Article Text

Abstract
Objectives Although various effective interventions are available to help individuals quit smoking, the effect of educational levels on cessation rates has rarely been studied, and of the few intervention studies on this topic, the results have been conflicting.
Design and setting From October 2008 to August 2013, a partly retrospective non-randomised study was conducted in a smoking cessation clinic of a large general hospital in Beijing, China.
Participants In total, 547 Chinese smokers who sought treatment were divided into two groups: a face-to-face counselling group (FC, n=149) and an FC group subjected to four telephone follow-up sessions (FCF, n=398).
Outcomes We evaluated self-reported cessation rates by day 7 and after 6 and 12 months and stratified the two groups by education levels.
Results The 7-day and 6-month and 12-month continuous cessation rates of smokers of low education levels in the FC group at the time of the 12-month follow-up were 12.5%, 7.1% and 7.1%, respectively, which were lower than those of the highly educated smokers (16.1%, 12.9% and 9.7%, respectively). The results were opposite for the FCF group. The corresponding results for the highly educated smokers of the FCF group were 25.0%, 17.2% and 10.3%, respectively, which were lower than those for the smokers of low education levels (28.3%, 22.9% and 18.1%, respectively). However, significant differences were observed only among the FCF group participants who had experienced 12 months of continuous abstinence, and the crude OR for these individuals was recorded at 0.52 (0.29 to 0.93), p=0.03. A stepwise logistic regression showed that education levels may play a role in various intervention methods. Being married and higher Fagerström test scores were also predictors of cessation tendencies.
Conclusions Education levels may affect the benefits of booster counselling sessions on smoking cessation among Chinese smokers.
- EPIDEMIOLOGY
- PUBLIC HEALTH
- SOCIAL MEDICINE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This partly retrospective non-randomised study evaluated the effect of ‘booster’ counselling sessions provided in combination with brief face-to-face counselling sessions with Chinese patients visiting a smoking cessation clinic.
The present study shows that education levels have varying effects on various types of behavioural supports; smokers with lower levels of education benefited more from the boosters.
Further trials comparing various levels of behavioural support should report outcomes stratified by educational levels.
Although the data were collected systematically in a smoking cessation clinic, the study is limited by its small sample size.
The findings are largely based on self-reports; thus, socially desirable responses may have been given.
Introduction
Tobacco consumption constitutes a major global public health challenge, especially in China. According to the Global Adult Survey conducted in 2010, smoking prevalence in China was recorded at 52.9% among men and 2.4% among women.1 ,2 In China, where smoking cessation and cessation services are in their infancy, smoking cessation services are scarce and of limited effectiveness. Although they have been proven effective in clinical practices in Mainland China,3 smoking cessation medications are too expensive to be used widely among Chinese smokers, especially among low-income smokers. Therefore, cost-effective ways of increasing cessation success rates in China are urgently needed.
Previous results of cross-sectional and population-based surveys have shown that smokers with higher levels of education or who occupy higher social positions are more likely to intend or attempt to quit or to refrain from smoking.4–6 Although there are various effective interventions that help individuals quit smoking,7–10 the effect of educational levels on cessation rates has seldom been studied, and the results of the few intervention studies that have been conducted are conflicting. Some of these studies have reported that higher education levels are associated with higher cessation rates.11–13 However, one study found the opposite result,14 and other studies have found no relationship between education levels and cessation rates.15 ,16 Although the results were not significant, two Chinese studies have implied that smokers with low levels of education are more likely to quit smoking in Mainland China.17 ,18 Most intervention studies have not reported on the frequency and intensity of counselling sessions or did not use a control group.
Given the conflicting results of previous studies, we hypothesise that educational levels may play various roles in various types of behavioural supports (different counselling frequencies and intensities). This study evaluates the impact of education levels on various intervention groups. We compare the effect of one session of face-to-face individual counselling in combination with four follow-up telephone counselling sessions (FCF) with that of face-to-face counselling alone (FC); both groups are stratified by education level. We apply a smoking cessation intervention of standard intensity levels in one of the longest running Smoking Cessation Clinics (SCC) in Mainland China.
Methods
The investigation involved an observational study based on a retrospective analysis of data collected systematically in an SCC. We established an SCC in the outpatient department of the People’s Liberation Army General Hospital in Beijing, which is one of the largest hospitals in China. The SCC began operations on 22 October 2008 and still exists. Trained physicians provide services similar to those offered in Hong Kong on 4-weekday evenings (Monday to Thursday, from 18:30 to 21:00).19 The participants were smokers who voluntarily sought treatment from our SCC and paid a ¥7 (US$1) registration fee.
Before the baseline treatment was offered, each clinic attendee was asked to sign an informed consent form. Information on the project objectives (their data were used only for scientific research), assessments and data collection methods was reported on a paper form. Each participant was also asked for a telephone number that he or she could be reached at for the follow-up interviews.
Inclusion and exclusion criteria
Study subjects were required to satisfy the following inclusion criteria: (1) current smokers (who smoked daily for at least 6 months at the time of the survey),20 Chinese, 18 years of age or older, and (2) consent to participate in the follow-up sessions and completion of an informed consent form. Subjects who were cognitively impaired (deaf, could not understand and complete the questionnaire reliably, etc.) were excluded from the study.
Subject recruitment and intervention
The FC group and FCF group included smokers who voluntarily sought treatment from our SCC in the PLA general hospital. Each smoker received the same intervention treatment at the time of his or her first visit, and no smoking cessation medications were provided. The participants’ smoking and related information was assessed using a baseline questionnaire in a face-to-face interview that lasted approximately 10 min prior to counselling. The physician then provided individual FC based on Prochaska's transtheoretical model21 and on the ‘five A's’ (ask, advise, assess, assist and arrange), lasting at least 30 min. The physician assessed each client's readiness to quit smoking, strengthened each client's motivation to quit smoking using the ‘five R's’ (relevance, risks, rewards, roadblocks and repetition),22 and provided advice on ways of overcoming psychological cravings, psychological dependence and sociocultural factors associated with tobacco dependency.19
After the baseline intervention, smokers who visited our clinic from October of 2008 to December of 2010 (n=254) participated in follow-up telephone conversations with counsellors after the first week and after one, three, 6 and 12 months. At the first week and first, third and sixth month follow-up meetings, after each client's smoking or cessation status was assessed, we conducted a ‘booster’ session and asked whether the smokers or quitters had experienced any problems, offered problem-oriented suggestions or advice when necessary, and encouraged the clients to quit or to continue abstaining from smoking. Each follow-up lasted approximately 15–20 min.
In studying the effect of the follow-up booster session, we could not perform a randomised controlled trial (RCT) under clinical conditions as randomly allocating the smokers to two groups with different follow-up interventions would have confused the smokers as they sought a service and did not expect to be randomised. Given the uncertainties regarding whether the follow-up booster was effective, we ceased booster counselling for all of the smokers first counselled in 2011. These smokers were given the same telephone follow-up assessment by trained counsellors after the first, third and sixth months that strictly involved conversations about smoking and quitting and that involved no further counselling. Each follow-up session lasted approximately 2–3 min. These smokers constituted the FC group (FC, n=149).
After 2011, we resumed the follow-up booster counselling sessions for all of the smokers. Those participating from February of 2012 to August of 2013 (n=144) and those participating from October of 2008 to December of 2010 formed the FC plus FCF group (total n=398). We completed 12 months of follow-up sessions with all of the smokers in August of 2014.
All participating physicians and counsellors completed a smoking cessation training programme and passed the required examinations. To guarantee the integrity and quality of the counselling services, the counsellors were supervised throughout the project. The counsellors were instructed to contact the smokers of the two groups at least seven times on different days before removing them from the follow-up group. The physicians who provided baseline counselling were unaware of the grouping methods. Although the counsellors who administered the follow-up booster sessions could not be blinded to the participants and their objectives during the booster sessions, they were not informed of the aims of the research and thus recorded tobacco use status levels with minimal subjective bias.
Data collection
Data collection was performed during the first visit and at each follow-up interview with the use of standardised and structured questionnaires. The questionnaires were developed on the basis of those widely used in Hong Kong.19 ,23 The following baseline demographic data were collected for each patient: age, marital status, occupation and monthly family income. Education levels were categorised as low (high school and below, including primary, intermediate and high school degrees; 0–12 years of formal schooling) and high (college and above, including tertiary education, higher vocational school degrees, and college or university degrees; more than 12 years of formal schooling).17 Tobacco-related questions focused on each client's readiness to quit smoking (precontemplation, contemplation, preparation and action); smoking history; smoking status; smoking destinations; cessation history; cessation motivations; and perceived confidence, importance and difficulties associated with smoking cessation (all three were based on a scale of 1–100, from the least to the most). All smokers were submitted to the Fagerström Test for Nicotine Dependence (FTND), and their dependence was classified as low (0–3), moderate (4–5) or severe (6–10).21 Exhaled carbon monoxide levels were measured by trained technicians following a standard protocol and a Micro CO Smokerlizer.23 Additional questions focused on previous medical advice given on smoking cessation, on physician diagnoses of tobacco-related chronic diseases and on alcohol use. The follow-up questionnaires were similar to the baseline questionnaires, with the omission of redundant questions and the addition of questions on cessation times, cessation attempts and withdrawal symptoms.
Statistical analysis
The data were entered (double entry) using Epidata (3.1) and were analysed using SPSS (Inc., Chicago, Illinois, USA) for Windows (19.0). The baseline characteristics were described via descriptive statistics. Cessation prevalence according to the baseline factors was compared with the χ2 test results. We employed forward stepwise logistic regressions to identify independent predictors of cessation success and to calculate adjusted OR and 95% CIs. Following intention to treat (ITT) analysis principles, smokers who could not be contacted during the follow-up period were considered non-quitters or non-reducers. A per protocol (PP) analysis was performed by excluding those who did not participate in the follow-up sessions as part of a sensitivity analysis. All of the p values were two sided, and p<0.05 was employed as the level of statistical significance.
The 7-day cessation condition was defined as smoking cessation for the past 7 days at the time of the 12-month follow-up following the USA Clinical Practice Guidelines.22 Six-month and 12-month continuous cessation rates were defined as smoking cessation over the past 6 or 12 months, respectively, at the time of the 12-month follow-up session. All of these results were self-reported by the smokers, and some of them were confirmed via biochemical validation.
Results
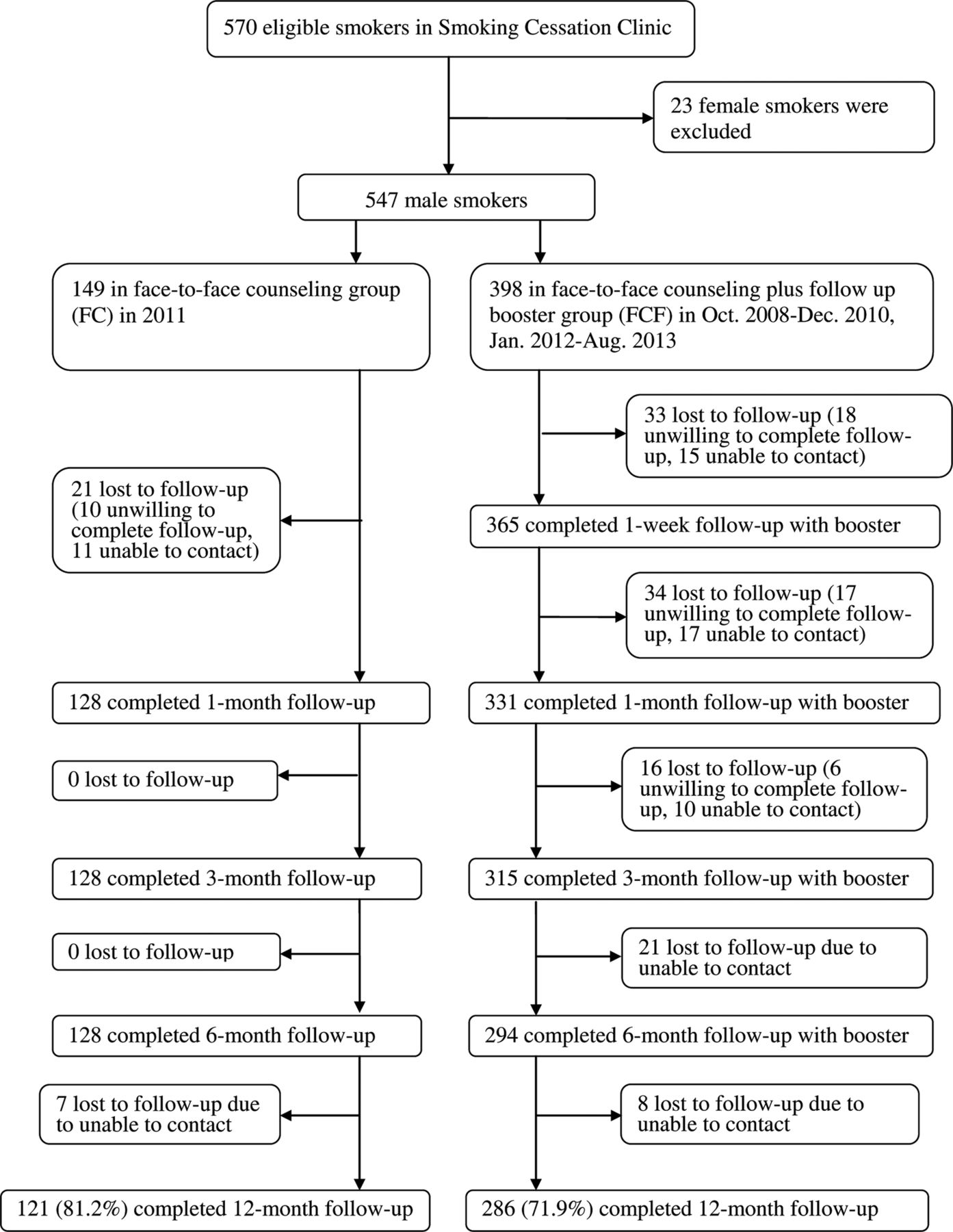
From 22 October 2008 to 31 August 2013, 547 eligible smokers were seen. By 31 August 2014, 407 smokers had completed the 12-month follow-up process, and 140 smokers (18.8% in FC, 28.1% in FCF, and 25.6% in total) did not participate in the follow-up session, primarily due to lack of contact (figure 1). These 140 individuals shared similar baseline demographic features and other characteristics with the 407 clients who completed the 12-month follow-up process (see online supplementary appendix table S1).

{kind=link}
Attrition flow chart.
Demographic and tobacco-related characteristics and other factors
This study examined 547 smokers, and the mean age of the smokers was 41.0 years, with an SD of 11.1. Most of the smokers were married (87.6%), currently employed (79.7%), smoked more than 20 cigarettes per day (61.6%) and had made prior cessation attempts (75.3%).
After we stratified each group into two education levels, the four groups were similar in most of the factors (table 1). Compared to well-educated smokers, smokers with a low level of education had lower incomes, were more likely to be unemployed, presented longer smoking histories and exhibited stronger intentions to quit smoking.
Demographic characteristics, tobacco related and other factors of 547 smokers in two groups of different education levels
Cessation rates
Overall, the 7-day and 6-month and 12-month continuous cessation rates of the FC group were recorded at 14.8%, 10.7% and 8.7%, respectively, which were lower than those of the FCF group (26.4%, 19.6% and 13.6%, respectively). Table 2 shows that according to the ITT analysis, at the time of the 12-month follow-up, the 7-day and 6-month and 12-month continuous cessation rates of the low education level smokers in the FC group were recorded at 12.5%, 7.1% and 7.1%, respectively, which were lower than those of the highly educated smokers (16.1%, 12.9% and 9.7%, respectively). However, inverse results were found for the FCF group. The 7-day and 6-month and 12-month continuous cessation rates of the highly educated smokers in the FCF group were recorded at 25.0%, 17.2% and 10.3%, respectively, which were lower than those of smokers with low levels of education (28.3%, 22.9% and 18.1%, respectively). However, only the 12-month continuous abstinence cessation rate of the FCF group showed a significant difference across educational levels (crude OR, 0.52; 95% CI 0.29 to 0.93; p=0.03). After adjusting for confounding variables, the difference was found to be marginally significant (adjusted OR, 0.59; 95% CI 0.29 to 1.21; p=0.15).
Quit rates of two groups at 12-month follow-up in 547 smokers by intention to treat N (%)
The PP analysis generated similar results, as shown in online supplementary appendix table S2. The 12-month continuous abstinence cessation rate of the highly educated smokers in the FCF group was significantly lower than that of the smokers with low levels of education, and the crude OR (95% CI) was recorded at 0.45 (0.25 to 0.81). The difference in the 6-month continuous abstinence cessation rate was marginally significant, and the crude OR (95% CI) was found to be 0.59 (0.35 to 1.01).
As shown in online supplementary appendix table S3, according to the ITT and complete case (PP) analyses, outcome patterns were similar for both FCF periods (from October of 2008 to December of 2010 and from January of 2012 to August of 2013), suggesting an absence of period effects.
Predictors of cessation
To diminish the confounding property of population differences, all factors were entered into the stepwise logistic model, with the exception of cigarette consumption (as cigarette consumption was a major item of the Fagerström test). According to the ITT analysis shown in table 3, low education levels in the FCF group and Fagerström test scores were strong predictors of smoking cessation at the time of the 12-month follow-up meeting for all cessation rates (7-day and 6-month and 12-month continuous cessation rates). Marital status was also a significant independent predictor of 6-month and 12-month continuous cessation rates.
By intention to treat, logistic regression (stepwise) analysis for adjusted OR for predictors of quitting at 12-month follow-up
The analysis of the 12-month continuous cessation rate showed that compared to smokers with low levels of education in the FC group, the ORs (95% CI) of highly educated smokers in the FC and FCF groups and of low education level smokers in the FCF group were 1.20 (0.34 to 4.16), 1.40 (0.46 to 4.28) and 3.06 (1.01 to 9.30), respectively. The Fagerström test score exhibited a negative dose–response relationship, wherein the ORs (95% CI) of the Fagerström scores of 4–5 and 0–3 were 3.34 (1.63 to 6.84) and 3.89 (2.00 to 7.57), respectively.
The cessation predictor results were almost identical according to the PP analysis (see online supplementary appendix table S4).
Discussion
Our SCC is one of the oldest part-time SCC in Mainland China for which research evidence on intervention effectiveness is scarce. Using systematically collected data, we evaluated the effectiveness of offering one FC session (40 min) in combination with four brief follow-up telephone counselling sessions (15–20 min each) in relation to the effectiveness of FC alone; we stratified the participant groups by education level. Our study generated new evidence of the impact of education levels on various intervention methods directed at Chinese male smokers. Although our study was not designed as an RCT, the results were most likely not affected by extraneous factors and may prove applicable to ‘real world’ contexts.
Sociodemographic factors may have impacted the smoking cessation tendencies of the smokers voluntarily participating in our clinic more relative to the general population. The smokers who participated in our SCC were largely middle-aged, which is consistent with China’s national census, which shows that the working population of 40–49 years of age exhibits the highest degree of smoking prevalence.2 Most smokers in our SCC exhibited higher levels of tobacco consumption and generated higher Fagerström scores than smokers in Hong Kong and Guangzhou and those represented in western SCC reports.17 ,23–25
In accordance with the results of previous reports,25–27 the telephone follow-up sessions significantly increased cessation rates. In this study, we found that the telephone follow-up sessions significantly increased both the 7-day and 6-month continuous cessation rates at the time of the 12-month follow-up sessions (the 12-month continuous cessation rate was marginally significant). However, after each group was stratified by education level, the results showed that education levels may play various roles in various intervention methods. In the FC group, the highly educated smokers were more likely to quit; and an inverse relationship was found in the FCF group. This study confirms previous research that shows that low SES groups are more likely to benefit from more intensive interventions,28 ,29 and low education levels typically correlate with low SES in China. Our study results are consistent with this conclusion. Smokers with low levels of education exhibit poor levels of health knowledge and weak comprehension skills, and thus they require more frequent and intensive psychological support. The well-educated smoker group included a larger proportion of middle-aged and currently employed individuals with higher family incomes. In China’s alcohol-consuming and tobacco-consuming culture, these smokers are more privileged and enjoy access to more forms of social entertainment that involve drinking and smoking in groups. These individuals also experience more work stress, which is relieved through drinking and smoking; thus, these individuals find it more difficult to quit. These individuals quit shortly after the first SCC visit, and the additional follow-up telephone sessions played a limited role.
This study showed that being married and lower levels of nicotine dependence were also significant predictors; these findings complement those of other recent studies.13 ,16 ,30 ,31 Smoking behaviours were found to be strongly related to social conventions and customs. Married smokers receive more support from family members, and thus they are more likely to quit. They experience fewer withdrawal symptoms as smokers with lower levels of nicotine dependence can quit easily after receiving smoking intervention services.
We did not detect other predictors of cessation found in previous reports (eg, older age, cessation action stage, occupation, lower cigarette consumption, and lower exhaled CO levels at the time of the first visit16 ,17 ,24 ,30–33). However, this may be attributable in part to differences in population characteristics and intervention methods, and thus a larger sample size is required when detecting more predictors in the future.
Our study presents several limitations. First, regarding our participant recruitment approach, smokers visiting the clinic were not assigned randomly. We did not perform a sample size calculation as quit rates are unpredictable. However, no statistically significant variations in demographic characteristics or tobacco consumption levels were found between the two groups. Although we adjusted for major confounding factors, undetected biases may have affected the results. Second, since approximately 65% of the smokers resided outside of Beijing, it was not convenient for them to return to our clinic for follow-up sessions and interviews. Only 49 smokers (9.0%) returned to the clinic and performed the biochemically validated test. Two of the 49 self-reported non-smokers showed carbon monoxide levels of more than 8 ppm, indicating that they had smoked (4.1%). Third, the smokers were volunteers and may have been more motivated to quit or less confident in their capacities to quit without professional help. Finally, although the counsellors were unaware of the study objectives, socially desirable responses (observer bias) may have been given.
In conclusion, this study shows that education levels may affect the benefits of repeated counselling sessions on smoking cessation directed at Chinese smokers. Smokers with low levels of education exhibited poor levels of health knowledge and weak levels of comprehension, and thus they were more likely to benefit from the telephone follow-up sessions. Such individuals must be offered more frequent and intensive psychological support than well-educated smokers. Thus, healthcare providers must employ both intervention methods while considering smoker education levels when identifying effective ways to help individuals quit smoking.
Acknowledgments
The authors thank Li Xiao, Jinghong Zhu and Jing Feng for their research assistance with the follow-up interview; Tai-hing Lam and Sophia S. C. Chan contributed to the establishment of the clinic and design of the interventions and provided training.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors LW, YH and BJ designed the study and analysed the data. BJ, FZ, QL, CZ, LZ, ML and HC helped in the data collection and field operations. LW wrote the manuscript.
Funding This study was supported by research grants from the National Natural Science Foundation of China, 81373080; Beijing Municipal Science and Technology Commission, Z121107001012070; Clinical Research Grants of Chinese PLA General Hospital, 2013FC-TSYS-1021, MJ201447.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The study was approved by the Independent Ethics Committee of the Chinese People’s Liberation Army General Hospital (S2013-066-01).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data on the quality appraisal of the included studies are available by emailing wlyg0118@163.com.