Article Text

Abstract
Objective Frequent users of healthcare services are a vulnerable population, often socioeconomically disadvantaged, who can present multiple chronic conditions as well as mental health problems. Case management (CM) is the most frequently performed intervention to reduce healthcare use and cost. This study aimed to examine the evidence of the effectiveness of CM interventions for frequent users of healthcare services.
Design Scoping review.
Data sources An electronic literature search was conducted using the MEDLINE, Scopus and CINAHL databases covering January 2004 to December 2015. A specific search strategy was developed for each database using keywords ‘case management’ and ‘frequent use’.
Eligibility criteria for selecting studies To be included in the review, studies had to report effects of a CM intervention on healthcare use and cost or patient outcomes. Eligible designs included randomised and non-randomised controlled trials and controlled and non-controlled before–after studies. Studies limited to specific groups of patients or targeting a single disease were excluded. Three reviewers screened abstracts, screened each full-text article and extracted data, and discrepancies were resolved by consensus.
Results The final review included 11 articles evaluating the effectiveness of CM interventions among frequent users of healthcare services. Two non-randomised controlled studies and 4 before–after studies reported positives outcomes on healthcare use or cost. Two randomised controlled trials, 2 before–after studies and 1 non-randomised controlled study presented mitigated results. Patient outcomes such as drug and alcohol use, health locus of control, patient satisfaction and psychological functioning were evaluated in 3 studies, but no change was reported.
Conclusions Many studies suggest that CM could reduce emergency department visits and hospitalisations as well as cost. However, pragmatic randomised controlled trials of adequate power that recruit the most frequent users of healthcare services are still needed to clearly confirm its effectiveness.
- case management
- outcome assessment
- effectiveness
- health services research
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This article is the first to review the evidence of case management (CM) for a general population of frequent users of healthcare services.
Although CM activities were well described in the studies, key elements associated with successful CM interventions were scarcely discussed and will deserve more attention in further studies.
Emergency department visits of frequent users show a natural decrease over time and regression to the mean may bias outcomes measured in before–after studies.
Pragmatic randomised controlled trials of adequate power and using good case finding strategies are still needed.
Introduction
Industrialised countries have recognised that a small number of patients account for a large proportion of healthcare costs.1–3 These patients use emergency department (ED) repeatedly, but their definition varies across studies.4 ,5 They also frequently use hospital services for increasingly complex health needs6–8 arising from factors such as multimorbidity, psychiatric comorbidities and psychosocial issues, or a combination of these factors.7 ,9 ,10 Requiring care and services from many partners in the health and social services care system as well as the community care network, frequent users are more likely to encounter difficulties in the integration of care11 and more at risk for incapacity and mortality.12 Healthcare providers often feel limited in their interventions with this clientele because of patients' complex needs, fragmentation of care and the episodic nature of their visits to ED.13 In this context, patients receive suboptimal care and healthcare systems are overwhelmed by the rising costs.14
To address this issue, case management (CM) is the most frequently performed intervention to reduce healthcare use and cost, and to provide better care.4 ,5 ,15 CM is a collaborative approach used to assess, plan, facilitate and coordinate care to meet patient and family health needs through communication and available resources with the intent to improve individual and health system outcomes.16 CM has been shown to improve satisfaction and quality of life17 and to reduce costs associated with frequent users of services.1 ,4–6 ,17–20 The National Case Management Network of Canada16 defined six standards of practice in CM: (1) determining and verifying patient eligibility for CM; (2) assessing patient needs; (3) documenting patient goals and priorities in a concerted strategy of intervention; (4) planning and adjusting services included in individualised service plans, including patient education and self-management support; (5) periodically reassessing patient needs and progresses; and (6) supporting transition process.
Three systematic reviews4 ,5 ,15 reported the effectiveness of CM interventions among frequent ED users and concluded they had variable benefits on clinical, social and organisational outcomes such as ED use and cost. Two reviews reported different kinds of interventions, including CM. Althaus et al4 included studies conducted before 2010, while the review by Soril et al15 did not report patient outcomes. Finally, the third review by Kumar and Klein5 looked at effectiveness of CM interventions but included articles concerning specific subgroups of patients such as psychiatric populations or patients with psychosocial problems.
Considering that many relevant studies13 ,21–24 were not included in these reviews, we aimed, in our review, to examine evidence regarding the effectiveness of CM interventions among a more encompassing population of frequent users of healthcare services.
Methods
Scoping review methodology is recognised as a process of mapping the main concepts of a research area to their source and evidence available in the literature.25 ,26 It also serves to identify gaps in the field and provide recommendations for implementation.25 This scoping review followed the five key phases of Arksey and O'Malley:25 (1) identifying the research question; (2) identifying relevant studies; (3) selecting studies; (4) charting the data; and (5) collating, summarising and reporting the results.
Research question
Based on the expertise of our research team and an initial review of the literature, we defined the following research question:
What is the evidence for the effectiveness of CM interventions among frequent users of healthcare services?
Search strategy
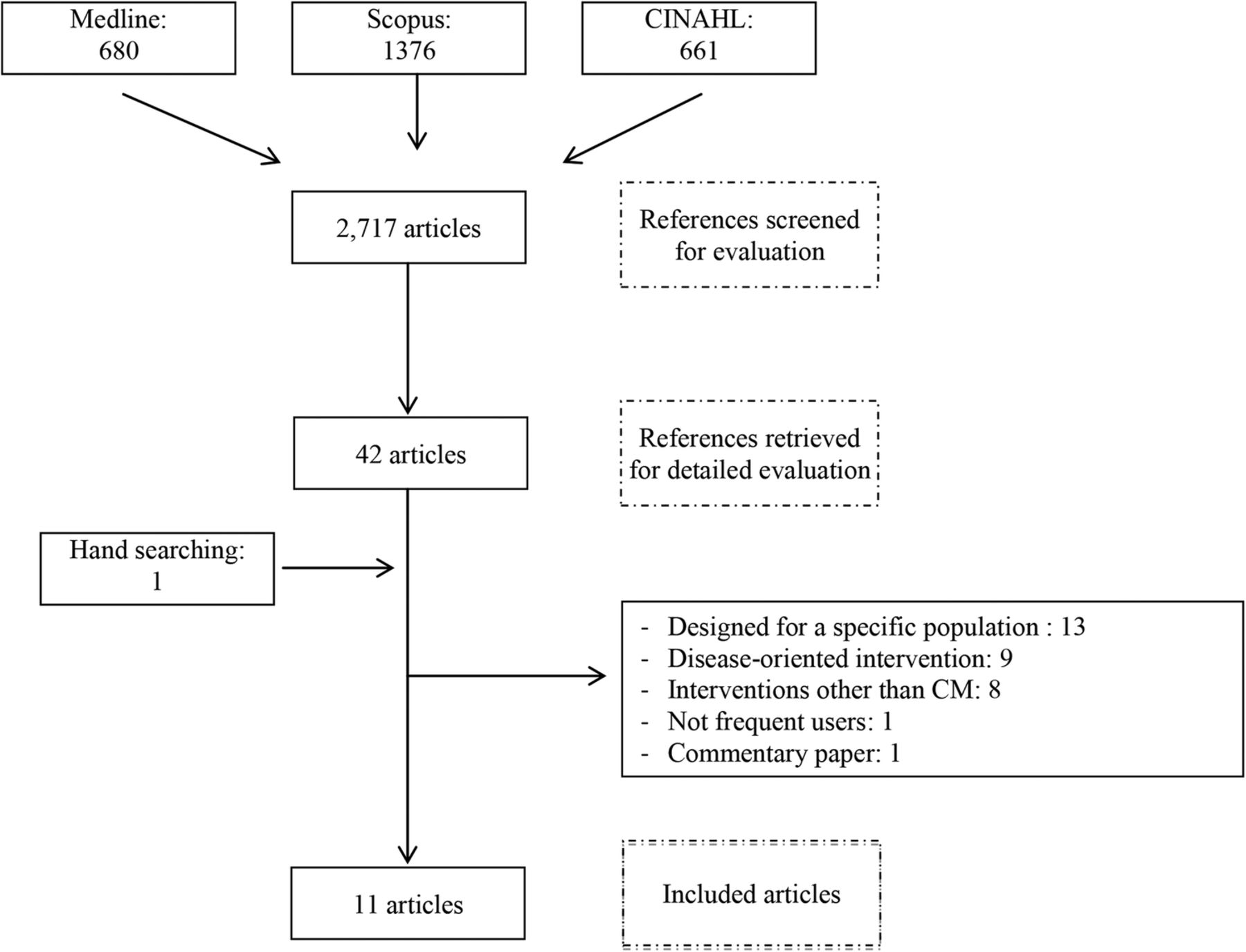
We conducted an electronic literature search of the MEDLINE, Scopus and CINAHL databases for English and French articles published between January 2004 and December 2015. The following MeSH terms and key words were used: case management, disease management, patient care management, patient care planning, health care services misuse, utilization review, frequent attend$, frequent consult$, frequent use$, high utilize$, high consult$, high attend$, high use, repeat use, frequent flyer, heavy use$, repeat$, recidivist, revolving door, misuse and hyperuse. We also examined reference lists of reviewed articles for additional relevant articles (hand searching). The search identified 2717 potentially relevant articles.
Study selection
To be included in the review, studies had to (1) report effectiveness of an intervention of CM for adult frequent users of healthcare services and (2) describe some form of comparison between patients who receive CM to those who do not receive the intervention (ie, randomised and non-randomised controlled trials, before–after studies) or between patients in preintervention and postintervention (same patients). The outcomes of interest were healthcare use and cost as well as patient-reported measures, such as quality of life and patient experience of care. To increase homogeneity and comparability among studies, we excluded studies limited to psychiatric, geriatric, paediatric, homeless, addicted patients or focusing on a single disease.
First, titles and abstracts were reviewed by one team member (ML) to exclude articles that were not eligible. At this stage, we excluded references clearly not meeting our inclusion criteria and retained all other references for analysis. In case of doubt, the full article was submitted to other team members (CH and M-CC) for a more detailed evaluation. Disagreement among team members (ML, CH and M-CC) was resolved by consensus. Forty-two articles were retained for detailed evaluation by team members (ML, CH and M-CC) and one additional reference was identified by hand searching. Of these 43 articles, 32 were excluded: 13 evaluated CM intervention designed for a specific population of frequent users (psychiatric, geriatric, paediatric, homeless or addicted patients), nine were disease-oriented interventions (mainly on diabetes, chronic obstructive pulmonary disease, rheumatoid arthritis, stroke and heart failure), eight evaluated interventions other than CM, one did not target frequent users and one was a commentary paper. A final sample of 11 articles was retained for data extraction (figure 1).

{kind=link}
Scoping review flow chart of search results.
Data extraction
For each paper included, we collected descriptive characteristics such as first author and year of publication, study location and population, setting, aim and design of the study, characteristics of the intervention (including type of activities and case manager profession), length of follow-up and data about effectiveness of the intervention.
Results
Description of the included studies
The characteristics of the 11 included papers are shown in table 1.10 ,13 ,21–24 ,27–31 Two papers were randomised controlled trials, three were non-randomised controlled studies and six were before–after studies. The number of participants varied from 10 to 2742, their mean age ranged from 35 to 65 years and the proportion of female varied from 36% to 74%. Most studies were carried out in the USA (n=8). CM intervention was conducted in ED (n=6), primary care (2), in-patient (1) and emergency medical services (EMS) (2).
Characteristics of the studies included
Definitions of frequent users varied across the 11 studies and were based on number of patient ED visits (ranging from 3 visits in a month to 10 visits in a year),10 ,13 ,27–31 number of patient admissions (ranging from two to more than four admissions in a year),23 ,30 number of EMS uses (10 transports or more in 1 year or the top 25 frequent users),21 ,24 annual hospital cost ($4000 and more in a year)22 and opinion of the healthcare staff.10 ,24 Three studies recruited low-income, uninsured frequent users.27 ,30 ,31 Nurses were the case manager in four studies,23 ,27 ,28 ,31 social workers in two studies30 ,31 and paramedic staff in one study,24 but majority of the studies (n=5) did not specify who the case manager was.
The CM intervention also varied across studies (table 2). All interventions assessed patient needs as well as planned and adjusted services included in individualised service plans. The majority determined and verified patient eligibility (n=10), supported transition process (n=8), reassessed patient needs and progress (n=7), and provided patient education and self-management support (n=6). Few studies documented patient goals and priorities (n=3) (see online supplementary appendix 1).
CM activities described in the included studies
supplementary appendix
As indicated in table 3, all studies reported the use of care as an outcome, six studies evaluated healthcare cost21–24 ,27 ,30 and three studies investigated the impact of a CM intervention on patient quality of life.22 ,23 ,31 Only one study evaluated healthcare use and cost as well as patient quality of life.23
Outcomes measured in the included studies
Healthcare use and cost
Among all the studies included, two described results of a randomised control trial.22 ,23 In a study of 2742 patients with high levels of in-patient healthcare expenditures, Segal et al22 showed an increase in healthcare cost mainly due to the extra costs for care planning and CM. However, the experimental group included only 5% of patients at risk of future hospital admission. This could indicate a problem in the selection of their patients who should represent frequent users. In a randomised controlled trial of 96 patients, Sledge et al23 observed a trend towards reduced admission, ED use and total healthcare cost in the experimental group, but they found that the difference was not significant, probably due to a lack of power.
Three articles presented non-randomised controlled studies.27 ,28 ,30 Shah et al30 conducted a study with 258 low-income, uninsured patients and demonstrated that ED use as well as cost had significantly decreased, but no difference was reported for in-patient admissions. The authors attributed positive results to patient engagement, frequent in-person contacts, liaison with social resources, and close relationships between case managers, local hospitals and providers at local clinics. However, a possible bias in favour of patients more willing to engage in the management of their health was noted. A study with 36 patients in the experimental group by Crane et al27 also demonstrated a reduction in ED use and healthcare cost ranging from US$ 1167 per patient per month to US$ 230 (p<0.001) in combined ED and inpatient hospital charges. The authors identified many factors contributing to the effectiveness of their CM intervention: long and frequent medical visits without limitation on the number, identification and resolution by the care team of barriers and frustrations in accessing medical care, emotional support provided to the patient by the group meetings, and personal qualities and competence of the care manager who gaining patient trust. However, of the 147 frequent users contacted, only 36 accepted to participate, probably the more motivated patients, something that could be seen as a possible bias. Another limitation could be attributed to the analysis of the data that came from only one hospital, although frequent users are known to seek care at multiple EDs. On the other hand, Peddie et al28 conducted a non-randomised controlled study with 164 frequent ED users and found no reduction in ED visits. After 4 years of follow-up, the percentage of patients in the experimental group still attending ED at least once a year in the fourth year was similar to the control group (respectively 64% vs 65%). The fact that the control group was an historical one, that is, individuals acted as their own controls, and possible lack of power could explain this result.
Six articles described results of before–after studies.10 ,13 ,21 ,24 ,29 ,31 Four articles demonstrated a reduction of healthcare use and cost,13 ,21 ,24 ,31 and two of them reported no change in ED use or admission.13 ,24 Pillow et al13 conducted a study with the top 50 chronic ED frequent users. By using data from one hospital, they reported a trend towards a reduction in ED use, but no significant change on admission. The main factors contributing to their repeat visits according to the CM team were psychiatric disease, substance abuse, malingering, medication non-compliance and unstable housing. In the same way, a before–after study of 60 patients by Phillips et al29 reported an increase in ED use. Seventy-three per cent of the patients presented either substance misuse or psychosocial issues as their primary problem, and only 27% had chronic medical problems. In a study of 492 low-income, uninsured frequent ED users, Wetta-Hall31 demonstrated a reduction in ED use. The author associated this result to the advocacy role of the CM team who facilitated participant access to medical care, prescription medications and social services. Rinke et al21 (n=10) and Tadros et al24 (n=51) observed a reduction in EMS cost and use among frequent EMS users. However, Tadros et al24 reported no change on admission as well as ED use and cost. Finally, in a pilot study with 50 patients, Lee and Davenport10 found no change in ED use.
Patient-reported outcomes
Among the three studies reporting quality-of-life outcomes,22 ,23 ,31 two randomised controlled trials reported no change,22 ,23 one of them included only 5% of patients at risk of future hospital admission22 and the other possibly lacked power with a sample of 96 patients.23 One before–after study found an improvement in patient quality of life.31 Wetta-Hall31 demonstrated that the physical dimension of quality of life improved significantly after the CM intervention (p<0.001). However, the mental dimension of the quality-of-life score showed minimal change. Physical dimension of quality of life probably improved due to the fact that the participants had access to medical care, prescription medications and social services. According to the author, mental dimension of quality of life did not change because it was not the focus of the CM intervention. Moreover, life circumstances of a low-income, less educated and uninsured population did not change between preintervention and postintervention.
Patient outcomes such as drug and alcohol use, health locus of control and patient satisfaction were evaluated in three studies,23 ,29 ,31 but no change was reported.
Discussion
This scoping review identified 11 studies evaluating the effectiveness of CM interventions among frequent users of healthcare services. Two non-randomised controlled studies27 ,30 and four before–after studies13 ,21 ,24 ,31 reported positive outcomes on healthcare use or cost. However, a selection bias may have been present in four studies because their participants were probably more motivated to change behaviour given their willingness to participate in the intervention.21 ,27 ,30 ,31 In addition, four studies included a small sample of patients (≤51),13 ,21 ,24 ,27 and three studies conducted their analyses on data from only one hospital.13 ,24 ,27 On the other hand, five studies presented mitigated results.10 ,22 ,23 ,28 ,29 One of the randomised controlled trials23 was unable to detect a difference in healthcare cost and use, while the other demonstrated an increase in healthcare cost22 but raised issues concerning case finding. One before–after study29 found an increase in ED use, but this was probably due to high levels of participants with substance abuse or psychosocial problems. A non-randomised controlled study28 and a before–after study10 reported no change in ED use, but possibly lacked power. Patient outcomes such as drug and alcohol use, health locus of control, patient satisfaction and psychological functioning were evaluated three studies, but no change was reported.23 ,29 ,31
A majority of the studies included a detailed description of their intervention and CM activities were clearly identified. ‘Documenting patient goals and priorities’ was the activity less frequently reported. Many interventions did not consider patient health objectives in individualised services plan13 ,21 ,23 ,24 ,27 ,28 even if goal setting is recognised as an important component of CM.16 Although CM activities were well described in the studies included, key elements associated with successful CM interventions were scarcely discussed. Considering their complexity, it is essential to understand the main mechanisms underlying CM activities and go beyond the cause–effect relationship by including a process evaluation considering the influence of contexts on outcomes.32 An explanatory analysis on how CM intervention works, in what populations/subpopulations, and in what circumstances and contexts is necessary to identify modifiable factors influencing intervention effects.33 These results would be very relevant for researchers and decision-makers who plan to implement CM interventions.
The studies included pointed out several problems in assessing the efficacy of CM interventions designed to manage frequent users. First, ED visits of frequent users show a natural decrease over time23 ,28 ,34 ,35 and regression to the mean may bias outcomes36 measured in before–after studies that demonstrated a reduction in ED use.13 ,27 ,30 ,31 Pragmatic randomised trials may help to attribute a reduction in use of care for frequent users of CM interventions and produce results that can be generalised to clinical practice settings, more than in a traditional controlled randomised trial.37 Second, case finding, that is, the identification of participants who will benefit the most from the intervention, could also affect results as shown in the study by Segal et al22 where experimental groups included only 5% of patients at risk of future hospital admission. In addition to the identification of frequent users based on data from hospital electronic medical records, opinion of healthcare providers is recommended to properly identify patients likely to be willing and able to participate in a CM intervention.38 Finally, many of the included studies had a small sample of frequent users10 ,23 ,28 ,29 and could result in a lack of power where effects are harder to detect. The fact that frequent users are vulnerable populations who may be reluctant to participate39 and represent only a small proportion of patients1–3 could explain the low sample size of the included studies.
Our review has some limitations. Conducting a meta-analysis of the effectiveness of CM interventions for frequent users of healthcare services would have contributed to fill gaps in the possible lack of power of some included studies, but the heterogeneity across studies in terms of definition of frequent users, healthcare settings and CM interventions makes direct comparisons difficult. Another limitation of a scoping review is the potential omission of relevant articles, as well as any unpublished material. Our search strategy relied on key words assigned by authors and may have missed relevant studies on the effectiveness of CM. However, our search strategy was adapted for different databases, and enabled an exhaustive literature review. Moreover, we identified further articles through hand searching. Finally, it would be interesting to conduct an evaluation of the quality of the studies included. However, the scoping review method does not imply an evaluation of quality because it aims to provide a description of available research rather than determine robust or generalisable findings.
Conclusion
In conclusion, our review suggests that CM could reduce ED visits and hospitalisations as well as cost, but additional studies still need to clearly confirm its effectiveness. Pragmatic randomised controlled trials of adequate power and the recruitment of well-defined frequent users of healthcare services are needed. The effectiveness of CM to improve patient outcomes such as self-management and experience of care would also have to be evaluated.
Acknowledgments
The authors thank Ms Susie Bernier for her editorial assistance.
References
Footnotes
Contributors CH and M-CC conceived the review and participated in its design and coordination. ML conducted the data collection and drafted the manuscript under the guidance of CH and M-CC. All authors were involved in drafting and editing the manuscript.
Funding This review was supported by the Canadian Institute of Health Research (CIHR).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.