Article Text

Abstract
Objectives Potentially inappropriate medication (PIM) occurs frequently and is a well-known risk factor for adverse drug events, but its incidence is underestimated in internal medicine. The objective of this study was to develop an electronic prescription-screening checklist to assist residents and young healthcare professionals in PIM detection.
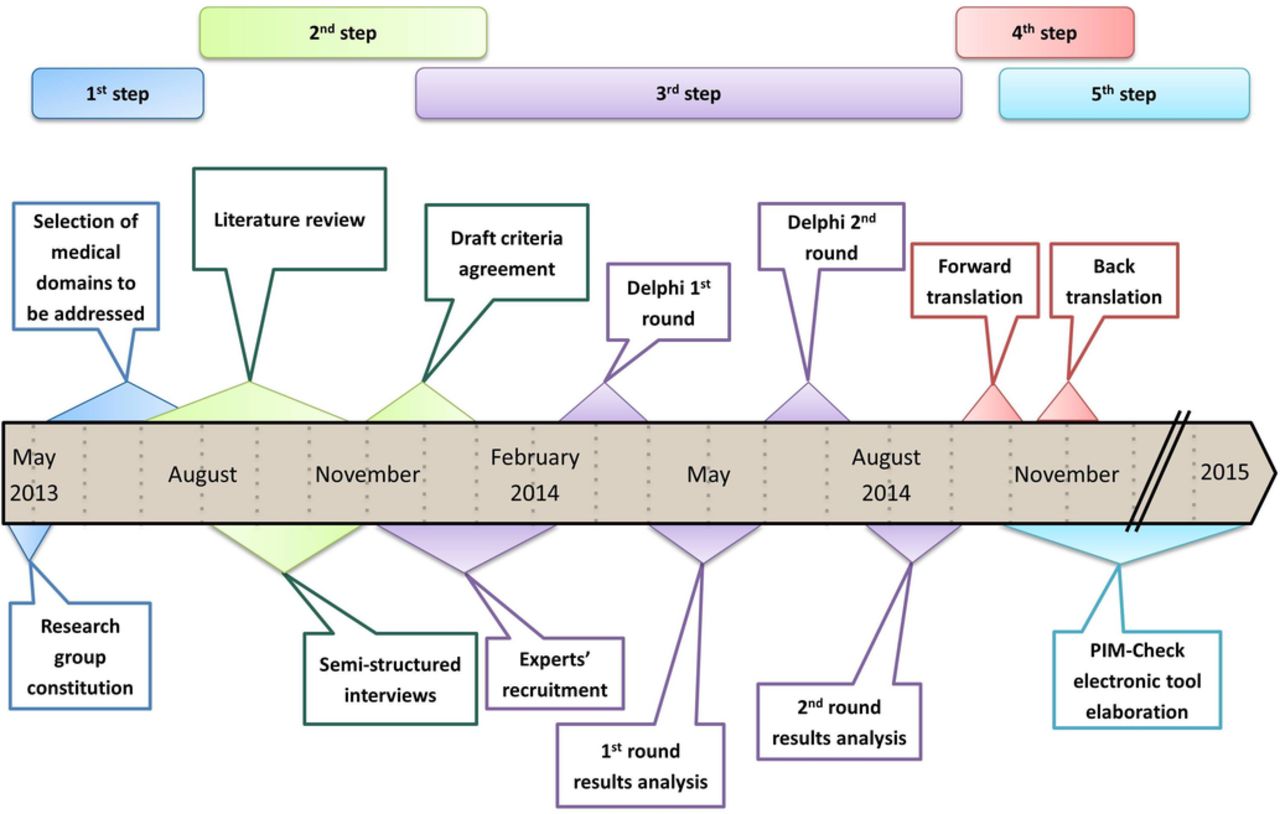
Design Five-step study involving selection of medical domains, literature review and 17 semistructured interviews, a two-round Delphi survey, a forward/back-translation process and an electronic tool development.
Setting 22 University and general hospitals from Canada, Belgium, France and Switzerland.
Participants 40 physicians and 25 clinical pharmacists were involved in the study.
Agreement with the checklist statements and their usefulness for healthcare professional training were evaluated using two 6-point Likert scales (ranging from 0 to 5).
Primary and secondary outcome measures Agreement and usefulness ratings were defined as: >65% of the experts giving the statement a rating of 4 or 5, during the first Delphi-round and >75% during the second.
Results 166 statements were generated during the first two steps. Mean agreement and usefulness ratings were 4.32/5 (95% CI 4.28 to 4.36) and 4.11/5 (4.07 to 4.15), respectively, during the first Delphi-round and 4.53/5 (4.51 to 4.56) and 4.36/5 (4.33 to 4.39) during the second (p<0.001). The final checklist includes 160 statements in 17 medical domains and 56 pathologies. An algorithm of approximately 31 000 lines was developed including comorbidities and medications variables to create the electronic tool.
Conclusion PIM-Check is the first electronic prescription-screening checklist designed to detect PIM in internal medicine. It is intended to help young healthcare professionals in their clinical practice to detect PIM, to reduce medication errors and to improve patient safety.
- Clinical Practice Guidelines
- Evidence-based Medicine
- Internal Medicine
- Medical Education
- Pharmacology and Toxicology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- Clinical Practice Guidelines
- Evidence-based Medicine
- Internal Medicine
- Medical Education
- Pharmacology and Toxicology
Strengths and limitations of this study
A screening checklist for potentially inappropriate medication detection in internal medicine patients was developed by an international and multidisciplinary panel of experts, using a validated consensus method.
Results from this study should be robust, because the number of experts involved in the Delphi survey and the participation rate were high (n=40 experts and 97.5%, respectively) and the reliability of a Delphi survey is directly proportional to the size of the expert group.
As participants involved in this study came from French-speaking countries, further work will be needed to assess the effectiveness of the English version of the tool in non-French-speaking areas.
Background
Improving medication safety and optimising drug prescribing are fundamental to patient safety and are priority goals of healthcare systems worldwide.1 2 Drug-related problems (DRPs) defined as an event or circumstance involving a patient's drug treatment that actually or potentially interferes with the achievement of an optimal outcome are common in internal medicine: approximately 80% of the inpatients have at least 1 DRP, with a mean of 2–3 DRPs per patient.3–7 DRPs include subtherapeutic dosage, failure to receive drugs, adverse reactions and potentially inappropriate medication (PIM), defined as the prescribing of medications without a valid indication or with a contraindication (overprescription); failure to prescribe a clinically indicated drug (underprescription); the occurrence of unwanted drug–drug or drug–disease interactions or the incorrect prescribing of an indicated drug (misprescription), such as duplicate prescribing, inappropriate follow-up and incorrect medication dose or duration.8 PIM is a well-known risk factor for adverse drug events and is therefore a source of morbidities and sometimes mortality, imposing clinical and economic burdens on patients and healthcare systems.9
Many prescription-screening checklists, such as the Beers Criteria (North America),10–14 the Assessing Care of Vulnerable Elders indicators (United States),15 16 a set of criteria developed in Australia17 and the STOPP/START criteria (Europe),18 19 have been developed to detect PIM in geriatric patients.8 20–22 Application of STOPP/START combined with education of physicians and pharmacists has been shown to be effective in minimising PIM in this population.23 However, no such checklist has been developed for general internal medicine patients. Nevertheless, multimorbidity and polypharmacy are frequent in this population4–7 and are independent risk factors for the occurrence of DRPs, whereas age is not.4 24 Geriatric checklists can be used for patients admitted in internal medicine, but such checklists are often much more focused on geriatric pathologies, not necessarily relevant in internal medicine (eg, dementia and Alzheimer's disease). Some pathologies and interventions commonly encountered in internal medicine are almost never covered by geriatric checklists (eg, obesity, contraception, infectious diseases, transplantation, renal failure and neuropathic pain).
Therefore, we have developed a new international electronic prescription-screening checklist for use with adults in general internal medicine. Specifically, we adapted the approach used by Gallagher et al 18 with the aim of achieving an international, multidisciplinary consensus on a checklist of statements that includes all types of PIMs, covers pathologies commonly observed in internal medicine and is available as an electronic version to assist and train junior healthcare professionals, in PIM detection in their daily practice and to improve medication safety.
Methods
This study was split into five steps (figure 1).

Study workflow.
First step: Selection of medical domains
A multidisciplinary international research group consisting of four internists, five clinical pharmacists, and three clinical pharmacologists from France and Switzerland was constituted to supervise the project. The group was responsible for selecting the medical domains (eg, medical specialties and medical acts, such as vaccinations and transplants) and subdomains (including pathologies, therapeutic classes and medical procedures (eg, prevention/prophylaxis, analgesia)) to be addressed in the draft version of the checklist. Selections of medical domains and subdomains were based on the main diseases observed in patients admitted to internal medicine,25 the therapeutic classes associated with adverse drug events in these patients,7 the Institute for Safe Medication Practices’ list of high-alert medications that includes drugs that bear an increased risk of causing significant patient harm when they are used in error26 and some of the pathologies included in previously published geriatric prescription-screening checklists.20 22 25 27 AD led the project and is the principal investigator in this study.
Second step: Literature reviews, semistructured interviews and draft criteria agreement
During this step, statements of potential interest for a prescription-screening checklist dedicated to adults in internal medicine (excluding pregnant women and inpatients with low life expectancy or requiring palliative care) were identified and selected for inclusion in the draft checklist.
Literature reviews and semistructured interviews
For each medical domain and subdomains selected during the first step, an extensive literature review of evidence-based optimal and inappropriate medication prescriptions was conducted. It preceded a semistructured interview, with a specialist physician of the domain to be addressed during the interview, working in the Geneva University Hospitals. The literature review process is detailed in the online supplementary appendix 1. Each interview comprised four parts: (1) project presentation, (2) presentation of statements previously published in geriatric prescription-screening checklists and statements related to the medical field addressed during the interview, (3) submission to the specialist of the pathologies and statements formulated during the literature review and (4) suggestions by the specialist of pathologies and statements to be added to the draft version. The semistructured interview topics and guide are provided in the online supplementary appendix 1 and supplementary table 1.
Supplementary file 1
Supplementary file 2
Draft criteria agreement
After semistructured interviews, redundant statements related to two or more domains and validated by at least two medical specialists were merged and the formulation of each remaining statement was standardised by the principal investigator. Finally, the statements were submitted to five members of the research group—three internists, one clinical pharmacist and one clinical pharmacologist—who anonymously rated the usefulness of the statements for practice in internal medicine by using a 5-point Likert scale ranging from 1 (not useful at all) to 5 (very useful). Statements with a mean rating greater than or equal to 3 were retained for the next step.
Third step: Delphi study
A two-round Delphi method was used to generate a consensual validation of the statements that were included in the draft checklist (figure 2).

{kind=link}
{kind=link}
Delphi flowchart.
Experts’ recruitment
To represent the views of the professional groups engaged in medication management in internal medicine, a panel of experts in French-speaking countries was recruited in roughly equal numbers by profession (internists and clinical pharmacists with a practice in internal medicine), hospital teaching status (university and non-teaching hospitals) and country (Canada (Québec), Belgium, France and Switzerland). The recruitment process is described in the online supplementary appendix 1.
Delphi rounds
We used the SurveyMonkey website to conduct the Delphi survey. As detailed in the online supplementary appendix 1, 1 week before each round, experts received by email the relevant documents to validate statements. For each round, the experts had to indicate their level of agreement with each statement using a 6-point Likert scale: 0, no opinion; 1, strongly disagree; 2, disagree; 3, neither agree nor disagree; 4, agree and 5, strongly agree. Using a second 6-point Likert scale, ranging from 1 (not useful at all) to 5 (very useful) (0, no opinion), the experts also had to rate the usefulness of each statement for daily practice and for training of students, residents and young healthcare professionals in internal medicine or clinical pharmacy. Finally, the experts were invited to add propositions including comments, modifications, references and useful links to each statement.
In accordance with previous studies, we used the following two validation rules. Statements that received the agreement (rating 4 or 5) of more than 65% of the experts after the first round were retained, were eventually modified according to the experts’ comments and were subjected to the second round.28 29 Statements with a lower percentage of experts’ agreement were excluded (ie, ≤65% of the experts rating 4 or 5 the statement). After the second round, only statements that received the agreement of more than 75% of the experts were retained for the final version of the checklist. The usefulness rating was considered a secondary endpoint and was not used to exclude statements. The expected durations of the first and second rounds were 3 and 2 weeks, respectively. For each round, reminders were sent to the experts, as described in the online supplementary appendix 1.
Integration of experts’ propositions
To reduce potential bias due to a single person doing all the data management, we used investigator triangulation to integrate comments and propositions from the experts.30 This triangulation process is detailed in the online supplementary appendix 1.
Fourth step: Forward/back-translation process
A forward/back-translation process was applied to translate the checklist in English.31 Briefly, the checklist was forward-translated into English by a bilingual native-English-speaking physician from Elsevier Translation Service who was familiar with French-speaking culture and with the terminology of internal medicine. Then, a bilingual native-French-speaking internist back-translated the checklist into French. Finally, three members of the research group identified and resolved any instances of inadequate expression between the back translation and the original version.
Fifth step: Electronic tool development
To facilitate the use of the tool in daily practice, an electronic version was created. A web-designer and a webmaster were involved in the development of a website and a web-mobile application. A ‘Screening’ function, allowing to select for a specific patient, his/her comorbidities and/or medications and to present only relevant statements, a ‘Favourite’ function to give quick access to statements identified as favourite and a ‘Learning’ function to allow users to follow their progress in the acquisition of recommendation knowledge were included in the application. To develop the ‘Screening’ function, members of the research group identified medications, and corresponding anatomical therapeutic chemical code, from Belgium, France, Quebec and Switzerland, using national databases.32–35 A dictionary of synonyms of subdomains included in the tool was also created. Then, an algorithm combining each validated statement with corresponding subdomains and medications was developed.
Statistical methods
Analyses were performed with Prism 6 software (GraphPad Software, San Diego, California, USA). Variables were summarised as numbers (percentages) for categorical variables, the mean and 95% CI for continuous variables. During each Delphi round and for each statement, the mean agreement rating, the mean usefulness rating, the percentage of experts who rated each statement as 4 or 5, the participation rate and the mean number of experts who responded with ‘no opinion’ (0) were evaluated. For each statement, the mean agreement and usefulness ratings were compared between the first and the second rounds using Mann–Whitney tests. p Values are two-tailed, with a significance level of 0.05.
Ethics considerations
The Swiss Law on Medical Research Involving Human Subjects did not require us to seek ethical approval as no participation by patients or use of patients’ data, human tissue or animals were involved in this study.
Results
First and second steps
The principal investigator conducted 17 semistructured interviews, one each with 17 specialist physicians. Seventeen medical domains and 69 subdomains associated with pathologies, therapeutic classes, medical procedures and DRPs commonly observed in internal medicine were identified. After the semistructured interviews and suppression or merging of redundant statements, 187 statements remained. Among them, 21 mean ratings were less than 3 (2.44 (2.33 to 2.55)) and were considered to be not useful for practice in internal medicine. These statements were excluded from the draft checklist (eg, statements related to sleep apnoea, cystic fibrosis, polymyalgia rheumatica and myasthenia gravis). The remaining 166 statements involved 17 medical domains and 65 subdomains that received a mean usefulness rating of 3.99/5 (3.89 to 4.08).
Third step: Delphi survey
Forty experts from 22 hospitals met the inclusion criteria and agreed to join the Delphi survey (table 1). During the first round, participation rate was 97.5% (39/40). A median of 37 (IQR 25%–75%: 36–38) experts rated their agreement for each statement, with a median of 2 experts with ‘no opinion’ per statement. Only one statement was evaluated by fewer than 30 experts (n=28); because this statement completed the first-round validation rule, it was clarified and modified according to the experts’ comments and submitted for the second round of Delphi. The mean agreement and usefulness rating were 4.32/5 (95% CI 4.28 to 4.36) and 4.11/5 (4.07 to 4.15), respectively according to the 0–5 Likert scales. Six statements were removed according to the validation rule for the first round (table 2). Of the 166 statements evaluated in the first Delphi round, 152 (91.5%) were rated by more than 65% of the experts as useful or very useful for the training of students, residents and young healthcare professionals in internal medicine and clinical pharmacy. The experts made 677 comments, which led the investigator triangulation group to add 3 new statements, modify 84, and merge 3 pairs of statements. The remaining 160 statements were retained and subjected to the second round.
Characteristics of Delphi panel of experts
Statements rejected by the expert panel during the first round of the Delphi survey
All the experts who completed the first round completed the second round (participation rate 100% (39/39)). They rated their level of agreement for 100% of the statements, without selecting the ‘no opinion’ option. The mean agreement and usefulness ratings were 4.53/5 (95% CI 4.51 to 4.56) and 4.36/5 (4.33 to 4.39), respectively (see online supplementary table 1). Both ratings were higher than the corresponding ratings from the first round (p<0.001). After the second round, all 160 submitted statements were validated according to validation rule for this round. Of these statements, 156 (97.5%) were rated as useful or very useful by more than 75% of the experts (see online supplementary table 2). During the second round, the experts made 399 propositions and on the basis of these propositions, 74 statements were clarified.
Supplementary file 3
The final checklist includes 160 statements, divided into 17 medical domains and 52 subdomains (table 3). Seventy-four (46%) statements are related to underprescription, 36 (23%) to overprescription, 16 (10%) to interactions and 34 (21%) to other PIM (eg, insufficient drug monitoring, incorrect dose adjustment, wrong choice of medication). The rationales for the statements are presented in online supplementary table 2, along with 233 references, 116 recommendations (eg, dose adjustment, alternatives and monitoring), 93 remarks (eg, definitions, reminders and useful lists of drugs) and 24 useful web links.
Final list of statements included in PIM-Check
Fourth step: Forward/back-translation
Among the 160 statements that were forward/back-translated, 16 were identified as having inadequate expression and were then corrected. The tool is available, both in French and in English (http://app.pimcheck.org/#/accueil/en).
Fifth step: electronic tool development
One hundred and ninety-three synonyms of the 52 subdomains included in the tool and 1635 medications were identified. To create the ‘Screening’ function, each statement was associated with corresponding subdomains and medications and an algorithm of approximately 31 000 lines was developed. This algorithm allows to ‘switch on’, or ‘switch off’, statements, depending on comorbidities and medications selected by the user. The ‘Favourites’ function created gives quick access to statements identified as favourite, and the ‘Learning’ function gives access to the list of all statements included in PIM-Check, those unread and those already read. Details regarding the conception of the tool, direct access to the references (n=333) and useful links (n=29) (through URL links), publications related to the tool and a contact section, are also available (http://www.pimcheck.org/en/).
Interpretation
PIM-Check was specifically designed to assist residents and young healthcare professionals in the detection of PIM in patients typically admitted in internal medicine (excluding pregnant women, patients with low life expectancy and patients requiring palliative care). The checklist consists of 160 statements for pathologies and drugs commonly encountered in internal medicine. The checklist does not replace the judgement of physicians and pharmacists but is intended to help young healthcare professionals to improve the medication review process and to reduce the incidence of PIM. Owing to the additional data and references associated with the statements, PIM-Check should also be helpful for training students and residents in prescribing-optimisation. Because most of the statements are based on current international clinical evidence and were validated by European and North American experts, we expect that the English version of PIM-Check will be useful in many healthcare settings. Finally, the availability of an electronic version should facilitate the use of PIM-Check in daily practice.
Comparison with other studies
PIM-Check includes more medical domains (n=17) and subdomains (n=52) than do the published geriatric checklists.20 Some of the domains and subdomains commonly found in geriatric checklists are not included in PIM-Check (eg, falls, dementia, orthostatic hypotension and sleep apnoea). In contrast, PIM-Check includes statements related to domains, such as transplantation, dependencies, obesity, antiviral therapy and proper use of antibiotics that are not generally covered by geriatric checklists. This last domain should be useful because interventions implemented in hospitals to improve the use of antibiotics have succeeded in preventing PIM.36 PIM-Check also includes therapeutic classes and drugs commonly associated with preventable hospitalisation and with PIM in internal medicine (eg, non-steroidal anti-inflammatory drugs, anticoagulants, antihypertensive or antidiabetic treatments, statins, proton pump inhibitors and corticosteroids).7 37 38 PIM-Check is also more focused on underprescription than are geriatric checklists. Seventy-four (46%) statements in PIM-Check are related to underprescription versus 18 (37%), 34 (27%) and 71 (18%) in the Australian checklist, STOPP/START v2, and Assessing Care of Vulnerable Elders indicators v3, respectively.16 17 19 This can be explained by the fact that recommending preventive treatment in older populations is sometimes inappropriate. In contrast, underprescription in internal medicine patients is not rare, and occurred 1.8 times as often as overprescription7; thus, PIM-Check should be more helpful than other checklists for preventing PIM in this population.
Strengths and limitations
The Delphi method is a robust method for reaching a consensus of opinion and is commonly used for validating PIM checklists.14 19 20 29 The reliability of a Delphi survey is directly proportional to the size of the expert group.39 Therefore, we are confident that results from this study are robust, because the number of experts involved in our Delphi survey was high, as was the participation rate. As previously demonstrated by Chang et al, checklists with higher numbers of statements, therapeutic classes and medical domains tend to show higher rates of PIM detection, although the use of long checklists can be time-consuming.21 However, PIM-Check is the first checklist available as an electronic device. The ‘Screening’ function allows users to perform an analysis for a specific patient, restricting the statements displayed to those that are most relevant to that patient, depending on his/her comorbidities and prescribed medications. This function should enable users to review a prescription in less than 5 min, as can be done with STOPP/START.9 37 40 However, these issues need to be addressed in the future, as the ability of PIM-Check to prevent PIM.
Implications for clinicians and policymakers
In our study, experts rated the statements as being highly useful for the training of students and residents. The inclusion of additional data and references with the statements can be expected to make PIM-Check helpful for improving trainee awareness of good prescription practices. Moreover, as previously demonstrated, interactive techniques in medication education and training in the use of systematic tool to reduce PIM are effective in improving prescribing-skill and patient care.41 42 The progressive learning function included in the electronic version of PIM-Check may constitute an effective intervention to improve prescribing performance. Finally, PIM-Check could be helpful for researchers and policymakers because it could be used to estimate the incidence of PIM in various settings, to evaluate prescription quality and safety and to evaluate factors and costs associated with PIM, as it has been proposed for STOPP/START and the Beers Criteria.9 43–48
Unanswered questions and future research
The next step will be to evaluate the incidence of PIM detected and prevented using PIM-Check in various healthcare settings. It will also be of interest to determine whether the use of PIM-Check, like the use of STOPP/START, is significantly associated with reductions in adverse drug events and improvement in young healthcare professionals prescribing training.23 40 49 We will test the English version of PIM-Check in non-French-speaking countries.50 Another project might be to integrate PIM-Check as a clinical decision support system in electronic health records, to assist physicians and pharmacists in their clinical practice. Finally, like geriatric checklists,10–14 16 18 19 51 PIM-Check will need to be updated in a few years as new research is published and new drugs are licensed.
Conclusion
In conclusion, this study offers an electronic prescription-screening checklist, including 160 statements. The application of this checklist combined with clinical judgement should contribute to help young physicians and pharmacists in their training and clinical practice, to detect and reduce PIM. In the context of expansion of the prevalence of multimorbidity and polypharmacy, PIM-Check could be a complementary strategy to reduce PIM and to improve patient safety.
Acknowledgments
The following people constituted the research group in charge of thestudy design: AD, BG, ALB,VP, MB, CFC, JD, AP, CS,and PB. AD, ALB,VP, MB, CFC, BG, and PB wereresponsible for the selection of the medical domains and subdomains to beaddressed in PIM-Check. We are grateful to the following medicalspecialists from the Hôpitaux Universitaires de Genève for theirindividual contributions to the semi-structured interviews: Victor Bancila(psychiatry), Philippe Bichard (gastroenterology), Françoise Boehlen(haematology and haemostasis), Sandra Boehncke (endocrinology),Yassine Bouatou (nephrology), JD (clinical pharmacology and pain clinic),Georg Ehret (cardiology), Stefan Harbarth (infectious diseases), Jean-PaulJanssens (pneumology), Loïc Locatelli (psychiatry and addictology),Philippe Meyer (cardiology and hypertension), Michael Nissen(rheumatology), Zoltan Pataky (obesity), CS (clinical pharmacology), TarekShaarawy (ophthalmology), Catherine Stoermann (nephrology), and Serge Vulliemoz(neurology). ALB,VP, MB, Olivier Grosgurin (HUG, Geneva,Switzerland) and Christophe Marti (HUG, Geneva, Switzerland) were involved inthe selection of statements before the first round of the Delphi survey. Wethank the Delphi panel of experts: Annie Athouel (pharmacy, Le Mans,France), Aurélie Barrail-Tran (pharmacy, K. Bicêtre, France), OlivierBerclaz (internal medicine, Valais romand, Switzerland), GuyBeuken (general internal medicine, Louvain, Belgium), Dorine Castillo(pharmacy, Macon, France), Remy Charette (pharmacy, McGill, Canada),Delphine Chenevier (pharmacy, Cognac, France), Emmanuelle Dernis(general internal medicine, Le Mans, France), Maxime Dore (pharmacy,Sacré-Coeur, Canada), Guillaume Faubert (pharmacy, Maisonneuve-Rosemont,Canada), Séverine Foucher (pharmacy, A. Béclère, France), Antoine Garnier(internal medicine, CHUV, Switzerland), Nathalie Gillard (pharmacy,Saint-Kuc, Belgium), BG, Pascal Guillemin (internal medicine, Macon,France), Bernard Hanson (internal medicine, IRIS Sud, Belgium), Ly Khuê(internal medicine, McGill, Canada), Pierre-Olivier Lang (internal medicine,Genolier, Switzerland), Anne-Marie Mansour (internal medicine, Sacré-Coeur,Canada), Ariane Mouzon (pharmacy, Mont-Godinne, Belgium), Carole Nachar(pharmacy, CHUV, Switzerland), Jean-Baptiste Nicolas (internal medicine,Mont-Godinne, Belgium), Nicolas Noel (internal medicine, K. Bicêtre, France),Pauline Papin (pharmacy, Saint Jean, Belgium), Marc Parent (pharmacy, Québec,Canada), Julie Peeterbroeck (pharmacy, A. Vésale, Belgium), Rachel Pham(pharmacy, IRIS Sud, Belgium), Fior Renato (internal medicine, A. Béclère,France), Thibaut Richard (internal medicine, A. Vésale, Belgium), ThierryRomanet (pharmacy, Grenoble, France), Nicolas Schaad (pharmacy, Morges,Switzerland), Mathieu Sergerie (internal medicine, Maisonneuve-Rosemont,Canada), Ionela Stifii (internal medicine, Le Cognac, France), JéromeStirnemann (internal medicine, HUG, Switzerland), Pierre-Alain Triverio (internalmedicine, Jura bernois, Switzerland), Vera Vongunten (pharmacy, Valais romand,Switzerland), Joel Wermeille (pharmacy, Jura bernois, Switzerland), ClaireWintenberger (internal medicine, Grenoble, France), Philippe Zaoui (generalinternal medicine, Grenoble, France). ALB, VP and MB made up the investigator triangulationgroup. We thank Elsevier Translation Service for the forward translationof PIM-Check. CS, AD, BG, and ALB participated in the back translation. Wethank Rolf Hauri (Geneva School of Business Administration (HEG)) andAlain Lorentz (for the web development and the web designing of PIM-Check website andwebmobile application and Carlotta Shearson (Shearson Editorial Services) forediting the manuscript.
References
Footnotes
Contributors All authors constituted the research group in charge of the design of the study and contributed to the conception of the work. AD, ALB, VP, MB, CFC, BG and PB were responsible for the selection of the medical domains and subdomains to be addressed in PIM-Check. ALB, VP and MB made up the investigator triangulation group. CS, AD, BG and ALB participated in the back translation of the tool. AD, PB and BG were responsible for the acquisition, analysis and interpretation of data for the work. AD, ALB, PB and BG drafted the work. VP, MB, CFC, JD, AP and CS revised it critically for important intellectual content. All authors approved the final version of the paper to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Full dataset are available with open access at www.pimcheck.org/en/ or from the corresponding author at audedesnoyer@gmail.com.