

Abstract
Objective. To compare outcomes over the first 8 years in patients with early rheumatoid arthritis (RA) recruited in the 1990s and the 2000s, with a special focus on functional disability and its possible predictors.
Methods. Data were acquired from 1938 patients with early RA (American College of Rheumatology 1987 criteria) included in the BARFOT study, who had completed the 8-year followup. The patients were divided into 2 cohorts: cohort 1 (n = 928, 68% women) included from 1992 to 1999 and cohort 2 (n = 1010, 70% women) included from 2000 to 2006. Health Assessment Questionnaire (HAQ), 28-joint Disease Activity Score (DAS28), visual analog scale pain, and radiographs of hands and feet scored by the van der Heijde modified Sharp method were assessed during the 8 years. Longitudinal data analyses were performed using a generalized linear model.
Results. Despite more active medical treatment during the 2000s, the courses of HAQ and pain showed no difference between the cohorts during followup, in either women or in men, with significantly higher levels in women compared with men. However, as expected, disease activity decreased more over time in cohort 2 compared with cohort 1, for both sexes, and women in cohort 2 had less radiographic progression compared with cohort 1. HAQ was associated with DAS28, pain, radiological scores, and sex in both cohorts, and in cohort 2 also with age and smoking.
Conclusion. Patients included in the 2000s had lower disease activity, but not less activity limitation and pain over 8 years of followup despite more active treatment. Pain, aging, and smoking might explain why patients included in the 2000s still had the same disability levels as those included in the 1990s.
The treatment strategy for patients with rheumatoid arthritis (RA) has changed considerably over recent decades. In the beginning of the 1990s, the importance of early treatment with disease-modifying antirheumatic drugs (DMARD) was emphasized, and then methotrexate (MTX) successively became the first drug of choice. In the beginning of the 2000s, a tight control regimen was introduced and at the same time the biological drugs became available.
The effect of the new treatment strategies on disease activity was reported in early RA cohorts in the 2000s1,2. However, studies comparing the longterm outcome in patients with disease onset in the 1990s and in the 2000s are scarce. In a longitudinal observational study over 5 years of patients with early RA from the BARFOT (Better Anti-Rheumatic PharmacOTherapy) cohort, we reported that patients diagnosed in the 2000s achieved a higher frequency of clinical remission and good/moderate European League Against Rheumatism (EULAR) response than those diagnosed in the 1990s, suggesting more active medical treatment3. In both cohorts, fewer women achieved remission and moderate/good EULAR response compared with men. Interestingly, however, improvement in pain, patient’s global health, and activity limitation/disability assessed with the Health Assessment Questionnaire (HAQ) did not differ between the 2 patient cohorts.
It is thus obvious that pain, patient’s global health, and disability are not solely consequences of inflammation. In some patients, the inflammatory pain becomes a more noninflammatory widespread pain with time4,5,6, which may also affect patient’s global health and disability7.
Earlier studies have reported dissociation between reduction in disease activity and reduction in activity limitation. In a study on patients with early RA from Sweden recruited in the 1980s, disease activity decreased while HAQ deteriorated during a 10-year followup8. Also, in another Swedish cohort recruiting patients with early RA during the 1990s, disease activity improved while disability slowly deteriorated during 2 and 8 years of followup9,10. Whether this dissociation also applies for patients diagnosed in the biological era is uncertain, although disability has been reported to decline in the 2000s11.
Disability in early RA is suspected to be influenced by inflammatory activity. But later in the disease course, at least in patients diagnosed in the previous century, disability seems related more to joint damage12,13. Because radiological progression has been reported to be milder with the new therapy strategies14, it has also been suggested that disability decreases. In fact, it has been reported that the progression of functional disability among patients with RA in the 2000s is largely explained by the aging process15.
To further analyze the course of functional disability, a patient-important outcome, our current extended study was performed. The 2 cohorts of patients with early RA recruited in the 1990s and 2000s, respectively, were prospectively followed and monitored over 8 years. The primary objective was to analyze the 2 patient cohorts with special focus on functional disability, and next its possible predictors, including radiological damage, with the hypothesis that functional disability in well-treated patients is mainly dependent on pain.
MATERIALS AND METHODS
Patients
In all, 1938 of the 2565 patients included in the BARFOT observational prospective multicenter study were available for the 8-year followup. Cohort 1 consisted of 928 patients from the 1990s and cohort 2 of 1010 patients from the 2000s. Of the 627 patients lost to followup (333 from 1992–1999 and 294 from 2000–2006), 406 died (cohort 1, 214 and cohort 2, 192), 36 moved (cohort 1, 16 and cohort 2, 20), 55 rejected participation (cohort 1, 11 and cohort 2, 44), and 130 of unknown reasons (cohort 1, 91 and cohort 2, 39). The patients lost for followup in both cohorts were older at baseline, had more inflammation, and had worse HAQ.
The patients were included consecutively between 1992 and 2006 when diagnosed with RA according to the American College of Rheumatology 1987 classification criteria16. At baseline, they had a disease duration of ≤ 12 months. The patients were assessed according to a structured protocol at baseline, 3 and 6 months, and 1, 2, 5, and 8 years. The patients were treated with DMARD in accordance with the recommended treatment strategy in Sweden as earlier described3.
Clinical disease assessments
Functional disability was assessed using the Swedish version of Stanford HAQ (0–3, best to worse)17. The minimal clinically important difference (MCID) was set to ≥ 0.22 for change in the HAQ score18.
Disease activity was measured by the composite index Disease Activity Score calculated in 28 joints (DAS28; range 0–9.4, best to worse)19. DAS28 includes the number of swollen joints (range 0–28, best to worse), number of tender joints (range 0–28, best to worse), patient’s global assessment of disease activity (PtGA) measured on a visual analog scale (VAS; range 0–100 mm, best to worse), and the erythrocyte sedimentation rate (ESR; 0–150 mm/h). The threshold of MCID for DAS28 was a change of ≥ 1.220. Pain was measured by VAS (0–100 mm, best to worse), with threshold of an MCID change of ≥ 10 mm18. ESR was analyzed by the Westergren method and rheumatoid factor (RF) was measured according to the current laboratory standards at the hospitals.
Radiographic assessments
Posterior-anterior radiographs of the hands and feet were assessed at baseline and at 1, 2, 5, and 8 years according to the van der Heijde modification of the Sharp score (SHS)21. The SHS (range 0–448), erosion score (ES; range 0–280), and joint space narrowing (JSN; range 0–168) were presented. The films were read by 1 of 2 experienced readers. Double readings of a fraction of films showed good agreement between the 2 readers. The intraclass correlation coefficient for SHS was excellent (0.940–0.998). Radiographic progression from baseline to 8 years was defined as a change in SHS > 8, i.e., > 1 unit/year, based on the assumption that a change of 1 unit per year is the lowest value of minor radiographic change22,23.
Statistics
Statistical analyses were performed using SPSS Statistics 21 software. All significance tests were 2-tailed and conducted at the 0.005 significance level because of multiple comparisons. To test differences between groups, the chi-square test was used for proportions and the Kruskal-Wallis with posthoc pairwise analysis when comparing more than 2 groups, or the Mann-Whitney U test when comparing 2 groups for continuous variables, because some of the variables were not normally distributed (Shapiro-Wilks < 0.05). For within-group comparisons, the Wilcoxon test was used. The longitudinal data analysis was performed with generalized estimating equations, similar to multiple linear regression analysis but with adjustment for within-patient correlations between different measurements, allowing investigation of longitudinal data24. Longitudinal associations between HAQ, clinical, and radiological predictors were split into 2 separate models because of the linearity of the HAQ curve, 1 from baseline to 1-year followup, and the other from 1 to 8 years of followup. Separate models were performed for DAS28, pain, ES, and JSN because of high correlations between these variables. In the analysis, HAQ was the dependent variable; DAS28, pain, ES, and JSN were the predictors; and age, sex, RF, smoking habits, and duration were analyzed as covariates. Variables were included in the models if they had a significance level of p < 0.1 in the univariate analyses.
Ethical considerations
All patients gave their informed consent and the study was performed in accordance with the Declaration of Helsinki. Ethical approval for the present study was obtained (EPN 2014/1986-31/1).
RESULTS
Baseline demographic and clinical characteristics
The 1938 patients were divided into 2 cohorts: cohort 1 (n = 928, 68% women) included 1992 to 1999 and cohort 2 (n = 1010, 70% women) included 2000 to 2006. Demographic and clinical characteristics at baseline are shown in Table 1. The women in cohort 2 were older, more frequently RF-positive, had higher DAS28, and had worse pain and global health. Men in cohort 2 had higher DAS28 (Table 1). When divided into groups according to age, there were more patients ≥ 75 years in cohort 2 than in cohort 1 (11% vs 5%, p < 0.001).
Demographic and clinical characteristics at baseline. P values denote the significance of differences between groups calculated by the Mann-Whitney U test if continuous and by the chi-square test if proportions. Values are mean (SD) unless otherwise specified.
Clinical assessments over 8 years
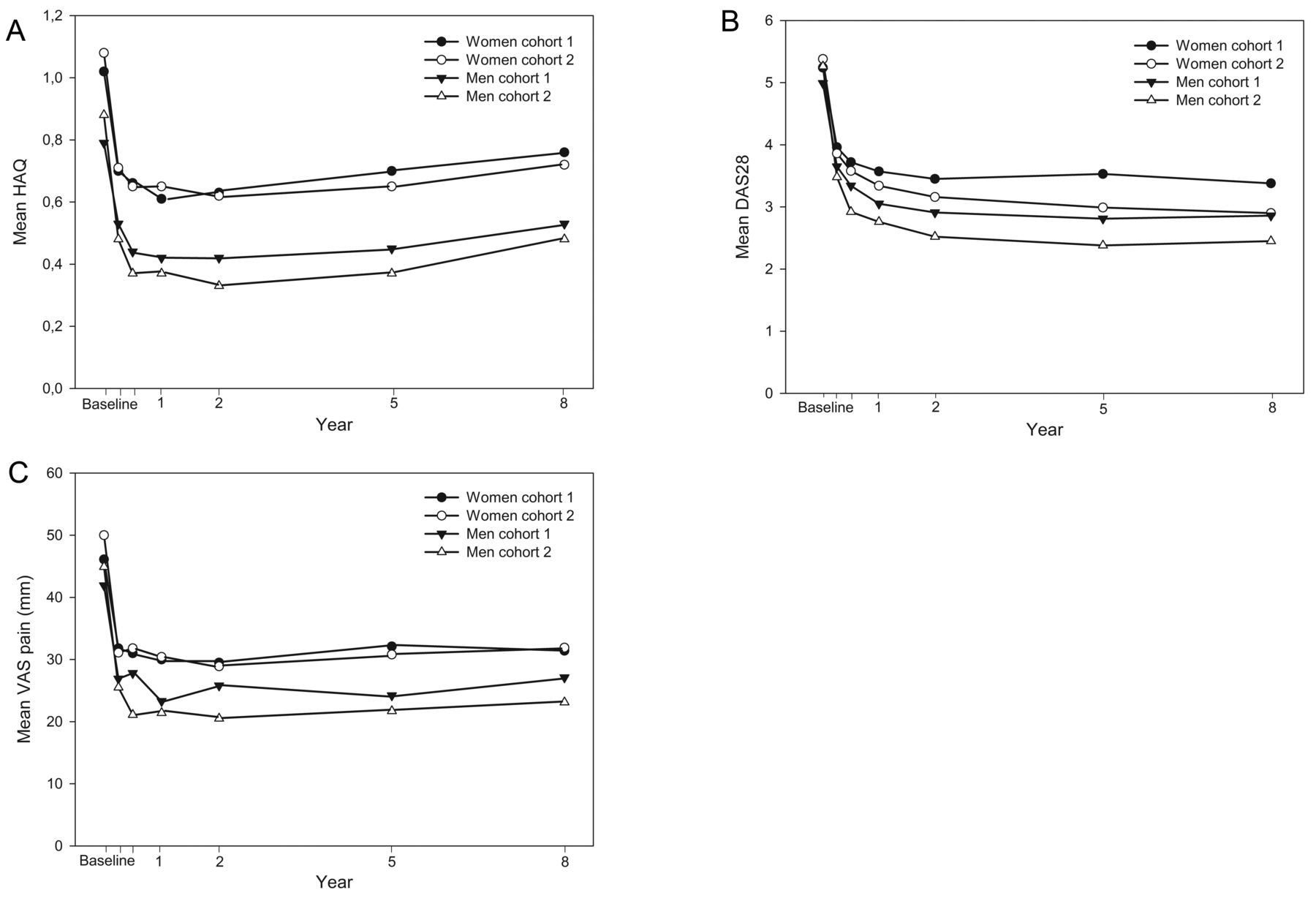
HAQ decreased significantly from baseline to the 1-year followup, but then slightly increased over time to the 8-year followup (Figure 1A). For the women in both cohorts, HAQ leveled off at a significantly higher level than in men, but there were no significant differences between the 2 cohorts for women or for men. Mean HAQ (95% CI) adjusted for sex, age, RF, and DMARD at baseline was 0.91 (0.86–0.95) in cohort 1 and 0.98 (0.94–1.02) in cohort 2 (p = 0.020). At 1 year it was 0.52 (0.48–0.55) in cohort 1 and 0.51 (0.47–0.54) in cohort 2 (p = 0.714). At the 8-year followup it was 0.64 (0.60–0.69) in cohort 1 and 0.59 (0.54–0.63) in cohort 2 (p = 0.079). According MCID for HAQ, 61% of the women in cohort 1 and 63% in cohort 2 improved in HAQ between baseline and 1 year (p = 0.555). The corresponding rates for men were 63% and 66%, respectively (p = 0.285). At the 8-year followup, 54% of the women in cohort 1 and 59% of the women in cohort 2 had a clinical improvement compared with baseline (p = 0.235). The corresponding rates for men were 55% and 63%, respectively (p = 0.109). Because disability increases with age, we further assessed HAQ over time in different age groups, and as shown in Figure 2, HAQ increased more in patients 65 years and older than in those younger at the 8-year followup (p < 0.001).
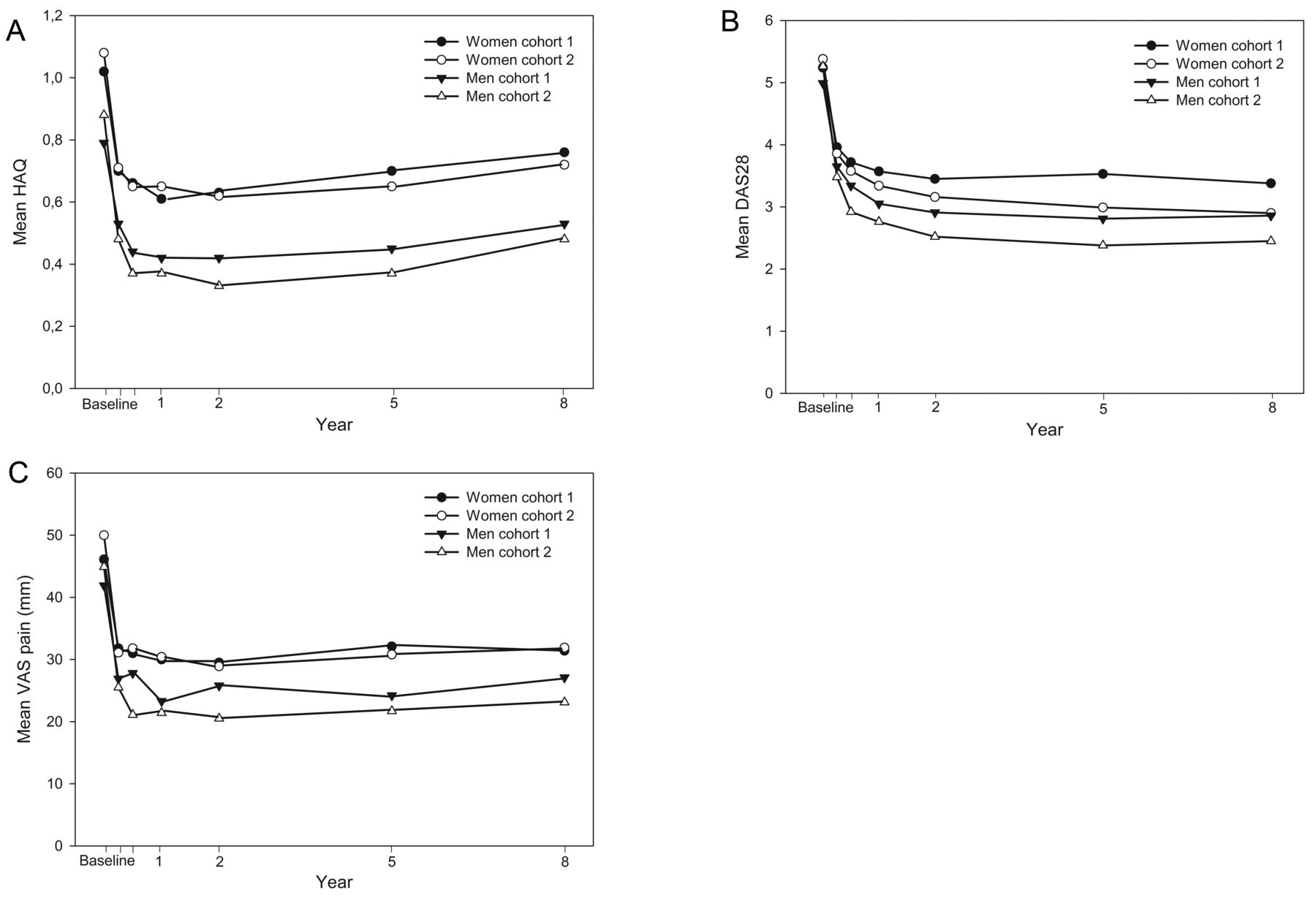
Functional disability, disease activity, and pain measures during 8 years of followup. Cohort 1 consists of patients included between 1992 and 1999, and cohort 2 of patients included between 2000 and 2006. Data are reported separately for women and men. (A) The mean HAQ in the separate cohorts over time. (B) The mean DAS28 in the separate cohorts over time. (C) Mean VAS pain in the separate cohorts over time. HAQ: Health Assessment Questionnaire; DAS28: 28-joint Disease Activity Score; VAS: visual analog scale.
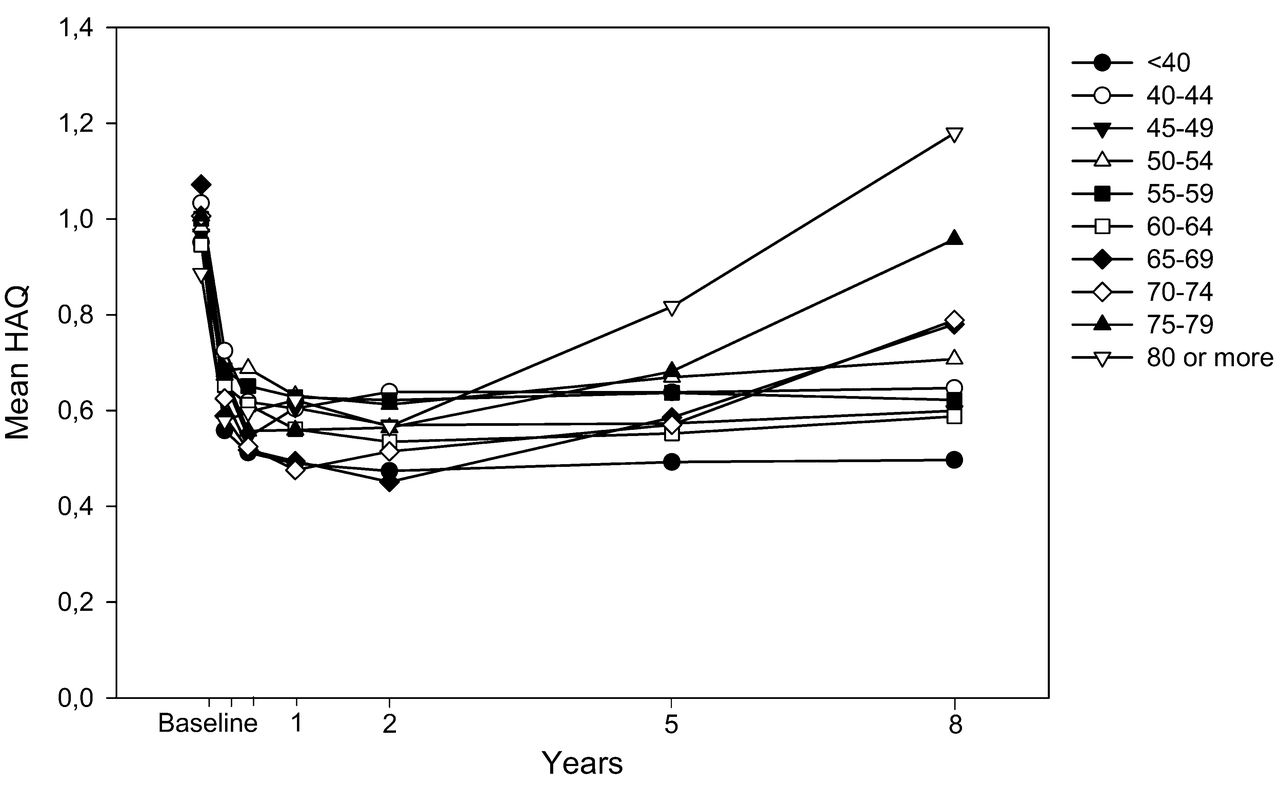
Mean HAQ over time in patients with rheumatoid arthritis based on age at baseline. HAQ: Health Assessment Questionnaire.
During the first year, DAS28 decreased significantly, thereafter it leveled off and decreased only slightly until the 8-year followup in both cohorts and for both sexes (Figure 1B). In women, however, the decrease was lower than in men in both cohorts.
Mean DAS28 (95% CI) adjusted for sex, age, RF, and DMARD at baseline was 5.09 (4.92–5.26) in cohort 1 and 5.40 (5.21–5.60) in cohort 2. Sixty-three percent of the women in cohort 1 and 72% in cohort 2 improved in DAS28 between baseline and 1 year according to MCID (p = 0.002). The corresponding rates for men were 68% in cohort 1 and 80% in cohort 2 (p = 0.008). At the 8-year followup, 66% of the women in cohort 1 and 80% of the women in cohort 2 had a clinically important improvement compared with baseline (p < 0.001). The corresponding rates for men were 71% and 86%, respectively (p < 0.001).
Pain showed a similar pattern as HAQ with a decrease during the first year in both cohorts and in both women and men. Then it leveled off in both cohorts, at a significantly higher level in women, but with no significant difference between the 2 cohorts for either women or men (Figure 1C). Mean pain at baseline (95% CI) adjusted for sex, age, RF, and DMARD was 45.4 mm (41.4–49.5) in cohort 1 and 49.2 mm (45.5–52.9) in cohort 2 (p = 0.183). Between baseline and the 1-year followup, 51% of the women in cohort 1 and 62% in cohort 2 improved in pain, according to MCID (p = 0.094). The corresponding rates for men were 61% versus 68% (p = 0.201). Fifty-five percent of the women in cohort 1 and 62% of the women in cohort 2 improved in pain according to MCID from baseline to the 8-year followup (p = 0.061). For men the percentages were 58% vs 62%, respectively (p = 0.011).
Radiology
At baseline, SHS was higher in women in cohort 2, mainly because of a higher JSN score (Table 1). In men, SHS did not differ between the cohorts at baseline. In both cohorts, women and men progressed radiographically (Figures 3A–C). The mean change in SHS (SD) during the 8 years for women was 20 (27) in cohort 1 versus 16 (20) in cohort 2 (p = 0.009), and in men was 16 (19) versus 14 (18), respectively (p = 0.186). Over 8 years, 52% of the women in cohort 1 were classified as radiographic progressors versus 51% in cohort 2 (p = 0.662), and in men the percentages were 55% versus 46%, respectively (p = 0.041). Women in cohort 2 had a higher JSN at baseline (Table 1), 1-year followup, and 2-year followup (p < 0.001 and p = 0.003, respectively; Figure 3B). In men, there was no significant difference in JSN between the cohorts at any timepoint (Figure 3B). Women in cohort 2 had a lower ES at 2-, 5-, and 8-year followup (p < 0.001, p < 0.001, and p = 0.010, respectively; Figure 3C). Men in cohort 2 had a lower ES at 2- and 5-year followup (p < 0.001 and p < 0.001, respectively; Figure 3C).

Radiographic scores during the 8 years of followup. Cohort 1 consists of patients included between 1992 and 1999, and cohort 2 of patients included between 2000 and 2006. Data are reported separately for women and men. (A) The mean SHS in the separate cohorts over time. (B) The mean JSN in the separate cohorts over time. (C) The mean ES in the separate cohorts over time. SHS: van der Heijde modification of the Sharp score; JSN: joint space narrowing score; ES: erosion score.
Associations between HAQ, clinical, and radiological variables
The cohorts were analyzed in separate models (Table 2). In both cohorts, HAQ was associated with DAS28, pain, ES, and sex in univariate models for the short time interval between baseline and 1-year followup. For the longterm interval, between the 1- and 8-year followup, there were associations in the univariate models between HAQ and DAS28, pain, ES, JSN, and sex in both cohorts, and for cohort 2 there was also an association with age (Table 2).
Association between disability (HAQ) and clinical characteristics with generalized estimating equations, univariate models in the separate cohorts.
In multivariate models for the short-term interval (baseline to 1 yr), HAQ was associated in both cohorts with DAS28, pain, and ES when controlled for sex, age, RF, and smoking habits (Table 3A). Additionally, HAQ was in all separate models associated with sex in both cohorts and smoking habits in cohort 2.
Association between disability (HAQ) and DAS28, pain, and ES, from baseline to 1-year followup with GEE and multivariate model, controlled for sex, age, smoking habit, and duration for the separate cohorts.
In multivariate models for the longterm interval (1–8 yrs), HAQ was associated with DAS28, pain, ES, and JSN controlled for sex, age, RF, and smoking habits in both cohorts (Table 3B). HAQ was also associated with sex in both cohorts in all separate models, and with smoking habits and age in cohort 2. Thus, the differences between the 2 cohorts in these longitudinal analyses were the relationship between HAQ and smoking habits, as well as age in cohort 2.
Association between disability (HAQ) and DAS28, pain, ES, and JSN, from 1 year to the 8-year followup with GEE and multivariate model, controlled for sex, age, RF, and smoking habit for the separate cohorts.
In a posthoc analysis of current smokers, cohort 2 had a mean HAQ of 0.63 (0.59) versus 0.53 (0.59; p = 0.008) at the 5-year followup compared with nonsmokers, and at the 8-year followup, 0.71 (0.64) versus 0.60 (0.64), respectively (p = 0.008). There were no differences in HAQ change over time, short- or longterm, among nonsmokers, current smokers, and previous smokers in any of the cohorts.
Medical treatment
At baseline, patients in cohort 2 were more often treated with MTX than patients in cohort 1 (cohort 2: women 64% and men 65%, cohort 1: women 26% and men 26%). At the 8-year followup, this difference had leveled off. Over time there were no differences in treatment with conventional DMARD between women and men in the 2 cohorts (data not shown).
The use of biologics had increased from none at baseline to 28% in women and 22% in men in cohort 2, and to 13% and 12% in cohort 1, respectively, after 8 years.
Concerning glucocorticoids (GC), 32% of the patients (30% women, 37% men, p = 0.035) in cohort 2 and 47% (45% women, 51% men, p = 0.077) in cohort 1 started therapy with GC, alone or in combination with DMARD at baseline. At the 8-year followup, there were no differences in GC treatment between the 2 cohorts or between women and men in either cohort (data not shown).
DISCUSSION
Our study compares clinical and radiological data over 8 years in 2 cohorts of patients with RA included in the 1990s and 2000s in an observational prospective multicenter study. Despite more active medical treatment in the 2000s, there was no difference in functional disability between the 2 cohorts over time. The functional disability was affected by both disease-specific and more general factors. During the first year, disease-specific factors such as DAS28 and pain seemed to be important, and at a later stage radiological progression, aging, and smoking also seemed to influence functional disability.
At presentation, the 2 cohorts differed in some characteristics. The women included in the 2000s were older and more often RF-positive, similar to the findings reported by Diffin, et al, who compared patients from the same time periods as in our present study25. The higher rate of RF positivity in women included in the 2000s might have been due to their older age26,27. Both women and men included in the 2000s had higher disease activity measured by DAS28, suggesting that pain-related measures, PtGA, and tender joint count could be the causes3,7.
In the 8-year longitudinal followup of clinical data, HAQ, DAS28, and pain showed similar patterns to the ones we found in the 5-year followup of these patients3. The lower level of disease activity over time in patients included in the 2000s might be explained by more active medical treatment in the 2000s, a result comparable with other longitudinal cohort studies28.
HAQ decreased over time in both cohorts and in both sexes, though women in both cohorts leveled off at a higher level than men. The difference in HAQ level between women and men has also been reported previously9,28,29.
From the 1-year followup, HAQ slightly increased in both sexes and in both cohorts. A more detailed study of HAQ in different age groups showed a more pronounced increase in patients ≥ 65 years at baseline. Sokka, et al reported a higher change in HAQ score over 5 years, in both patients with RA and in the general population, in individuals older than 70 years15, and similar findings were described by Michaud, et al30. The association between HAQ and age is also described by Kapetanovic, et al, but in that study, age affected HAQ only slightly, at baseline and at the 10-year followup, perhaps because the patients in that study were younger at baseline31.
Interestingly, despite more active treatment and a larger reduction of inflammatory activity in cohort 2, there was no difference in HAQ over time between the 2 cohorts in either women or men. The same pattern was seen for pain. A suggested explanation for this common pattern for HAQ and pain was the high correlation between HAQ and pain measures3,6,7,32.
HAQ was found to be associated with disease activity and pain in the short- and the longterm followup in both cohorts; these associations have been shown earlier3,7,28,30,31. Studies in animal models report that pain could be triggered in an autoantibody-dependent manner. In patients with RA, this might be the case independent of inflammation, which could explain the results in our present study, with a rather high pain score in patients with low or moderate disease activity, resulting in the increased HAQ in those patients33.
The similar HAQ pattern in the 2 cohorts could hardly be explained by the radiological severity. Patients in both cohorts and both sexes progressed radiographically. However, both women and men included in the 1990s progressed more compared with those included in the 2000s. The slower progression and lower ES in patients included from the 2000s could be a consequence of more active treatment15. HAQ associated during the first year with ES and in the longterm with both ES and JSN in cohort 1 and with JSN in cohort 2. A possible explanation for the difference in associations between the cohorts might be the more active treatment in cohort 234.
With radiography, only skeletal damage and indirect damage of cartilage can be assessed, not the inflammation in the synovium. New imaging modalities (magnetic resonance imaging and ultrasound) have shown that patients in DAS28 remission still had considerable subclinical inflammation in the joints, a condition that could be responsible for the persistent pain, at least in part35.
We further addressed whether smoking could contribute to the HAQ development because smoking was found to be associated with HAQ in patients included in the 2000s. Michaud, et al has also reported that smoking appears to be associated to HAQ because smokers reported higher HAQ compared with nonsmokers30. In our present study, however, there were no differences in HAQ changes over time between patients with different smoking habits in any of the cohorts.
Other factors reported to influence the HAQ levels were coping strategies36 and comorbidities37, e.g., psychiatric illness, heart disease, and lung disease30,31, which we have not been able to study or to control for. Neither did we have any information on obtained physiotherapy. Another limitation was that we did not have any data on the subclinical inflammation. Further, radiological data were missing in 18% of the patients at baseline, but that appeared to have no effect on the results.
Patients included in the 2000s did not experience less disability and pain over the 8 years of followup, despite more active treatment and lower disease activity. HAQ was affected by many factors, both disease-specific ones such as disease activity and radiological progression, as well as more general factors such as pain, age, sex, and smoking. During the first year, disease activity, pain, and sex and at a later stage also radiological progression seemed to be the most important factors in determining functional disability in both cohorts. Pain, aging, and smoking might thus explain why patients included in the 2000s still had the same disability levels as those included in the 1990s. It is evident that the need for adjunct approaches must be considered for those with remaining functional disability.
APPENDIX 1.
List of collaborators: BARFOT Study Group: Sofia Ajeganova, Valentina Bala, Björn Svensson, Stefan Bergman, Ann Bremander, Åsa Häggström, Catharina Keller, Ido Leden, Annika Teleman, Jan Theander, and Anneli Östenson.
Footnotes
Financial support from The Regional Board of Southern Sweden research fund, the Swedish Rheumatism Association, The Thelma Zoegas foundation in Helsingborg, and the Foundation for Assistance to Disabled People in Skane.
- Accepted for publication February 3, 2017.








{kind=link}
{kind=link}
{kind=link}