Article Text

Abstract
Objectives This prospective cohort study aimed to investigate whether there are differences in health outcomes among persons with mild or moderate injuries who were hospitalised compared with those not hospitalised following a road traffic crash.
Setting Sydney Metropolitan, New South Wales, Australia.
Participants Persons aged ≥18 years involved in a motor vehicle crash were surveyed at baseline (n=364), and at 12 (n=284) and 24 months (n=252). A telephone-administered questionnaire obtained information on a range of socioeconomic, and preinjury and postinjury psychological and heath characteristics of all participants.
Primary outcome measure Participants who reported admission to hospital for 24 h or more (but less than 7 days) after the crash were classified as being hospitalised; those admitted for less than 24 h were classified as non-hospitalised.
Results Around 1 in 5 participants (19.0%) were hospitalised for ≥24 h after the crash. After adjusting for age and sex, hospitalised participants compared with those not hospitalised had approximately 2.6 units (p=0.01) lower Short Form-12 Physical Component Summary (SF-12 PCS) scores (poorer physical well-being) and approximately 4.9 units lower European Quality of Life visual analogue scale (EQ-VAS) scores (p=0.05), 12 months later. After further adjusting for education level, whiplash, fracture and injury severity score, participants who were hospitalised had approximately 3.3 units lower SF-12 PCS (p=0.04), 12 months later. The association with EQ-VAS did not persist after multivariable adjustment. No significant differences were observed between the 2 groups in health outcomes at 24-month follow-up.
Conclusions These findings indicate that long-term health status is unlikely to be influenced by hospitalisation status after sustaining a mild/moderate injury in a vehicle-related crash.
- PUBLIC HEALTH
- REHABILITATION MEDICINE
- ACCIDENT & EMERGENCY MEDICINE
- EPIDEMIOLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study has a prospective design and availability of rich, confounder data including sociodemographic and a range of preinjury correlates.
This study used compensation system data which could lead to selection bias, that is, compensable persons might not represent the broader injury population.
Recall bias may have been more pronounced in our study due to the 3-month delay between the injury event and measurement of recalled preinjury characteristics at the baseline survey.
Introduction
In Australia, musculoskeletal injuries are the most common type of injury sustained following a road traffic crash.1 Injured people with poor recovery generate the highest costs1 ,2; hence, it is important to understand the burden and predictors associated with poor outcomes following vehicle crash-related injuries. Few studies have investigated outcomes for non-hospitalised people, perhaps due to the assumption that injured people who are not hospitalised are likely to have short recovery periods.3 ,4
A Dutch study showed that people followed up after an emergency department (ED) visit for an injury had recovered to a functional level equivalent to the general population, while those admitted to hospital for their injury had not.5 Conversely, a meta-analysis found poor outcomes associated with injuries not commonly involving hospitalisation (eg, sprains and strains).6 The UK Burden of Injury Study also estimated considerable burden following injury for people seen in ED but not hospitalised, partly due to the greater numbers with injuries not resulting in hospitalisation.7 Recently, the New Zealand Prospective Outcomes of Injury Study (POIS)3 showed that disability was experienced by 53.6% of the hospitalised group 3 months after injury, while 39.4% of the people not hospitalised were also experiencing disability at this time. By 24 months after injury, a 13% prevalence of disability was reported for both groups, which was higher than the preinjury prevalence of disability (5%).8
We hypothesise that hospitalisation could be associated with greater injury severity and other factors such as iatrogenesis (adverse condition induced in a patient by a physician's activity or therapy), and reinforcement of illness behaviour that could worsen health outcomes in the longer term. However, to best of our knowledge, there have been no longitudinal studies that have compared the health status of hospitalised versus non-hospitalised persons who sustained a minor injury in a road traffic crash, and who had made compensation claims. Hence, using a cohort of people with mild/moderate injuries (eg, whiplash and leg fracture) following a motor accident, we aimed to establish whether there are differences in health status (quality of life measures and pain severity) between hospitalised and non-hospitalised injured persons at 12 and 24 months, independent of potential confounders.
Methods
Study population
Potential participants were identified from the New South Wales (NSW) Motor Accident Authority (MAA) Personal Injury Registry database. The MAA is the government regulator of companies providing third party motor vehicle accident insurance in NSW. This database consists of people who made claims on the Compulsory Third Party scheme. Claimants aged ≥18 years who had sustained injuries in a motor vehicle crash in NSW between March and December 2010 were identified and invited to participate in the study. Participants were excluded if they: (1) sustained catastrophic injuries (severe traumatic brain injury or spinal cord injury; (2) had an injury requiring hospitalisation for more than 7 days; (3) had a New Injury Severity Score (NISS) >8; (4) were unable to complete questionnaires by telephone in English; and/or (5) if contact could not be initiated within 60 days of the crash date.
A total of 1515 insurance claims that were lodged between March 2010 and December 2010 were deemed to be potential participants (figure 1), and the individuals who had lodged these claims were sent a letter of invitation by the MAA together with the Participant Information Sheet. An opportunity to opt out of the study within 2 weeks was provided, following which, verbal consent was sought. As the survey was conducted over the phone, obtaining verbal consent was deemed to be appropriate. Completion of the survey was documented as giving consent to participate, and this was recorded by the research nurse who administered the survey.
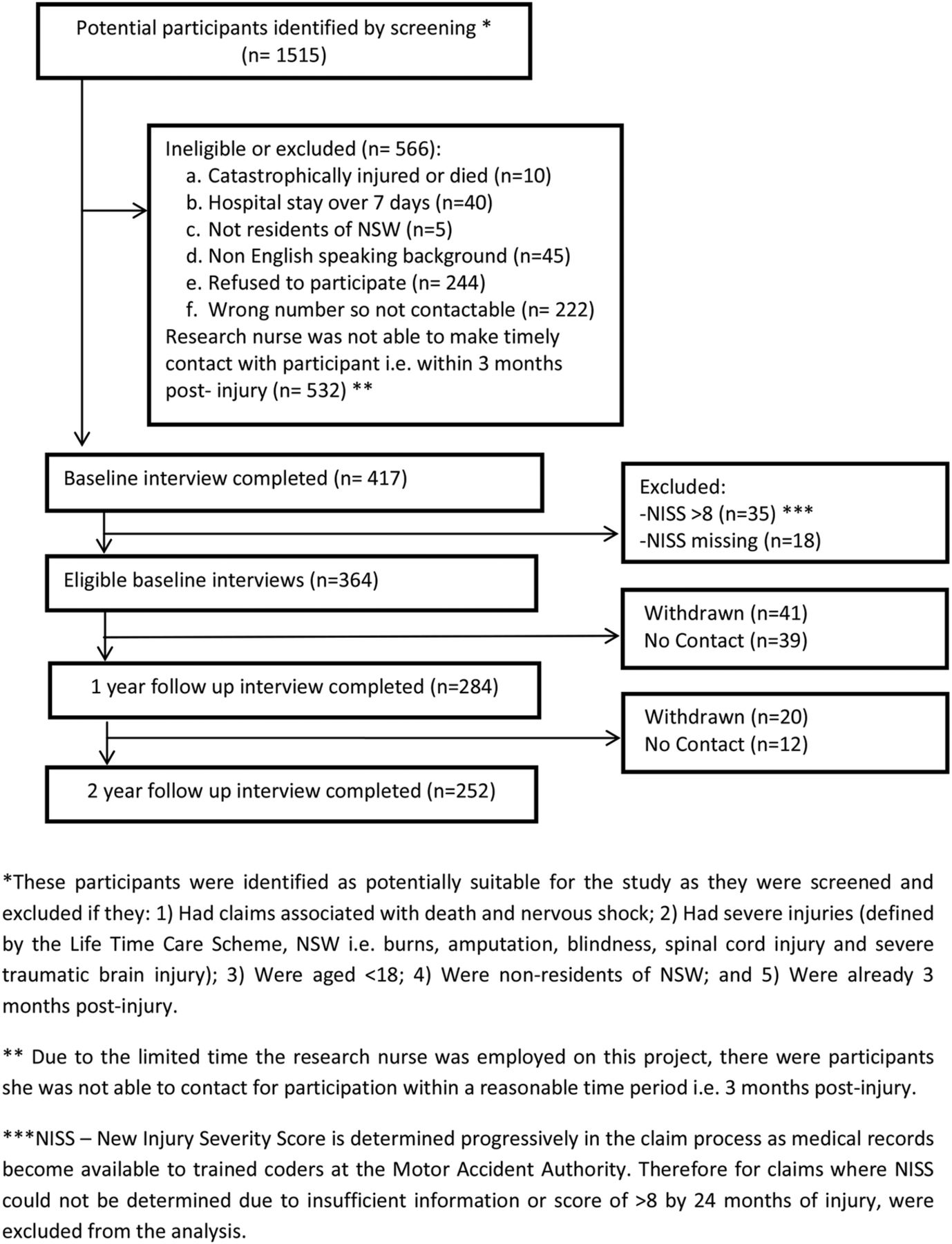
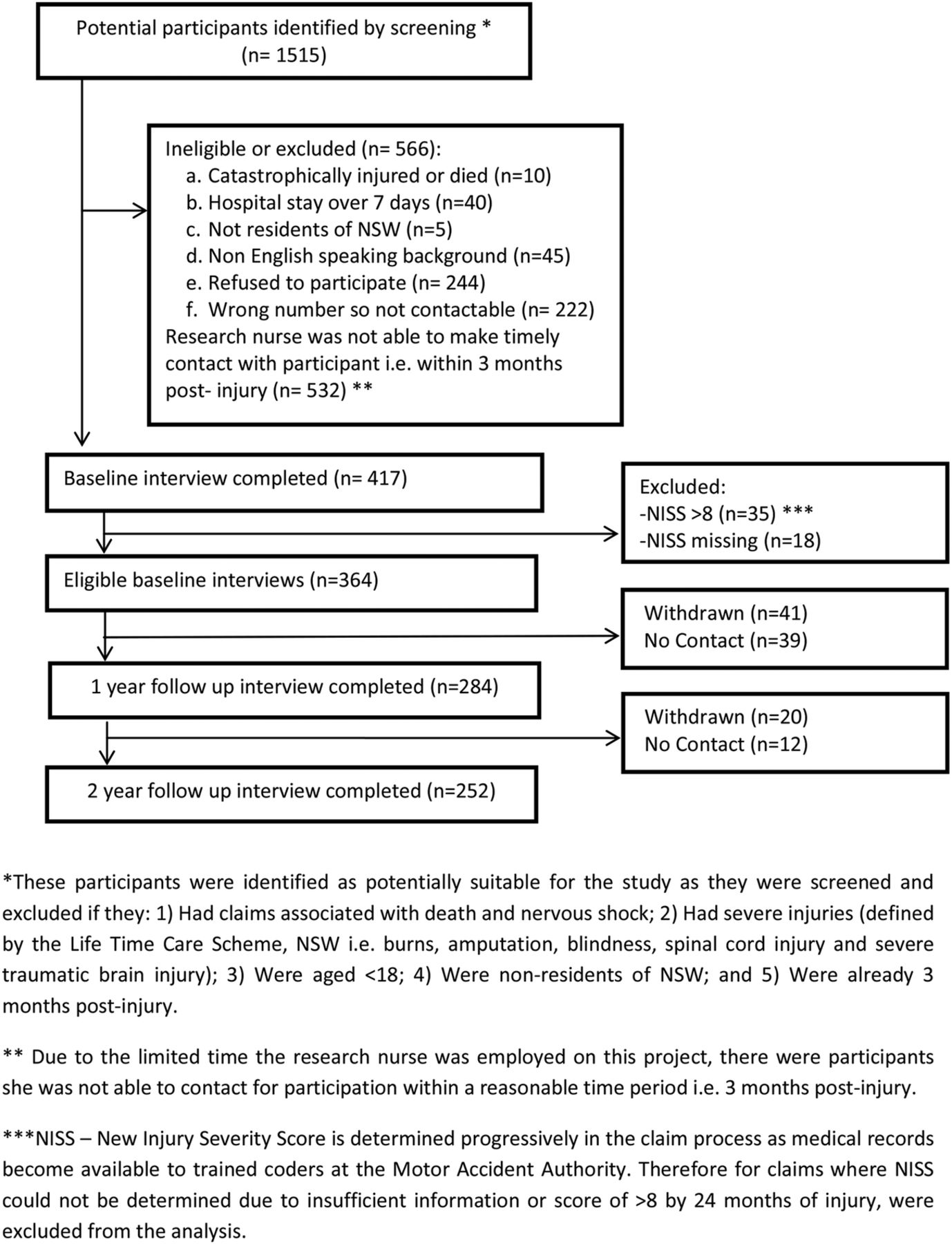{kind=link}
Flowchart of study participation.
Determining hospitalisation status
Participants in the study were interviewed by telephone by a trained and experienced research nurse, and the interview schedule was structured and used a closed response format. Participants were asked how many hours they had spent in hospital after the crash. They were then dichotomised into those who spent <24 h in hospital (non-hospitalised group) and those who spent ≥24 h or more in hospital (hospitalised group) after the crash.
Assessment of sociodemographic, psychological, injury-related and health-related predictors
Trained and experienced coders were used to code the reported injuries. The Abbreviated Injury Scale coding system was used to classify the participants into: mild (1–3) and moderate (4–8) injury groups based on the NISS.9 Around 17 trained and experienced coders were used to code the reported injuries. Chronic illness was determined by asking participants if they had been diagnosed with any of the following: asthma, cancer, heart or circulatory condition, diabetes, mental and behavioural problems, and/ or other in the past 3 months. If participants reported that they had had any of the above long-term illnesses for more than 3 months, they were considered as having a chronic illness. Chronic pain was characterised by participants reporting that they had been diagnosed with the following for more than 3 months: arthritis, and neck or back problems/disorder.
Participants were asked to describe their general health status prior to the motor vehicle accident, using a five-point Likert scale (excellent, very good, good, fair or poor). Body mass index (BMI) was calculated from self-reported height and weight. BMI was classified according to WHO guidelines: <20 kg/m2 (underweight), 20–24.9 kg/m2 (normal), 25–29.9 kg/m2 (overweight), ≥30 kg/m2 (obese).
The Pain-Related Self-Statements Scale-Catastrophizing Subscale (PRSS-Catastrophizing) is a nine-item self-report inventory that measures the frequency of a patient’s catastrophic cognitions that may impede the individual’s ability to cope with severe pain.10 Patients were asked to rate the frequency with which they experience particular catastrophic thoughts during an episode of pain, and the overall score is calculated with a range of 0 (almost never) to 5 (almost always), with higher scores reflecting more frequent endorsement of catastrophic thoughts. The total score for all items was divided by 9 to obtain a mean item score. The PRSS-Catastrophizing is a well-validated and widely used measure in clinical chronic pain samples.10 ,11
Assessment of health outcomes
The European Quality of Life-5 Dimensions (EQ-5D) questionnaire was used to measure health-related quality of life.12 The first part of the EQ-5D has five dimensions: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. Each dimension is divided into 3° of severity: no problem, some problems and major problems. The EQ visual analogue scale (EQ-VAS) is a 20 cm scale which was modified slightly from the original version with a repetition of the question: ‘To help you say how good or bad your health state is, I have a scale in front me (rather like a thermometer), on which the best health state you can imagine is marked 100 and the worst health state you can imagine is marked 0. How would you rate your health on this scale?’12 ,13 The Medical Outcomes Survey Short Form-12 (SF-12) was used as another measure of health-related quality of life.14 The SF-12 has 12 questions selected from the SF-36 Health Survey.15 Scoring of the SF-12 provides results on eight domains (physical functioning, role limitations due to physical problems, bodily pain, general health, vitality, social functioning, role limitations due to emotional problems and mental health). Two component scores, the physical and mental component summaries (ie, SF-12 PCS and SF-12 MCS), are derived from the domain scores; the domain scores and component scores are standardised to a mean of 50 and SD of 10. An average overall pain severity was assessed using a 0 (no pain) to 10 (worst pain imaginable) Numeric Rating Scale (NRS).
Statistical analysis
Univariate analysis was performed using χ2 test for dichotomous variables. Fisher's exact test was applied where appropriate. Trend in proportions was tested using χ2 for trend (degree of freedom 1). Repeated measures analysis of variance was used to test the impact of hospitalisation on a range of outcomes. These analyses were first adjusted for age and sex, and then further adjusted for baseline education level, whiplash, fracture and NISS. The short-term and long-term impacts were assessed separately at 12-month and 24-month follow-up. At 12 months, participants included in the analysis were claimants who responded to both interviews at baseline and follow-up. This was also applicable at 24-month assessment. Owing to the loss to follow-up, the number of participants at both assessments was different. All statistical analyses were done using SPSS V.19.0. The level of significance was set at 0.05.
Results
Of the 1515 potential participants, 1098 were not eligible or refused to participate (figure 1). Of the remaining 417 who participated in the baseline interview, 53 were excluded as they had missing NISS or an NISS >8 (severe injury). This left 364 participants that could be included in analyses. Twelve-month and 24-month follow-up assessments were completed on 284 (78% of eligible participants at baseline) and 252 (69% follow-up rate) of 364 enrolled and eligible participants, respectively (figure 1). Table 1 shows the baseline characteristics of those followed up at 12 months (n=284) compared with those who were not followed up past baseline, that is, they were not surveyed at 12 months or beyond (n=80). Participants compared with non-participants did not significantly differ in any of the baseline study characteristics. Similarly, participants at 24 months (n=252) did not differ in any of the study characteristics compared with those participants who were surveyed at 12 months but not at 24 months (n=32; data not shown). At baseline, participants hospitalised for 24 h or more (n=69) compared with those hospitalised for less than 24 h after the crash (n=295) were more likely to be male, have a moderate injury and fracture, but less likely to be tertiary qualified and have whiplash (table 2).
Study characteristics of participants compared with non-participants not followed up past the baseline survey (ie, did not participate in the 12-month follow-up onwards)
Sociodemographic, psychological, health and injury-related characteristics of participants at baseline, stratified by hospitalisation status (n=364)
Table 3 shows that after adjusting for age and sex, participants who were hospitalised for ≥24 h or more compared with those hospitalised for <24 h after the crash had 2.6 (p=0.01) and 4.9 units (p=0.05) lower SF-12 PCS and EQ-5D VAS scores 12 months later, respectively. The association between hospitalisation status and lower SF-12 PCS (∼3.3 units difference) persisted after further adjusting for education level, whiplash, fracture and injury severity score (p=0.04; table 3). However, the association with EQ-5D VAS became non-significant (p=0.07), after multivariable adjustment. Further, at 24-month follow-up, there were non-significant differences in all quality of life measures and pain NRS scores between participants hospitalised for ≥24 h and those hospitalised for <24 h (table 4).
Quality of life scores and severity of pain among hospitalised and non-hospitalised participants 12 months after a mild/ moderate injury (n=284)
Quality of life scores and severity of pain among hospitalised and non-hospitalised participants 24 months after a mild/moderate injury (n=252)
Discussion
Around one in five participants (19.0%) with a mild or moderate injury sustained in a road traffic crash were hospitalised for 24 h or more. Participants who were hospitalised for 24 h or more compared with those hospitalised for less than 24 h at baseline, had significantly lower (worse) SF-12 PCS and EQ-VAS scores at the 12 month follow-up, after adjusting for age and sex. This association between hospitalisation status and poorer physical well-being (significantly lower SF-12 PCS scores) persisted after further adjusting for education level, whiplash, fracture and injury severity scores. However, hospitalised and non-hospitalised participants did not differ appreciably in health status after 24 months.
Univariate analyses indicated that a greater proportion of the hospitalised compared with the non-hospitalised group were male and not tertiary qualified. These data concur with findings from other injury cohorts (eg, head injury), which demonstrated that the length of stay in hospital and likelihood of readmission to hospital is influenced by an individual's social circumstances, for example, education.16 Given that the NISS was shown to be an accurate predictor of the length of hospital stay in a general urban trauma population,17 and also among those with multiple orthopaedic injuries,18 it was not surprising that the univariate analyses showed a greater proportion of those who were hospitalised ≥24 vs <24 h having a fracture or moderate injury severity score.
Interestingly, we found that those who were hospitalised ≥24 h compared with those hospitalised for <24 h were less likely to have sustained a whiplash injury in the road traffic crash. Similar findings were reported in a Swedish study showing a low proportion of persons with whiplash injury after a road traffic accident being admitted to the hospital (4%), for not more than 5 days.19 Specifically, the Swedish research showed that 52% of those with whiplash injury sought help from primary healthcare units or from hospital care (48%), where they were sent without treatment or discharged with a prescription (eg, analgesics) and a referral to a physiotherapist.19 Our findings also reinforce that a greater proportion of individuals with whiplash diagnosis are less likely to be admitted to a hospital for long periods, and possibly more likely to seek help from primary care.
Age-adjusted and sex-adjusted analyses showed that participants who were hospitalised for ≥24 h versus those hospitalised for <24 h demonstrated poorer physical functioning and lower overall well-being (ie, lower EQ-VAS scores) 12 months later. However, the only significant association that persisted after multivariate adjustment for other factors such as education, whiplash, fracture and injury severity, was with SF-12 PCS scores or physical well-being. These findings indicate that those who have been hospitalised for 24 h or more at baseline are individuals that are more likely to have poorer physical functioning 12 months after the injury. There have been prior studies to suggest that the PCS score is inversely associated with length of hospital stay.20 The observed magnitude of difference in adjusted mean SF-12 PCS scores between those hospitalised ≥24 and those hospitalised for <24 h (∼3.3 units) after 12 months is considered clinically meaningful, as it falls within the range of 3–10 points which was previously defined as a meaningful difference in quality of life scores in a clinical setting.21 We need to caution, however, that all study participants were engaged in the compensation process, and previous research has shown that persons who claimed compensation had overall worse health status and impeded recovery following mild to moderate injuries in the longer term.1 ,22 Therefore, it is not possible to conclusively delineate whether the negative effect on physical well-being is due to hospitalisation per se, or due to the possible negative effects of engagement with the compensation process, or both.
Among persons with mild or moderate injuries, hospitalisation status was not an independent predictor of general health status at either 12 or 24 months after accounting for the effects of socioeconomic status (ie, education) and injury-related variables such as whiplash, fracture and injury severity scores. This finding is consistent with the POIS8 comprising a range of injury types, which reported non-significant differences in 24-month disability ratings between the hospitalised and non-hospitalised groups. Nevertheless, we cannot discount that our relatively small sample size could have led to insufficient study power to detect a modest association between hospitalisation status and specific health outcomes over 24 months. We also stress that our conclusions are not applicable to people with catastrophic or severe traumatic brain or spinal cord injuries. Further population cohort studies of people with mild/moderate injuries with larger sample size are warranted to confirm or refute our findings.
The strengths of our study are its prospective design and availability of rich, confounder data including sociodemographic and a range of preinjury correlates. Limitations also deserve discussion including that our study used compensation system data which could lead to selection bias. However, selection bias as a result of loss to follow-up is likely to be minimal, as participants compared with those who were not followed up at 12 and/or 24 months did not differ significantly in terms of baseline characteristics. We need to caution that compensable persons might not represent the broader injury population, and that associations between hospitalisation status and future health outcomes could be different in non-compensable groups. Also, just over one-third of potential participants identified at the initial screening of the compensation database were not able to be contacted within 3 months of the injury (see figure 1). This is a relatively substantial number of participants who could not be included in this study; hence, we cannot discount the possibility that these missing data are likely to have influenced observed associations. Finally, recall bias may have been more pronounced in our study due to the 3-month delay (or sometimes more before participants were interviewed, even though initial contact was made by 3 months) between the injury event and measurement of recalled preinjury characteristics at the baseline survey.23
In summary, this unique study shows that being hospitalised following a non-catastrophic injury sustained in a road traffic crash independently predicts poorer physical health or functioning 12 months later. Our cohort study, however, suggests that hospitalisation status is unlikely to influence the health status of persons with mild or moderate injury in the longer term or 24 months after the injury. Additional population-based cohort studies with a large sample size are required to confirm or refute our findings, particularly given the current lack of temporal data on the relationship between hospitalisation status and health outcomes following a non-catastrophic injury.
References
Footnotes
Contributors BG, JJ and IDC were involved in study concept and design. IDC was involved in acquisition of data. BG, DS, IDC, CGM, MN and FB were involved in analysis and interpretation of data. BG was involved in drafting of the manuscript. BG, JJ, IAH, MN, CGM, PC, FB, DS and IDC were involved in critical revision of the manuscript.
Funding The work was supported by the Motor Accidents Authority of New South Wales. CGM and IDC's fellowships are funded by the Australian National Health and Medical Research Council.
Competing interests None declared.
Patient consent Obtained.
Ethics approval This study was approved by the University of Sydney Human Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.