Article Text

Abstract
Introduction Chronic lateral epicondylosis (CLE) of the elbow is a prevalent condition among middle-aged people with no consensus on optimal care management but for which surgery is generally accepted as a second intention treatment. Among conservative treatment options, ultrasound (US)-guided fenestration has shown encouraging results that should be explored before surgery is considered. The primary objective of this study is to compare the efficacy of US-guided fenestration with open-release surgery in patients with failure to improve following a minimum 6 months of conservative treatment.
Methods and analysis This study protocol entails a two-arm, single-blinded, randomised, controlled design. Sixty-four eligible patients with clinically confirmed CLE will be assigned to either US-guided fenestration or open-release surgery. Fisher’s exact test will be used to compare the proportion of patients reporting a change of 11/100 points or more in the Patient Rated Tennis Elbow Evaluation score at 6 months, according to an intention-to-treat analysis. Secondary analyses will compare the two treatment groups in terms of pain and disability, functional limitations at work, pain-free grip strength, medication burden, patients’ global impression of change and level of satisfaction at 6 weeks, 3, 6 and 12 months, using mixed linear models for repeated measures or Fisher’s exact test, as appropriate. Finally, recursive partitioning analyses will investigate US and elastography parameters as predictors of treatment success at 6 and 12 months. This data will contribute to evidence-based treatment guidelines for CLE and explore the value of imaging biomarkers to improve risk stratification plans and assist clinicians.
Ethics and dissemination The study has been approved by the Research Ethics Board of our institution on 23 March 2016 (REB 15.327). In case of important protocol modifications, a new version of the protocol with appropriate amendments will be submitted to the REB for approval. Study results will be published in peer-reviewed journals and presented at local, national and international conferences.
Trial registration number NCT02710682.
- elbow tendinopathy
- randomized controlled trial
- acoustic radiation force impulse imaging
- ultrasonography, interventional
- minimally invasive surgical procedures
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- elbow tendinopathy
- randomized controlled trial
- acoustic radiation force impulse imaging
- ultrasonography, interventional
- minimally invasive surgical procedures
Strengths and limitations of this study
This is the first randomised trial to compare the efficacy of ultrasound (US)-guided fenestration and open-release surgery for the treatment of chronic lateral epicondylosis (CLE).
This is the first study to explore the predictive value of shear-wave elastography in response to treatment by US-guided fenestration or open-release surgery, at 6 and 12 months following intervention.
This is the first study to prospectively evaluate the evolution of US findings, up to 12 months following treatment of patients with CLE.
While the generalisability of the results of this phase II study might be limited, the outcomes and evaluation of the processes used in this study will inform a multicenter, phase III definitive study.
Introduction
Chronic lateral epicondylosis (CLE) of the elbow, commonly known as tennis elbow or epicondylitis, is a debilitating condition with a prevalence of 1%–3% in the general population, most commonly affecting adults in their fourth and fifth decades of life.1 The socioeconomic burden of this disorder is substantial, with a yearly absenteeism rate as high as 5% in the working age population.2 Affected patients usually complain of pain just distal to the lateral humeral epicondyle and are likely to have a history of repetitive upper limb movements or of prolonged manipulation of heavy weights.1 2 The pathophysiology of CLE entails repetitive overuse, leading to microtears and progressive degenerative changes of the common extensor tendon, combined with ineffective healing mechanisms.3 Histopathological findings include collagen fibre disorganisation, neoangiogenesis, mucoid degeneration, fibroplasia and dystrophic calcifications, with invariable involvement of the extensor carpi radialis brevis (ECRB) component of the common extensor tendon.4 A CLE diagnosis is usually made clinically, with the elbow extended and the forearm in pronation, by pain provocation on palpation of the region of the lateral epicondyle, or using a resisted wrist or middle finger extension manoeuvre.5
Treatment of CLE: many options, no clear guidelines
The treatment arsenal for CLE is vast; however, no successful and universally accepted trajectory of care has been established and patient management remains deficient in many cases. Well-conducted conservative treatment that includes rest, stretching and strengthening exercises with emphasis on eccentric movements, combined with ergonomic interventions has been shown to provide pain relief in 80% of patients at 8–12 months.6 7 However, this approach may necessitate a prolonged reduction in stressful activities or extended absences from work that involves movements of the wrist extensors. Consequently, financial impacts are often important for workers and compliance with treatment may be suboptimal in those without compensated sick leave.
Corticosteroid injections are commonly used for the quick pain relief they provide, but studies have shown that, in the majority of cases, pain relief and physical functioning improvement is short termed, recurrence rate is high and prognosis may be worsened in the long term.8 9 Despite the growing evidence of their long-term inefficacy and potential deleterious effects, corticosteroid injections are still routinely used as part of the conservative management of CLE, mainly because they are easy to administer, inexpensive and provide pain relief, although of short duration.
Extracorporeal shockwave therapy may also be employed in the management of patients with CLE; however, systematic reviews have concluded that this approach provides little to no benefit in the treatment of chronic tendinopathy, including CLE, when compared with placebo.6 10
Hoskrud et al reviewed studies investigating the use of injections of platelet-rich plasma (PRP) (six studies), autologous blood (five studies) and sclerosing agents (14 studies) for treating various types of tendinopathy, including CLE and concluded that although these modalities may appear promising, the quality of evidence supporting their use is deficient.11 Other systematic reviews surveyed several individual experimental studies comparing the effectiveness of PRP injections to placebo, corticosteroid injections, autologous blood injections, local anaesthetic injections, tendon fenestration and exercise therapy for different types of tendinopathies, including CLE. They concluded that, at best, PRP injections moderately improve pain scores in the short to medium term but that the heterogeneity in study methodology and contradictory results preclude from recommending PRP injections for treatment of chronic tendinopathy.12–14
Ultrasound (US)-guided tendon fenestration for CLE
Tendon fenestration is a minimally invasive, low risk, dry-needling technique performed under direct US visualisation. After local anaesthesia of the skin and subcutaneous tissues, a needle is used to create micropunctures in the affected region of the tendon and to abrade the adjacent periosteum. The goal is to disrupt areas of tendinosis and cause local bleeding to stimulate physiological mechanisms of fibroblastic proliferation and tendon healing through scar remodelling.15 Hence, the rationale behind this treatment is to convert a chronic degenerative painful process into an acute inflammatory condition that can lead to tendon regeneration and healing.16 Bleeding that occurs within the tendon during the procedure delivers growth factors and inflammatory cells that are essential to initiate the first phase of tendon healing response. US-guided tendon fenestration has shown promising results in various chronic tendinopathies including CLE,17 18 patellar19 and gluteal tendinopathies.15 20 In a 2006 retrospective study, McShane et al reported 63.6% excellent, 16.4% good, 7.3% fair and 12.7% poor outcomes at a mean follow-up of 28 months, in 58 consecutive patients with CLE treated with US-guided tendon fenestration, combined with a corticosteroid injection.21 Two years later, in a retrospective study, the same authors reported on the results of US-guided tendon fenestration in a subsequent group of 57 consecutive patients with 57.7% excellent, 34.6% good, 1.9% fair, 5.8% poor outcomes at a mean follow-up of 22 months and concluded that a concomitant corticosteroid was not necessary. Comparison with other treatments aiming to increase growth factors within the tendon and stimulate the physiological healing processes, including PRP and autologous blood injections, is difficult since these procedures incorporate a fenestration technique. Mishra et al in a multicenter randomised trial, compared fenestration alone to fenestration combined with PRP injection in 119 patients with CLE. At 24-week follow-up, the success rates in the PRP group (n=56) were 82.1% compared with 60.1% for the fenestration group (n=63) as defined by a minimum improvement of 50% in pain scores (p=0.015, two-sided) and both treatment groups demonstrated equivalent improvement in the Patient Rated Tennis Elbow Evaluation (PRTEE) scores.22 In a small randomised study of 28 patients with CLE, comparing fenestration alone to fenestration with PRP injection, Stenhouse et al demonstrated a trend for greater clinical improvement at 2 months in patients receiving the PRP injection but no significant difference between the two groups at 6 months in terms of mean visual analogue scale scores.18 The available scientific evidence supporting percutaneous treatments of CLE remains limited and two recent systematic reviews conclude that the available evidence is inadequate to provide treatment recommendations.23 24
Surgery for CLE
Surgery is considered a second intention treatment for CLE and may be indicated when symptoms persist after 6 months of conservative treatment. A recent study examining the trends in surgical techniques for CLE, among newly trained orthopaedists, found that the vast majority use an open technique (92%) as opposed to an arthroscopic technique (8%).25 The authors also report that percutaneous tenotomy, debridement only and debridement with tendon repair represent 6.4%, 46.3% and 47.3%, respectively, of open operative techniques when treating CLE.25 We were able to find only one study comparing a conservative treatment (injection of botulinum toxin into the wrist extensor muscles) to a surgical technique; good to excellent results were reported 1 year after treatment in 65% and 75% of cases, respectively.26 A retrospective study comparing open release to the arthroscopic technique in 75 patients reported good to excellent results in 69% of open-release cases and 72% of arthroscopic cases.27 A randomised controlled trial comparing the open release and the percutaneous tenotomy techniques in 45 patients with CLE showed significant improvement of all outcomes in both groups at 12 months, with a more rapid clinical improvement and return to activities in the percutaneous tenotomy group.28 Notwithstanding the clinical perception that surgery is an effective treatment for CLE, a recent Cochrane systematic review found insufficient evidence to formally conclude on the efficacy of surgery for lateral elbow pain, because of the retrospective designs used and the heterogeneity of interventions among studies.5
Role of diagnostic ultrasonography in CLE
US with colour and power Doppler evaluation and MRI are useful to confirm the diagnosis in clinically suspected CLE and for surgical planning in cases refractory to conservative treatment.29 Because US is less expensive than MRI, offers high spatial resolution and allows for timely image-guided intervention, it is particularly well suited to the management of CLE. However, no US or MRI-based outcome relevant grading system to assist clinical and surgical decision-making has been developed to date.29
US findings of CLE have been well documented and may include common extensor tendon abnormal hypoechogenicity, tendon thickening, the presence of an enthesophyte, calcifications and intrasubstance cleavage tears, neoangiogenesis and radial collateral ligament tears.30 31 US assessment of CLE remains largely qualitative and subject to interobserver variability.31 Hypoechogenicity of the common extensor tendon was found to be the most effective US finding to identify elbows with CLE,32 whereas the presence of large intrasubstance cleavage tears or of an associated tear of the radial collateral ligament has been associated with poorer clinical outcomes.33 Through a meta-analysis of four studies examining the diagnostic value of grey-scale US findings for suspected CLE, Latham et al reported a pooled sensitivity of 0.82 (95% CI 0.76 to 0.87) and specificity of 0.66 (95% CI 0.60 to 0.72) with clinical diagnosis used as a gold-standard criterion.34 Regarding the importance of vascularity assessment in the evaluation of CLE, when considered alone, colour Doppler was found to be a poor predictor of clinical outcome in the study by Clark et al,33 whereas power Doppler was found poorly sensitive (0.26) but highly specific (1.00) in a systematic review by Dones et al 32 and seemed to have moderate diagnostic accuracy (63%–77%)%) in a blinded case–control study by Heales et al.35
Recently, researchers have demonstrated that sonoelastography, which assesses the elastic properties of soft tissues, was correlated to histological alterations in the common extensor tendon of cadaveric elbows.36 Other in vivo studies have shown that sonoelastography can be used to differentiate between normal and diseased tendons.37–39 This modality is based on the premise that ageing and tendinopathy-related changes cause a decrease in tendon stiffness which correlates with an increase in tissue strain. More recently, Yamamoto et al using compression-based US elastography with an acoustic coupler showed that strain ratio measurement was associated with time-dependent mechanical and histological changes of the healing tendon in a rabbit model.40 This suggests that quantitative US elastography could be used to assess the mechanical properties of a healing tendon.40 However, sonoelastography requires the application of an external compression force with the transducer and thus is subject to operator variability. Acoustic radiation force impulse (ARFI)-based elastography uses a focused US pulse to generate mechanical displacements of the tissue.41 The velocity of the induced shear waves propagating through the tissue is measured to provide a quantitative evaluation of the shear modulus and consequently of tissue elasticity. Recently, shear wave imaging has been used to assess tendon stiffness changes associated with tendinopathy and normal ageing.42 43 Although promising for the evaluation and characterisation of tendinopathies, to the best of our knowledge, shear wave elastography has yet to be studied in the context of CLE prognosis.44
Significance
The absence of a standardised therapeutic algorithm for patients with CLE and the lack of imaging parameters to establish prognosis and monitor the healing tendon process represent limitations in current knowledge. Promising preliminary results of US-guided tendon fenestration for the treatment of CLE suggest that this intervention may prove a valuable alternative to standard conservative treatment. To the best of our knowledge, no previous study has compared the use of US-guided fenestration to open-release surgery for the treatment of CLE.
Study objectives
Primary objective
To compare the efficacy of one US-guided tendon fenestration procedure with open-release surgery for the treatment of CLE refractory to ≥6 months of conservative management. A reduction of ≥11/100 points in PRTEE score at 6 months following the intervention will be considered a successful outcome. Because US-guided fenestration is less costly, less invasive and more accessible than surgery, it may still be relevant as a conservative treatment despite statistically significant differences between the proportion of responders, unless the difference is greater than a clinically acceptable threshold. Therefore, we wish to test whether the proportion of responders in the fenestration group will be non-inferior to the proportion of responders in the surgery group, by a margin of >15%.
Hypothesis
H0: Psurgery−Pfenestration >15%.
H1: Psurgery−Pfenestration ≤15%.
Secondary objectives
To compare the effect of the two interventions on various clinical outcomes including: pain and disability, functional limitations at work, pain-free grip strength, patients’ global impression of change and level of satisfaction, at each follow-up time point (6 weeks, 3, 6 and 12 months).
To compare pain medication intake in both treatment groups at 6 weeks, 3, 6 and 12 months.
To explore the predictive value and time-dependant changes of various qualitative/quantitative US and elastography parameters in response to treatment at 6 and 12 months following intervention.
Methods and analysis
Overview of study design
This is a phase II, prospective, randomised, single blind, controlled study, which will be carried out at the Centre Hospitalier de l’Université de Montréal (CHUM) between April 2016 and April 2020. The study has been approved by the institutional research ethics board on 23 March 2016 (IRB 15.327) and adheres to the Standard Protocol Items of the Recommendations for Intervention Trials 2013 guidelines.45 Study results will be reported according to the Consolidated Standards of Reporting Trials guidelines for randomised clinical trials46 and registered with ClinicalTrials.gov, identifier NCT02710682.
Patient and public involvement
The development of the research question and outcome measures of this study was informed by issues regarding care management of patients with CLE, encountered in our clinical practice. However, patients were not directly involved in the design of the study, nor in the recruitment and conduct of the study. To assess the burden of the interventions, as part of the study outcome measures, the participants’ global impression of change and treatment satisfaction will be measured. The results of the study will be disseminated to the study participants and the general public through a report published by the Institut de recherche Robert-Sauvé en santé et sécurité du travail (IRSST), Montreal (Quebec), Canada, which participates in the funding of the study.
Subjects and recruitment strategy
Figure 1 shows the participant flow chart throughout the study. Participants will be recruited over a period of 36 months, from the intake clinics of two fellowship-trained orthopaedic surgeons specialised in upper-extremity surgery, at the CHUM. Additionally, we will recruit participants through other physicians and healthcare professionals, via advertisements intended for the general public, the hospital intranet, the university’s social media profiles, and local newspaper and medical association newsletters. Those interested will contact the research coordinator who will provide further information about the study objectives and procedures and will perform an initial eligibility screening interview by telephone.

Participant flow chart.
Medical evaluation
Participants found to be eligible after the initial telephone interview will be invited to attend a medical examination by one of two orthopaedists. The orthopaedist will perform a standardised clinical examination to confirm the CLE diagnosis and assess eligibility to participate in the research project (table 1).
Study eligibility criteria
Enrolment procedure
Following the medical evaluation, the research coordinator will meet with the eligible participants and obtain written informed consent. Demographic variables (age, sex, height and weight), employment status (full-time or part-time work, on workers’ compensation/insurance leave) and professional activity characteristics (repetitive movements for >4 hours/day; light/heavy physical workload; wrist flexion for >2 hours/day; elbow flexion and extension for >2 hours/day; use of computer keyboard/mouse (number of hours/day); use of vibrating instruments for >2 hours/day) will be collected. Participants will also be asked relevant questions about their previous medical history, duration of CLE symptoms, and previous treatments (rehabilitation programme of stretching and/or strengthening exercises, tendon injections or extra-corporeal shockwave therapy). Finally, maximal pain free grip strength will be evaluated using a dynamometer according to a validated standardised protocol.47
US and elastography evaluation
Using an Acuson S3000 US scanner (Siemens Medical Systems, Mountain View, California, USA) with an optimised standardised imaging protocol, a fellowship-trained musculoskeletal radiologist with 23 years of experience in musculoskeletal US will perform a grey-scale US scan, colour and power Doppler evaluation with a linear 14L5SP or 14L5 MHz transducers and ARFI-mode elastography with a linear 9L4 MHz transducer, of the common extensor tendon on the lateral aspect of the elbow, at the initial visit following enrolment in the study, and at 6 and 12 months’ after the intervention. Participants will be sitting with the elbow flexed at approximately 70° and with the forearm resting on the examination table in a pronated position. For grey-scale US, standardised static images and dynamic cine clips in the long and short axes of the common extensor tendon will be taken to characterise tendon abnormalities.30 31 48 The US and elastography parameters assessed are presented in table 2. Cine clips will be reviewed at a later time point by two musculoskeletal radiologists, not otherwise involved in the project, for a blinded characterisation of tendon abnormalities. For ARFI-mode elastography, a linear 9L4 MHz probe will be placed in the long and short axes of the tendon, using dedicated software (Siemens virtual touch imaging quantification (VTIQ)) to record data. A generous amount of coupling gel and minimal pressure will be applied by the probe so as not to compress the tissues to avoid tissue hardening artefact. The machine will be set at a maximal shear wave propagation velocity (10 m/s), and quality and velocity parametric images will be recorded. All images and cine clips will be stored on a picture archiving and communication system database.
Study evaluation procedures and timeline
Randomisation and blinding scheme
Following the US and elastography examinations, participants will be randomised in two intervention groups with block sizes of eight, without stratification, according to a computerised randomisation list generated under the supervision of one of the author (FD) who is not otherwise involved with the participants. A research assistant, not otherwise involved with participant evaluations, will be responsible for keeping the allocation sequence in sealed envelopes. At the appropriate time, this assistant will open the envelope and assure coordination of the therapeutic interventions. The research coordinator assessing the grip strength and administering the questionnaires throughout the study will remain blinded to the treatment group allocation.
Data management
Participant responses will be considered outside the permitted follow-up time points if they are completed more than 2 weeks following the planned 6 week follow-up, more than 3 weeks at the 3 month follow-up, and 1 month before or after the 6 and 12 month follow-up. Registered subjects will be withdrawn from the study if: (1) subject withdraws his/her consent and (2) exclusion criteria are discovered after registration. Consent to use the data already collected prior to a subject’s withdrawal will be included in the consent form.
Therapeutic interventions
US-guided tendon fenestration
One of two fellowship-trained musculoskeletal radiologists, with 23 and 10 years of experience in US-guided interventions, respectively, will perform the percutaneous tendon fenestration interventions. Participants will be instructed to avoid taking non-steroidal anti-inflammatory medication 10 days prior and up to 14 days following the intervention, but will be allowed to continue other oral analgesics such as acetaminophen. The participant will be lying on a stretcher with his or her arm resting on an examination table next to the stretcher. With the elbow flexed at 70° and the forearm pronated, the common extensor tendon will be identified on US and the needle entry point on the skin will be marked. Using the standard aseptic technique, the skin at the lateral aspect of the elbow will be disinfected with an alcoholic chlorhexidine solution and draped. The skin and subcutaneous tissues will be anaesthetised with 3 cc of lidocaine 1% and a 25G needle. Then, fenestration of the tendon will be performed with a 22G needle under continuous US guidance by repeatedly passing the needle along the long axis of the tendon and abrading the underlying bone, in order to cover the entire affected zone. Participants will then be provided with a pamphlet detailing the recommendations following the intervention (figure 2), accompanied by verbal instructions.

Instructions intended for participants following an US-guided fenestration intervention. This pamphlet is given to the study participants who are randomised in the fenestration group.
Open-release surgery
Using an open-release approach, the surgical intervention will be undertaken by one of the two participating orthopaedic surgeons. Following skin disinfection, local anaesthesia and application of a tourniquet to the upper limb, a short longitudinal skin incision will be performed, slightly anterior to the lateral epicondyle. After subsequent dissection, the extensor carpi radialis longus (ECRL) tendon will be reclined to expose the conjoint tendon, and pathological tissue of the subjacent ECRB tendon will be excised. Then, the ECRL tendon will be sutured back to the extensor aponeurosis, followed by skin closure. Postoperative follow-up is planned at various intervals, up to 6 months, as per the usual clinical care management of each orthopedist and the post-operative progress of each participant.
Any adverse effect will be assessed by the physician responsible for the intervention and recorded at the time of the interventions. According to the usual procedure, any unexpected adverse effect will be reported to the research ethics board.
Baseline and follow-up evaluations at 6 weeks, 3, 6 and 12 months
During the enrolment visit and at each follow-up time point, patients will complete various self-administered validated outcome questionnaires using an electronic database (REDCap electronic data capture tools hosted at McGill University Health Centre–Research Institute, Montreal, Canada)49 with user interface controls developed for the present study. Data will be collected during the participants’ visits to the university hospital at baseline, 6 and 12 months and online at the 6 week and 3 month time points. To maximise participant compliance in questionnaire completion at the 6 week and 3 month follow-up time points, reminder emails and a telephone call by the research coordinator will be programmed (table 2).
Baseline and outcome measures
Pain and disability severity
The primary outcome measure will be the PRTEE score (scale 0 to 100=worst possible pain and very significant loss of function). This questionnaire is specific to elbow pathology and is sensitive to change.50 A variation of 11/100 points or 37% is considered a clinically significant change, that is, ‘much better’ or ‘completely recovered’.51
Elbow symptoms of pain and physical dysfunction, as well as impact of symptoms on ability to work, will be measured with the self-reported shortened version of the Disabilities of the Arm, Shoulder and Hand (11-item QuickDASH) disability/symptom and the four-item QuickDASH Work modules, respectively.52 Total and individual module scores will be calculated out of 100, with a higher score indicating a worse status. A minimal clinically important difference of 15.91 points and a minimum detectable change of 12.85 points have been reported.52
Functional instability at work
In order to gather information that is complementary to the pain and disability scales, functional instability at work will be measured with the 23-item Work Instability Scale for Rheumatoid Arthritis (RA-WIS).53 The score is on a scale from 0 to 23, with levels of functional instability at work described as: weak <10; moderate 10–17; severe >17. This scale has been validated for elbow pathologies,54 and its sensitivity to change and its predictive capabilities have been established.55
Pain free grip strength
The research coordinator, having received appropriate prior training, will measure participant pain free grip strength, using a Jamar Plus+ dynamometer (Park City, USA). Participants, holding their arm adducted along the body and the elbow in full extension, will be instructed to slowly squeeze the dynamometer until the occurrence of pain. The mean of three consecutive trials, separated by a 20 s pause, will be calculated. Results will be presented as a ratio of values of the symptomatic side/asymptomatic side×100.7
Participant global impression of change and treatment satisfaction
Participants global impression of change regarding their condition will be assessed at follow-up with a scale ranging from 1 to 7 with ‘unchanged’ as the midpoint and ‘considerably improved’ and ‘considerably deteriorated’ as anchors.56 Success rates will be calculated by dichotomising responses. Participants who report their overall condition as ‘much improved’ or ‘considerably improved’ since the beginning of the study will be counted as successes, while other responses will be counted as failures.
Similarly, participants’ level of satisfaction on the evolution of their condition will be determined on a seven-point Likert scale ranging from ‘considerably satisfied’ to ‘considerably unsatisfied’, with ‘no change’ as the midpoint.
Pain medication intake
The participants will be asked to record in a pain medication diary, their total intake of analgesics during the week preceding the 6 week, 3, 6 and 12 month follow-up time points. Their pain medication intake will be quantified at each time point, using the Medication Quantification Scale (MQS).57 This tool will make it possible to calculate the scores for each pain-related medication, based on weights assigned by pharmacologic class and dosage level, before being summed to yield the total MQS score. The minimal clinically important difference in MQS score is 4.57
US and elastography parameters
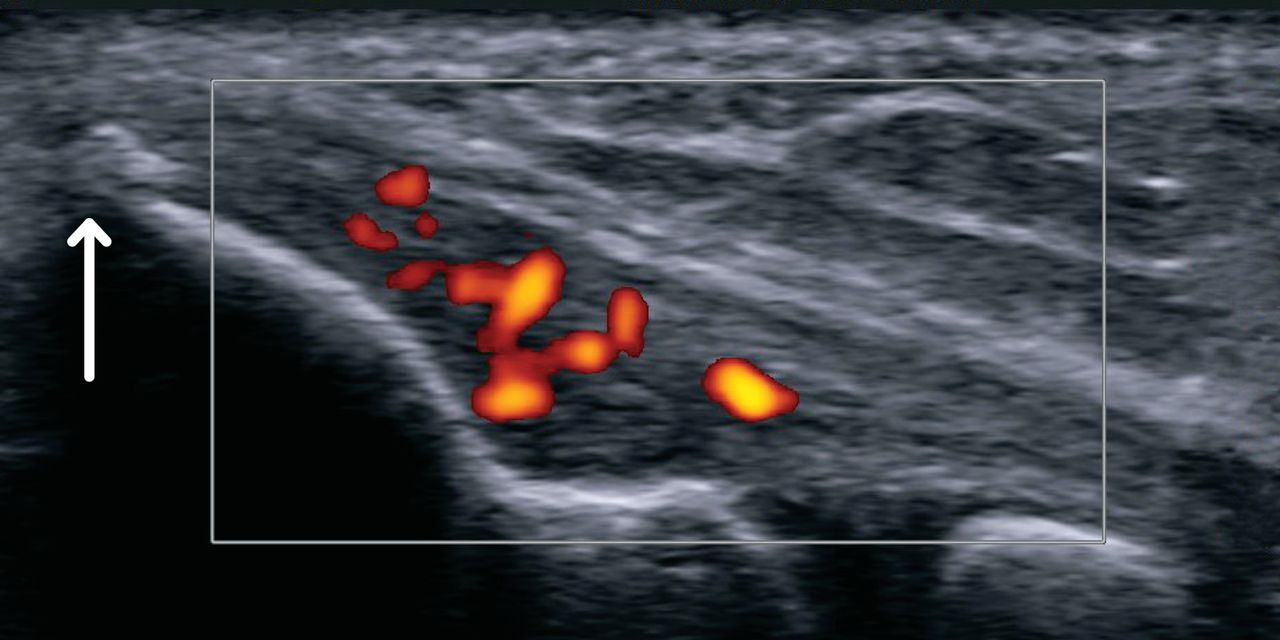
Common extensor tendon thickness will be measured at the base of the lateral epicondyle, with the transducer in the long axis (figure 3). Tendon (figure 3) and radial collateral ligament (figure 4) echostructure will be determined based on echogenicity and the presence of fissures or tears. The presence or absence of enthesophytes and of calcifications will be assessed (figure 5). Colour and power Doppler US will be used to determine density of neovessels on a long axis image of the common extensor tendon (figures 6 and 7). In ARFI-mode elastography, on a long axis image showing the base of the lateral humeral epicondyle, three regions of interest (ROI) will be identified within the tendon, along the humeral cortex, at equidistant positions, from the apex to the base of the epicondyle to measure shear wave velocities (SWV) (figures 8 and 9). Similarly, on a short-axis image of the common extensor tendon, two ROI will be placed parallel to the cortex. SWV will be measured at each ROI. Because stiffness measurements are sensitive to the angle between the probe axis and the orientation of the tendon fibres, care will be taken to align the probe parallel to the tendon fibres for the measurements taken in the long axis and perpendicular to the humeral cortex in the short axis. A maximum value of 10 m/s will be assigned to the sample volume (ROI) in the eventuality that some measurements exceed the limit of the Siemens unit. The mean of these measurements will be retained for analysis. The degree of anisotropy of the tendon will be assessed using the ratio of SWV measured in the short axis to the SWV measured in the long axis.58 Details of grading schemes for the imaging parameters are listed in table 3.
Ultrasonographic and elastographic parameters of the common extensor tendon at the lateral aspect of the elbow

Chronic lateral epicondylosis in a patient’s right elbow. Long axis ultrasound (US) scan image of the common extensor tendon demonstrates diffuse hypoechogenicity and small anechoic clefts of the common extensor tendon representing a Grade 3 degree of severity. The maximal tendon thickness as shown by the cursors is measured between the surface of the tendon and the base of the lateral humeral epicondyle (H). An enthesophyte is present at the apex of the lateral epicondyle (arrow) as well as a small calcification adjacent to the cortex. R, radial head.
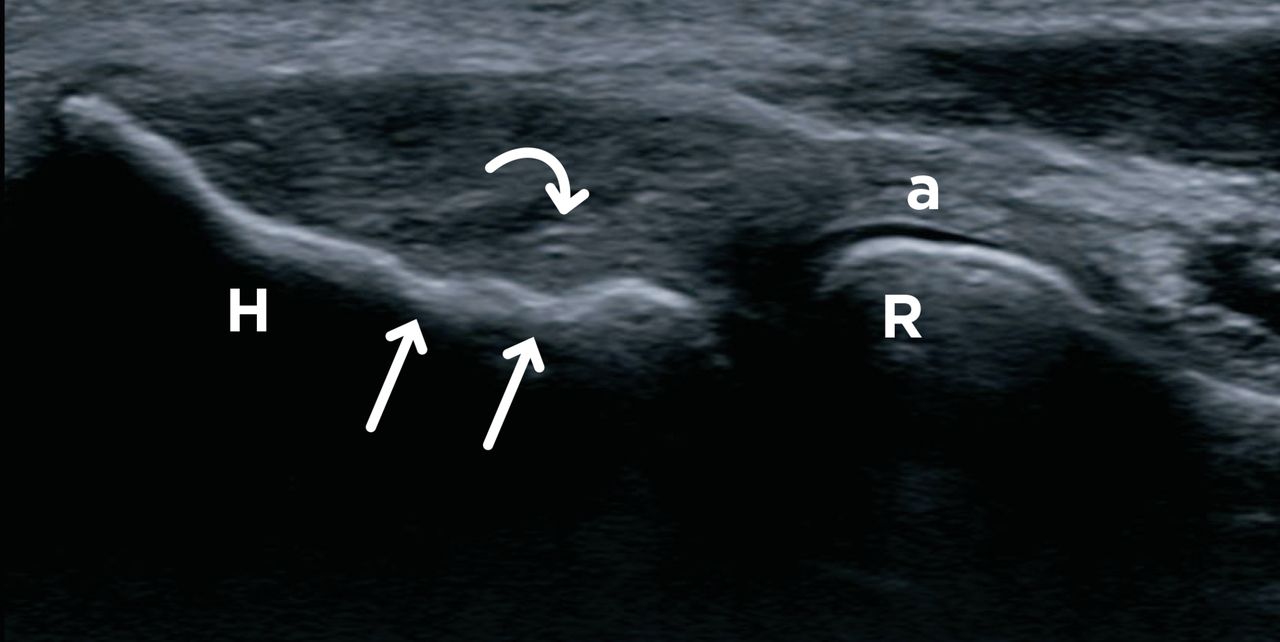
Chronic lateral epicondylosis in a patient’s right elbow. Long axis ultrasound scan image shows the radial collateral ligament (curved arrow) which occupies approximately 50% of the surface of the lateral epicondyle (arrows). a, annular ligament; H, lateral humeral epicondyle; R, radial head.

Chronic lateral epicondylosis in a patient’s right elbow. Long axis ultrasound scan image of the common extensor tendon shows intratendinous calcific foci with (arrow) and without (dashed arrow) acoustic shadowing. Also note cortical irregularities and an enthesophyte, respectively, near the base and at the apex of the humeral epicondyle (H).

Grade 2 neoangiogenesis in a patient’s right elbow with chronic lateral epicondylosis. Long axis ultrasound scan with Power Doppler demonstrates neoangiogenesis involving approximately 50% of the tendon surface consistent with a Grade 2 severity. Note the presence of an enthesophyte at the apex of the lateral humeral epicondyle (arrow).

Grade 1 neoangiogenesis in a patient’s left elbow with chronic lateral epicondylosis. Long axis ultrasound scan with Power Doppler in a patient’s left elbow with chronic lateral epicondylosis showing a few pixels of Doppler signal indicative of a Grade 1 severity.

Virtual Touch Image Quantification parametric quality map in a patient’s right elbow with chronic lateral epicondylosis. Long axis ultrasound scan in acoustic radiation force impulse-mode elastography shows a parametric quality map image with homogeneous green colour of the soft tissues indicating an adequate elastography read out.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Virtual Touch Image Quantification parametric velocity map in same patient’s right elbow as in figure 8. Corresponding parametric velocity map image with three regions of interest placed along the lateral epicondyle cortex to measure shear-wave velocities within the common extensor tendon. The mean of the three velocities is retained for statistical analysis.
Data analysis plan
Descriptive statistics will be used to characterise both treatment groups at baseline.
Primary objective analysis plan
Fisher’s exact test will be used to compare the proportion of patients reporting a reduction of ≥11/100 points in PRTEE score at 6 months in each group. The primary analysis will follow the intention-to-treat principle.
Secondary objectives analysis plans
In order to compare the impact of US-guided tendon fenestration and open-release surgery on pain, function, professional activity, grip strength, medication burden and tendon elasticity and anisotropy, mixed linear models for repeated measures will be used to assess the differences between the treatment groups in terms of the PRTEE, QuickDASH disability/symptom and work modules, RA-WIS, grip strength, MQS scores, mean SWS and ratio at respective time points. To evaluate and compare the impact of the two interventions on the participant’s global impression of change and degree of satisfaction, the proportion of participants in each group who are feeling ‘much improved’ or ‘considerably improved’ and ‘satisfied’ or ‘considerably satisfied’, respectively, will be compared using Fisher’s exact test. Finally, recursive partitioning analyses will determine whether US and elastography parameters recorded at baseline predict treatment response (reduction of ≥11/100 points of the PRTEE score) at 6 and 12 months following intervention and predictive statistics with corresponding 95% CI will be calculated.
Sample size considerations
Sixty-four participants equally divided into the two treatment arms will be enrolled in this study. Accounting for an attrition rate of 15%, a sample size of 28 patients per treatment group will yield 87% power to test for non-inferiority between surgery and US-guided fenestration, with success rates of 70%27 and 60%,22 respectively, and a clinically relevant difference of ≤15% between the proportion of patients in each arm reporting a reduction of ≥11/100 in PRTEE score at 6 months after treatment, with a two-sided significance level of 5%.
Ethical and study monitoring considerations
This randomised controlled trial will be conducted in accordance with the approved trial protocol, the Tri-Council Policy Statement on Ethical Conduct for Research Involving Humans (TCPS2 2014) and the Quebec civil code.
Data collection and management will be organised by the research coordinator and supervised by the principal investigator (NJB). A research chart will be created for each subject. The chart will include the signed consent form and the standardised data entry forms. The research charts will be kept in locked file cabinets. The standardised data will be entered into the secured electronic database (REDCap) in a de-identified and coded format. All US images will be kept in the research picture archiving and communication system in a de-identified and coded format. The data monitoring committee (DMC) will be composed of the principal investigator and three co-investigators (FD, MC, GC) who are not directly involved with the participants. An external DMC is not deemed necessary in this phase II study. The principal investigator and all co-investigators will have access to the full dataset.
Dissemination
Results of this study will be published in peer-reviewed journals and presented at local, national and international conferences. A study report, intended for the participants, healthcare professionals and general public will also be published by the Institut de recherche Robert-Sauvé en santé et sécurité du travail (IRSST), Montreal (Quebec), Canada, which is funding this study.
Discussion
CLE is a highly prevalent condition, which causes pain with functional limitations associated to a significant socioeconomic burden and still lacks consensus on optimal care management. Although the majority of patients will experience improvement at 1 year with a combination of conservative measures, it is estimated that 4%–11% will eventually undergo surgery.59 Due to the absence of clinically relevant staging of lateral epicondylosis, it remains undetermined which forms will respond to conservative measures and which forms are more likely to require surgical treatment.25
To the best of our knowledge, this study is the first to compare US-guided fenestration to surgery, for the treatment of CLE. US-guided fenestration is less invasive, less expensive and more accessible than surgery and, if proved to be effective, could be offered to selected patients as part of non-operative care management. In view of recent literature, the use of corticosteroid injections in the treatment of CLE should be discouraged. Nevertheless, corticosteroid injections are still commonly used, as physicians wish to satisfy their patients’ need to relieve pain. Therefore, a change in paradigm in CLE treatment is needed. This change will come about through proposed evidence-based treatment guidelines. Other authors are now conducting a clinical trial48 on CLE treatment and our prospective randomised study proposes to complement and add to this relevant and much needed scientific effort. Furthermore, this study will explore the value of imaging biomarkers to improve the characterisation of CLE and help establish prognosis. This secondary objective is part of an effort to develop better guidelines and risk stratification plans to assist clinicians and other healthcare professionals in the care management of CLE.
Acknowledgments
The authors wish to thank Ms Kathleen Beaumont for providing manuscript review assistance. We would like to acknowledge Siemens Healthineers for the loan of the S3000 ultrasound machine for the duration of this project. Siemens Healthineers had no role in study design and will have no role or authority in collection, management, analysis and interpretation of data; writing of the report and the decision to submit the report for publication.
References
Footnotes
Contributors PG, PT, FD, MC, GC and NJB significantly contributed to designing the study protocol. EL drafted the manuscript under NJB’s supervision. PG, PT, FD, MC and GC critically reviewed the manuscript. All authors approved the final version of this study protocol.
Funding This work is supported by Institut de recherche Robert-Sauvé en santé et sécurité du travail (IRSST), Montreal (Quebec), Canada (grant # 2015-0034).
Competing interests NJB MD MSc is supported by the Fonds de recherche du Québec–Santé (FRQ-S), Montreal (Quebec), Canada (Research Scholarship Grant # 31144, 2015–2019). The IRSST and the FRQ-S had no role in study design and will have no role or authority in collection, management, analysis and interpretation of data; writing of the report and the decision to submit the report for publication.
Patient consent Obtained
Ethics approval Centre Hospitalier de l’Université de Montréal (CHUM)
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Study data are collected and managed using Research Electronic Data Capture (REDCap) electronic data capture tools hosted at McGill University Health Centre, Research Institute, Montreal, Canada. REDCap is a secure, web-based application designed to support data capture for research studies, providing: (1) an intuitive interface for validated data entry; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages and (4) procedures for importing data from external sources.