Article Text

Abstract
Objective To explore evidence on the links between patient experience and clinical safety and effectiveness outcomes.
Design Systematic review.
Setting A wide range of settings within primary and secondary care including hospitals and primary care centres.
Participants A wide range of demographic groups and age groups.
Primary and secondary outcome measures A broad range of patient safety and clinical effectiveness outcomes including mortality, physical symptoms, length of stay and adherence to treatment.
Results This study, summarising evidence from 55 studies, indicates consistent positive associations between patient experience, patient safety and clinical effectiveness for a wide range of disease areas, settings, outcome measures and study designs. It demonstrates positive associations between patient experience and self-rated and objectively measured health outcomes; adherence to recommended clinical practice and medication; preventive care (such as health-promoting behaviour, use of screening services and immunisation); and resource use (such as hospitalisation, length of stay and primary-care visits). There is some evidence of positive associations between patient experience and measures of the technical quality of care and adverse events. Overall, it was more common to find positive associations between patient experience and patient safety and clinical effectiveness than no associations.
Conclusions The data presented display that patient experience is positively associated with clinical effectiveness and patient safety, and support the case for the inclusion of patient experience as one of the central pillars of quality in healthcare. It supports the argument that the three dimensions of quality should be looked at as a group and not in isolation. Clinicians should resist sidelining patient experience as too subjective or mood-oriented, divorced from the ‘real’ clinical work of measuring safety and effectiveness.
- patient experience
- Patient safety
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
Should patient experience, as advocated by the Institute of Medicine and the NHS Outcomes Framework, be seen as one of the pillars of quality in healthcare alongside patient safety and clinical effectiveness?
-
What aspects of patient experience can be linked to clinical effectiveness and patient safety outcomes?
-
What evidence is available on the links between patient experience and clinical effectiveness and patient safety outcomes?
Key messages
-
The results show that patient experience is consistently positively associated with patient safety and clinical effectiveness across a wide range of disease areas, study designs, settings, population groups and outcome measures.
-
Patient experience is positively associated with self-rated and objectively measured health outcomes; adherence to recommended medication and treatments; preventative care such as use of screening services and immunisations; healthcare resource use such as hospitalisation and primary-care visits; technical quality-of-care delivery and adverse events.
-
This study supports the argument that patient experience, clinical effectiveness and patient safety are linked and should be looked at as a group.
Strengths and limitations of this study
-
This study demonstrates an approach to designing a systematic review for the ‘catch-all’ term patient experience, and brings together evidence from a variety of sources that may otherwise remain dispersed.
-
This was a time-limited review and there is scope to expand this search based on the results and broaden the search terms to uncover further evidence.
Introduction
Patient experience is increasingly recognised as one of the three pillars of quality in healthcare alongside clinical effectiveness and patient safety.1 In the NHS, the measurement of patient experience data to identify strengths and weaknesses of healthcare delivery, drive-quality improvement, inform commissioning and promote patient choice is now mandatory.2–4 In addition to data on harm avoidance or success rates for treatments, providers are now assessed on aspects of care such as dignity and respect, compassion and involvement in care decisions.4 In England, these data are published in Quality Accounts and the Commissioning for Quality and Innovation payment framework which makes a proportion of care providers’ income conditional on the improvement in this domain.5
The inclusion of patient experience as a pillar of quality is often justified on grounds of its intrinsic value—that the expectation of humane, empathic care is requires no further justification. It is also justified on more utilitarian grounds as a means of improving patient safety and clinical effectiveness.6 ,7 For example, clear information, empathic, two-way communication and respect for patients’ beliefs and concerns could lead to patients being more informed and involved in decision-making and create an environment where patients are more willing to disclose information. Patients could have more ‘ownership’ of clinical decisions, entering a ‘therapeutic alliance’ with clinicians. This could support improved and more timely diagnosis, clinical decisions and advice and lead to fewer unnecessary referrals or diagnostic tests.8 ,9 Increased patient agency can encourage greater participation in personal care, compliance with medication, adherence to recommended treatment and monitoring of prescriptions and dose.9 ,10 Patients can be informed about what to expect from treatment and be motivated to report adverse events or complications and keep a list of their medical histories, allergies and current medications.11
Patients’ direct experience of care process through clinical encounters or as an observer (eg, as a patient on a hospital ward) can provide valuable insights into everyday care. Examples include attention to pain control, assistance with bathing or help with feeding, the environment (cleanliness, noise and physical safety) and coordination of care between professions or organisations. Given the organisational fragmentation of much of healthcare and the numerous services with which many patients interact, the measurement of patient experience may help provide a ‘whole-system’ perspective not readily available from more discrete patient safety and clinical effectiveness measures.11
Focusing on such utilitarian arguments, this study reviews evidence on links that have been demonstrated between patient experience and clinical effectiveness and patient safety.
Methods
Identifying variables relevant to patient experience
Patient experience is a term that encapsulates a number of dimensions, and in preliminary database searches, this phrase, on its own, uncovered a limited number of useful studies. To broaden and structure the search for evidence, identify search terms and provide a framework for analysis, it was necessary to identify what patient experience entails and outline potential mechanisms through which it is proposed to impact on safety and effectiveness. As such, we combined common elements from patient experience frameworks produced by The Institute of Medicine,1 Picker Institute12 and NICE.13
Table 1 delineates different dimensions of patient experience and distinguishes between ‘relational’ and ‘functional’ aspects.10 ,14 Relational aspects refer to interpersonal aspects of care—the ability of clinicians to empathise, respect the preferences of patients, include them in decision-making and provide information to enable self-care.10 It also refers to patients’ expectations that professionals will put their interest above other considerations and be honest and transparent when something goes wrong.8 ,15 Functional aspects relate to basic expectations about how care is delivered, such as attention to physical needs, timeliness of care, clean and safe environments, effective coordination between professionals, and continuity.
Identifying aspects of patient experience and search terms
Using these frameworks and discursive documents in this area of research9 ,10 ,16 ,17 as a guide, we identified words and phrases commonly used to denote aspects of patient experience, examples of which are listed in box 1.
Search terms denoting patient experience
Patient-centred care; patient engagement; clinical interaction; patient–clinician; clinician–patient; patient–doctor; doctor–patient; physician–patient; patient–physician; patient–provider; interpersonal treatment; physician discussion; trust in physician; empathy; compassion; respect; responsiveness; patient preferences; shared decision-making; therapeutic alliance; participation in decisions; decision-making; autonomy; caring; kindness; dignity; honesty; participation; right to decide; physical comfort; involvement (of family, carers, friends); emotional support; continuity (of care); smooth transition; emotional support.
These were combined with search terms representing patient safety and clinical effectiveness outcomes, hypothesised to be associated with patient experience in discursive literature. We searched for a broad range of outcome measures, including both self-rated and ‘objective’ measurements of health status, physical health and mental health and well-being, the use of preventive health services, compliance or adherence to health-promoting behaviour and resource use.
Combining these two sets of search terms in the EMBASE database, we identified 5323 papers whose abstracts were then reviewed. If deemed relevant, the full article was retrieved to assess whether it met the inclusion criteria.
Given concerns about the sole use of protocol-driven search strategies for complex evidence,18 for the full-text articles retrieved for review, we used a ‘snowballing’ approach to identify further studies. This involved sourcing further articles in these studies for assessment and using the ‘related articles’ function in the Pubmed database. We repeated this for new articles identified until the approach ceased to identify new studies.
Inclusion criteria, assessment of quality and categorisation of evidence
We included studies that measured associations between patients’ reporting of their experience and patient safety and clinical effectiveness outcomes. These included studies measuring associations between patient experience and safety or effectiveness outcomes either at a patient level (ie, data on both types of variables for the same patients) or at an organisational level (ie, associations between aggregated measures of patient experience and safety and effectiveness outcomes for the same type of organisation such as a hospital or primary-care practice).
We included studies where the variables denoting patient experience and patient safety and clinical effectiveness were measured in a credible way, through the use of validated tools. For patient experience variables, these include surveys covering several aspects of experience (such as Picker surveys and the Hospital Consumer Assessment of Healthcare Providers and Systems survey) and specific aspects (such as a ‘Working Alliance Scale’,19 Multidimensional Health Locus of Control Scale scale20 or Usual Provider Continuity index21). For patient safety and clinical effectiveness, these include, for example, generic health and quality of life surveys (such as Short-Form 36), disease-specific surveys (such as the Seattle Angina Questionnaire22), measures of the technical quality of care (such as the Hospital Quality Alliance (HQA) score), reviews of medical records and care provider data.23 Details of the methods used to measure variables in each study are included in tables 5 and 6.
We included studies where the sample size of patients or organisations appeared sufficiently large to conduct a meaningful statistical analysis (excluding studies with fewer than 50 subjects). When extracting data relevant to our study from systematic reviews, we selected only those studies that met these criteria.
We then searched the studies’ results for positive associations (where a better patient experience is associated with safer or more effective care), negative associations (where a better patient experience is associated with less safe or less effective care) and no associations. Associations refer to cases where one measure of patient experience (typically an overall rating of patient experience for a care provider) has a statistically significant association with one or more clinical effectiveness or patient safety variable. If a study showed associations between several aspects of patient experience that appeared to be closely related (eg, ‘listening’, ‘empathy’, or ‘respect’) and an aspect of effectiveness or safety, this was counted as one association found. This was to avoid exaggerating the weight of the evidence by ‘over counting’ associations.
Two main types of studies emerged in the search—those focusing on interventions to improve aspects of patient experience and those exploring associations between patient experience variables and patient safety and clinical effectiveness variables. To manage the scope of this time-limited review, we decided to restrict analysis of the large number of interventions to the evidence contained within systematic reviews.
Results
Overall, the evidence indicates positive associations between patient experience and patient safety and clinical effectiveness that appear consistent across a range of disease areas, study designs, settings, population groups and outcome measures. Positive associations found outweigh ‘no associations’ by 429–127. Of the four studies where ‘no associations’ outweigh positive associations, there is no suggestion that these are methodologically superior. Negative associations were rare. Of the 40 individual studies assessed in table 5 negative associations (between patient experience of clinical team interactions and continuity of care and separate assessment of the quality of clinical care) were found in only one study.24
Table 2 shows surveys to be the predominant method used to measure variables for individual studies (figure 1).
Methods used to measure variables

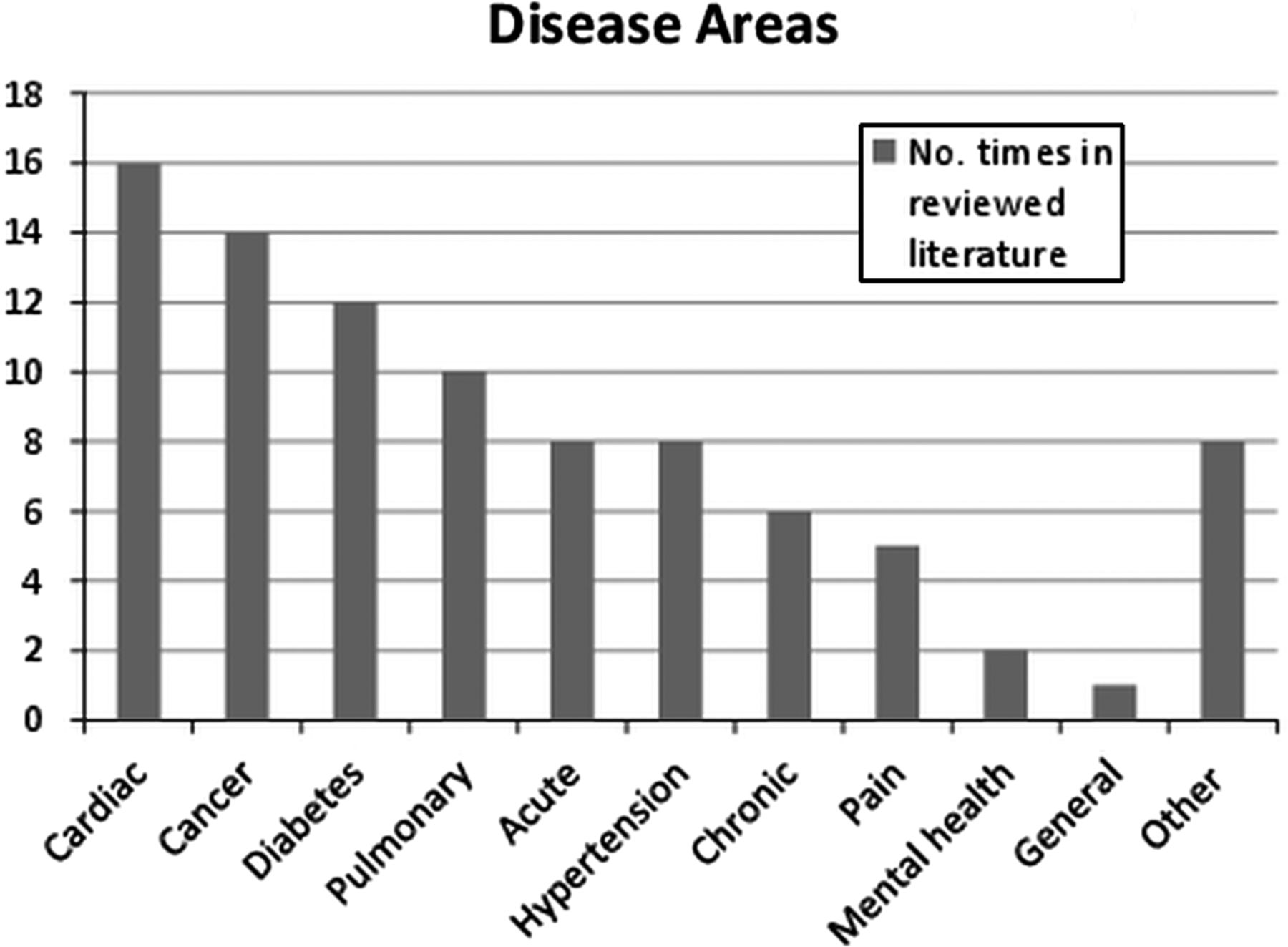{kind=link}
Outlines the disease areas covered.
Table 3 presents the frequency of positive associations and ‘no associations’ categorised by type of outcomes (for 378 of the 556 cases where sufficient information was available to categorise). These include objectively measured health outcomes (eg, ‘mortality’, ‘blood glucose levels’, ‘infections’, ‘medical errors’); self-reported health and well-being outcomes (eg, ‘health status’, ‘functional ability’ ‘quality of life’, ‘anxiety’); adherence to recommended treatment and use of preventive care services likely to improve health outcomes (eg, ‘medication compliance’, ‘adherence to treatment’ and screening for a variety of conditions); outcomes related to healthcare resource use (eg, ‘hospitalisations’, ‘hospital readmission’, ‘emergency department use’, ‘primary care visits’); errors or adverse events and measures of the technical quality of care.
Associations categorised by type of outcome
Table 4 shows associations categorised by type of care provider (for the subset of studies focusing on one setting) and for studies focused on chronic conditions.
Weight of evidence by provider and for chronic conditions
Tables 5 and 6 present details of all studies identified, specifying the analytical focus of each study, methods to measure variables and positive associations and ‘no asscoiations’ found.
Individual studies
Systematic reviews
Discussion
Overall, the evidence indicates associations between patient experience, clinical effectiveness and patient safety that appear consistent across a range of disease areas, study designs and settings.
As table 3 indicates, the evidence shows positive associations found outweigh those not found for both self-assessment of physical health and mental health (61 vs 36) and ‘objective’ measures of health outcomes (eg, where measures are taken by a clinician or by reviewing medical records) (29 vs 11). For objective measures, one study25 shows positive associations for ulcer disease, hypertension and breast cancer. Two studies on myocardial infarction show positive associations with survival 1 year after discharge26 and inpatient mortality.27 Objective measurement is less frequently explored than self-rated health and is an area that could benefit from further research.
Evidence is strong in the case of adherence to recommended medical treatment. A meta-analysis included in this study showed positive associations between the quality of clinician–patient communications and adherence to medical treatment in 125 of 127 studies analysed and showed the odds of patient adherence was 1.62 times higher where physicians had communication training.28 Regarding compliance with medication, positive associations found to outweigh those not found.20 ,29–35 A review of interventions to increase adherence to medication (not included in this study) showed communication of information, good provider–patient relationships and patients’ agreement with the need for treatment as common determinants of effectiveness.36 There is evidence of better use of preventive services, such as screening services in diabetes, colorectal, breast and cervical cancer; cholesterol testing and immunisation.24 ,25 ,37–39 There is also evidence of impacts on resource use of primary and secondary care (such as hospitalisations, readmissions and primary care visits).21 ,29 ,40–45
For studies exploring associations between patient experience and technical quality of care measured by other means, the evidence is mixed. Two studies in acute care showed positive associations between overall ratings of patient experience and ratings of the technical quality of care (using HQA measures) for myocardial infarction, congestive heart failure, pneumonia and complications from surgery.23 ,46 Another found an association with adherence to clinical guidelines for acute myocardial infarction.27 A similar study in primary care found positive associations between patient experience of processes and measurement of care quality (from the Healthcare Effectiveness Data and Information Set (HEDIS) system measuring care quality for disease prevention and management in chronic conditions).24 However, two other studies found no associations between patients’ ratings and ratings based on an assessment of medical records.47 ,48
Some studies show positive associations between patients’ perspective or observations of processes of care and the safety of care recorded through other means. Isaac46 found positive associations between ratings of patient experience and six patient-safety indicators (decubitus ulcer; failure to rescue; infections due to medical care; postoperative haemorrhage, respiratory failure, pulmonary embolism and sepsis). Two studies examining evidence for patients’ ability to identify medical errors or adverse events in hospital showed positive associations between patients’ accounts of their experience of adverse events and the documentation of events in medical records.49 ,50 But another study shows only 2% of patient-reported errors were classified by medical reviewers as ‘real clinical medical errors’ with most ‘reclassified’ by clinicians as ‘misunderstandings’ or ‘behaviour or communication problems’.51 Overall, there is less evidence available on safety compared to effectiveness and this should be a priority for future research in this area.
Research from other studies not included in this review support these findings. For example, research on ‘decision aids’ to ensure that patients are well informed about their treatments, and that decisions reflect the preferences of patients indicates that patient engagement has a beneficial impact on outcomes. For example, awareness of the risks of surgical procedures resulted in a 23% reduction in surgical interventions and better functional status.52 Another review showed that provision of good information and emotional support are associated with better recovery from surgery and heart attacks.53
Study strengths and limitations
This review builds on other studies9 ,10 ,16 ,17 exploring links between these three domains. This study also demonstrates an approach to designing a systematic search for evidence for the ‘catch-all’ term patient experience, bringing together evidence from a variety of sources that may otherwise remain dispersed. This approach can be used or adapted for further research in this area.
This was a time-limited review and there is scope to expand this search, based on our results. There may be scope to broaden the search terms and this may uncover further evidence. The first search was confined to one database and the review focused primarily on peer-reviewed literature excluding grey literature. To manage the scope of this review, we restricted the analysis of interventions to improve patient experience to evidence within systematic reviews. While we used some quality criteria to filter studies (including the use of validated tools to measure experience, safety and effectiveness outcomes and sample size), with more time a more detailed formal quality assessment may have added value to the study. Although all positive associations included in the study are statistically significant, the strength of associations vary. Because of time constraints and the heterogeneity of measures used, we did not systematically compare the strengths of positive associations in different studies, but this may be an area for future work. There may also be scope to explore whether future research in this area could go beyond the counting of associations in this study through, for example, meta-analysis. As always, there may be a publication bias in favour of studies showing positive associations between patient experience variables and safety and effectiveness outcomes.54 In addition, 28 of the 40 individual studies assessed were conducted in the USA and caution is needed about their applicability to other healthcare systems.
Conclusion
The inclusion of patient experience as one of the pillars of quality is partly justified on the grounds that patient experience data, robustly collected and analysed, may help highlight strengths and weaknesses in effectiveness and safety and that focusing on improving patient experience will increase the likelihood of improvements in the other two domains.3
The evidence collated in this study demonstrates positive associations between patient experience and the other two domains of quality. Because associations do not entail causality, this does not necessarily prove that improvements in patient experience will cause improvements in the other two domains. However, the weight of evidence across different areas of healthcare indicates that patient experience is clinically important. There is also some evidence to suggest that patients can be used as partners in identifying poor and unsafe practice and help enhance effectiveness and safety. This supports the argument that the three dimensions of quality should be looked at as a group and not in isolation. Clinicians should resist sidelining patient experience measures as too subjective or mood-orientated, divorced from the ‘real’ clinical work of measuring and delivering patient safety and clinical effectiveness.
Acknowledgments
The authors of this work thank Mandy Wearne at NHS Northwest who commissioned this work and provided comments on earlier drafts, We are also grateful to Jocelyn Cornwell who provided comments on an early draft of this article. This article presents independent research commissioned by the National Institute for Health Research (NIHR) under the Collaborations for Leadership in Applied Health Research and Care (CLAHRC) programme for North West London. The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
References
Footnotes
-
Contributors CD and DB conceived of the study and were responsible for the design and search strategy. CD and LL were responsible for conducting the search. CD and LL conducted the data analysis and produced the tables and graphs. Derek Bell provided input into the data analysis and interpretation. The initial draft of the manuscript was prepared by CD then circulated among all authors for critical revision. All authors helped to evolve analysis plans, interpret data and critically revise successive drafts of the manuscript.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement There are no additional data available.