Article Text

Abstract
Introduction Childhood overweight and obesity tracks into adulthood, increasing the risk of developing future chronic disease. Implementing initiatives promoting healthy eating and physical activity in childcare settings has been identified as a priority to prevent excessive child weight gain. Despite this, few trials have been conducted to assess the effectiveness of interventions to support population-wide implementation of such initiatives. The aim of this study is to assess the effectiveness of a multicomponent intervention in increasing the implementation of healthy eating and physical activity policies and practices by centre-based childcare services.
Methods and analysis The study will employ a parallel group randomised controlled trial design. A sample of 128 childcare services in the Hunter region of New South Wales, Australia, will be recruited to participate in the trial. 64 services will be randomly allocated to a 12-month implementation intervention. The remaining 64 services will be allocated to a usual care control group. The intervention will consist of a number of strategies to facilitate childcare service implementation of healthy eating and physical activity policies and practices. Intervention strategies will include implementation support staff, securing executive support, consensus processes, staff training, academic detailing visits, performance monitoring and feedback, tools and resources, and a communications strategy. The primary outcome of the trial will be the prevalence of services implementing all healthy eating and physical activity policies and practices targeted by the intervention. To assess the effectiveness of the intervention, telephone surveys with nominated supervisors and room leaders of childcare services will be conducted at baseline and immediately postintervention.
Ethics and dissemination The study was approved by the Hunter New England Human Research Ethics Committee and the University of Newcastle Human Research Ethics Committee. Study findings will be disseminated widely through peer-reviewed publications and conference presentations.
Trial registration number Australian Clinical Trials Registry ACTRN12612000927820.
- PUBLIC HEALTH
- PREVENTIVE MEDICINE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
The study has a strong design incorporating random allocation and blinding of data collection interviewers.
-
The intervention consists of a broad set of intervention strategies and is based on a theoretical framework and past research evidence.
-
The study is one of only a handful of randomised trials of such interventions internationally, and the first of its kind in Australia.
Introduction
Globally the prevalence of child overweight and obesity is increasing, with 9% of children aged 0–5 years expected to be overweight or obese by the year 2020.1 Overweight and obesity in childhood tracks into adulthood,2 increasing the risk of developing a number of chronic health conditions. Given early childhood represents a critical period in the development of diet and physical activity behaviours, interventions that aim to improve such behaviours have been recommended to prevent the onset of obesity among young children.3–7
Childcare services have been identified as a key setting to create environments supportive of child healthy eating and physical activity.8 In developed countries, childcare services provide access to a large and growing number of children for prolonged periods each day.8–11 Evidence from randomised and quasi-experimental trials suggests that healthy eating and physical activity promoting policies and practices can increase time children spend being physically active, improve child fundamental movement skill proficiency, improve child diet quality in care and prevent excessive weight gain.12–15 As such, licensing and accreditation requirements and best practice guidelines for the childcare setting recommend that services implement a number of policies and practices to support healthy eating and physical activity.16–21
Despite such evidence and recommendations from best practice guidelines, childcare service implementation of healthy eating and physical activity policies and practices appears to be limited internationally17 and within Australia.22 Australian research, for example, suggests that just 48–50% of centre-based childcare services have a written physical activity policy, 46–60% programme time each day for fundamental movement skill development, while 25–28% provide opportunities each day for children to participate in sedentary screen time,22 and 60% of Australian preschooler lunchboxes contain more than one serve of high fat, salt or sugar foods or drinks.23
Without adequate implementation, the potential public health benefits of interventions to prevent childhood overweight and obesity in childcare services will not be realised. An agency for healthcare research and quality systematic review, however, identified no trials examining the effectiveness of interventions to improve childcare service implementation of healthy eating and physical activity promoting policies and practices.24 Further, trials published since the review search period have reported non-significant improvements or improvements in only a minority of healthy eating or physical activity policies of practices targeted by the intervention.13 ,14 ,25–27 Previous trials have also utilised a narrow set of implementation strategies (eg, workforce development and resource provision)14 ,28 or developed interventions without the guidance of conceptual or theoretical frameworks,13 ,28 limiting their potential effectiveness. Finally, most previous trials have been conducted on small numbers of childcare services (less than 20) limiting their capacity to guide approaches aimed at achieving population-level service improvements.27 ,28
Given the limitations of the existing evidence base, a randomised trial of a theoretically based, multicomponent implementation intervention to increase the implementation of healthy eating and physical activity policies and practices in childcare services in Australia will be conducted. This paper describes the protocol by which this trial will be conducted.
Methods and analysis
Study aim
The aim of this study is to assess the effectiveness of multicomponent intervention in increasing the implementation of healthy eating and physical activity policies and practices by centre-based childcare services.
Study design
The study will employ a parallel group randomised controlled trial design (see figure 1). A sample of eligible childcare services in the study region will be randomly selected and invited to participate in the trial. Sixty-four services will be allocated to receive a 12-month implementation intervention, and 64 services will be allocated to receive usual care and will serve as a control group. To assess the effectiveness of the intervention, across each service, surveys administered via computer assisted telephone interview (CATI) will be conducted with the nominated supervisor (service manager) and room leader (room supervisor) caring for children 3–5 years. The surveys will be conducted at baseline and immediately postintervention. CATI interviewers will be blind to group allocation.
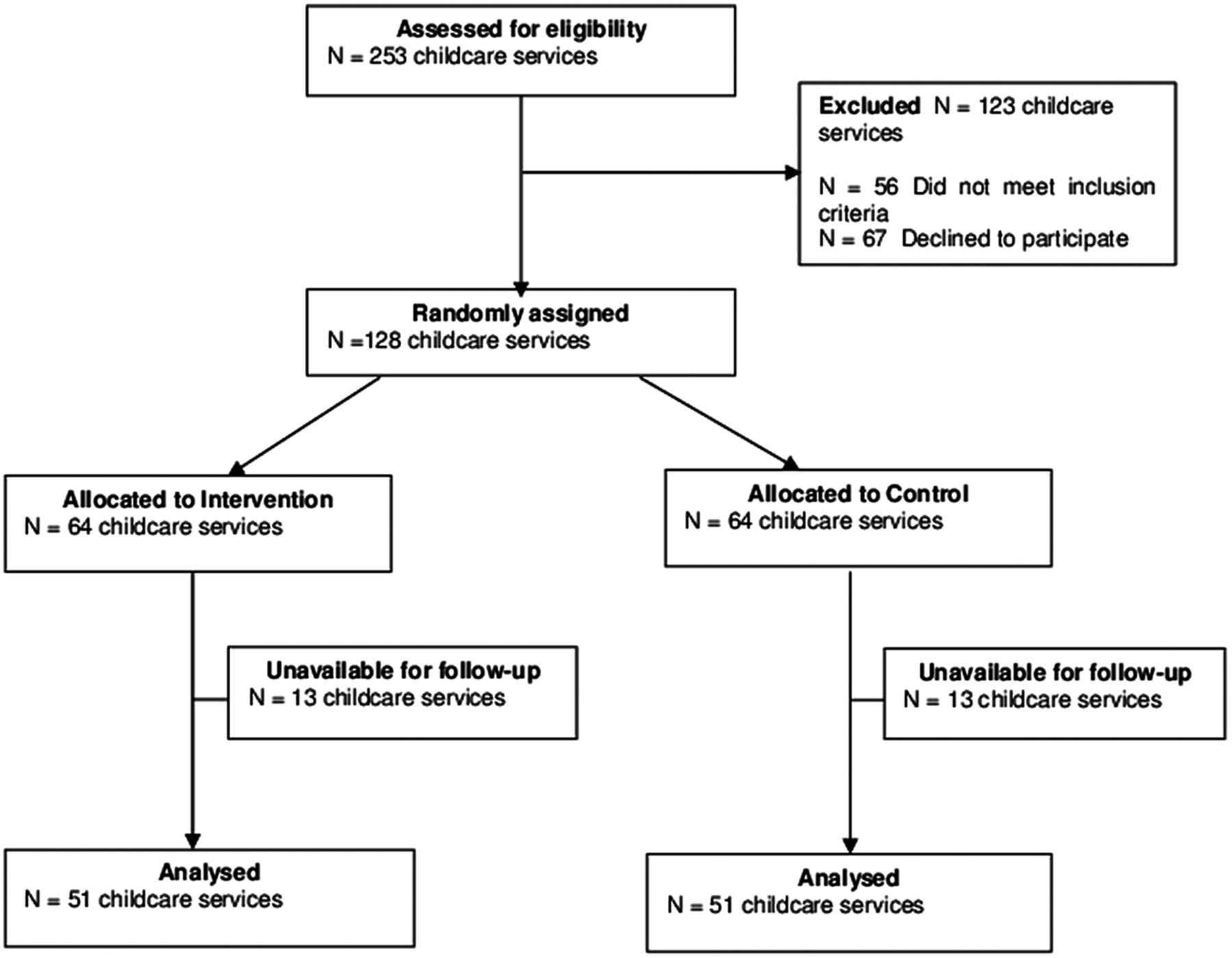
{kind=link}
CONSORT flow diagram estimating the progress of childcare services through the trial.
The research will be reported in accordance with the requirements of CONSORT Statement.29 The trial is funded by the Australian National Preventive Health Agency (reference: 95WOL2011) with in-kind support for the trial provided by Hunter New England Population Health.
Research setting
The study will take place in the Hunter region of New South Wales, Australia. The region encompasses non-metropolitan ‘major cities’ and ‘inner regional’ areas as described by the Australian Statistical Geography Standard.30 There are 586 000 people residing in the area, of which 23 000 are children aged 3–5 years.31 ,32 Approximately 3% of residents are of Aboriginal or Torres Strait Islander origin and 4% speak languages other than English.31 ,32 The Hunter region has lower indices of socioeconomic status than the New South Wales state average.31 ,32
Sample
Childcare services
For the purpose of the study, centre-based childcare services include preschools and long day care services. More than 60% of Australian children aged 3–5 years attend preschool or long day care.11 In New South Wales, preschools provide centre-based care for 6–8 h/day and enrol children aged between 3–6 years. Long day care services provide centre-based care for eight or more hours per day and usually enrol children aged from 6 weeks up to 6 years. Both types of services provide specific programmes for children aged 3–5 years that include educational and developmental activities to assist children in their preparation for school.33 Across Australian states and territories, the role and function of preschools and long day care services are similar and licensing and accreditation requirements regarding healthy eating and physical activity policies and practices are identical.21 Physical activity policies and practices are similar across both service types.22
In 2012, there were over 250 centre-based childcare services in the study region. A current list of all childcare services in the region provided by the New South Wales Ministry of Health will serve as the sampling frame for the study. Services catering exclusively for children requiring specialist care will be excluded from the trial (representing less than 1% of services in the region), as will services that provide on-site meals to children (representing approximately 30% of services in the region). Government funded, Department of Education services (representing approximately 3% of services in the region) will also be excluded as ethics approval has not been obtained from the relevant government department.
Nominated supervisors and room leaders
Within participating childcare services, nominated supervisors and room leaders will be invited to participate in CATI surveys to assess the effectiveness of the intervention. The nominated supervisor is the person responsible for the management of the service and will be asked to report on the implementation of whole-of-service policies and practices. The room leader caring for 3–5-year-old children is the head teacher of the classroom and will be asked to report on the implementation of specific healthy eating and physical activity policies and practices within their room. Where there are more than one nominated supervisors or room leaders within a service, a member of the research team will randomly select one staff member to be invited to participate by requesting the staff member with the most recent birthday. There are no exclusion criteria for nominated supervisor or room leader participation.
Recruitment procedures
In order to maximise service participation in the study, a recruitment strategy will be employed based on a review of effective recruitment practices within the school setting34 which has also been successfully executed in childcare settings by the research team.35–37 Specifically, one member of the research team will act as a dedicated recruitment coordinator. The coordinator will manage the recruitment of services into the trial and monitor consent rates. Services will be provided with the direct phone number of the coordinator for enquiries regarding the research. Study information will be mailed to childcare services inviting participation in the study. Nominated supervisors will be invited to provide consent for their service participation in the study, consent for their participation in a CATI survey and consent to contact a room leader to participate in a CATI survey. Two weeks after receipt of the information, nominated supervisors and room leaders will be telephoned by a research assistant who will confirm eligibility, invite study participation and schedule a time to conduct the baseline CATI surveys. To minimise attrition, prior to follow-up data collection, services will receive letters thanking them for their participation to date and reminding them that they will be telephoned again to participate in follow-up data collection.38
Random allocation of childcare services
Following the completion of baseline data collection, childcare services will be randomly allocated to either the intervention or control condition using a computerised random number function in Microsoft Excel. Allocation of services will be undertaken by a statistician who will have no other involvement in the trial. The random allocation of childcare services will not be stratified, given previous studies have found only slight differences in implementation of healthy eating and physical activity policies and practices by service type (preschool or long day care service), size or the socioeconomic or geographic characteristics of the service locality.22 Services will be randomised in a 1:1 (intervention:control) ratio. Owing to the difficulty in blinding services to their group allocation, this trial will be an ‘open’ trial and services will not be blind to study allocation.
Intervention
Implementation intervention
The intervention was designed by an expert advisory group of health promotion practitioners, psychologists, dietitians, behavioural scientists and physical activity experts, in consultation with nominated supervisors from local childcare services.
The intervention will seek to increase service implementation of healthy eating and physical activity policies and practices. The policies and practices are consistent with best practice Australian healthy eating and physical activity guidelines for the childcare setting,39 ,40 and evidence reviews of policies and practices shown to be associated with child healthy eating and physical activity.17 ,19 Specifically the intervention will target the implementation of the policies and practices described in the measures section.
Intervention strategies
The intervention will consist of a number of strategies to facilitate childcare service implementation of healthy eating and physical activity policies and practices. The strategies to support implementation have been developed to address identified barriers reported by childcare service staff to implementing health promoting policies and practices.41 The effectiveness of the intervention components are supported by reviews of implementation and practice change interventions,42–45 and are consistent with recommendations for scaling up health programmes.46
Specifically, the intervention will include the following strategies:
-
Implementation support staff47: Each service will be allocated an individual implementation support staff member who will provide ongoing implementation support and positive reinforcement to the service during the 12-month intervention. Support will be provided via face-to-face visits, telephone and email contacts.47 Each contact will draw on continuous quality improvement principles to review progress, provide positive reinforcement and facilitate reflection, problem solving, goal setting and action planning.47 ,48 Services will be allocated to staff members at a ratio of 20 services for every one full-time equivalent staff member.
-
Securing executive support49: To secure executive support and leadership, the importance and benefits of implementing healthy eating and physical activity policies and practices will be communicated by implementation support staff to nominated supervisors during telephone contact, face-to-face meetings, training workshops, service visits and newsletters.49 Nominated supervisors will be supported to monitor the implementation of policies and practices and will be asked to demonstrate leadership and managerial support, by leading the development and implementation of nutrition and physical activity policies, communicating expectations to childcare service staff during staff meetings, cofacilitating training workshops with implementation support staff and participating in consensus processes during staff training workshops. Such factors have been associated with implementation success.48–50
-
Employment of consensus processes45 ,51 ,52: Consensus processes will be employed to reduce childcare service staff resistance to policy and practice change by resolving any discrepancies between existing standards and expectations of childcare service staff.51 A consensus process will occur following each staff training workshop where implementation support staff will facilitate a discussion involving nominated supervisors and childcare service staff, to reach agreement and a group decision regarding an implementation strategy for the targeted policies and practices.51 The discussion will involve all childcare service staff and will allow for sharing of information, group goal setting, problem solving of barriers that may impede implementation and action planning.45 ,51 ,52
-
Provision of staff training53: A series of three 1 h training workshops will be provided to childcare service staff at their service, typically outside of operating hours. The workshops will introduce key healthy eating and physical activity intervention messages and will focus on introducing and supporting the implementation of the healthy eating and physical activity policies and practices. The workshops will combine didactic and interactive components, including opportunities to practice new skills and to role-play, have group discussions, discuss case studies and receive facilitator provided feedback, as such elements have been suggested to be more effective than didactic education alone.45 ,53–55 Training workshops will be facilitated by experienced implementation support staff with expertise in early childhood education and health promotion and will be tailored to address the specific policies or practices that childcare services are not currently implementing.
-
Provision of academic detailing visits48 ,56: On three occasions following each training workshop, implementation support staff will conduct academic detailing visits with childcare service staff at their service. The visits will draw on the principles of academic detailing outlined by Soumerai and Avon48 and will involve support staff observing childcare service staff implementation of practices targeted by the intervention. During the visits, implementation support staff will provide immediate feedback based on observations of practice regarding policy or practice implementation, provide further advice or support as required and reinforce observed practice improvements. Subsequent visits will be similarly structured by tailoring based on the policies and practices that services are having difficulty implementing.56
-
Provision of tools and resources47: All services will receive a package of tools and resources to support and sufficiently equip childcare service staff to implement the healthy eating and physical activity policies and practices. The resources were reviewed by local nominated supervisors and childcare service staff to ensure that they are relevant, attractive and user friendly in order to increase the likelihood of use.47 Specifically the resource package includes an implementation manual, policy templates, reflection and goal-setting document, self-assessment forms, a DVD with age appropriate physical activity games to encourage the development of fundamental movement skills, lanyards to be worn by childcare service staff during outdoor play with pictures and instructions for each fundamental movement skill, healthy food guideline posters and parent lunchbox resources. Resources will be provided to services in electronic and hard copy forms.
-
Provision of performance monitoring and feedback57 ,58: Performance feedback will be delivered by implementation support staff to nominated supervisors and childcare service staff members. Data for the performance feedback will be compiled initially using information collected via the baseline CATI and thereafter project records maintained by implementation support staff. Feedback will describe individual service progress towards implementation of the targeted healthy eating and physical activity policies and practices at six intervals throughout the 12-month intervention. Feedback will be provided in written, graphic and verbal modalities.57 ,58 In order to maximise the effectiveness of this strategy, performance will be compared against agreed benchmarks and the performance of all services receiving the intervention. Action plans will be negotiated with services to facilitate further performance improvement.57
-
Employment of a communications strategy59: Services will receive bimonthly printed newsletters which will communicate key messages relating to the healthy eating and physical activity policies and practices.59 The newsletters will case study individual services which have undertaken successful and innovative approaches to implementation, and include content to help overcome key implementation barriers. Services that demonstrate achievement of all healthy eating and physical activity policies and practices will also receive a certificate of recognition and will be promoted to other services through newsletters and staff training workshops.47 Nominated supervisors will also be able to nominate individual childcare service staff members who demonstrate significant achievement towards the key policies and practices for a certificate of recognition.
Theoretical perspective
The use of comprehensive theoretical frameworks, particularly those operating at multiple levels within complex systems, has been recommended to guide the development of implementation interventions.24 Given the lack of evidence for the effectiveness of theoretical frameworks for community-based implementation interventions,24 the intervention draws on implementation theory previously utilised in clinical settings.24 Specifically, the intervention draws on Damschroder's consolidated framework for implementation research.60 The framework integrates 19 theoretical models and is composed of five major domains identified as influential in successful intervention implementation: intervention characteristics, outer setting, inner setting, characteristics of the individuals involved and the process of implementation. The constructs contained within the five domains of the consolidated framework for implementation research and the application of the relevant constructs to the intervention are described in table 1.
Application of the consolidated framework for implementation research
Intervention personnel, training, supervision and monitoring
Implementation support staff will attend a 2-day training workshop which will focus on equipping staff with sufficient knowledge and skills to deliver the intervention. Intervention delivery will be overseen by a project manager. All implementation support staff will participate in fortnightly group meetings, where a self-regulatory model of peer supervision will be utilised to facilitate learning, improve staff performance and help standardise intervention delivery.61 Project records will be maintained by implementation support staff and will be used to monitor intervention delivery according to the protocol. Such staff will also have access to dietitians, psychologists and childcare service staff for specialist advice and support.
Control group
Participating services randomised to the control group will not receive any intervention by the research team during the study period.
Data collection procedures
Baseline and follow-up data will be collected through two CATI surveys—one administered to the nominated supervisor and one administered to the room leader caring for 3–5-year-old children at all participating services. Similar surveys have been used previously by the research team to assess the policies and practices of childcare services.22 ,25 ,35 The CATI survey will take approximately 15–25 min to complete. CATI interviewers will be provided with training to ensure they understand and adhere to data collection protocols. Interviewers will also be required to practice the survey script prior to administration. Interviewers will not participate in the delivery of the intervention and will be blind to service group allocation. Baseline data will be collected 1–2 months prior to start of intervention delivery. The survey administered at baseline will be repeated immediately postintervention.
Measures
Childcare service operational characteristics
Operational information will include the number of years in operation, the number of enrolled and attending children aged 3–5 years, the type of service (preschool or long day care service), number of primary contact teaching staff and hours of operation. Items to assess operational characteristics will be similar to those used in other Australian surveys of childcare services.22 ,25 ,35
Service healthy eating and physical activity policies and practices
The primary outcome is the change in prevalence of services meeting all healthy eating and physical activity policies and practices. Given there are no validated items to assess such policies and practices in Australian childcare services, survey items assessing healthy eating and physical activity policies and practices will be based on (where available) those previously used in the description of the obesity prevention environments of Australian childcare services,22 ,25 ,35 and validated items from the USA Nutrition and Physical Activity Self-Assessment for Child Care instrument 62 ,63 and the Child Care Nutrition and Physical Activity Assessment Survey.64 The validated items have adequate agreement (A) and κ scores (K). The items will assess:
-
Presence of written nutrition (K = 0.76; A=88.1%) and physical activity policies (K=0.79; A=91%);
-
Staff monitoring of children's lunchboxes against written nutritional guidelines (A=88%) and provision of feedback to parents when a non-compliant food is packed (statistic unavailable);
-
Provision of water (A=82%) or reduced fat milk only to children (K=0.73; A=82.1%);
-
Staff role modelling of physically active play (K=0.59; A=69.1%) and healthy eating (A=90%);
-
Staff provision of prompts and positive comments to children to encourage physical activity (statistic unavailable) and healthy eating (statistic unavailable);
-
Provision of adult guided fundamental movement skill development activities (statistic unavailable);
-
Restriction of sedentary screen time (A=97%).
Intervention acceptability
At follow-up, the CATI survey for intervention services will include items assessing the use, acceptability and satisfaction with the intervention resources, training and support provided to services. The items will require nominated supervisors and room leaders to respond to a series of statements on a four-point Likert scale ranging from ‘strongly agree’ to ‘strongly disagree’. Acceptability items will be developed by the research team based on previous assessments of staff acceptability in delivering health promotion programmes.25
Context
For descriptive purposes and to aid an assessment of the external validity of the trial findings, a systematic search will be conducted to describe the context in which the trial was conducted. Specifically the search will include local news archives, websites of national and New South Wales health and education departments, accreditation standards and professional healthy eating and physical activity guidelines to identify the existence of or changes in government policy, standards, funded programmes or guidelines that may influence the healthy eating and physical activity environments of childcare services. The search will include the 12 months prior to and 12 months during the intervention delivery.
Sample size and power calculations
A 20% study attrition rate is estimated based on the previous research in this setting.25 Given this, recruitment of 128 services into the trial at baseline would be sufficient to provide follow-up data from approximately 102 childcare services (51 per group) and enable the detection of an absolute difference between groups in the prevalence of services meeting all policies and practices of 27% with 80% power and an α value of 0.05 (as outlined in figure 1). The sample size calculation is based on an expected prevalence of control group services meeting all policies and practices at follow-up of 25% (unpublished data).
Statistical analysis
Descriptive statistics will be calculated to describe the demographic and service characteristics of intervention and control groups at baseline. All statistical tests will be 2-tailed with an α value of 0.05. The primary trial outcome will be analysed under an intention-to-treat framework where services are analysed based on the groups to which they were allocated, regardless of the treatment type or exposure received.65 Intervention effectiveness will be determined using a logistic regression model adjusted for baseline values. Consistent with the approach of White et al,66 the primary analysis will use all available data and include baseline policy and practice implementation as a covariate. A sensitivity analysis will be performed by imputing baseline observations at follow-up for missing data. Subgroup analyses will also be conducted by comparing service type (preschool or long day care service), socioeconomic characteristics (service postcode in the top or bottom 50% of New South Wales according to the Socioeconomic Indices for Areas) and geographic characteristics (service locality, classified as urban or rural areas according to the Australian Statistical Geography Standard).
Discussion
There is a clear need for intervention studies to extend the research regarding the implementation of healthy eating and physical activity policies and practices by childcare services. This trial aims to advance the currently limited evidence in this field and will contribute important information regarding the effectiveness of intervention strategies to facilitate the population-wide implementation of healthy eating and physical activity policies and practices in childcare services.
Strengths of this study include the trial's randomised design, the use of theoretical framework and broad set of intervention strategies, the long duration of the intervention (12 months), the implementation of procedures to reduce potential threats to internal validity, such as the blinding of data collection interviewers and computer-based randomisation of groups.
Conclusion
This manuscript provides a description of the study methods to be employed as part of a randomised controlled trial of a multicomponent intervention to facilitate the implementation of healthy eating and physical activity policies and practices in childcare services. The study is one of only a handful of randomised trials of such interventions internationally, and the first of its kind in Australia, and will contribute greatly to the evidence regarding the effectiveness of interventions in this setting.
Acknowledgments
The authors wish to thank members of the Good for Kids. Good for Life Early Childhood Education and Care advisory group.
References
Footnotes
-
Contributors JJ led the development of the manuscript. LW conceived the intervention concept. All the authors contributed to the research design and trial methodology and read and approved the final version of the manuscript.
-
Funding This study is funded by the Australian National Preventive Health Agency (reference: 95WOL2011) with in-kind support for the trial provided by Hunter New England Population Health. The project also received infrastructure support from the Hunter Medical Research Institute (HMRI).
-
Competing interests LW secured grant funding from the Australian National Preventive Health Agency.
-
Ethics approval Ethical approval to conduct the study has been obtained from the Hunter New England Human Research Ethics Committee (reference: 12/08/15/5.01) and the University of Newcastle Human Research Ethics Committee (reference: H-2012-0321).
-
Provenance and peer review Not commissioned; externally peer reviewed.