidity level) will be considered for inclusion in multivariable models. An independent statistician at the Faculty of Nursing, will conduct the statistical analyses, based on an intent-to-treat approach.
Primary outcome
We will use a latent variable framework to test if change in quality of life from baseline to 3 months varies by group allocation.47 This analytic strategy has the advantage of being able to address both cross-sectional and longitudinal measurement error, as well as accounting for missing data over time using Full Information Maximum Likelihood.48 As study dropout may not be random in the context of the proposed trial (ie, the missing data mechanism, declining quality of life, may be related to the missing values), we will analyse the data using two types of models as recommended.47 First, a growth curve model (which is based on the assumption of data missing at random) will be specified to obtain an estimate of the slope regressed on group allocation; both linear and non-linear patterns of change will be considered. Next, a pattern mixture model, which extends the growth curve model by explicitly accounting for drop out over time, will be specified in a similar manner.47 Results of both modelling strategies will be reported.
Trial-based cost-effectiveness analysis
We will conduct a within-trial cost utility analysis using standard methods, focusing only on interventions directly evaluated in the trial49 from both payer and societal perspectives. The time horizon will be 12 months. Outcomes will be reported as quality-adjusted life years (QALYs) and cumulative costs, in undiscounted (short time horizon) 2016 Canadian dollars.
Costs: We will estimate costs for all healthcare use in both arms, including: (a) the intervention; (b) physician services; (c) hospitalisation, emergency visits and day surgery; (d) outpatient diagnostic tests; (e) drugs, including drug costs unrelated to cancer; (f) home care; (g) long-term care; (h) health-related out-of-pocket costs and (i) productivity costs. Utilisation will be estimated from chart reviews and patient diaries.50 Valuation will be conducted using province-specific estimates when possible (eg, schedule of physician benefits, cost per weighted case) and standard methods (eg, Ontario Health Insurance Plan schedule of benefits, resource intensity weights and average cost per weighted case).51 Productivity losses will be valued both by the human capital (with adjustment for labour force participation) and friction cost methods.52
Outcomes: QALYs will be estimated based on patients' responses to the EQ-5D-5L health-related quality of life questionnaire53 collected monthly for the first 6 months, and at 9 and 12 months. The EQ-5D-5L provides a description of a patient’s health state, to which a utility score derived from a set of preference weights measured in a representative sample of the Canadian population can be applied. The EQ-5D-5L weighted utility scores at each time-point will be used to estimate QALYs following standard procedures.54
Analysis: Cumulative costs and QALYs for each trial arm will be estimated and compared in order to calculate the incremental cost utility ratio, and incremental Net Health Benefit. Censoring for both outcomes will be handled through inverse probability weighting.55
We will evaluate uncertainty and estimate confidence intervals around the estimates, using both deterministic and probabilistic methods. We will account for correlation between costs and health outcomes using appropriate bivariate methods.49 Cost-effectiveness acceptability curves will be used to graphically represent the probability that the intervention would be cost-effective for cost-effectiveness thresholds of $20 000, $50 000 and $100 000 per QALY gained (multiple thresholds for sensitivity analyses). Reporting will follow the Consolidated Health Economic Evaluation Reporting Standards statement.56
Other secondary outcomes
For functional status, we will calculate the proportion of patients with one or more impairments in each group and compare across time using a logit mixed model.57 We will use descriptive statistics for the proportion of geriatric issues successfully addressed and cancer treatment modification. For all other secondary outcomes except survival, we will use t tests for continuous and χ2 test for categorical variables to test for any differences between intervention and control group. We will use Kaplan-Meier survival curves and the Log Rank test to see if there are differences in time to death between the groups followed by a multivariable Cox regression model.
Process evaluation
We will conduct a process evaluation (see table 4) as recommended by the Medical Research Council Framework58 involving all key stakeholders. According to this framework,58 the process evaluation in an effectiveness study of a complex intervention should evaluate the quantity and quality of what was delivered taking into account that a larger-scale study leads to greater variation in participation characteristics as well as different contexts where the intervention is implemented. A process evaluation aims to understand how this greater diversity impacted the implementation and effect of the intervention. The process evaluation will include a description of the fidelity, dose delivered (completeness), dose received (adherence to the recommendations and satisfaction), reach (participation rate), recruitment and context. We will collect data through chart reviews of all participants and interviews with a sample of clinicians from all study centres. We will explore if intervention fidelity is similar across our different clinical sites (those with experienced geriatric oncology teams (Princess Margaret Cancer Centre/Mount Sinai Hospital and the Jewish General Hospital), sites with geriatrics and oncology with limited collaboration prior to this study (Odette Cancer Centre, St. Mary’s Hospital, and the Fraser Valley Cancer Centre Surrey in collaboration with the Royal Columbian Hospital), and sites with no current such collaboration (R.S. McLaughlin Durham Regional Cancer Centre, and the Ottawa Hospital Cancer Centre). We will include a one-item satisfaction with all patient surveys at 3, 6, 9 and 12 months (not all time points to reduce participant burden). We will conduct semi-structured interviews with a selection of clinicians (both oncologists and intervention team members) to assess satisfaction with the intervention; 4–5 of each group per site, which with seven sites should lead to data saturation.59 If differences between clinical sites are noted, we will recruit more participants until data saturation per site is reached. We will use descriptive analysis for the quantitative data collected such as recruitment and retention, and adherence rates, etc. The qualitative data will be analysed using content analysis60 to assess fidelity and satisfaction with the intervention.
Details on process evaluation using the Medical Research Council Framework58
Patient and public involvement
In our previous conducted phase II RCT, we conducted a process evaluation where all participants (older adults and oncologists) were invited to provide feedback on the data collection methods used in that study and their recommendations for a future larger study.17 This feedback was used (eg, preference for telephone interviews/face-to-face follow-up interviews during treatment instead of self-administered surveys by mail as they get lost) together with the study results (eg, monthly follow-up to be able to better the trajectory in the main outcome quality of life instead of 3-month follow-up with missing follow-up data) to design the current protocol. During the development of this study, there were four older adults with cancer involved in the study design. One of them was a member of our phase II study, and three were older adults who signed up to the participant pool developed as part of the Senior Toronto Oncology Panel study.61 All four were involved at the writing of the grant proposal, they all have read and commented on the study protocol, were involved in discussions about how to collect the data. They provided their input on the burden to participants and encouraged to do to ask the older adult about their preference for method of data collection (in person or by telephone) and thus all their suggestions were incorporated in our study protocol. They vetoed all materials that are used/provided to older adults. They selected the token of appreciation in that will be provided to older adults during the study for completing interviews. They have edited all our healthy ageing booklets that will be provided to older adults. The outcomes were selected based on the researcher’s team review of the literature that older adults considering cancer treatment if it improves their quality of life38 as well as the aim of the intervention is to improve function,9 and experts around the world that recommend using quality of life/functional status outcomes.39 62 The older adults are not involved in the data collection of the study. The two remaining older adults are involved in the design and content of the quarterly newsletter that will be provided to our older adult participants to enhance retention. Our older adults will be involved in the development of lay summaries to disseminate our findings and we will provide them with the opportunity to present the findings at meetings but this will be determined once the study has been completed.
Ethics and dissemination
All participants will provide informed consent prior to enrollment (see online supplementary appendix 1 for the sample Informed consent form).
Supplemental material
We plan to disseminate our findings using a targeted approach aimed at clinicians, researchers, policy-makers and funding agencies: (1) presentations at key national and international oncology and geriatric medicine meetings; (2) media press-releases and interviews; (3) through the website and media relation divisions of the Canadian Cancer Society Research Institute, SIOG, etc) and (4) presentations to clinicians at each site.
To facilitate implementation of the intervention in routine clinical care, we will present our findings first to the study participants, their families, the clinicians and healthcare administrators.
Discussion
Currently, there are several randomised trials ongoing that are examining the benefits of implementing geriatric assessment and management for older adults with cancer (see for overview table 3 in ASCO geriatric oncology guideline7). Of the three, other ongoing trials listed in the ASCO geriatric oncology guideline table 3, three will be conducted in the USA, ours in Canada and one in France. Our intervention model is very similar to the PREPARE study led by Dr Soubeyran (https://clinicaltrials.gov/ct2/show/NCT02704832) in which participants aged 70 years and over with first and second-line treatment are eligible and the delivery of the geriatric assessment and management will be done by a geriatrician and study RN. In addition, our 5C study’s primary endpoint has as primary endpoint quality of life, similar to the PREPARE study who has as co-primary endpoint OS. The three US-based studies led by Dr Hurria (https://clinicaltrials.gov/ct2/show/NCT02517034) and Dr Mohile’s studies (https://clinicaltrials.gov/ct2/show/NCT02107443 and https://clinicaltrials.gov/ct2/show/NCT02054741) use oncology care professionals to deliver the intervention and focus on chemotherapy toxicity as primary outcome. In our study, we chose the primary outcome based on the recommendations that quality of life is an important endpoint for studies with older adults and this is also one of the most important considerations to consider receiving chemotherapy.
In this study, we have chosen to exclude those patients who are already receiving palliative care services on recruitment to avoid burdening the patient as well as it will confound our intervention effect as they receive additional care to their usual oncology care. While geriatrics and palliative care do not provide identical services, both use a comprehensive assessment of the patient and address issues with the aim of improving quality of life. We will include patients who have received up to one cycle of chemotherapy, as many older adults cannot decide on study participation until they have clarity about their treatment plan. The intervention is still expected to benefit them in terms of quality of life during treatment.
Our study will be examining cost-effectiveness which has not been included in the other ongoing studies. This is highly relevant to the publically funded healthcare system in Canada for implementation in routine clinical practice. In addition, in this study we have included two cancer centres who do not have onsite geriatricians. These sites will be collaborating with the intervention team in Toronto. In our process evaluation, we will study whether there is a difference in the different intervention delivery methods. However, this requires an adequate sample for whom this telegeriatrics mode was used and thus we may not be able to do it. The other centres are tertiary cancer centres thus our final recruited sample may be biased and not representative of community cancer centres. However, this study with recruitment at eight centres across three provinces in Canada in both English and French in a study in which patients have involved in the design will hopefully recruit a representative sample of older adults with cancer considering cancer treatment in Canada.
Acknowledgments
We would like to thank our older adult representatives Mr Andrew Choate and Mr Andrew Orr (deceased).
References
Footnotes
Contributors MTEP, SB, NK, SMHA: conception and design, data collection, data analysis and interpretation, writing of the manuscript and approval of final article. TH, CM, JM, DW-C-W, MKrz, EA, CE, RJ, AP, MKra, FB, SB, RK, ML, ES, JZ, SF, AL, UE, RM, KF: conception and design, data analysis and interpretation, writing of the manuscript and approval of final article. EP and JR: conception and design, writing of the manuscript and approval of final article. HB: data collection, data analysis and interpretation, writing of the manuscript and approval of final article.
Funding The 5C study is funded by the Canadian Cancer Society (grant #705046). MTEP is supported with a Canada Research Chair in Care of Frail Older Adults
Competing interests None declared.
Ethics approval We have obtained research ethics approval from the Ontario Institute of Cancer Research Ethics board (REB; one application for all five cancer centres located in Ontario), the Jewish General Hospital (which also is the REB for St. Mary’s Hospital) and the Royal Columbian Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.