Article Text

Abstract
Objectives To understand how and why effective multi-chronic disease management interventions influence health outcomes in older adults 65 years of age or older.
Design A realist review.
Data sources Electronic databases including Medline and Embase (inception to December 2017); and the grey literature.
Eligibility criteria for selecting studies We considered any studies (ie, experimental quasi-experimental, observational, qualitative and mixed-methods studies) as long as they provided data to explain our programme theories and effectiveness review (published elsewhere) findings. The population of interest was older adults (age ≥65 years) with two or more chronic conditions.
Analysis We used the Realist And MEta-narrative Evidence Syntheses: Evolving Standards (RAMESES) quality and publication criteria for our synthesis aimed at refining our programme theories such that they contained multiple context-mechanism-outcome configurations describing the ways different mechanisms fire to generate outcomes. We created a 3-step synthesis process grounded in meta-ethnography to separate units of data from articles, and to derive explanatory statements across them.
Results 106 articles contributed to the analysis. We refined our programme theories to explain multimorbidity management in older adults: (1) care coordination interventions with the best potential for impact are team-based strategies, disease management programmes and case management; (2) optimised disease prioritisation involves ensuring that clinician work with patients to identify what symptoms are problematic and why, and to explore options that are acceptable to both clinicians and patients and (3) optimised patient self-management is dependent on patients’ capacity for selfcare and to what extent, and establishing what patients need to enable selfcare.
Conclusions To optimise care, both clinical management and patient self-management need to be considered from multiple perspectives (patient, provider and system). To mitigate the complexities of multimorbidity management, patients focus on reducing symptoms and preserving quality of life while providers focus on the condition that most threaten morbidity and mortality.
PROSPERO registration number CRD42014014489.
- multimorbidity
- older adults
- complex interventions
- realist review
- chronic disease management
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
To our knowledge, this is the first realist review to explain why multimorbidity interventions work, for whom, and under what circumstances to improve outcomes for older adults with multimorbidity —findings can be used to inform practice and policy decisions in the management of older adults with multiple chronic conditions
Our search strategy was in part informed by a systematic review investigating the effectiveness of multimorbidity interventions for older adults that we conducted alongside this realist review.
We created a 3-step synthesis process drawn from meta-ethnography to separate units of data from articles, and to derive explanatory statements across them.
Many of our included studies did not have complete data to enable optimised investigation of context-mechanism-outcome (CMO) configurations.
Incomplete reporting also impacted our ability to fully test our theories and therefore, we could not completely elucidate the interrelationships within and between all of our CMO configurations.
Background
The global population is ageing, with 2 billion people expected to reach 60 years of age and older by 2050.1 2 It is now more common for older adults to have multiple chronic diseases than to have single diseases or no chronic medical conditions at all.3 The burden of chronic disease is also on the rise globally1 4 with more than half of older adults (age ≥65 years) living with high-burden chronic conditions (ie, highly prevalent and associated with premature death and increased healthcare utilisation).3 5 Older adults also have greater healthcare needs, are at higher risk for adverse health outcomes, and experience more frequent hospitalisations,6 yet only 55% receive appropriate care.7 8 In response, different chronic disease management (CDM) interventions have been created. For example, a programme designed to encourage older adults with Chronic Obstructive Pulmonary Disease (COPD) and depression to adhere to antidepressants and pulmonary rehabilitation.9 Although promising, CDM interventions have shown varying effectiveness10 11 in part, because they are not usually developed for older adults or created for sustained use; and very few are designed to deliberately address multimorbidity.8 12
Given our rapidly ageing population, there is an urgent need to understand how and why multimorbidity interventions influence health outcomes to optimise patient care. To address these gaps, we conducted a systematic review to identify effective CDM interventions that integrate the care of ≥2 high-burden chronic diseases affecting older adults (published elsewhere).13 However, a systematic review is not always enough to inform practice and policy decisions as knowing ‘what’ works seldom reveals which desired outcomes may occur under different contexts. Our objective was to conduct a realist review alongside to explore the underlying mechanisms and contexts by which these CDM interventions work or do not work, for whom, under what circumstances and why.14 Realist review is particularly relevant for making sense of complex interventions (such as those focusing on CDM) that have context-sensitive outcomes. It can add important contextual and mechanistic detail to existing knowledge on this topic.15 Such detail is likely to contribute to the limited existing clinical practice guidelines on multi-morbidity management such as those developed by National Institute for Health and Care Excellence (NICE),16 by explaining the contexts in which intended and unintended outcomes are likely to occur. Additional resources about realist reviews can be found the RAMESES Project website.17 Our overall objective of this review is to: understand how and why effective CDM interventions influence health outcomes in older adults 65 years of age or older.
Methods
Study design
Our protocol was published18 and registered with PROSPERO registration number. We applied the RAMESES quality19 and reporting criteria.20 The systematic review methods and findings are reported elsewhere.13
Programme theory development
To identify our initial programme theories (ie, what multimorbidity interventions are composed of, how and why they are expected to work and what outcomes they might generate), we used an iterative, consensus-based process. We considered two major sources to identify any published or unpublished literature21: (1) Medline and Google Scholar describing models, frameworks, theories of multimorbidity, CDM and complex interventions and (2) content and methods experts on our team (geriatricians, family physicians, and health services and realist review experts). Duplicate screening of 97 reports by two reviewers identified 18 documents that contained data that helped us to understand CDM interventions. Through team discussion and a Delphi survey among our team, we identified that our initial programme theory would have to incorporate the following concepts: (1) CDM interventions are complex interventions that do provide different outcomes in different settings; (2) health prioritisation is an important aspect of multimorbidity and (3) interventions that consider patient values and circumstances, the evidence and the clinician’s expertise were more likely to produce desired outcomes. We then used the data from our included studies to gradually refine our understanding of these concepts and how (if at all) they fit into our more refined programme theory developed from this review.
Search strategy
Since we performed our realist review alongside our systematic review of multimorbidity interventions,13 the search strategy was done simultaneously for both reviews. As such, we identified potentially relevant articles for our realist review (ie, to provide data to test our programme theories) through our systematic review search strategy (inception to December 2017)13 and performed additional iterative, targeted searches as needed for the realist review.19 An experienced information specialist performed these additional searches in Medline and Embase (online supplementary appendix 1).
Supplementary file 1
Selection and appraisal of documents
To increase the efficiency of our searching and screening process, reviewer pairs independently screened titles and abstracts simultaneously for both the systematic review and realist review. We considered any study design for inclusion (ie, experimental quasi-experimental, observational, qualitative and mixed-methods studies). During full-text screening, we considered all articles that were identified for the systematic review as well through additional targeted searches to explain our programme theories and effectiveness review findings. Two reviewers independently assessed each article for relevance (does the source contain any data that could be interpreted as having our relevant context, mechanism or outcome for programme theory development?) and rigour (How trustworthy are the data? Does the article provide enough detail on how conclusions were reached irrespective of study design?).
Data extraction
We created and pilot tested a standardised data extraction form. Data items were driven by our purpose to refine our programme theories through context-mechanism-outcome (CMO) configurations (ie, if we were able to infer an explanation for the cause [M] for a particular outcome [O] under the influence of one or more particular contexts [C]). For example, computer-based counselling systems (intervention) targeting older adults and providers in primary care (C) are not acceptable (O) if they do not show any relative advantage over the current system (M1) and if inconsistent with providers’ current practice workflow (M2). After extracting excerpts in duplicate, reviewer pairs independently assigned an associated concept code and iteratively developed a codebook of concepts (online supplementary appendix 1) that was used to code subsequent excerpts; any discrepancies were discussed and resolved as a team.
Analysis and synthesis processes
We used the RAMESES quality19 and publication20 criteria to guide the synthesis. Our goal was to refine our programme theories such that they contained multiple CMO configurations describing the ways different mechanisms fire to generate outcomes. We created a 3-step synthesis process grounded in meta-ethnography22 to separate units of data from articles, and to derive explanatory statements across them. Step 1: Reviewer pairs independently extracted relevant excerpts from articles. Step 2: One reviewer sorted excerpts by concept for each study and developed consolidated statements (groups of CMO configurations) for each. A second reviewer audited the first reviewer’s statements by checking for agreement and consistency with their own interpretations. Step 3: As a team, we examined and compared consolidated statements across studies to derive explanatory statements. These were then used to refine our programme theories aimed at explaining the outcome patterns we found within the effectiveness review. When the consolidated statements seemed to disagree, we unpacked the concepts and further examined them, consulting our literature and content experts as necessary for additional data and insights.
Deviations from our protocol in conducting our realist review
We followed the methods as outlined in our protocol18 with a few exceptions. First, we switched to an auditing process during Step 2 of the analysis to make our process more efficient. This involved an auditor checking the work of a primary reviewer. Second, since our process to finalise the list of initial programme theories identified an area that was not covered by our systematic review search (ie, health prioritisation), we added a secondary search strategy to capture this literature as described above.
Patient and public involvement
Patients were not involved in the conduct of the review but older adults with multiple chronic conditions are involved in developing key messages for this research. These patients are also part of our broader integrated knowledge translation team to co-design an electronic self-management tool that integrates the care of multiple chronic conditions (KeepWell); this tool is being informed by this review.
Results
Study characteristics
Figure 1 is our Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram, which shows the flow of article selection. Of 2435 potentially, relevant citations that were screened for relevance, 124 articles were reviewed in full-text, and 106 articles contributed to the analysis.3 9 15 23–125 Studies were published between 2002 and 2016 mostly in the USA (n=32), the UK (n=19), Canada (n=14), Germany (n=11) and Australia (n=10). Most of the articles (75%) were about multimorbidity (n=50) or disease prioritisation (n=29), and 27 studies (25%) addressed specific chronic disease combinations.

Flow of article selection for the Realist Review.
Programme theories
Using data from our included studies, we iteratively developed and refined our initial two programme theories and a third programme theory that emerged from our data. To make our findings more succinct, in the following paragraphs, we have provided narratives that summarise the most important aspects of our programme theories. This approach obscures the detailed CMO configurations that underpin these narratives and may make our manuscript less useful for those interested in realist review methodology. To address this issue, we have provided indications of the CMO configurations that our narratives are based on. For those interested in seeing the links between our data and CMO configurations, please see online supplementary appendices 3–6 that explains the outcomes that may be achieved by the different intervention strategies used in care coordination under different contexts.
Programme theory 1: Care coordination interventions for multimorbidity management
Almost one-half of the interventions described in our realist review were ‘care coordination’ interventions (ie, changes in how healthcare workers interact with each other or patients to ensure timely and efficient delivery of healthcare).126 Online supplementary appendix 3 shows their detailed CMO configurations that underpin this programme theory. Overall, we found that care coordination interventions in primary care are effective for older adults with multimorbidity because they represent a structured approach to holistic care. They address multiple conditions through interdisciplinary teams or multidisciplinary disease management, providing specific processes for communication and establishing formal roles for providers and patients. We identified three types of care coordination approaches that healthcare providers may wish to use that have potential for impact: (1) Team-based or collaborative approaches involve highly trained clinicians53 providing holistic and coordinated care88 including spending time with patients to discuss all their concerns, and to prevent care overlap and gaps.80 Patients are given education, counselling and other support services to address their disease(s), medications, and lifestyle.44 Team-based approaches can provide access to specialists53 and a wider range of services, and provide evidence-based care solutions for multiple conditions in parallel (not in tandem).38 Optimised care outcomes are most likely to occur through interdisciplinary communication and collaboration,38 81 when teams comprise highly trained and skilled members53 who understand and accept each other’s roles,53 provide opportunities38 88 and time53 to share information,81 and collaborate on patient care.38 45 53 88 Other contexts in which mechanisms are likely to be triggered include teams that have dedicated members who provide additional support to patients38 53 or providers,81 receive training,38 53 81 and have a robust and well-functioning communication system.38 45 (2) Disease management programmes follow a ‘script’ for how to provide effective patient care via care protocols or plans, which define the division of tasks, support the follow-up and coordination of action,103 110 and help to sustain a philosophy of common care.45 Systematised care is achieved through checklists, follow-up timetables45 103 110 and treatment targets,45 which can lead to a shared philosophy of care45 103 and optimised decision making.45 (3) Case management: Case managers are trained healthcare professionals who are the main contact (and conduit of information) between a patient and involved providers,53 and most appropriate for multimorbidity management when there may be multiple and diverse providers involved in a patient’s care. When case managers are the primary contact,80 103 care is perceived by patients as continuous,78 79 coordinated79 and more individualised,9 80 and fosters the development of the skills and confidence patients need to self-manage their health.78
Programme theory 2: Disease prioritisation in multimorbidity management
The detailed CMO configurations of disease prioritisation that underpin this programme theory are described in online supplementary appendix 4. Multimorbidity management is perceived as confusing for patients and overwhelming for providers due to the heterogeneous nature of multimorbidity,102 disease and treatment interactions and possible conflicts,57 92 and the difficulty of attributing symptoms to conditions.57 Multimorbidity can create a cognitive and emotional overload in patients and providers,64 so a common strategy they use is to focus on one condition at a time. Patients and providers focus their attention by prioritising one condition over another for a specified period of time, or until particular outcomes are achieved.64 91 However, patients and providers approach prioritisation differently. Patients make prioritisation judgements based on the symptoms they experience and need the most attention. They identify the most undesired symptoms and focus on their associated condition(s)32 56 63 66 68 125 or those that threaten their social activities,25 63 76 limit their independence25 91 and have potentially severe long-term consequences if not addressed.63 91 Providers prioritise conditions based on their judgements about the prognosis or severity of the condition and place greater emphasis on conditions with more serious outcomes25 57 66 68 76 125; they focus on conditions that threaten a patient’s morbidity and mortality,25 57 66 68 125 those they think they are better equipped to address (eg, physical over emotional32 124), and whether the patient is likely to benefit from treatment.57 114 124 125 What’s common among patients and providers, is that they both consider conditions that they feel capable of addressing,64 91 124 125 and both consider the cascading effects of multimorbidity and the interrelatedness of these conditions during the prioritisation process.65 91 For patients, the cascading effects of multimorbidity are particularly challenging. Patients may find it difficult to determine which chronic disease is causing a particular symptom because conditions may share similar symptoms72 or the treatment of one condition may aggravate the other61 62 90 91 or cause other antagonistic effects.64 90 91 Self-management is therefore a challenge for patients because the diagnosis of (and receipt of information) about a new condition compounds the complexity and uncertainty of what to do.87Figure 2 shows our conceptualisation of optimised disease prioritisation from the perspective of providers and patients. For this simplified overall programme theory, we have analysed and interpreted our findings in such a way as to provide a programme theory that presents out findings in a more familiar format using the concepts of ‘barriers’ and ‘facilitators’. The programme theory sets out the factors that need to be taken into account if providers and patients wish to optimise disease prioritisation. In particular we provide an overview of factors that healthcare providers may need to address to help patients to: (1) identify what symptoms are bothering them; (2) why they bother them and (3) exploring options that are acceptable to them for addressing their symptoms.
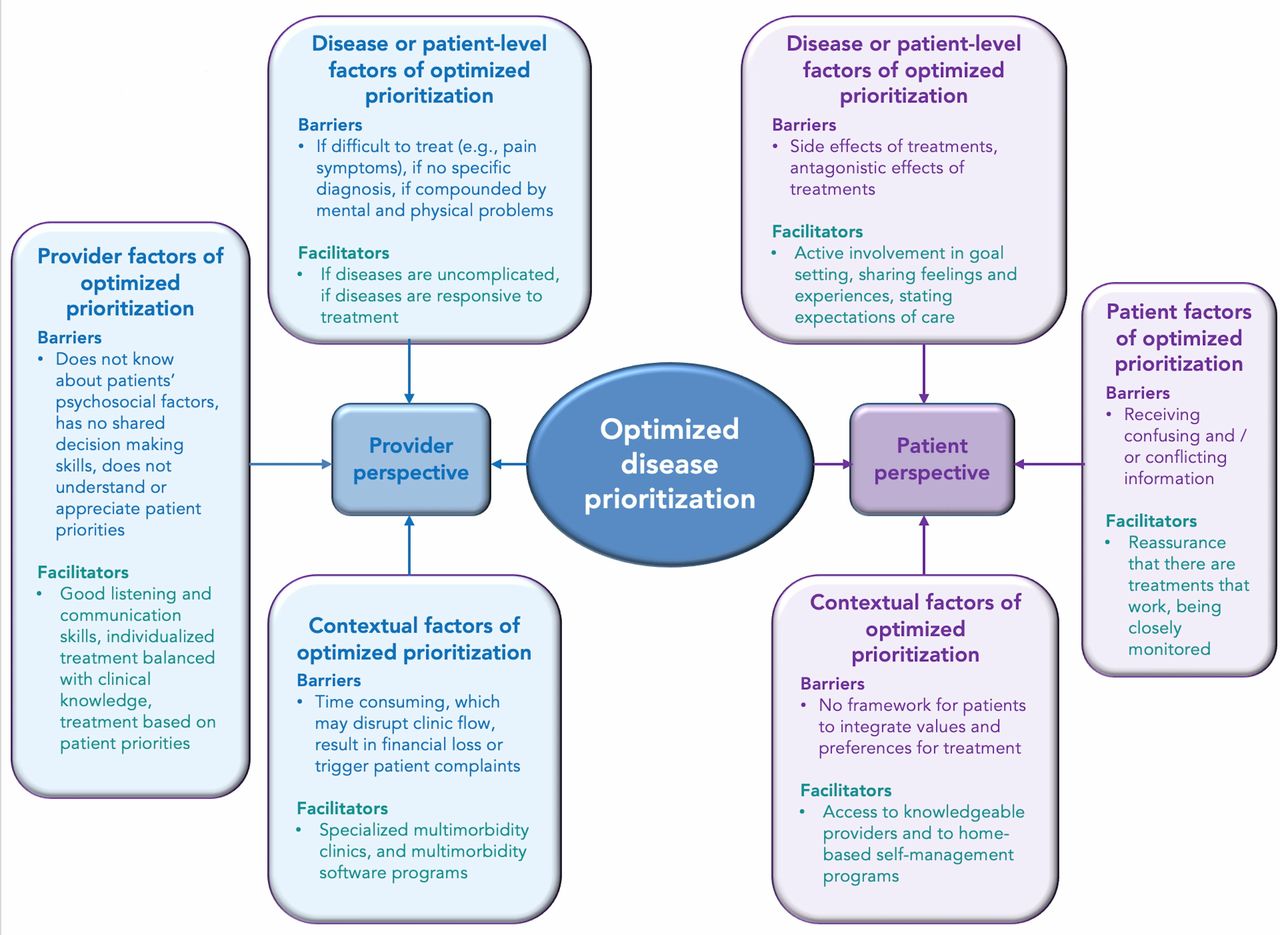
Framework of optimised disease prioritization in multimorbidity management. A simplified overarching programme theory of identifying factors (conceptualised as barriers and facilitators) that need to be considered by patients and providers when trying to optimise disease prioritization.
Programme theory 3: Patient self-management in multimorbidity
The detailed CMO configurations of multimorbidity self-management that underpin this programme theory are in online supplementary appendix 5. Multimorbidity is perceived by patients as a burden because of the volume of information and recommendations provided51 74 which are often inconsistent or conflicting, and the cognitive and emotional overload required to assimilate this information or to make lifestyle changes.87 Subsequently, this can lead to confusion and non-adherence to recommendations25 43 91–93 and may also trigger cognitive and emotional overload. Specific explanations to these outcomes include (1) self-management regimens are designed to fit their condition rather than their health priorities, lifestyle and available resources89 94; (2) prescribed medications are unwieldy (too many, taken often, and difficult to keep track of)15 51 or mismanaged71; (3) difficulties with following the required diet and exercise routine36 51 91; and to see multiple providers71; (4) not knowing how to respond to adverse drug effects15 71 and (5) experiencing communication barriers due to linguistic and cultural diversity.71 Self-management is especially challenging for older adults with cognitive impairment89 or anxiety90 in addition to other chronic conditions, as these contexts can interact to increase people’s perceived illness burden.63 In particular, if depression is the additional condition, older adults may choose not to do anything at all because they either consider it a normal part of ageing or reluctant to seek treatment due to the stigma associated with mental health problems.30 Depression, as a context, can therefore also trigger additional mechanisms that reduce a patient’s ability to self-manage chronic conditions30–32 59 64 87 91: reduced motivation, energy, self-efficacy and feelings of hopelessness,31 and stress.87 A number of feedback loops are activated because illness burden can interfere with a person’s ability to engage in health promotion (eg, exercise). This can lead to negative consequences (eg, weight gain,87 reduced quality of life, functional decline), and in turn impair mood, social networks, and self-management behaviours.62 Multimorbidity self-management is also influenced by the lack of available resources64 (eg, adequate finances,62 91 social supports23 62 88 89 91 or transportation91) or low health literacy29 or skills to manage adverse effects.43 90 Older adults are interested in self-management tools that provide health condition information51; share, coordinate and synthesise information with and between providers; and connect them with other patients.51 Physicians can support this by tailoring information to the stage of the patient’s condition,26 having interactions with patients,93 providing information93 and fostering a collaborative approach to care.115
Discussion
In this realist review we developed and refined our programme theories to explain why coordination of care interventions (found to have the most potential for impact in our systematic review) work to improve outcomes for older adults with multimorbidity. Care coordination interventions may be effective in primary care because they represent a structured approach to comprehensive care, and address multiple conditions through interdisciplinary teams or multidisciplinary disease management by providing specific processes for communication, and establishing formal roles for providers and patients. Team-based approaches provide the right care at the right time, disease management offers a systematised approach to care, and case management offers a dedicated case manager as the conduit of care.
In addition to refining our programme theories, we generated explanations associated with these theories. Online supplementary appendix 6 shows the CMO configurations to explain of multimorbidity management overall. Figure 3 shows our conceptualisation of multimorbidity management, which suggests that optimised care requires both clinical management and patient self-management, with the caveat that each needs to consider identified challenges from the perspective of those affected by them (patient, provider, system). From the patient perspective, clinical management can be confusing due to conflicting messages, which is compounded in the presence of depression, impaired cognition, or poor health literacy. The mental health needs of patients can further complicate clinical management by impeding selfcare, creating communication barriers with providers (eg, patient complaints may not be clear), and patients receiving less intensive treatment. Self-management is difficult for patients because of the high burden of required lifestyle changes and adherence to multiple and often conflicting treatment regimens. Multimorbidity can also have cascading effects due to the nature of how chronic diseases are interrelated and the influence of a patient’s mental and emotional health on self-management. From the provider perspective, clinical management of multimorbidity may be perceived as overwhelming because of the heterogeneous nature of multimorbidity, and conflicting or lack of evidence to guide clinical decision making. Lack of skills and confidence, not having decision support systems and protocols that are too rigid can also lead to inadequate preparation to manage multimorbidity. From a system perspective, even if primary care is the optimal setting for multimorbidity management, it may not always have the infrastructure to support optimal strategies such as care coordination and can also lead to fragmentation of care.

{kind=link}
{kind=link}
{kind=link}
Framework of optimised multimorbidity management . A simplified overarching programme theory identifying factors (conceptualised as barriers and facilitators) that need to be considered when trying to optimise multimorbidity management from the patient, provider and system perspective.
Recommendations
Findings from programme theory 1 suggests that healthcare providers may wish to use care coordination interventions that are: (1) Team-based or collaborative approaches that involve highly trained clinicians providing holistic and coordinated care through effective interdisciplinary communication and collaboration, and the provision of education and counselling to patients to address their disease(s), medications and lifestyle; (2) Disease management programmes via care protocols or plans, checklists, follow-up timetables and treatment targets and (3) Case management strategies for situations when there may be multiple and diverse providers involved in a patient’s care. For programme theory 2, the specific types of disease prioritisation approach that healthcare providers may wish to consider is to work with patients to identify what symptoms are bothering them and why, and exploring options that are acceptable to both clinicians and patients for addressing their symptoms. For programme theory 3, the specific types of self-management approach that healthcare providers may wish to consider include not assuming that all patients are capable of selfcare, identifying who is capable of selfcare and to what extent, and establishing with the patient what they need (eg, information, support) to enable selfcare.
Strengths and limitations
To our knowledge, this is the first realist review investigating older adult multimorbidity aimed at explaining why effective multi-CDM interventions (identified through a systematic review13) work/do not work for whom, under what circumstances and why. This can better inform practice and policy decisions about multimorbidity management than a systematic review alone. A Cochrane review investigated interventions in multimorbid patients of any age15 and found mixed results, but concluded that interventions that were integrated with care and targeted specific risk factors or functional difficulties may be more effective.15 A rapid realist review investigating the underlying mechanisms of care planning strategies found that the mechanisms driving positive outcomes for people with long-term conditions are those that motivate them and promote an understanding of their role in self-management and how their lifestyle affects their conditions.127 Our findings build on these studies by providing explanations for why multimorbidity interventions may be effective for older adults. Additionally, we focused exclusively on older adults because they represent a relatively unstudied population, and given their projected population growth, they urgently need our attention to optimise their care. NICE guidelines on clinical assessment and management of multimorbidity16 (one of few existing multimorbidity guidelines) support many of our findings. They emphasise the need to find synergies in care regimes and simplifying care where possible. They also describe a preferred approach to care, which involves establishing patient goals, values and priorities, where patients are encouraged to describe their preferred decision making approach and what aspects of their life they prioritise.16 A recent qualitative systematic review also highlights the need for providers to simplify the burden of care for multimorbid patients.128 Our findings highlight the importance of focusing multimorbidity management by prioritising one or more specific condition(s) and ensuring that prioritisation is undertaken in collaboration with patients.
Our study has some limitations. First, it is possible that other teams may have identified different programme theories or interpretations. However, we used a rigorous and systematic process, and we let our data guide our interpretations. Second, many of our included studies did not have complete data to enable optimised CMO investigations. This may in part be due to an over-emphasis on effectiveness research in the literature, and an under-representation of qualitative inquiry, particularly about elucidating ‘mechanisms’. For example, the literature rarely addressed the social determinants of health (a potentially significant trigger for multimorbidity outcomes) even though many older adults experience social isolation129 and financial130 challenges. Incomplete reporting also impacted our ability to fully test our theories. As such, while we developed and refined a number of explanations for our data, we could not completely elucidate the interrelationships within and between all of our CMO configurations. Finally, it is important to note that since this analysis was interpretive and inductive, it is possible that another team of researchers would have arrived at a different set of programme theories that incorporate the mechanisms and contexts of multi-CDM interventions for older adults. Thus, these findings should only be used as potential mid-range theories to explore and interrogate.
Conclusions and future directions
Our realist review contributes to the current, limited knowledge of the underlying mechanisms of complex multi-CDM interventions for older adults with multimorbidity. We found that care coordination interventions are effective because they represent a structured approach to holistic care. To mitigate the complexities of multimorbidity management, patients focus on reducing their undesired symptoms and preserving their quality of life, while providers focus on the condition that most threaten a patient’s morbidity and mortality. To optimise care, multimorbidity management requires both clinical management and patient self-management, and be considered from multiple perspectives (patient, provider and system).
Acknowledgments
In addition to our core research team, we would like to thank Becky Skidmore and Alissa Epworth for helping to develop and execute the search strategies for this review. We would also like to thank our Patient and Family Advisory Council members at North York General Hospital in Toronto, Ontario, who are helping to support the dissemination of findings from this review and are using findings to codesign a multimorbidity self-management tool for older adults (KeepWell).
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
Footnotes
Contributors MK: Manuscript development and final approval, methods design, data acquisition, data extraction, data analysis, research question development. LH: Manuscript development and final approval, data extraction, data analysis. GW: Manuscript development and final approval, methods design and data interpretation. YL: Manuscript development and final approval, data extraction, data analysis, methods. JM: Manuscript development and final approval, data extraction, data analysis, methods. VT: Manuscript development and final approval, data extraction, data analysis, methods design. JC: Manuscript development and final approval, data extraction, data analysis. JL: Manuscript development and final review, data extraction, data analysis. NMI: Manuscript development and final approval, methods design, data acquisition. JH-L: Manuscript development and final approval, methods design, data acquisition. SES: Manuscript development and final approval, methods design, data acquisition.
Funding This research was supported by an Ontario, Canada Ministry of Health and Long-term Care (MOHLTC) Health Systems Research Fund (HSRF) Capacity Award. The funder was not involved in conducting the realist review. Monika Kastner is funded by a Canadian Institutes of Health Research (CIHR) New Investigator Award. Geoff Wong is partly funded by The Evidence Synthesis Working Group of the United Kingdom’s National Institute for Health Research School for Primary Care Research (NIHR SPCR) [Project Number 390]. Noah Ivers is funded by a CIHR New Investigator Award and a Clinician Scientist Award from the Department of Family and Community Medicine, University of Toronto. Jayna Holroyd-Leduc is funded by a University of Calgary BSF Chair in Geriatric Medicine. Sharon Straus is funded by a Tier 1 Canada Research Chair in Knowledge Translation.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement We included most of the data generated or analysed for this study in this published article and associated appendices. Any additional datasets are available from the corresponding author upon request.
Patient consent for publication Not required.