Article Text

Abstract
Aims: The aim of this study was to compare the outcomes of radiofrequency thermal ablation (RFTA), percutaneous ethanol injection (PEI), and percutaneous acetic acid injection (PAI) in the treatment of hepatocellular carcinoma (HCC).
Patients and methods: A total of 187 patients with HCCs of 3 cm or less were randomly assigned to RFTA (n = 62), PEI (n = 62), or PAI (n = 63). Tumour recurrence and survival rates were assessed.
Results: One, two, and three year local recurrence rates were 10%, 14%, and 14% in the RFTA group, 16%, 34%, and 34% in the PEI group, and 14%, 31%, and 31% in the PAI group (RFTA v PEI, p = 0.012; RFTA v PAI, p = 0.017). One, two, and three year survival rates were 93%, 81%, and 74% in the RFTA group, 88%, 66%, and 51% in the PEI group, and 90%, 67%, and 53% in the PAI group (RFTA v PEI, p = 0.031; RFTA v PAI, p = 0.038). One, two, and three year cancer free survival rates were 74%, 60%, and 43% in the RFTA group, 70%, 41%, and 21% in the PEI group, and 71%, 43%, and 23% in the PAI group (RFTA v PEI, p = 0.038; RFTA v PAI, p = 0.041). Tumour size, tumour differentiation, and treatment methods (RFTA v PEI and PAI) were significant factors for local recurrence, overall survival, and cancer free survival. Major complications occurred in 4.8% of patients (two with haemothorax, one gastric perforation) in the RFTA group and in none in two other groups (RFTA v PEI and PAI, p = 0.035).
Conclusions: RFTA was superior to PEI and PAI with respect to local recurrence, overall survival, and cancer free survival rates, but RFTA also caused more major complications.
- RFTA, radiofrequency thermal ablation
- PEI, percutaneous ethanol injection
- PAI, percutaneous acetic acid injection
- HCC, hepatocellular carcinoma
- US, ultrasonography
- CT, computed tomography
- PTC, percutaneous transhepatic cholangiogram
- HBV, hepatitis B virus
- RR, risk ratio
- hepatocellular carcinoma
- radiofrequency thermal ablation
- percutaneous ethanol injection
- percutaneous acetic acid injection
- local recurrence
- cancer free survival
Statistics from Altmetric.com
- RFTA, radiofrequency thermal ablation
- PEI, percutaneous ethanol injection
- PAI, percutaneous acetic acid injection
- HCC, hepatocellular carcinoma
- US, ultrasonography
- CT, computed tomography
- PTC, percutaneous transhepatic cholangiogram
- HBV, hepatitis B virus
- RR, risk ratio
- hepatocellular carcinoma
- radiofrequency thermal ablation
- percutaneous ethanol injection
- percutaneous acetic acid injection
- local recurrence
- cancer free survival
A small hepatocellular carcinoma (HCC) can be detected early by regular ultrasound screening and measurement of serum alpha fetoprotein.1 Several treatments are available for the successful treatment of small HCCs. Of these, surgical resection is the treatment of choice for small HCCs with compensated liver function.2,3 However, local intratumoral ablation therapies, including percutaneous ethanol injection (PEI), percutaneous acetic acid injection (PAI), and radiofrequency thermal ablation (RFTA) achieve a tumour ablation rate similar to that of resection.2,11
Of the local ablation therapies, PEI has been extensively used for the past 20 years and has been found to be safe and effective.4–8,12 PAI has been used by several investigators11,13,14 and one investigation reported that PAI was more effective than PEI with respect to lower local recurrence rates and higher survival rates.11 RFTA has been reported to be superior to PEI because of a slightly higher rate of complete tumour necrosis, the need for fewer treatment sessions,8 and a significantly higher local recurrence free survival.9 However, there have been no randomised controlled trials comparing these three treatments in terms of complications, complete tumour necrosis, local tumour recurrence, new tumour recurrence, overall survival, and cancer free survival. This randomised controlled study was therefore conducted to compare the above clinical outcomes of HCC following PEI, PAI, and RFTA.
MATERIALS AND METHODS
Study design and characteristics of the patients
The study was conducted with the approval of the institutional ethics committee. Written informed consent was obtained from each patient and a family member.
The primary end point of the study was local recurrence. Secondary end points were overall survival and cancer free survival. At the time of planning this study, local recurrence rate after PEI was reported to be 10.5–26%,6,7 after PAI 13%,11 and after RFTA 3.6%.15 Based on the assumption that the local HCC recurrence rate would be 20% or more in the PEI group, we calculated that approximately 50–60 patients would be required in each group to achieve a power of 0.80 and a significance level of 0.05 to assess differences across the three groups. However, it was decided to prematurely terminate the study if there was a significant difference in survival rates between the three groups by carrying out an interim analysis every three months.
Enrolment criteria were: (a) adult patients with 1–3 HCCs measuring ⩽3 cm in diameter each, (b) HCC located at least 1 cm away from the hepatic hilum or gall bladder, (c) absence of vascular invasion or extrahepatic metastasis, (d) liver cirrhosis classified as Child-Pugh class A or B, (e) prothrombin time three seconds less than that of control values, (f) platelet count greater than 50 000/mm3, and (g) no previous treatment for HCC. Exclusion criteria were patients with Child-Pugh class C, previous HCC treatment, and tumour located within 1 cm of the liver hilum or common bile duct. Chang-Gung Memorial Hospital, Taipei and LinKuo, is a teaching hospital with a total of 3000 beds, and 185 of these were available for patients from the outpatient clinic of 35 attending physicians belonging to the Department of Hepatogastroenterolgy, including the Liver Research Unit. According to our computer files, on average, 1200 naïve HCC patients visited our hospital annually between 2000 and 2003. Between April 2000 and June 2002, 337 cirrhotic patients with HCCs <3 cm were encountered in our unit for percutaneous tumour ablation. Of these, 36 patients refused randomisation and 114 patients with HCCs <3 cm were enrolled into another randomised controlled trial comparing RFTA, conventional PEI, and high dose PEI.16 The remaining 187 patients were randomised to receive RFTA (62 patients), PEI (62 patients), or PAI (63 patients) during alternative weeks between April 2000 and April 2002 and then every week between May 2002 and June 2002. Randomisation of treatments was generated by a computer randomisation list that was not available to the treating physician. HCC was diagnosed by pathological or cytological studies of all tumours. Tumour diameters were determined as the largest dimension measured by ultrasonography (US). The number of tumours and absence of vascular invasion were determined by US, colour Doppler US, and dynamic helical computed tomography (CT) imaging. Table 1 lists the clinical baseline parameters. There were no significant differences between the three groups for any of the parameters.
Clinical characteristics in the radiofrequency thermal ablation (RFTA), percutaneous ethanol injection (PEI), and percutaneous acetic acid injection (PAI) groups
Conventional liver biochemical tests, prothrombin time, and complete blood cell counts were measured before treatment. Three phase helical CT imaging was used to detect any enhancement of the tumour.
Percutaneous ethanol injection (PEI)
The first session of PEI was performed one day after CT arterioportography. PEI was performed at the outpatient clinic if there were no severe adverse effects after the first PEI during hospitalisation. PEI was performed as described previously.4,6–8,18 After local anaesthesia, a 22 gauge percutaneous transhepatic cholangiogram (PTC) needle was introduced into the tumour under ultrasound guidance. Absolute (99.5%) ethanol was injected at a dose of 2–10 ml per session. Total volume was approximated using the modified equation
V (ml) = 4/3 × π (γ+1)3
where γ represents the radius of the tumour in centimetres.6,11 The procedure was repeated twice weekly until the hyperechoic change of the tumour was complete, or for up to six sessions per tumour per course, with a maximum of 12 sessions of treatment per tumour.8,17
Percutaneous acetic acid injection (PAI)
The first session of PAI was performed one day after CT arterioportography. PAI was performed at the outpatient clinic if there were no severe adverse effects after the first PAI during hospitalisation. PAI was performed as described previously.11,14 After local anaesthesia, 1–3 ml of 50% acetic acid were injected using a 15–20 cm long 22 gauge PTC needle under ultrasound guidance. Total volume was approximated using a similar equation to that of PEI but with one third of the volume of the ethanol injection.11 The procedure was repeated and ended as for PEI.
Radiofrequency thermal ablation (RFTA)
RFTA was performed as described previously.15,18 After intravenous analgesia and sedatives, as well as local anaesthesia, a 12 cm or 15 cm long 15 gauge LeVeen electrode was introduced into the tumour under US guidance. The 10 hooks of the electrode were then deployed into the tissue encompassing a diameter of 2–3.5 cm and the electrode was connected to an RF generator (RF 2000; RadioTherapeutics, Sunnyvale, California, USA). RFTA was performed using either the manufacturer’s standard algorithm or an interactive algorithm. The standard algorithm was performed with a gradual increase in power until either the power roll off was achieved or 15 minutes of treatment time had elapsed. RF energy was then applied in a second phase until either a second roll off was achieved or 10 minutes of treatment had elapsed. The beginning and end of the interactive algorithm was identical to the standard algorithm but the electrode’s array was partially retracted or fully deployed depending on the change in impedance during the procedure.20 The electrode was repositioned as required to encompass large target tumours and mimic a surgical margin of 1 cm for the target tumour. The procedure was repeated two weeks later until hypoattenuation of the tumour on CT scan was achieved, or for up to two courses, two weeks apart, per tumour.8
Assessing the effect of RFTA, PEI, and PAI
The immediate effects of ablation were assessed using helical CT performed two weeks after treatment. Helical CT was performed using a Prospeed plus system (General Electric Medical System, Yokogawa, Japan). If foci of nodular enhancement were noted in the treated tumour under CT, then PEI, PAI, and an RFTA booster were given as part of another course of treatment. The CT scan was repeated two weeks after the booster treatment. Complete tumour necrosis was defined as persistent hypoattenuation of the tumour on CT scan four months after the most recent ablation therapy.8,20 Serum alpha fetoprotein was also measured two weeks after ablation. When baseline levels of serum alpha fetoprotein were abnormal they was rechecked every month.
Long term outcome was assessed in terms of complications, local recurrence, new HCC recurrence, overall survival, and cancer free survival. Major complications were defined as those that if left untreated might threaten the patient’s life, lead to substantial morbidity and disability, or result in hospital admission or a substantially lengthened hospital stay.21 Follow up examinations included monitoring serum alpha fetoprotein levels, and US and helical CT every two to three months periodically. Follow up ended on 31 January 2004. Local recurrence of HCC (equivalent to persistence of the original target tumour) was defined as the presence of an enhanced tumour on CT, corresponding to the initial target tumour. New occurrence of HCC was defined as the development of an enhanced tumour on CT in a different segment from that of the original tumour.
Statistical analysis
The Student’s t test was performed to compare differences between the PEI, PAI, and RFTA groups. The χ2 or Fisher’s exact test was used to compare proportions between the three groups. Local recurrence, new recurrence, overall survival, and cancer free survival were estimated using the Kaplan-Meier method, and differences between groups were compared using the log rank test. Multiple comparisons were made when the three groups were involved. Univariate and multivariate analysis with age (>60 v ⩽60 years), sex, Child-Pugh grade (A v B), hepatitis B virus (HBV) related versus non-HBV related underlying liver disease, two or three tumours versus single tumour, size of tumour (>2 cm v ⩽2 cm), tumour stain on angiography, Edmondson’s grade (III, IV v I, II), serum alpha fetoprotein level (⩾200 v <200 ng/ml), platelet count (⩽60 000 v >60 000/mm3), and treatment (RFTA v PEI or PAI) were performed using Cox’s regression model with proportional hazards. A p value of less than 0.05 was considered to be statistically significant.
RESULTS
Adverse effects
Severe pain was experienced by one patient treated with PEI, three patients treated with PAI, and three patients treated with RFTA, which required analgesia. Transient pleural effusion was encountered in three patients following RFTA, two of whom developed haemothorax and required chest tube drainage; these patients subsequently recovered. Gastric injury with bleeding and perforation of the gastric fundus was evident in one patient 10 days after RFTA. This patient underwent gastric repair during operation and subsequently recovered. The major complication rate was 4.8% (3/62 patients, including two patients with haemothorax and one with gastric bleeding and perforation) in the RFTA group and 0% of 125 patients in the PEI and PAI groups (RFTA v PEI and PAI; p = 0.035). No other severe adverse effects were observed.
Complete tumour necrosis
Of 187 patients, three tumours in two patients in the RFTA group, nine tumours in seven patients in the PEI group, and six tumours in five patients in the PAI group did not achieve complete tumour necrosis following two courses of therapy and were considered treatment failures, as defined by other investigators.8,17 These 14 patients received additional and alternative therapies. The rate of complete tumour necrosis was 96.1% (75/78 HCC tumours) in the RFTA group, 88.1% (67/76 HCC tumours) in the PEI group, and 92.4% (73/79 HCC tumours) in the PAI group. The number of sessions required to achieve complete tumour necrosis were significantly fewer in the RFTA group than in the PEI or PAI group. Hospitalisation of patients in the PEI group was significantly shorter than that in the PAI or RFTA group (table 2).
Factors in relation to achievement of complete tumour necrosis following radiofrequency thermal ablation (RFTA), percutaneous ethanol injection (PEI), and percutaneous acetic acid injection (PAI)
Ninety eight of 134 patients exhibited elevated baseline alpha fetoprotein levels, and these levels decreased to normal (<20 ng/ml) within 4.5 months after therapy. For 53 patients with normal baseline alpha fetoprotein concentrations, levels remained normal in 48, six months after therapy. Fifty seven of 98 patients with normalisation of alpha fetoprotein levels after therapy experienced another rise in alpha fetoprotein levels when either local or new HCC recurrence was detected.
Local and new HCC recurrence
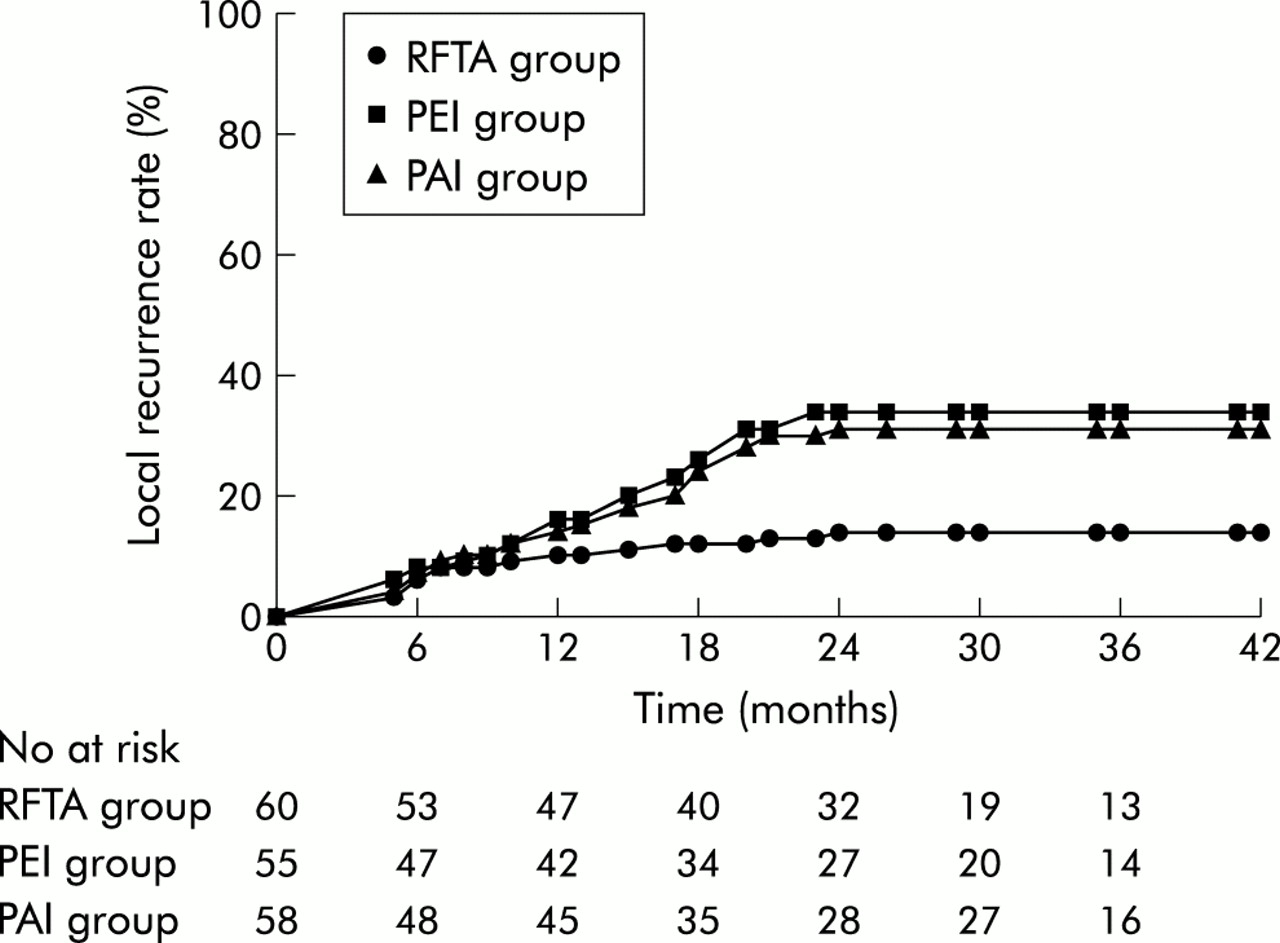
After a median of 35 months (mean 26.3 (SD 12.7); range 4–44) of follow up, two patients in the RFTA group, two in the PEI group, and three in the PAI group were lost to follow up due to HCC recurrence; these patients opted for Chinese herbal treatments. The local recurrence rate was 13.3% (8/60) in the RFTA group, 34.5% (19/55) in the PEI group, and 29.3% (17/58) in the PAI group. Cumulative local recurrence rates for the main tumour at the end of one, two, and three years were 10%, 14%, and 14% in the RFTA group, 16%, 34%, and 34% in the PEI group, and 14%, 31%, and 31% in the PAI group, respectively. The local recurrence rate was significantly lower in the RFTA group compared with the PEI group (risk ratio (RR) = 0.35 (95% confidence interval (95% CI) 0.21–0.89); p = 0.012) and the PAI group (RR = 0.41 (95% CI 0.23–0.91); p = 0.017) (fig 1). The cumulative local recurrence rate was significantly lower in patients with HCCs smaller than 2 cm compared with those with HCCs larger than 2 cm in each group. The cumulative local recurrence rate in patients with HCCs >2 cm was only significantly lower in the RFTA group compared with the PEI group (RR = 0.19 (95% CI 0.08–0.48); p = 0.009) and the PAI group (RR 0.36 (95% CI 0.25–0.89); p = 0.011) whereas the comparison was not significant in patients with HCCs ⩽2 cm across the three groups (table 3). Multivariate analysis revealed that the only significant factors related to local recurrence were tumour size (>2 cm v ⩽2 cm; p = 0.012), Edmondson’s grade (III, IV v I, II; p = 0.018), and treatment method (RFTA v PEI and PAI; p = 0.021). All patients with local recurrence were treated with the same treatment.
Comparisons of cumulative local recurrence, new recurrence, overall survival, and cancer free survival rates among the radiofrequency thermal ablation (RFTA), percutaneous ethanol injection (PEI), and percutaneous acetic acid injection (PAI) subgroups

Comparison of local recurrence rate for the main tumour in the radiofrequency thermal ablation (RFTA), percutaneous ethanol injection (PEI), and percutaneous acetic acid injection (PAI) groups. Local recurrence rate was significantly lower in the RFTA group compared with the two other groups (RFTA v PEI, p = 0.012; RFTA v PAI, p = 0.017). Differences between the three groups were significant (p = 0.015).
New HCC occurred in 18 patients in the RFTA group, 19 in the PEI group, and 21 in the PAI group. The cumulative new HCC recurrence rates at the end of one, two, and three years were 25%, 37%, and 45% in the RFTA group, 23%, 40%, and 48% in the PEI group, and 21%, 40%, and 46% in the PAI group. No significant difference was found among the three groups. Extrahepatic metastasis to intra-abdominal lymph nodes was found in one patient in the RFTA group. Forty six patients with new HCC recurrences were treated with the same treatment, and the remaining 12 patients were treated with alternative therapies.
Overall survival rate and cancer free survival rate
Ten, 17, and 15 patients in the RFTA, PEI, and PAI groups, respectively, died during follow up. The causes of death included HCC progression in four, hepatic failure in three, oesophageal variceal bleeding in two, and pre-existing uraemia in one patient in the RFTA group; HCC progression in 10, hepatic failure in four, spontaneous bacterial peritonitis and sepsis in one, and oesophageal variceal bleeding in two patients in the PEI group; HCC progression in nine, hepatic failure in five, and oesophageal variceal bleeding in one patient in the PAI group. The overall survival rates at one, two, and three years were 93%, 81%, and 74% in the RFTA group, 88%, 66%, and 51% in the PEI group, and 90%, 67%, and 53% in the PAI group (fig 2). Overall survival rate was higher in the RFTA group compared with the PEI group (RR = 0.42 (95% CI 0.21–0.98); p = 0.031) and PAI (RR = 0.45 (95% CI 0.06–0.58); p = 0.038) groups. No significant difference was seen between the PEI and PAI groups. Multivariate analysis revealed that the only significant factors related to overall survival were tumour size (>2 cm v ⩽2 cm; p = 0.037), Edmondson’s grade (III, IV v I, II; p = 0.031), and treatment method (RFTA v PEI and PAI; p = 0.024).

Comparison of overall survival rate in the radiofrequency thermal ablation (RFTA), percutaneous ethanol injection (PEI), and percutaneous acetic acid injection (PAI) groups. Overall survival rate was significantly higher in the RFTA group compared with two other groups (RFTA v PEI, p = 0.031; RFTA v PAI, p = 0.038). Differences between the three groups were significant (p = 0.033).
Cancer free survival rates at one, two, and three years were 74%, 60%, and 43% in the RFTA group, 70%, 41%, and 21% in the PEI group, and 71%, 43%, and 23% in the PAI group (fig 3). Cancer free survival rate was higher in the RFTA group compared with the PEI group (RR = 0.31 (95% CI 0.18–0.85); p = 0.038) and the PAI group (RR = 0.26 (95% CI 0.13–0.81); p = 0.041). No significant difference was found between the PEI and PAI groups. Multivariate analysis revealed that tumour size (>2 cm v ⩽2 cm; p = 0.041), Edmondson’s grade of tumour (III, IV v I, II; p = 0.036), and treatment method (RFTA v PEI and PAI; p = 0.031) were the only significant independent factors that affected the cancer free survival rate.

{kind=link}
{kind=link}
{kind=link}
Comparison of cancer free survival rate in the radiofrequency thermal ablation (RFTA), percutaneous ethanol injection (PEI), and percutaneous acetic acid injection (PAI) groups. Cancer free survival rate was significantly higher in the RFTA group compared with the two other groups (RFTA v PEI group, p = 0.038; RFTA v PAI, p = 0.041). Differences between the three groups were significant (p = 0.039).
DISCUSSION
The advantages of PEI and PAI are that they are easy to perform and have greater safety and tolerance than RFTA. However, RFTA has the advantage of requiring fewer treatment sessions and yielding a higher rate of complete tumour necrosis and local recurrence free survival at the risk of a higher rate of major complications.8,9 Moreover, there have been no trials comparing all three treatments, which are necessary to determine the incidence of major complications and clinical outcome in a single centre.
RFTA is generally considered a relatively low risk procedure.21 In this study, although the incidence of major complications was significantly higher in the RFTA group (RFTA v PEI and PAI: 4.8% v 0%; p = 0.035), no RFTA related deaths occurred. The rate (4.8%) of major complications in this study was less than the 13.1% (10) of 76 patients in the study of Curley et al using the same LeVeen electrode and RF generator15 but slightly higher than the 2.4% (56) of 2320 patients (p>0.1), including six deaths, in a multicentre analysis using a cool tip electrode.21
The present results showed a slightly higher rate of complete necrosis in the RFTA group. The rate of complete tumour necrosis between the RFTA and PEI groups after two treatment cycles was similar to that of Livraghi and colleagues8 (90% v 80%) and that of Lencioni and colleagues9 (98.5% v 94.5%).
The local recurrence rate was higher in patients with HCCs larger than 2 cm (table 3). This finding was similar to those in other reports.11,22 The independent factors related to local recurrence were large tumour size (>2 cm) and high Edmondson’s grade of tumour. This result was consistent with that of Komorizono and colleagues.22 A larger tumour usually has a higher rate of local recurrence because it frequently requires multiple overlapping ablations, and targeting of its viable foci is difficult because of lack of clarity of the image obtained between the ablated and non-ablated tumour after repeated ablation is performed under sonography.23 Moreover, a high grade HCC probably has satellite nodules that are further away from the main nodule,24 possibly implying that local recurrence in the same segment can be caused by satellite nodules that may be obscured under sonography. Moreover, a larger tumour is more often manifest with higher differentiation,25 thus having satellite nodules along or above the margin of the tumour which might be obscured during sonography. Despite the wider range (1 cm safety margin) of injections of ethanol or acetic acid herein, the distribution of ethanol or acetic acid might be unpredictable both within the tumour and outside due to interference of the fibrous septum11 and the presence of satellite nodules around the target tumour,24 respectively. Therefore, a 1 cm safety margin can be achieved in patients treated with RFTA but not in patients treated with PEI or PAI. This limitation of the homogenous distribution of ethanol or acetic acid around the safety margin of the target tumour may explain the benefit of lower local recurrence favouring RFTA than PEI or PAI in treating HCCs larger than 2 cm in the present study or in other investigations.11,22
The rates of new HCC recurrence were also similar among the three groups, perhaps because of the similar baseline parameters.
Our results also showed that overall survival was significantly higher in the RFTA group than in the PEI and PAI groups. This finding is different from that of Lencioni and colleagues.9 The reason may be that the observation period was longer in our study (mean follow up 26.3 months in this study compared with 22 months in Lencioni’s study). However, Lencioni’s study also showed a trend towards increased survival in the RFTA group.9 The cause of death was HCC progression in most cases. Therefore, a more effective local treatment such as RFTA can achieve lower HCC recurrence and consequently contributes to better survival.
Cancer free survival reflects local recurrence and new tumour formation elsewhere in the liver. Because lower recurrence was lower in the RFTA group therefore the cancer free survival rate was also lower in RFTA group than in the two other groups in this study. This finding is similar to that of Lencioni and colleagues.9
Although we used an RF generator with a lower power (100 W) and the LeVeen electrode with a small diameter (up to 3.5 cm only), the study still showed a better clinical outcome with RFTA than with PEI or PAI in treating HCCs of 3 cm or less. More recent advances in the RF generator with a higher power (up to 200 W) and RF electrodes with a larger ablation zone (up to 5 cm in diameter) may increase the rate of complete necrosis, local recurrence, and overall survival and cancer free survival when these new devices are used to perform RFTA in small HCCs or even in larger HCCs.
We conclude that RFTA yielded a better outcome with respect to lower local recurrence, higher overall survival, and higher cancer free survival than PEI or PAI in treating HCCs of 3 cm or less. However, RFTA also caused significantly higher major complications than PEI or PAI.
REFERENCES
Footnotes
-
Conflict of interest: None declared.