

Abstract
Objective. Our aim was to assess prior use of core recommended non-surgical treatment among patients with knee osteoarthritis (OA) scheduled for total knee arthroplasty (TKA), and to assess potential patient-level correlates of underuse, if found.
Methods. This was a cross-sectional study of patients undergoing TKA for primary knee OA at 2 provincial central intake hip and knee clinics in Alberta, Canada. Standardized questionnaires assessed sociodemographic characteristics, social support, coexisting medical conditions, OA symptoms and coping, and previous non-surgical management. Multivariable logistic regression was used to assess the patient-level variables independently associated with receipt of recommended non-surgical knee OA treatment, defined as prior use of pharmacotherapy for pain, rehabilitation strategies (exercise or physiotherapy), and weight loss if overweight or obese (body mass index ≥ 25 kg/m2).
Results. There were 1273 patients included: mean age 66.9 years (SD 8.7), 39.9% male, and 44.1% had less than post-secondary education. Recommended non-surgical knee OA treatment had been used by 59.7% of patients. In multivariable modeling, the odds of having received recommended non-surgical knee OA treatment were significantly and independently lower among individuals who were older (OR 0.97, 95% CI 0.95–0.99), male (OR 0.33, 0.25–0.45), and who lacked post-secondary education (OR 0.70, 0.53–0.93).
Conclusion. In a large cross-sectional analysis of knee OA patients scheduled for TKA, 40% of individuals reported having not received core recommended non-surgical treatments. Older individuals, men, and those with less education had lower odds of having used recommended non-surgical OA treatments.
Total knee arthroplasty (TKA) for the treatment of advanced knee osteoarthritis (OA) is one of the most common and fastest-growing surgical procedures in developed countries1,2,3. In 2016–2017, over 67,000 TKA were performed in Canada4, with a rate that is projected to continue to increase5. While on average TKA is highly effective, 15–30% of recipients report little or no symptom improvement and/or dissatisfaction with the results6,7. Thus, there is consensus that effective non-surgical options should be maximized before referral to surgery is considered8,9,10,11,12,13.
Despite national and international evidence-based guidelines14,15,16,17,18 for the non-surgical treatment of knee OA, underuse of effective therapies has been documented across multiple treatment settings19,20,21,22. Barriers to receipt of knee OA treatment include lack of awareness of treatment availability or effectiveness, financial constraints and other difficulties accessing care, and presence of coexisting medical conditions that are prioritized or might contraindicate some therapies23,24,25.
Two small studies have examined the prior use of non-pharmacological and pharmacological therapies in patients with knee OA receiving TKA. A UK study of 105 patients undergoing hip or knee arthroplasty found that 72% had used systemic analgesics, but only 49% had tried physiotherapy (PT)26. A Dutch study of 195 patients found similar use of systemic analgesics, higher use of PT (73%), and that 30% of obese patients had tried a weight management strategy27. These findings suggest a gap in care that, if addressed, has the potential to reduce or delay need for TKA for patients with knee OA. For example, Skou, et al showed that two-thirds of patients scheduled for TKA who received a 12-week comprehensive non-surgical treatment program elected to delay their surgery for at least 2 years28.
The objectives of our study were to determine (1) the proportion of patients undergoing TKA for primary knee OA who had received core recommended non-surgical treatments, defined as prior use of a recommended pharmacotherapy for pain, exercise or PT, and weight loss if over-weight or obese; and (2) potential patient-level correlates of underuse, if found. Guided by the Andersen healthcare use model29 (Figure 1), we hypothesized that prior use of non-surgical knee OA treatments would be related to predisposing factors (e.g., education and income resulting in lower health literacy and inability to pay out-of-pocket costs for some treatments), enabling factors (e.g., social support, given the importance of peer support on uptake of and adherence to physical activity; and coexisting medical conditions, which may act as competing clinical demands and contra-indications to some OA medications), and perceived need factors of patients (e.g., pain and disability, which may increase perceived need for treatment).
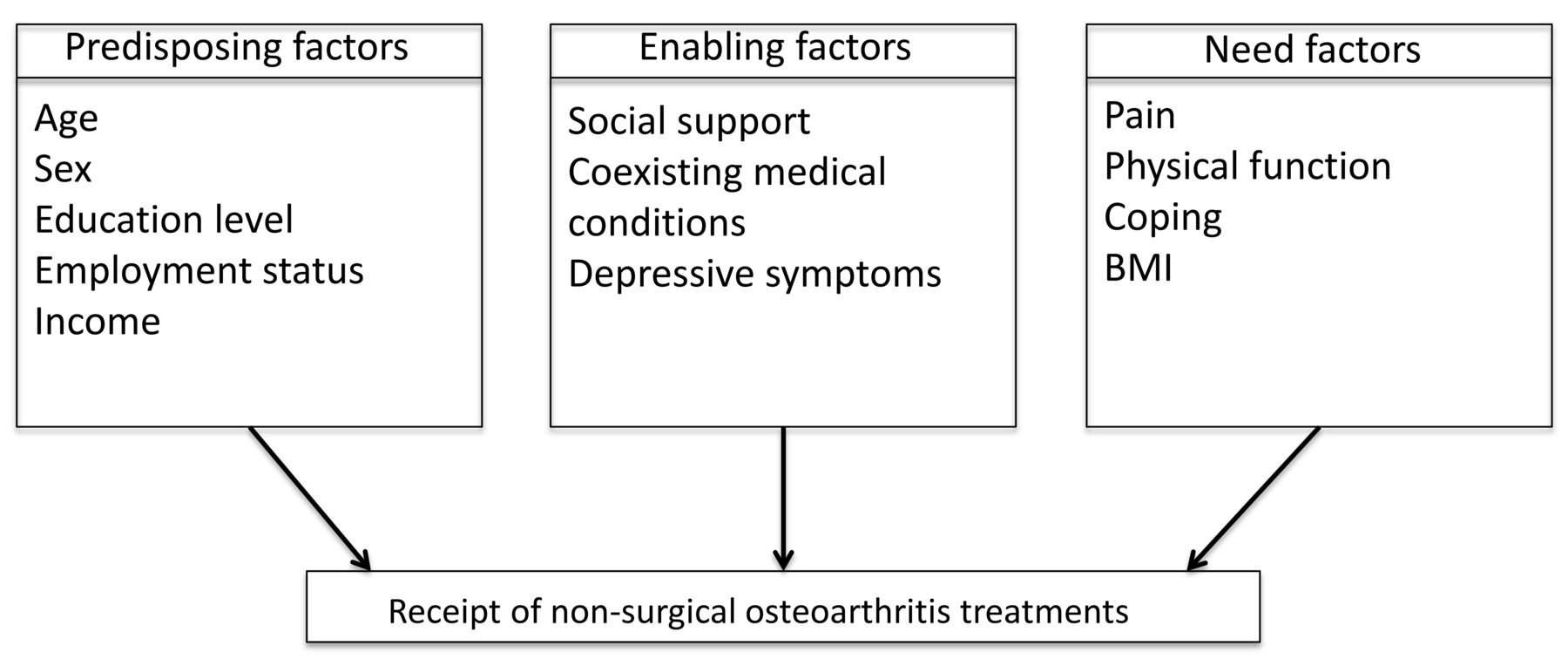
Conceptual framework for receipt of recommended non-surgical osteoarthritis treatments. BMI: body mass index.
MATERIALS AND METHODS
Setting and design
This was a cross-sectional study nested within a prospective cohort study. Participants were recruited consecutively between October 27, 2014, and September 30, 2016, at 2 provincial central intake orthopedic hip and knee clinics in Calgary and Edmonton, Alberta, Canada. These sites annually perform about 60% of the TKA in the province. All surgeons (n = 45) who perform TKA surgery at these centers were invited, they agreed, and provided written consent to participate in the study.
Participants
Inclusion criteria were the following: a diagnosis of primary knee OA, age 30 years or older, ability to read and comprehend English, and consultation with an orthopedic surgeon regarding elective primary unilateral TKA. Eligible patients who were recommended for and consented to undergo TKA were included. We excluded participants who had missing data for the primary outcome.
Assessments
After providing written consent, participants self-completed a standardized computer-based questionnaire prior to consultation with the orthopedic surgeon. The questionnaire assessed the following variables:
Predisposing factors: Participants were asked to report their annual household income (< $60,000 vs ≥ $60,000, all Canadian dollars), level of education (< post-secondary vs post-secondary), and employment status (working for pay vs other).
Enabling factors: Social support was measured with the 6-item Lubben Social Network Scale30, scored 0–30 (higher scores indicate more support). Participants were also asked to self-report (yes/no) the presence of the following chronic conditions, which may contraindicate use of some recommended OA therapies: heart disease, hypertension (HTN), lung disease, diabetes, ulcer or stomach disease, kidney disease, and liver disease. The 8-item Patient Health Questionnaire Depression Scale (PHQ-8)31, scored 0–24 (higher indicating more depressive symptoms), was used to assess depressive symptoms, which may affect treatment uptake and adherence.
Need factors: Self-reported knee OA symptoms were assessed using the 5-item Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain subscale32,33, scored 0–20 (higher scores indicate worse pain), and the 7-item Knee Injury and Osteoarthritis Outcome Score Physical Function Short Form (KOOS-PS)34, scored 0–100 (higher scores indicate worse disability34). Perceived ability to cope with different aspects of having knee OA was assessed using the 4-item arthritis coping efficacy scale35,36, scored 4–20 (higher indicating greater coping efficacy).
To assess prior use of non-surgical knee OA treatments, patients were asked to indicate which of the following therapies for knee OA they had “ever tried” (yes/no): exercise (“exercise on your own or formal exercise program”), weight loss through any means (“weight loss”), PT (“assessment by a physiotherapist”); joint injections [“joint injections to your knee (i.e., cortisone, hyaluronic acid)”], acetaminophen [(“acetaminophen (Tylenol [regular or extra strength] or Tylenol Arthritis)”], oral or topical nonsteroidal antiinflammatory drugs [NSAID; “anti-inflammatory drugs (by mouth or topically) i.e., Advil, naproxen, Voltaren, Arthrotec, ibuprofen, Celebrex”], and opioid analgesics [“Painkillers with codeine (e.g., Tylenol #1,2,3; Percocet, oxycodone, MS Contin)”]. Participants’ age, sex, and height and weight, to calculate body mass index (BMI), were obtained from clinic records.
Outcomes
The primary outcome was a composite measure of prior use of recommended non-surgical OA treatment (yes/no), defined as having indicated “yes” to having tried exercise or PT and weight loss if over-weight or obese (BMI ≥ 25 kg/m2) and at least 1 of acetaminophen, oral or topical NSAID, or joint injection. This reflects the core recommended non-surgical knee OA treatments across multiple national and international guidelines14,15,16,17,18, and is in keeping with published quality standards for the expected knee OA treatments that should be used before referral for consideration of joint surgery13.
Secondary outcomes were prior use of recommended non-pharmacological treatments [exercise or PT and weight loss if overweight or obese (yes/no)], which was of interest because non-pharmacological OA treatments have been reported to be the most underused; and prior use of NSAID (yes/no), which we hypothesized might be underused in individuals with specific medical comorbidities.
Statistical analyses
Distributions of all continuous variables were assessed for normality. Participant characteristics were summarized using frequencies, means and SD or medians and interquartile ranges (IQR), as appropriate, overall and for those who had and had not received non-surgical OA treatment. Characteristics were compared using the chi-square test, t test, or Wilcoxon rank-sum test, as appropriate.
For each outcome of interest, logistic regression was used to examine the relationship of the outcome with age, sex, level of education (post-secondary vs less), social support (Lubben score), knee symptom severity (WOMAC pain, KOOS function), and comorbid conditions. In the primary models, we examined the effects of specific comorbidities that may contra-indicate use of NSAID [heart disease, HTN, diabetes, kidney disease, and gastrointestinal (GI) disease] in addition to depressive symptoms (PHQ-8) and BMI. In a secondary analysis, these specific conditions were replaced with the number of comorbid conditions to assess the effect of overall burden of comorbidity. Because self-report of trying to lose weight may reflect variable practices, we conducted a sensitivity analysis, removing the requirement of weight loss from our primary outcome. We used a forced entry multivariable model. We assessed for multicollinearity of covariates using Spearman and tetrachoric correlation coefficients and confirmed none were correlated at a ρ ≥ 0.6. With the exception of annual household income, where 11% of the data were missing, the level of missingness for all other variables of interest was very low (< 2%); thus, imputation for missing data was not performed.
All statistical analyses were performed using SAS Studio version 3.71 (SAS Institute Inc.). We presented all estimates of association with 95% CI. Statistical significance was considered met at a 2-sided p value of 0.05 in logistic regression analyses. For descriptive analyses, given multiple comparisons, we used a cutoff of 0.01.
Ethics approval
The study was approved by the Research Ethics Boards of the Universities of Alberta (PRO-00051108) and Calgary (REB 14-1294), and from Women’s College Hospital (REB 2014-0092) at the University of Toronto.
RESULTS
Participants characteristics
Of 2277 eligible patients with knee OA assessed for TKA, 1373 were recommended for and consented to undergo the procedure. Of these, 1273 individuals (92.7%) with complete data for our primary outcome were included in our analyses. Their mean age was 66.9 years (SD 8.7), 39.9% were male, 44.1% did not have a post-secondary education, and 54.3% had an annual household income < $60,000 (Table 1). Mean BMI was 33 kg/m2 (SD 6.3); 92.2% were overweight or obese. Seventy-seven percent had at least one of the conditions of interest (heart disease 15%, HTN 53%, diabetes 17%, kidney disease 3%, and GI disease 12%). Median PHQ-8 score was 5.0/24 (IQR 2–10) and mean score for arthritis coping efficacy was 13.2/20 (SD 3.9). Mean WOMAC pain score was 11.6 (SD 3.5) and mean KOOS-PS score was 53.6 (SD 17.3). Prior use of recommended non-surgical treatments, as we defined it, was associated with younger age, female sex, receipt of post-secondary education, and less depression (p < 0.01; Table 1).
Participant characteristics (n = 1273).
Prior use of non-surgical OA treatments
Among participants scheduled for TKA, most reported having used pharmacologic treatments; 75.2% had used acetaminophen, 76.0% had used NSAID, and 75.1% had received at least 1 knee injection. Fewer reported having used recommended non-pharmacological treatments: 75.4% had used exercise, 44.3% had received PT, and 69.2% of those who were over-weight or obese had tried weight loss (Table 1).
Primary outcome: recommended non-surgical treatment for knee OA (non-pharmacological and pharmacological treatment)
Over half the participants (59.7%) met our criteria for having received core recommended non-surgical knee OA treatment. In univariate analyses, the odds of reporting having ever used recommended non-surgical treatment, as defined, were significantly lower among individuals who were older, male, and had less education and significantly higher among individuals with symptoms of depression, and greater knee pain and disability (p < 0.05 for all; Table 2). In multivariable analysis, the odds of prior use of recommended non-surgical knee OA treatment remained significantly and independently lower among individuals who were older (OR per year 0.97, 95% CI 0.95–0.99; OR per 10 years 0.74, 95% CI 0.62–0.89), male (OR 0.33, 95% CI 0.25–0.45), and with less education (OR for less than post-secondary education 0.70, 95% CI 0.53–0.93). The odds were significantly higher in those with depressive symptoms (OR per unit increase PHQ-8 1.06, 95% CI 1.03–1.09). Prior use of recommended non-surgical knee OA treatment was also significantly higher in individuals with greater social support (OR per unit increase on Lubben 1.03, 95% CI 1.00–1.06) and in those with GI (OR 1.64, 95% CI 1.04–2.58) and cardiovascular disease (OR 1.64, 95% CI 1.09–2.48; Table 2). The final model had good fit (Hosmer-Lemeshow goodness-of-fit p = 0.82; C-statistic = 0.70). A sensitivity analysis, removing the weight loss from our primary outcome, gave similar results (data not shown).
The relationship of patient-level factors to prior use of recommended treatments (composite variable): results of logistic regression modeling.
In secondary analyses, when specific comorbid conditions were replaced in the model by the number of coexisting conditions, we found no significant relationship between number of conditions and our outcome of interest (1 comorbidity vs none: OR 1.03, 95% CI 0.72–1.45; 2 comorbidities vs none: OR 1.27, 95% CI 0.86–1.85; 3 comorbidities vs none: OR 1.35, 95% CI 0.91–1.99).
Secondary outcomes: non-pharmacological treatment (exercise and/or PT and weight loss if overweight/obese)
Among participants, 61.6% met our criteria for having used recommended non-pharmacological OA therapies, as defined. In multivariable analysis, the odds of reporting prior use of recommended non-pharmacological OA treatment were significantly and independently lower in individuals who were older (OR per year 0.98, 95% CI 0.96–1.00), male (OR 0.38, 95% CI 0.28–0.50), had less education (OR for high school education or less 0.66, 95% CI 0.50–0.88) and lower income (OR for income < $60,000 0.71, 95% CI 0.52–0.96). Odds were higher in those with depressive symptoms (OR per unit increase PHQ-8 1.06, 95% CI 1.02–1.09), greater social support (OR per unit increase on Lubben 1.03, 95% CI 1.01–1.06), GI disease (OR 1.79, 95% CI 1.13–2.85), and cardiovascular disease (OR 1.70, 95% 1.12–2.57; Table 3).
The relationship of patient-level factors to prior use of non-pharmacological treatments: results of logistic regression modeling.
NSAID
In multivariable analysis, the odds of reporting having ever used NSAID were significantly and independently lower among individuals who were older (OR per year increase 0.97, 95% CI 0.94–0.99) and male (OR 0.68, 95% CI 0.48–0.94). NSAID use was also lower among individuals with cardiovascular disease, kidney disease, and diabetes, but these effects did not reach statistical significance (Table 4).
Relationship of patient-level factors to prior use of NSAID: results of logistic regression modeling.
DISCUSSION
In a large cohort of patients with knee OA scheduled to undergo TKA, only 60% had previously received core recommended non-pharmacological and pharmacologic therapies for knee OA. Non-pharmacologic treatments, including exercise, PT, and weight management, were disproportionally underused; while 97% had received pharmacological therapies for pain, only 62% had received non-pharmacological therapies. Given that orthopedic surgeons have indicated that having “an adequate trial of non-surgical arthritis treatment” is an important criterion in assessing patient appropriateness for TKA10, these findings indicate a worrisome care gap. More appropriate use of evidence-based non-surgical care has the potential to improve the pain, physical function, and quality of life for patients with knee OA and may reduce or delay the need for TKA28.
From the literature, major barriers to effective knee OA care include societal beliefs of patients and physicians about OA as a normal part of aging for which nothing can be done and the high prevalence of comorbid conditions, such as diabetes and heart disease, that present competing demands and/or contraindicate the use of some OA therapies (e.g., NSAID37,38). Consistent with this, participants with heart disease and GI disease had higher odds of receipt of recommended OA treatment, and particularly non-pharmacological therapies, but lower odds of having received NSAID. These findings suggest that non-pharmacological treatments are sought preferentially when the risks of pharmacological therapy are increased. We also found higher odds of use of non-pharmacological care in individuals with more depressive symptoms. A potential explanation for this finding is that these individuals are experiencing greater OA pain and seeking relief from their healthcare providers.
Individuals with low income may be less likely to have used treatments that incur out-of-pocket costs. In Alberta, Canada, outpatient NSAID and knee injection medications are not publicly funded, and funding for PT is limited. Consistent with the findings of others39, individuals with lower income were less likely to have received PT or exercise. Given the effectiveness of therapeutic exercise in the management of knee OA40, enhanced public funding for rehabilitation programs may be warranted. Lower education was also associated with lower odds of prior use of recommended treatments. Lower health literacy has been shown to reduce the uptake of treatments or health services41,42. Both patient income and education need to be considered in future implementation strategies.
Although the effect was modest, participants with more social support had higher odds of having used non-pharmacological therapies for their knee OA. This is because these therapies require active patient engagement. Social support has been shown to be important in patient adherence to medical treatment43 and should be harnessed in efforts to improve quality of OA care. Further research is warranted to examine the role of social support in improving knee OA care.
Male sex was strongly associated with lower odds of use of all OA treatments. Reasons for this are unclear, although they are consistent with prior research on sex differences in healthcare use44,45. Compared with men, women with knee OA seek and receive TKA later in the course of their disease46. Thus, a potential explanation is simply that women accrue a longer duration of time to have used treatments than their male counterparts.
Strengths of the study include the large sample size (patients and surgeons) and the breadth of patient characteristics assessed, which enhances generalizability, albeit within one healthcare system. A total of 45 surgeons practice in the 2 orthopedic centers from which we recruited participants; these surgeons collectively perform 60% of the TKA in the province (> 6000/yr). Thus, our results are likely to reflect a breadth of orthopedic practices. However, there are also some important limitations. First, prior treatment was self-reported, thus subject to recall bias, and we did not assess the doses, frequency, and duration of use of the various treatments to distinguish who has received adequate trials of treatment from those who did not. Previous studies have shown that individuals tend to overreport participation in exercise47,48 and that fewer than 10% of individuals who self-report using weight loss strategies have consulted their family physician or a weight loss specialist49. When it comes to pharmacotherapy, in a study by Snijders and colleagues, while 75% of patients reported having previously tried acetaminophen, only 36% had used an adequate trial that they defined as 1000 mg 2–4 times per day for at least 14 consecutive days50. Therefore, our results are likely an overestimate of the proportion of individuals who have received adequate trials of these therapies. Third, reported treatments may not reflect what healthcare providers actually prescribed and we acknowledge some heterogeneity across OA treatment guidelines (e.g., use of acetaminophen). Fourth, the cross-sectional features of this study does not allow us to draw conclusions about causal associations between participant characteristics and use of treatments. Finally, whether improved use of non-surgical therapies for knee OA will lead to reduced need for TKA remains to be shown.
We found substantial underuse of recommended non-surgical treatments in patients with knee OA recommended for TKA. Underuse was particularly high for non-pharmacological therapies, which have the greatest potential to improve symptoms18 and are safe for use in patients with multimorbidity. Implementation strategies are required to optimize non-surgical treatment of patients with knee OA before progressing to surgical treatment, particularly in older men and those with less education. Ultimately, improved use of non-surgical treatments has the potential to delay or reduce need for TKA, increase healthcare system efficiency, reduce healthcare costs, and improve patient outcomes.
APPENDIX 1.
Members of the BEST-Knee Research Team: Dr. Gillian A. Hawker (University of Toronto, Toronto, Ontario), Dr. Deborah A. Marshall (University of Calgary, Calgary, Alberta), Dr. Eric Bohm (University of Manitoba, Winnipeg, Manitoba), Dr. Michael J. Dunbar (Dalhousie University, Halifax, Nova Scotia), Dr. Peter Faris (University of Calgary, Calgary, Alberta), Dr. C. Allyson Jones (University of Alberta, Edmonton, Alberta), Dr. Tom Noseworthy (University of Calgary, Calgary, Alberta), Dr. Bheeshma Ravi (University of Toronto, Toronto, Ontario), Dr. Linda Woodhouse (University of Alberta, Edmonton, Alberta).
Edmonton Bone and Joint Centre, Edmonton, Alberta, Canada: participating study surgeons [Dr. Gordon Arnett, Dr. Robert Balyk, Dr. Jeffery Bury, Dr. John Cinats, Dr. Donald Dick, Dr. D’Arcy Durand, Dr. Lee Ekert, Dr. Don Glasgow, Dr. Robert Glasgow Sr. (deceased), Dr. Gordon Goplen, Dr. Ben Herman, Dr. Catherine Hui, Dr. Larry Hunka, Dr. Hongxing Jiang, Dr. William C. Johnson (deceased), Dr. Frank Kortbeek, Dr. Guy Lavoie, Dr. Mitch Lavoie, Dr. Paul K. Leung, Dr. James Mahood, Dr. Edward Masson, Dr. Richard McLeod, Dr. James McMillan (deceased), Dr. Greg O’Connor, Dr. David Otto, Dr. Carlo Panaro, Dr. Paulose Paul, Dr. Gordon Russell, Dr. Don Weber, Dr. Colleen Weeks, Dr. Andrea Woo (FP, screening)], clinic staff (Jane Squire Howden), and research staff (Anne-Marie Adachi, Jessica Beatty, Shakib Rahman, Braden Woodhouse).
Alberta Hip & Knee Clinic, Calgary, Alberta, Canada: participating study surgeons (Dr. Greg Abelseth, Dr. Kelley De Souza, Dr. John Donaghy, Dr. Paul Duffy, Dr. Kelly Johnston, Dr. Robert Korley, Dr. Raul Kuchinad, Dr. Michael Monument, Dr. Maureen O’Brien, Dr. James Powell, Dr. Shannon Puloski, Dr. Ed Rendall, Dr. Alex Rezansoff, Dr. Raj Sharma, Dr. James Stewart, Dr. Scott Timmerman, Dr. Jason Werle), clinic staff (Tanya Reczek), and research staff (Jeffrey Depew); Bukky Dada (Department of Community Health Sciences, University of Calgary); Barbara Conner-Spady (Department of Community Health Sciences, University of Calgary); and Ian Stanaitis (Women’s College Hospital/University of Toronto).
Footnotes
This study was funded by an operating grant from the Canadian Institutes of Health Research (grant no. MOP-312807).
G.A. Hawker has received research support as the Sir John and Lady Eaton Professor and Chair of Medicine, Department of Medicine, University of Toronto. D.A. Marshall is supported through a Canada Research Chair in Health Systems and Services Research and the Arthur J.E. Child Chair in Rheumatology.
- Accepted for publication November 5, 2019.








{kind=link}