

Abstract
Objective. To determine the feasibility of a 12-week Internet-based self-management program of disease-specific information, self-management strategies, and social support with telephone support for youth with juvenile idiopathic arthritis (JIA) and their parents, aimed at reducing physical and emotional symptoms and improving health-related quality of life (HRQOL).
Methods. A nonblind pilot randomized controlled trial (NCT01011179) was conducted to test the feasibility of the “Teens Taking Charge: Managing Arthritis Online” Internet intervention across 4 tertiary-level centers in Canada. Participants were 46 adolescents with JIA, ages 12 to 18 years, and 1 parent for each participant, who were randomized to the control arm (n = 24) or the Internet intervention (n = 22).
Results. The 2 groups were comparable on demographic and disease-related variables and treatment expectation at baseline. Attrition rates were 18.1% and 20.8%, respectively, from experimental and control groups. Ninety-one percent of participants randomized to the experimental group completed all 12 online modules and weekly phone calls with a coach in an average of 14.7 weeks (SD 2.1). The control group completed 90% of weekly attention-control phone calls. The Internet treatment was rated as acceptable by all youth and their parents. In posttreatment the experimental group had significantly higher knowledge (p < 0.001, effect size 1.32) and lower average weekly pain intensity (p = 0.03, effect size 0.78). There were no significant group differences in HRQOL, self-efficacy, adherence, and stress posttreatment.
Conclusion. Findings support the feasibility (acceptability, compliance, and user satisfaction) and initial efficacy of Internet delivery of a self-management program for improving disease-specific knowledge and reducing pain in youth with JIA.
Juvenile idiopathic arthritis (JIA) is a common chronic childhood illness1 that can lower health-related quality of life (HRQOL)2. The disease course can be unpredictable and children commonly experience a myriad of physical3,4,5,6,7 and emotional5,6,7,8,9 symptoms that may restrict physical and social interactions5,7,9,10. While management of JIA is shared by the child and family, adolescents are expected to assume a greater role in disease management as they mature11. Greater involvement in self-management could prevent worsening of the disease and symptoms11,12 and facilitate successful transition to adult healthcare13. However, the vast majority of adolescents do not receive comprehensive disease education linked with self-management care because of (1) difficulty accessing these services, (2) limited availability of trained professionals, especially in rural areas, and (3) costs associated with these therapies14,15,16.
With emerging interactive and communication technologies, especially the Internet, new media for the delivery of health interventions are now available17. The Internet has emerged as one of the top health information resources and modes of social communication for youth18 and is therefore ideally suited to improve the accessibility and acceptability of healthcare services for young people19. Internet interventions are treatments based on effective face-to-face interventions that are transformed for delivery through the Internet. Usually they are highly structured, self-guided, or partly self-guided (i.e., with therapist or coach support), tailored to the user’s needs, and interactive17. While this is a burgeoning field, formal evaluations of the effect of Internet health interventions on health outcomes, level of resource utilization, and user satisfaction have lagged far behind their development20. Positive outcomes have been found for Internet self-management interventions for adult21,22,23,24,25,26,27 and pediatric28 health problems across a range of outcomes related to knowledge, behavioral change, symptom management, and health status/HRQOL; however, too few rigorous randomized controlled trials (RCT) have been conducted to endorse their use and none have been conducted in JIA28.
A qualitative study was conducted to determine the information and self-management needs of adolescents with JIA and their caregivers16. This information was used in the development of an interactive Internet intervention with brief telephone support to deliver self-management care for youth with JIA and their parents. A pilot RCT (NCT01011179) was used to determine the feasibility of the “Teens Taking Charge: Managing Arthritis Online” Internet program. The feasibility objectives included (1) piloting the intervention, attention control strategies, and outcome measures; and (2) determining adolescents’ compliance with and perceptions regarding the acceptability of and satisfaction with the Internet program. Our study also provided an opportunity to obtain estimates of treatment effects in primary (HRQOL), secondary (physical and emotional), and mediating (JIA-specific knowledge, self-efficacy and adherence) outcome measures to allow the calculation of an appropriate sample size for the future RCT, while acknowledging that these estimates may be unstable because of the sample size.
MATERIALS AND METHODS
Participants included 46 adolescents with JIA who were recruited between October and November in 2008 from 4 pediatric tertiary care centers across Canada. Adolescents were eligible to participate if they were (1) between 12 and 18 years of age, (2) diagnosed with JIA, (3) able to speak and read English or French, and (4) able to complete baseline online outcome measures. Adolescents were excluded if they had cognitive impairments or major comorbid illnesses (medical or psychiatric) that could have affected their ability to understand and use the Web-based program.
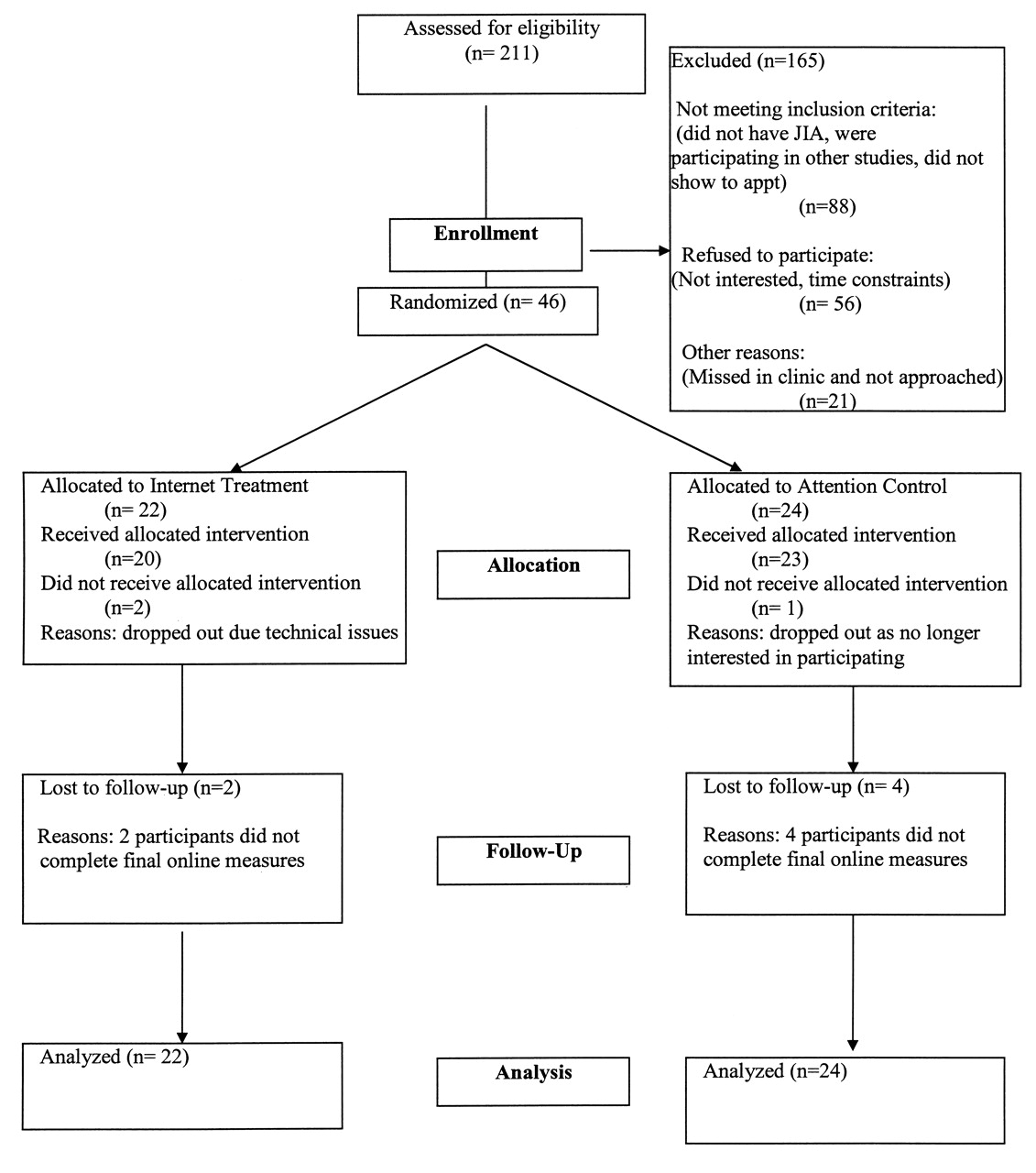
Figure 1, developed from the Consolidated Standards of Reporting Trials statement29, illustrates the enrollment progression of participants throughout our study. A total of 211 adolescents were assessed for eligibility and 165 were excluded. Therefore our participation rate was 45%, with a range of 26% to 59% across sites. Two participants in the experimental group and 1 control group participant actively withdrew from our study. Six participants (2 in the experimental group; 4 in the control group) did not complete online posttreatment assessments (Figure 1). Thus our attrition rate was 19.5%. Intent-to-treat analysis was used, and therefore the effective number of cases analyzed was 22 for the experimental group and 24 for the control group.
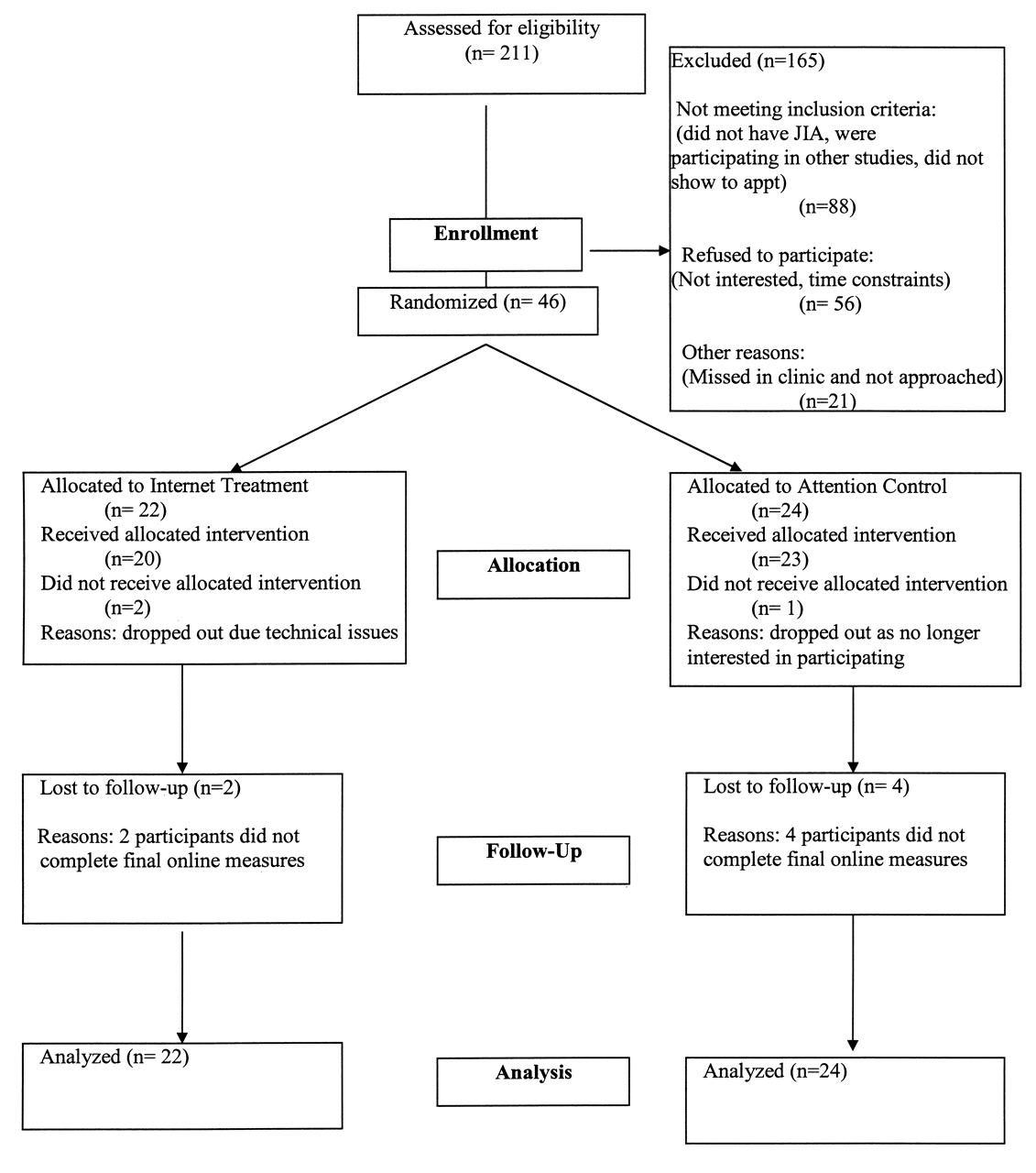
The progress of participants through the study.
Procedures
A pilot nonblind RCT design (NCT01011179) was used to test the feasibility of the “Teens Taking Charge: Managing Arthritis Online” Internet intervention, as outlined in Figure 1. Our study was approved by the Research Ethics Boards at the participating institutions. Eligible patients listed on the 4 participating hospitals’ Rheumatology Database Registries who had a regularly scheduled clinic appointment during the 2-month recruitment period were sent a study information letter inviting them to participate.
Once informed consent was obtained, the research assistants obtained baseline demographic and disease-related data on participants from their medical charts. All measures were completed online by adolescents and parents in the clinics prior to randomization. A fixed allocation randomization scheme was used. Specifically, blocked randomization was employed, using blocks of 10 to assign participants to the 2 treatment conditions during the course of randomization by each of the 4 study centers. An online random number generator was used to produce the blocked randomization. Group assignments were identified by ID number in sealed envelopes during the recruitment period. Following completion of online pretreatment assessments, the project coordinator opened the sealed envelope to reveal group assignment. After randomization, adolescents and their parents were contacted and instructed on the procedures to be followed. Both treatment groups continued to receive medical care through a subspecialty pediatric rheumatology clinic.
Treatment conditions
For the experimental group, the intervention was a 12-week multicomponent treatment protocol that consisted of self-management strategies, disease-specific information, and social support that was available in English and French. It was delivered on a restricted website and through regular telephone contact with a trained coach (a non-health-care professional with an undergraduate degree in psychology). The 12 modules for adolescents included learning about the different types of arthritis, understanding how arthritis is diagnosed, arthritis medications, managing symptoms (pain, stiffness, and fatigue), managing stress and negative thoughts, relaxation, distraction, other types of care (exercise, nutrition, splints), self-monitoring and supports, lifestyle issues, and looking ahead (education, vocation, transitional care issues). There were 2 modules specifically for parents/caregivers, to help them encourage healthy behavior (the effect of arthritis and helping parents learn to let go). Parents were able to view the materials on the teen website. The content is multilayered, interactive, written at a grade 6–7 level and geared to the self-management needs identified by adolescents and their parents16. Adolescents were asked to log on to the site once per week to complete a module that was designed to take between 20 and 30 minutes. At the beginning of the program, adolescents developed their own personal goals for the program and kept track of their progress in “My Journal.” Usability testing of the Internet program and an outline of the program content has been described30.
The intervention group was contacted by a coach on a weekly basis for 12 weeks using standardized scripts. The weekly telephone calls were structured and the primary coach duties were to (1) review the previous week’s homework, knowledge quiz, and goals; (2) determine whether the participant completed the module and answer questions regarding the material and/or practice exercises (self-management strategies); and (3) provide guidance and help solve any problems that had arisen. If participants asked questions that the coaches could not answer, the coach redirected them to their rheumatology provider. The coach also monitored discussion board postings daily. All calls were recorded to ensure integrity of the intervention. Participants received a mean of 1.6 phone calls per week to maintain contact, with the average duration of calls 17.3 min (range 7–30 min).
For the attention control group, credible attention strategies consisting of weekly phone contact by a trained research assistant to discuss adolescents’ “own best efforts” at managing their JIA were administered over the 12-week period. The research assistant used a standardized script for these calls. Participants received a mean of 1.4 phone calls per week to maintain weekly contact; the average duration of calls was 3 min (range 2–6 min). If participants asked for information related to self-management of their JIA, the research assistant responded that she was not trained to provide such information and redirected them to their doctor or nurse. All calls were recorded to ensure integrity of the attention strategies. Following completion and receipt of their posttreatment assessment, participants were offered the opportunity to receive the Internet intervention treatment and directed to their healthcare team for questions regarding website materials. Only 7/24 (29%) control group participants chose to access the Internet treatment following posttreatment assessment.
Assessment procedures
Prior to randomization, all participants completed pretreatment measures online during regularly scheduled clinic visits. Following completion of the 12-week study period, participants were contacted to complete the same measures online at home. Adolescents and parents were able to complete these measures in less than 30 minutes.
Primary outcome measure
HRQOL was measured using the Juvenile Arthritis Quality of Life Questionnaire (JAQQ)31. The questionnaire is divided into 4 dimensions: gross motor function, fine motor function, psychosocial function, and general symptoms. A 7-point ordinal scale is used to rate responses to each item from 1 (none of the time) to 7 (all of the time), based on how often the item was a problem for the child over the past 2 weeks. Total score was composed of the 4 dimension scores (top 5 items of that dimension) divided by 4, with higher scores denoting poorer HRQOL. The JAQQ has evidence of construct validity and responsiveness2,31,32,33,34,35.
Secondary outcome measures
Pain was measured using the 47-item Recalled Pain Inventory (RPI), which has evidence of construct validity in adolescent arthritis populations4. RPI measures current, least, average, and worst pain intensity over the past week on an 11-point numerical rating scale (NRS; e.g., 0 = no pain to 10 = severe pain), as well as pain unpleasantness and interference ratings and number of painful body locations.
Stress was measured using the 30-item perceived severity of stress questionnaire (PSQ), which has evidence of reliability and validity in general populations36. Adolescents were asked to rate how often certain experiences of stress occurred within the past 2 weeks on a 4-point ordinal scale from “almost never” to “usually.”
Mediating outcome measures
JIA-specific knowledge was measured using the 24-item Medical Issues, Exercise, Pain, and Social Support Questionnaire (MEPS)37. Items were rated on an 11-point NRS with higher scores indicating greater knowledge. This measure has evidence of construct validity as well as test-retest reliability37.
Self-efficacy was measured using the Children’s Arthritis Self-Efficacy (CASE) scale, which is an 11-item measure38. Adolescents were asked to rate how well, on a 5-point ordinal scale, they are able to manage symptoms, emotional consequences, and activities related to their arthritis, with higher scores indicating better self-efficacy. The CASE has evidence of face, content, concurrent, as well as internal consistency reliability38.
Adherence to treatment (medications, exercises, and wearing splints) was assessed using the JIA-specific Child Adherence Report Questionnaire (CARQ) and the Parent Adherence Report Questionnaire (PARQ)39. Preliminary data provide evidence of good construct validity and reproducibility39.
Other Internet program outcome data included treatment acceptability and satisfaction, determined using a questionnaire developed by the investigators. The questionnaire used a Likert scale for items regarding health coach performance and asked the teens to indicate whether they found the program tools to be helpful. This questionnaire also allowed participants to provide comments about the program’s ease of use and features as well as to provide suggestions for program improvements and to indicate whether they would recommend the program to other families. Other outcome data included compliance (defined as completion of a minimum of 9/12 modules) and usage patterns (number of times each module was accessed) during the 3-month intervention. Expectation about treatment effectiveness was determined at baseline using an 11-point NRS (0 = don’t think it will help at all, to 10 = think it will help a lot)40.
Data analyses
Given that this was a feasibility pilot RCT, we did not conduct an a priori sample size calculation. We planned to recruit 20 participants per group. Data were analyzed using SAS software41. As per the “intention to treat” approach, all participants were included in the final analysis and according to the arm (experimental or control) to which they were randomized. Descriptive statistics were used to describe characteristics of the sample using means and SD for continuous factors, and frequencies and proportions for categorical factors. T-test and chi-squared analyses were conducted to compare baseline characteristics between the 2 treatment arms. Separate analyses were conducted for each outcome. Linear mixed models were used to assess the effects of the intervention on outcomes using an analysis of covariance (ANCOVA) approach in which the posttreatment measures were compared between treatment groups using the baseline score as a covariate42. Effect sizes for mixed linear ANCOVA are expressed as Cohen’s d, interpreted as a small effect at 0.2, medium effect at 0.5, and large effect ≥ 0.843. A level of 0.05 was used as the criterion for statistical significance.
RESULTS
Sample characteristics
Table 1 summarizes the demographic and disease characteristics of the sample. Participants were 46 adolescents (32 girls, 14 boys) between the ages of 12 and 18 years (median 14.5, SD 1.48) and 1 parent of each child (83.3% women; 68.8% aged 40 to 49). The average school grade of participants was grade 9 with 35% (n = 16) and 63% (n = 29) in grade and high school, respectively. Sixty-seven percent of parents had a college degree or higher. All adolescents felt comfortable using the computer/Internet, while 89.6% (n = 41) of parents felt comfortable with Internet use. Most of the participants (82.9%, or n = 38) were on medications at baseline and the number on medications dropped to 76% (n = 35), with a similar pattern observed in both groups posttreatment. Treatment groups were similar at baseline on demographic and disease characteristics and outcome measures as outlined in Tables 1 to 4. Further, there were no significant differences in treatment expectations prior to randomization (experimental median 7.3, SD 2.6; control median 6.9, SD 2.6).
Characteristics of the sample, combined and by treatment group.
Unadjusted descriptive statistics on primary outcomes for adolescents by treatment condition.
Unadjusted descriptive statistics on secondary outcomes for adolescents by treatment condition.
Unadjusted descriptive statistics on mediating outcomes for adolescents by treatment condition.
Feasibility analyses
Participants in the experimental group were satisfied with the Internet treatment, rating the website as easy to use and highly acceptable. In particular, participants liked the content and video and audio features (relaxation and guided imagery), and personalization through interactive features. Most participants felt the e-mail system with the coach and technical assistance was helpful; however, 2 participants had initial difficulties logging on to the site, which resulted in them dropping out. Adolescents felt the coach was an essential component of the program and that the weekly calls helped to tailor the information and strategies to meet their individual needs. Participants indicated that they would recommend the site to other youth with JIA and their families.
In terms of compliance, of the 20 adolescents and their parents who stayed in the experimental group, 100% completed all their respective modules. Participants took 12 to 21 weeks to complete the program, allowing for breaks for exams, illnesses, and hospitalizations, with an average completion time of 14.7 weeks (SD 2.1). Adolescents completed on average 33.1 of the 48 interactive fields while progressing through the modules. Seventy-three percent of the adolescents entered at least 3 personal treatment goals, such as “take medications consistently,” “increase my knowledge on arthritis,” and “learn ways to relieve my pain.” Teens used the e-mail message system to communicate with the coach (range 0–8 messages, median 3.9, SD 3.2). During the intervention, participants logged in for a total of 436.9 h, resulting in 6757 hits to the website. Aside from the introduction, the website sections with the most hits were the sessions “About Arthritis,” “Managing your Symptoms,” and “Arthritis Medications.” In contrast to this, when control participants were given self-guided access to the website, there were only 156 hits to the website and 6.42 h logged on. Table 5 gives a summary of website hits by section.
Total hits by section of website for experimental and control groups.
Outcome analyses
Baseline-adjusted ANCOVA were computed to evaluate group differences on outcomes of HRQOL, symptoms (pain and stress), disease-specific knowledge, treatment adherence, and self-efficacy. No statistically significant differences were found between the 2 arms (experimental and control) with respect to the overall JAQQ score, nor any of the subscales (p > 0.05 for all subscales), as shown in Table 2. Overall, effect sizes (ES) were either very small or small (gross motor function ES 0.21; fine motor function ES 0.06; psychosocial ES 0.22; systemic systems dimension ES 0.06; and JAQQ total score ES 0.20). In terms of symptoms, average weekly pain intensity on the RPI at posttreatment was significant (p = 0.03), as shown in Table 3, with a medium ES 0.78. Over time, average weekly pain intensity scores increased in the control group, while it decreased in the experimental arm. There was no apparent relationship between intervention status and stress levels as measured by the PSQ (p = 0.66; ES = 0.20). The greatest change was observed in disease-specific knowledge. After adjusting for baseline values, postintervention disease-related and medication-related knowledge scores were significantly higher (p < 0.001) for patients in the experimental group, as shown in Table 4, with a large ES of 1.32. No statistically important differences were found for treatment adherence (medical or exercise; p > 0.05; ES ranged from 0.26 to 1.11) or self-efficacy (p > 0.05 for all subscales; ES ranged from 0.11 to 0.31). No statistically significant results were found for any of the outcome measures completed by parents.
DISCUSSION
Our study examined the feasibility of an Internet-based self-management intervention for youth with JIA. Overall there was a moderate accrual rate across the 4 centers, with low dropout rates in both groups. Program usage patterns showed that users completed the program as instructed, used communication features, and were engaged through goal-setting and completing personalized information. The Internet treatment was rated as acceptable and satisfying to use by youth and their parents. There was initial evidence of the efficacy of the Internet self-management program in improving knowledge and decreasing pain in youth in the experimental group compared to those in the control group.
Because of the novel method of treatment delivery, we were interested in documenting the feasibility (acceptability, satisfaction, and compliance) of the Internet treatment program. The participation rate in our study (45%) was similar to rates in other Internet-based self-management programs for youth with chronic health conditions, suggesting acceptability of this mode of treatment28. Moreover, the attrition rate, including dropouts and those lost to followup, was low compared to other Internet-based studies in adolescents (0–28, mean 14.3) and adults, in which higher dropout rates were found22,23,24,25,26,27,28. Overall, adolescent compliance with the program was high, with the majority of participants completing the entire program. We found that parents were less compliant than adolescents in completing their treatment modules. Similar usage patterns have been described in other Internet-based studies in youth28,44. Future studies should evaluate strategies to improve user engagement and encourage parental participation with treatment. The ability to track patterns of user activity and website usage is a research advantage provided by Internet programs45,46. This enabled us to identify website modules that adolescents used more than other modules, and we will use this information to target future program enhancements.
It is evident from the usage data and participant feedback that the health coach was an integral component of the Internet program. Adolescents in the control group spent considerably less time on the website when they were given self-guided (no coach) access. This was most likely due to not having access to the coach as well as timing of access (end of school and summer holidays). Human support through brief telephone contact has improved motivation and adherence to online healthcare services, which are typically delivered over weeks to months, thereby facilitating achievement of desired health and/or behavioral outcomes21,22,23,24. The level (intense vs brief contact), type of human support (health professionals, trained personnel, and peers), and mode (phone, e-mail, telehealth) needed to maintain engagement in Internet health interventions is unknown21,22. Future research is needed to determine the minimal amount of human support required with distance treatment programs.
Our study extends work on distance treatment in youth with chronic health conditions28 by demonstrating the feasibility and initial efficacy (improved knowledge and reduced pain) of an Internet intervention with minimal therapist time in youth with JIA. A recent systematic review of Internet interventions for youth with chronic health conditions found that there was some beginning evidence that self-management interventions delivered by the Internet improved selected health outcomes in certain chronic childhood illnesses. There was conflicting evidence regarding disease-specific knowledge and HRQOL28. In our study, it is not surprising that HRQOL did not improve given the small sample size. Further, symptoms, knowledge, and other outcomes were expected to change posttreatment, while noticeable improvements in HRQOL were hypothesized to take longer (up to 12 months)47.
There are several limitations to our study that should be considered in interpreting our findings. First, our sample size is small as this was a pilot RCT, and the resultant loss in power allowed us to identify only medium and large effects, while smaller effects may have been missed. However, our results are generalizable as we recruited participants from 4 large tertiary care centers across Canada. Second, the attention control group may not have been a fair comparator to control for the attention provided by the coach as the time spent on the phone was significantly less (mean 3 min) than in the experimental group (mean 17.3 min). Future studies employing attention control strategies should not restrict the duration of telephone calls. Our study did not examine durability or maintenance of treatment effects of the program over time. In future studies it will be important to use study designs that allow for examination of maintenance of treatment effects.
Our study provides strong initial support for the feasibility (high compliance, acceptability, and satisfaction) of the Teens Taking Charge: Managing Arthritis Online Internet program for youth with JIA. Findings from our study will be used to lay the groundwork for a large multicenter RCT to determine the efficacy of the online self-management intervention in improving symptoms and HRQOL in youth with JIA. Moreover, if effective, this Internet intervention could be the first step in a “stepped care” approach for healthcare for all youth with JIA. A stepped care approach provides adolescents and their families with a simple, accessible intervention for management of their disease and proceeds to more intense (face-to-face) treatments as necessary48. A self-guided Internet self-management program with brief telephone support may help overcome current barriers that prevent adolescents with JIA and their families from receiving these therapies.
Acknowledgments
The authors thank all the adolescents and parents who participated in our study. We also thank Michele Gibbon, Aleasha Warner, and America Uribe for their help in recruiting participants from the study centers. We also thank Nina Vitopolous for her help.
Footnotes
-
Supported by The Canadian Arthritis Network and The Arthritis Society. Dr. Stinson’s postdoctoral work was supported by a Canadian Institutes of Health Research Post-Doctoral Research Fellowship and Canadian Child Health Clinician Scientist Program Career Enhancement Award. Drs. Feldman and McGrath hold Canada Research Chairs.
- Accepted for publication February 4, 2010.








{kind=link}