

Abstract
Patient-centered care is widely advocated in rheumatology. This involves collaboration among patients, caregivers, and health professionals and is particularly important in chronic rheumatic conditions because the disease and treatment can impair patients’ health and well-being. Qualitative research can systematically generate insights about people’s experiences, beliefs, and attitudes, which patients may not always express in clinical settings. These insights can address complex and challenging areas in rheumatology, such as treatment adherence and transition to adult healthcare services. Despite this, qualitative research comprises 1% of studies published in top-tier rheumatology journals. A better understanding about the effect and role, methods, and rigor of qualitative research is needed. This overview highlights the recent contributions of qualitative research in rheumatology, summarizes the common approaches and methods used, and outlines the key principles to guide appraisal of qualitative studies.
The need for patient-centered care is widely recognized in rheumatology, with shared decision-making being one of the cornerstone attributes in this paradigm1,2,3. Clinical guidelines for rheumatic conditions have consistently emphasized that decision-making should explicitly consider the patients’ values, preferences, and needs3,4,5. In addition, the World Health Organization recommends that qualitative evidence is incorporated into the development of guidelines6. This is particularly relevant because the interventions for patients with rheumatic conditions may have associated risks of complications and side effects, and other effects on the social, work-related, and personal facets of their lives. Evidence on patients’ experiences, attitudes, and goals is thus needed to inform practice and policy.
Qualitative research methods can generate rich and detailed data to provide explanations and insights into the complexity of human behavior and decision-making7. Qualitative methods are used to generate hypotheses and address questions of “how” and “why”; whereas quantitative research methods are usually designed to test a hypothesis, and to answer questions of “how much” or “how often”8,9. Over the past decade, there appears to have been a growing number of publications of qualitative studies in biomedical journals across medical specialties, including rheumatology10,11,12,13 (Supplementary Table 1, available with the online version of this article). However, qualitative studies remain a small percentage of the published rheumatology research.
Between January 2015 to December 2019, qualitative studies comprised only 94 (1%) of the 8484 original research articles published in the 10 rheumatology journals with the highest impact factors (Journal Citation Reports, Social Science Edition, Clarivate Analytics) in 2018 (Annals of the Rheumatic Diseases, Arthritis & Rheumatology, Rheumatology, Seminars in Arthritis and Rheumatism, Therapeutic Advances in Musculoskeletal Disease, Osteoarthritis and Cartilage, Arthritis Care & Research, Arthritis Research & Therapy, Current Rheumatology Reports, and The Journal of Rheumatology. Only journals that publish original research articles have been listed; Supplementary Table 1, available with the online version of this article). In part, this may be because health professionals and researchers have little training and experience in conducting and appraising qualitative research methods or are uncertain as to how it can inform or affect practice and policy14.
This overview will highlight recent contributions of qualitative research to care and policy in rheumatology and introduce qualitative research, including key approaches and appraisal of qualitative work.
Contributions of qualitative research to clinical practice and policy
In this section, we summarize the insights that qualitative studies have provided in clinically relevant areas affecting multiple rheumatic conditions in adult and pediatric rheumatology: medication adherence, transition from pediatric to adult care, and the experience and management of fatigue. We have also summarized additional, selected qualitative studies in selected rheumatic conditions [gout, rheumatoid arthritis (RA), systemic lupus erythematosus] that are commonly managed by health professionals in rheumatology (Table 1).
Selected examples of qualitative studies in rheumatology.
Medication adherence. Nonadherence to medications is common across many rheumatic conditions with consequent effects on patient morbidity and even mortality15,16,17,18. Qualitative studies have been conducted in patients with rheumatic conditions to elucidate their experiences of and attitudes toward medications19,20. For example, patients with inflammatory arthritis are motivated to take disease-modifying antirheumatic drugs in an attempt to return to their normal life and avoid future disability, though many often view their medications as a “necessary evil” with “toxic” side effects and uncertain efficacy19,21,22. Medications may be perceived as a confronting reminder of their sickness and a threat to their health and well-being19,21,23. For this reason, patients may decide not to take medications in order to regain control of their health and minimize lifestyle intrusions23,24. Patients can also be overwhelmed by the burden of deciphering multiple and sometimes conflicting sources of information in order to make informed decisions about medications19,23,25,26. Studies have suggested that physicians can mitigate fears by facilitating shared decision-making and providing a supportive environment that allows patients to voice their concerns about their medications19,26,27,28.
Transition from pediatric to adult healthcare. As young patients with rheumatic conditions transition from pediatric to adult care, they must establish relationships with new clinicians, and navigate different healthcare facilities and an adult model of care during a turbulent time of physical, social, vocational, and psychological growth and change29,30. This is particularly relevant in rheumatology as many young people with juvenile-onset rheumatic diseases continue to have disease activity or significant sequelae in adult life31. Qualitative studies in adolescents transitioning to adult rheumatology care highlight the challenges they face. They describe feeling abandoned and ill-prepared to face a healthcare setting that is perceived to be sterile, depersonalized, and uninviting32,33,34. The transition process could be isolating if healthcare staff in the adult clinic focused only on medical aspects of care, with little consideration for psychosocial effects of the condition32,35,36. Patients could feel overwhelmed by the expectations to attend clinic appointments without their parents or to hand over their own clinical information to new adult providers34. In contrast, they felt more confident and secure when given an opportunity to become familiar with the adult physician and clinic, if information on the patient’s knowledge and understanding of their disease was clarified, documented, and handed over, and if they have the support of a specialist nurse in an adult clinic30,35. Patients undergoing transition to adult care appreciated a flexible approach that was tailored to their willingness and ability to take on more responsibilities and involvement in adult care34,35. Qualitative research has been used to help design and evaluate a transitional care program that incorporates the need for gradual and prepared transfer, regulated parental involvement, and an adapted setting for adolescents34,37. Qualitative studies demonstrate the importance of transitional care programs to include familiarization, joint clinics, nursing support, adequate transfer of information, and the provision of care that addresses the psychosocial priorities of young people.
Experience and management of fatigue. Fatigue is a common and debilitating symptom, and is of high priority to patients with rheumatoid arthritis (RA)38. Previously, it was rarely addressed in clinical practice as a treatment target in long-term care of patients with RA39. However, in the last few years, rheumatologists have become more aware of fatigue in the clinical setting, for example, with the increasing use of patient-reported outcomes that evaluate fatigue40. A semistructured interview study with patients with RA found that fatigue permeated multiple aspects of life including work, leisure, and family roles, and led to feelings of uselessness and loss of self-esteem41. The frustration, irritability, and loss of control from fatigue negatively affected relationships. Fatigue was overwhelming, unpredictable, and much more intense than the tiredness they felt prior to the onset of RA. Participants felt their fatigue was dismissed by health professionals, and assumed that it was not treatable and that they had to manage it on their own. The findings from this study41 were used to develop a conceptual model of fatigue42, a patient-reported outcome measure for fatigue43, and a randomized controlled trial of cognitive behavioral approaches taught to nurses and occupational therapists in rheumatology care teams to improve fatigue44. These studies highlighted the need for health professionals to address fatigue and for ways to involve a multidisciplinary team in supporting patients with this debilitating symptom.
Common approaches and methods used in qualitative health research
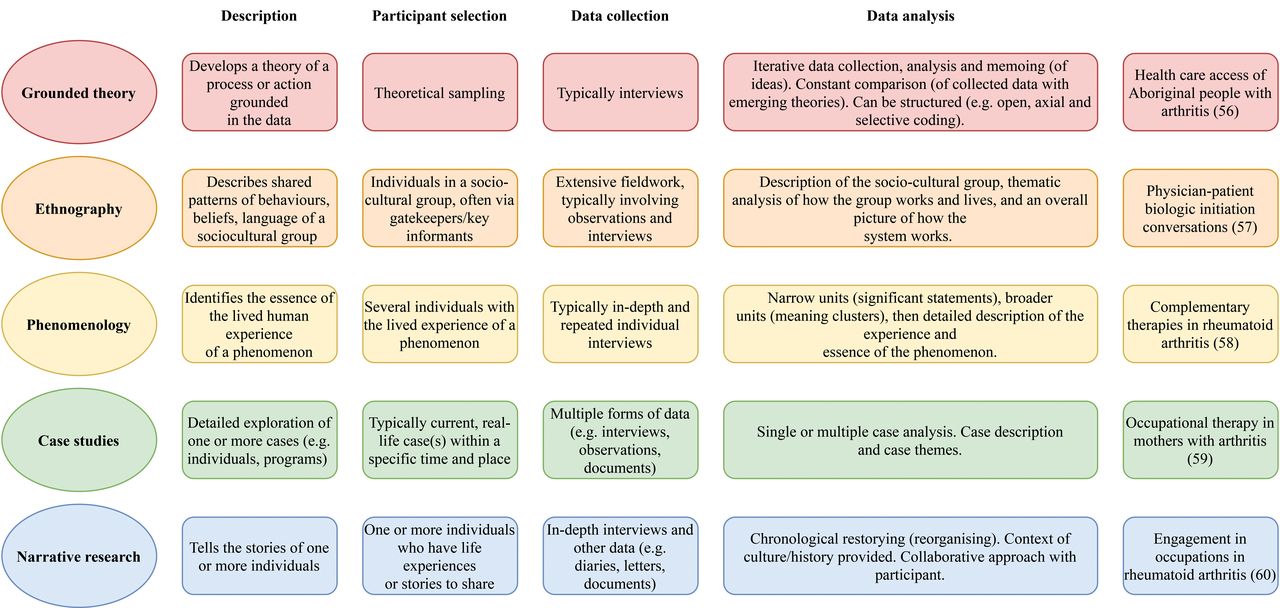
Qualitative research is inherently subjective, as the purpose is to elicit opinions and understand human behavior. The data are co-constructed between the researcher and participants. Theory may be used to inform the design and approach of the study. For some approaches, including grounded theory, the study is designed to generate theory from the findings. There are several specific approaches (i.e., strategies of inquiry, theoretical frameworks) that are used as a basis of conducting qualitative research45,46. These approaches can guide the procedures for participant selection, data collection, and analysis. Although many approaches exist, 5 of the most common approaches in health research47 are grounded theory48, ethnography49,50, phenomenology51,52,53, case studies54, and narrative research55. The differences in these approaches are summarized in Figure 1 with illustrative examples of qualitative research in rheumatology56,57,58,59,60. General characteristics of participant selection, data collection, and data analysis that can apply to several qualitative approaches are described below. Researchers may design their study based on a single specific qualitative approach, or not specify a single approach but still use procedures that may be encountered within multiple approaches45. Qualitative methods can also be used as part of mixed methods research and is discussed below.
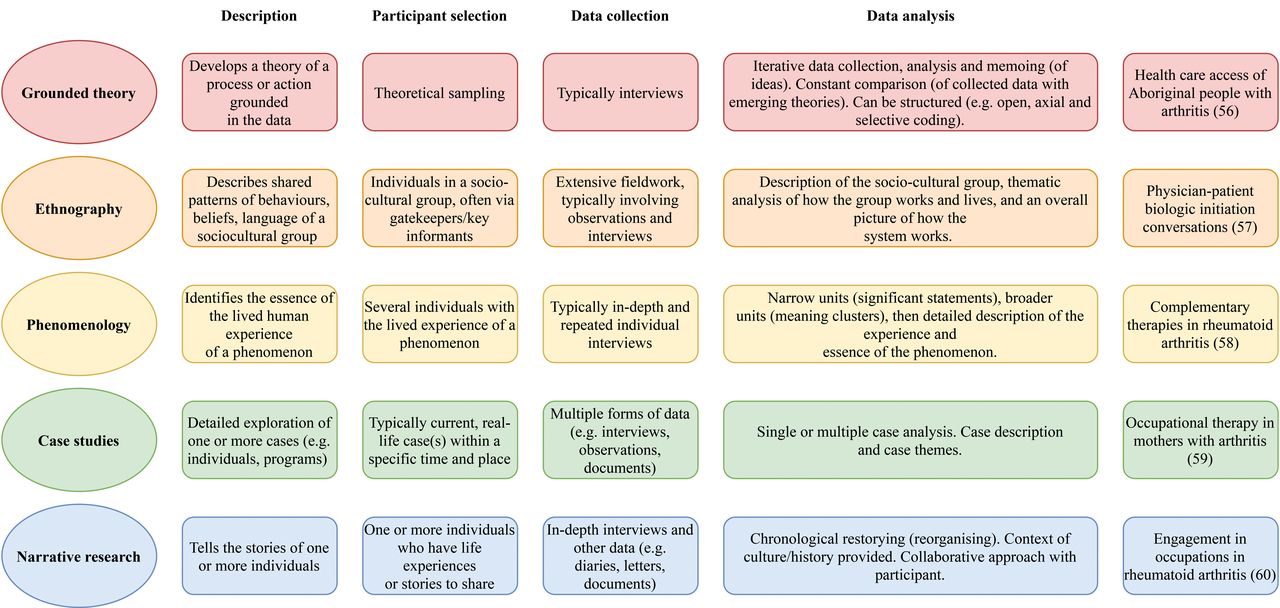
Five key qualitative approaches used in health research.
Participant selection. Qualitative research typically involves an in-depth inquiry within a selected population. Purposive sampling is often used and involves selecting participants who are relevant to the research question with the aim of including a diversity of relevant perspectives8. Other sampling strategies include snowballing, which requires participants to identify other potential participants61. This approach may be useful for including individuals who are hard to access, or those with specific expertise or divergent opinions. These sampling methods are preferred to convenience sampling, which involves recruiting participants who are the most easily accessible8 (e.g., consecutive patients from a single rheumatology clinic who are willing to participate in the study), because it is less likely to capture a broad range of perspectives.
Sample sizes are guided by the methodological approach, study design, participant population, research question, and available resources. As a guide, semistructured interview studies may have 30–60 participants depending on the amount of data obtained per interview62. In grounded theory, 20–30 participants of each population included in the study are generally reported to be adequate. For phenomenological studies that require interviewing each person multiple times, 6–10 participants may be sufficient62. For focus groups, 6–8 participants are recommended to optimize group interaction, with 3–5 groups for each characteristic of interest (e.g., based on a clinical diagnosis)63. Rather than having prespecified sample sizes, recruitment in qualitative research may cease when saturation is achieved61. This is defined as the point when the collection and analysis of new data no longer elicits new insights.
Data collection. Semistructured interviews and focus groups are commonly used in qualitative health research64. These methods are effective in eliciting individual experiences, preferences, and values to inform clinical practice. Focus groups capitalize on group interaction and allow participants to talk to each other, compare points of view, brainstorm ideas, and can be used to record interpersonal language, culture, and dynamics8,64. The facilitator keeps the group on task, asks probing questions, and encourages the participation of all members of the focus group. Semistructured interviews may be particularly useful when discussing sensitive issues or if participants are concerned about maintaining their confidentiality64. The interview guide includes open-ended questions pertinent to the research questions64. The guide is designed to encourage participants to openly pursue their perspectives in detail. Audio or visual recordings and transcription of interviews and focus groups ensure that data is comprehensively captured for further analysis; these can be complemented by field notes that encapsulate contextual details, nonverbal communication, and interactions within a group setting as well as initial reflections of the qualitative researcher8.
Data may also be collected through observations or documents. Observations are a way of gathering data by systematically watching events and people to study their relationships and routine behaviors, and is frequently applied in studies using ethnographic methodology64. In qualitative health research, this is particularly suited to understand how organizations work or how different members in the healthcare environment interact with each other64. Observations may be covert or overt, and may involve the researcher as a participant or nonparticipant in the environment64. Documents include printed and electronic materials such as diaries, newspaper articles, and organizational and institutional reports. These may be used for historical or policy studies or to evaluate healthcare organizations or programs8,65.
Data analysis. The analysis of qualitative data generally seeks to develop a comprehensive understanding and description of the phenomenon being investigated. The output of qualitative research differs depending on the methodology. For example, thematic analysis will yield themes (patterns of shared meaning that together give a comprehensive picture of the population of interest’s experience)66, ethnographic studies are designed to provide insights into the behaviors and perceptions of a sociocultural group49, phenomenology seeks to describe a phenomenon from the lived experience of individuals67, and grounded theory develops a theory arising from the data48. The processes used in qualitative data analysis involve data reduction (by coding and identifying meaningful sections of the data into labels), data organization (in which codes are collected and sorted), and interpretation (where data are analyzed to understand meaning; codes are categorized and compared; and emerging themes or theories are developed)64. Data analysis should be an iterative process that involves cycles of data collection, analysis, and then resumption of data collection to further explore and challenge emerging themes or theories61.
Qualitative analysis software manages qualitative data and provides efficient methods for storing, organizing, and retrieving qualitative data8. These programs, however, cannot conduct the analysis of the data. Investigators must create their own codes and interpret their data. The interpretive nature of qualitative research inevitably means that the researcher’s background, knowledge, and values can influence the analysis of the data. Several methods can be used to ensure the results accurately reflect the spectrum of the participants’ perspective. These include member checking (sharing preliminary findings with participants to check whether their viewpoints are accurately captured), investigator triangulation (incorporating input from team members in the analysis, especially from different backgrounds), and reflexivity (reflecting on personal experiences and biases using a diary or field notes in relation to the data analysis)8,61.
Combining qualitative and quantitative research methods
A study may also use a mixed methods approach, which is a distinct research methodology where both qualitative and quantitative data are collected. Mixed methods research requires an integrated analysis and the use of rigorous qualitative and quantitative research methods68. Mixed methods research can be classified into 3 core mixed methods designs: convergent (where qualitative and quantitative data are collected and analyzed simultaneously within a single phase)69,70,71; sequential explanatory (where quantitative data is collected first, then qualitative data is collected to explain the quantitative findings)72; and sequential exploratory (where qualitative data is collected, a feature such as a new instrument or intervention is built, and then the feature is tested quantitatively)43,73,74. These core mixed methods designs can be built into more complex research designs such as within a randomized controlled trial41,44,75,76 and is recommended for process evaluations of complex interventions77. Before a trial, qualitative studies could generate hypotheses for examination, help develop and refine the intervention or outcome measures78,79, or enhance patient recruitment80,81. During a trial, qualitative methods could examine whether the intervention was delivered as intended, explore the participants’ responses to the intervention, and understand processes of implementation and change. After a trial, qualitative research can explain reasons for positive or negative findings of the trial, explain variations in effectiveness among trial participants, assess the acceptability of the intervention, or be used to generate further questions or hypotheses82.
Reporting and appraisal of qualitative research
The Enhancing Quality of Transparency of Health Research network recommends using the Consolidated Criteria for Reporting Qualitative Health Research (COREQ) as a guideline for the reporting of qualitative research using interviews and focus groups83. There are several other guides available for the conduct and evaluation of qualitative research8,61,64,83,84,85, including the American Psychological Association’s Journal Article Reporting Standards for Qualitative Research (JARS-Qual)86, which also provides guidance on how to structure a qualitative manuscript. However, the appraisal of qualitative research remains contentious, and there is debate as to how and even whether quality can be legitimately judged64,87,88. There is no empirical evidence to indicate which criteria are critical and how to assess them64,88. The framework by Lincoln and Guba addresses the rigor of qualitative research based on 4 criteria: credibility, confirmability, dependability, and transferability89. The links between the COREQ reporting items and these constructs of rigor are shown in Table 2.
Appraisal of qualitative studies using the Lincoln and Guba framework91 linked to examples from the Consolidated Criteria for Reporting Qualitative Health Research (COREQ) items.
Credibility: Are the findings trustworthy? Credibility refers to having confidence in the truth of the findings (analogous to internal validity in quantitative research)85. Readers may be confident that the findings are credible if the researcher provides a comprehensive and sensible explanation of the data. Comprehensiveness includes ensuring that the true breadth and depth of the phenomena in question were explored. Breadth of data can be captured using purposive sampling, continuing to sample until data saturation, and the final sample size. Depth of data may be gauged by reviewing the question guide and duration of the interview or focus group to determine if they allow the participant to discuss the topic of interest in detail, and whether efforts were made to provide a setting that allows participants to feel comfortable to express their opinions. In addition, triangulation in qualitative research allows a generation of deeper and richer insights. This includes using multiple data sources or data collection methods (data triangulation), or involving multiple researchers (investigator triangulation) in the analysis of data8. Involving multiple researchers in coding can ensure that findings adequately capture all aspects of the data. A clear and insightful presentation of major and minor themes provides a final check on the comprehensiveness of data findings. Member checking allows participants to provide feedback on preliminary findings and ensures that findings are a sensible interpretation of their experiences.
Confirmability: Are the findings linked to the data? Confirmability refers to the extent to which findings of the study are shaped by the data and are not a misinterpretation of findings by the researcher (analogous to objectivity in quantitative research)85. This can be demonstrated by showing raw data such as quotations and linking them to findings from the study. The researcher may describe self-reflexivity, whereby they recognize and reduce any undue influences on their interpretations of the data. Interpretations of data can also be confirmed using multiple data coders, triangulation, and member checking, as noted in relation to credibility85.
Dependability: Is the process auditable? Dependability is analogous to reliability in quantitative research85. Due to the nature of qualitative research, it is not possible for another researcher to fully replicate a qualitative study. However, a rigorous and systematic approach to qualitative research can be followed with a coherent link formed between the findings and methods used in the study. Audio or video recordings, transcription of data, and the use of qualitative software for coding allow transparent and auditable documentation of the research process8. The raw data and analysis can thus be reviewed by others.
Transferability: Are the findings relevant to other contexts? Transferability describes the degree to which themes or concepts from a qualitative study can be applicable to other contexts (analogous to external validity in quantitative research)85. By providing details about participants’ characteristics and study setting in enough detail (termed thick description), readers of qualitative research can determine whether the findings may be applicable to their own setting. In addition, comparing the results of the study with other studies in different populations or to existing theory can also help demonstrate the broader relevance of the study findings.
Conclusion
Qualitative studies have the potential to generate a deep understanding of people’s experiences, motivations, beliefs, goals, expectations, and needs. In rheumatology, evidence from qualitative studies has made a unique and valuable contribution to practice and policy. Qualitative research can be systematic, rigorous, and evaluated using the principles of credibility, confirmability, dependability, and transferability. We suggest that further qualitative research is needed in rheumatology to address evidence gaps regarding patient priorities in the management of rare rheumatic conditions, coordination and integration of care among healthcare professionals, and education about the psychosocial effects of disease. Incorporating insights from qualitative studies into clinical care, policies, and trials can help promote patient-centered care to improve outcomes for patients with rheumatic conditions.
Footnotes
A.T. is supported by a National Health and Medical Research Council Fellowship (ID 1106716). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
- Accepted for publication June 26, 2020.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.
- 91.↵
- 92.
- 93.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.








{kind=link}