Article Text

Abstract
Objective To determine whether variation in gastroscopy rates in English general practice populations is associated with inequality in oesophagogastric (OG) cancer outcome.
Design Retrospective observational study of the Hospital Episode Statistics (HES) dataset for England (2006–2008) linked to death registration.
Methods were validated using independent local and national data. General practices with new cases of OG cancer were included. Practices were grouped into tertiles according to standardised elective gastroscopy rate per capita (low, medium or high). Outcome measures for cancer cases were: emergency admission during diagnostic pathway, major surgical resection and mortality at 1 year. Covariates were: age group, gender, comorbidity, general practice average deprivation and patient deprivation.
Results 22 488 incident cases of OG cancer from 6513 general practices were identified. Patients registered with the low tertile group of practices had the lowest rate of major surgery, highest rate of emergency admission and highest mortality. The inequality was widest for the most socioeconomically deprived cases. After adjustment for covariates in logistic regression, the gastroscopy rate (low, medium or high) at the patient's general practice was an independent predictor of emergency admission, major surgery and mortality.
Conclusions There is wide variation in the rate of gastroscopy among general practice populations in England. On average, OG cancer patients belonging to practices with the lowest rates of gastroscopy are at greater risk of poor outcome. These findings suggest that initiatives or current guidelines aimed at limiting the use of gastroscopy may adversely affect cancer outcomes.
- Gastroscopy
- Oesophageal Cancer
- Gastric Cancer
- Primary Care
- Dyspepsia
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
-
Current UK referral guidelines for gastroscopy focus on alarm symptoms although these symptoms have poor sensitivity and specificity for cancer, and may signify advanced disease.
-
Rates of referral for gastroscopy from primary care show wide variation suggesting a spectrum of clinical practice and differing interpretation of guidelines.
-
It is not known whether variation in rates of gastroscopy in general practice populations is associated with inequality in outcomes for OG cancers.
What are the new findings?
-
We confirmed wide variation in per capita rates of elective gastroscopy within general practice populations. The magnitude of variation and pattern of diagnostic findings suggest differing thresholds for referral across primary care.
-
After adjusting for confounders, we showed that OG cancer patients belonging to practices with low rates of gastroscopy were at increased risk of poor outcome for OG cancer.
How might it impact on clinical practice in the foreseeable future?
-
Practices with low rates of gastroscopy should review their current practice, particularly those serving deprived populations. Targeted interventions may be required to increase rates of gastroscopy in populations exposed to inappropriately low rates of investigation.
-
Current dyspepsia referral guidelines may contribute to suboptimal OG cancer outcomes in the UK owing to their emphasis on alarm symptoms.
Introduction
Gastroscopy is the gold standard investigation for identifying serious causes of dyspepsia, although the incidence of major pathology is low and the test is expensive, uncomfortable and not without small risk. In the UK, foregut symptoms account for at least 3% of consultations in primary care.1 However, a typical general practitioner (GP) serving a population of 2000 patients may see only one new case of oesophageal or gastric cancer every 1–2 years.2
Direct access to gastroscopy from primary care was established in England during the 1980s,3 and fast-track access for those with alarm (or ‘red flag’) symptoms was introduced into the National Health Service (NHS) over 10 years ago under the national cancer plan.2 ,4 However, there has been little improvement in detection of curable cancer over this period. Overall, approximately three-quarters of cases of oesophagogastric cancer (OG cancer) are diagnosed at a late and inoperable stage in the UK.5 ,6 The ‘gatekeeper’ role of primary care in deciding which patients are referred for specialist investigation is cited as a potential source of avoidable delay in cancer diagnosis within the NHS and other countries with similar systems.6
Modern dyspepsia referral guidelines focus on alarm (or ‘red flag’) symptoms as key triggers for gastroscopy, and recommend empirical symptomatic treatment and non-invasive Helicobacter pylori testing in those with simple dyspepsia.7 However, the early symptoms of OG cancer may be non-specific, and the traditional alarm symptoms have poor sensitivity or specificity for malignancy.2 ,8 ,9 When alarm symptoms are present in a case of cancer, such clinical features may indicate advanced, incurable disease.10 This has fuelled considerable controversy regarding the role for gastroscopy in the investigation of simple dyspepsia, and in detecting cancer at a treatable stage.4 ,10 ,11 There is limited evidence to suggest that implementation of fast-track services based on current guidelines has promoted earlier cancer diagnosis.12
Given the unresolved questions regarding the value of gastroscopy both in managing dyspepsia and in detecting curable cancer, variation in the threshold for referral, and rates of gastroscopy across primary care is inevitable. Analysis of gastroscopy activity data for Primary Care Trusts (PCT) showed a twofold range across England.13 However, aggregated data for groups of practices may mask wider variation between individual general practice centres.
We wished to test the idea that outcomes for OG cancer patients may be associated with the local rate of gastroscopy in the general practice population. We postulated that general practices with relatively low per capita rates of gastroscopy may be less likely to identify curable cancers, whereas those with higher levels of gastroscopy may increase the chance of earlier diagnosis and curative treatment. The assumption underlying this hypothesis is that variation in gastroscopy activity reflects different referral practice thresholds. Any association between local rates of gastroscopy and outcome of OG cancer should be independent of patient factors, such as age, gender, comorbidity or deprivation.
In this study, we analysed routine NHS datasets to identify all general practices in England with incident cases of oesophageal or gastric cancer, and extracted data on their total elective diagnostic gastroscopy activity and diagnostic profile of investigated patients. We then developed and validated linkage methods to describe outcomes of OG cancer cases. This allowed us to test whether there was an association between cancer outcome and general practice gastroscopy rate after adjustment for covariates.
Methods
Data sources
Hospital episode statistics
The Hospital Episode Statistics (HES) database is an administrative dataset that stores information on all NHS and private patients admitted to NHS hospitals in England. Each care episode contains administrative information (eg, dates of admission and discharge, method of admission), a primary diagnosis and up to 13 secondary diagnoses (coded according to the ICD-10 system), and up to 14 procedure fields coded using OPCS-4 system (Office of Population Censuses and Surveys Classification of Surgical Operations and Procedures 4th revision).14 ,15 The quality of HES data has been validated,16 and this dataset has been used recently to study surgical outcome in OG cancer.17
Death registrations
Deaths were derived through a linkage between HES records and the Office of National Statistics (death registrations), hence, capturing deaths both in and out of hospital.14 ,15
Registered adult patient population for general practices
In England, all residents receiving NHS healthcare are registered with a general practice that comprises one or more family doctors providing primary care services to a defined practice population. Each general practice has an identifier code within HES. Published data are available for the total number of adult patients (≥16 years) registered at each general practice, their gender and age profile for the relevant years.18–20 We assigned each general practice to a deprivation category (deprivation quintiles; 1=most deprived to 5=least deprived). This was based on national ranking of a practice-level average deprivation score based on the Index of Multiple Deprivation (IMD). The practice score represents a weighted average of the IMD scores for each Lower Super Output Area in which a given practice has patient registrations.21
Gastroscopy rates for general practices and diagnostic profile
Using a 2-year download of the HES dataset containing more than 24 million care episodes (2006/2007 and 2007/2008),14 ,15 we extracted all hospital episodes containing a procedure code for elective diagnostic gastroscopy for adult patients (≥16 years) using published procedure codes and definitions.22 ,23 All elective gastroscopy episodes were summed for persons registered at each general practice, and we calculated the average count of elective gastroscopies performed per practice per year. Using the data for practice population demographic profile,18 we calculated an age-adjusted and sex-adjusted rate of gastroscopy for each practice by the indirect standardisation method.24
To study the overall diagnostic profile of patients undergoing elective gastroscopy procedures, we screened diagnostic fields within the episode containing each patient's first gastroscopy procedure. ICD-10 codes recorded at each coding position were assigned to one of six mutually exclusive diagnostic categories using listings of diagnostic codes. Each patient was then allocated to a final diagnostic category based on the most serious’ condition coded: (1) upper gastrointestinal (GI) cancer, (2) major acid-peptic diseases (eg, peptic ulcers or strictures), (3) minor findings (eg, gastritis or hiatus hernia), (4) benign GI neoplasms (eg, polyps or metaplasia), (5) upper GI symptom codes only (eg, heartburn or dyspepsia) and (6) miscellaneous (all other codes).
Extraction of data for incident cases of oesophageal and gastric cancers in England
We developed and then validated linkage methods to extract a patient population of incident (new) cases of oesophageal or gastric cancer from the main HES dataset, selecting only cases with a valid chronological series of care episodes compatible with a new (incident) case of OG cancer undergoing diagnosis and treatment.
First, we identified all patients with one or more episodes containing a diagnostic code for oesophageal or gastric cancer. Using the unique identifier for each cancer case, we then extracted all their care episodes from the main HES dataset and ordered them chronologically. We then developed algorithms to identify episodes that contained key procedure milestones (eg, first diagnostic gastroscopy and major surgical resection) based on OPCS-4 procedure codes.
HES data does not contain a date of diagnosis, and the first episode of care coded with a definitive cancer code is not a reliable starting point for the patient's journey.25 Manual review of the coding sequence for individual cancer cases revealed that the original primary diagnoses recorded at the time of first (index) gastroscopy were often non-specific symptom codes (eg, dysphagia) or non-malignant diagnostic labels that would be compatible with cancer (eg, oesophageal stricture or gastric ulcer). The first appearance of a cancer code for such cases was typically within a few days or weeks of the index diagnostic gastroscopy when the patient attended for another hospital episode (eg, therapeutic gastroscopy or surgery). By selecting cases whose first diagnostic gastroscopy episode occurred within 3 months of the first cancer-coding episode (either as a day-case or during a hospital admission), we extracted a cohort of patients with a sequence of care episodes and diagnostic procedures compatible with a new diagnosis of OG cancer.
Eligibility criteria for general practices included in the study
The study included all general practices in England that satisfied the following entry criteria: (1) data available for mid-year practice population list size and demographics and average deprivation score of registered patients; (2) one or more incident cases of OG cancer identified for the practice from the HES dataset.
Patient demographic, comorbidity and socioeconomic variables
The recorded age of cancer cases at index gastroscopy was grouped into age bands (<55, 55–64, 65–74, 75–84 and ≥85 years). All secondary diagnostic fields were screened for comorbidities using ICD-10 codes from the Charlson index, and a categorical comorbidity variable was assigned to each patient (none, 1 or ≥2 comorbidities) as previously described.14 ,15
Within HES data, each patient episode contains a deprivation variable for the socioeconomic status of the lower super output area of residence at the time of admission. Lower super output areas from the whole of the country (each including about 400 houses) were grouped into quintiles from most deprived to least deprived based on their ranking in the Indices of Multiple Deprivation for England 2007.26 Quintile 1 denotes patients living in the most socioeconomically disadvantaged areas of the country.
Patient outcome variables
Emergency admission during diagnostic pathway
Although emergency admission during the diagnostic pathway may be unavoidable for a minority of presentations of OG cancer (eg, acute GI bleeding), the widespread availability and effective use of elective gastroscopy services should minimise unplanned acute hospitalisation for diagnosis. Emergency admission rates for cancer diagnosis in the UK has been a focus of public concern.27 ,28 We classified admission method for the episode containing the index (first) diagnostic gastroscopy as either elective admission (ie, day-case gastroscopy) or non-elective admission (ie, gastroscopy performed during an unplanned ‘emergency’ hospitalisation). This defined the mode of diagnosis as either elective or emergency using the ADMIMETH variable in HES which identifies categories of unplanned (emergency) admission (codes 21, 22, 23, 24 and 28).14 ,15
Surgery
Surgical intervention for OG cancer was defined on the basis of coding of a major surgical resection compatible with curative intent using a list of previously reported OPCS-4 codes.29
Validation of linkage methods and data outputs
In order to test the reliability of our database inclusions, coding algorithms and linkage methods, we assessed the face validity of the national cancer patient population extracted from HES data by comparing their characteristics and outcomes with independent reports from the National Oesophagogastric Cancer Audit5 and the National Cancer Intelligence Network (NCIN).30 These sources represent the most accurate national data available.
To verify the linkage methodology for determining emergency admission status during the diagnostic pathway, we used a local audit dataset relating to a sample of 143 cases diagnosed at our institution within the same study timeframe. By linking on patient age (±12 months), gender, general practice code and diagnostic gastroscopy date (as obtained from the hospital endoscopy reporting tool) we successfully matched each case with a corresponding case within our extract of HES data for our Trust. In comparison with the hospital clinical records, admission method during the diagnostic pathway (elective or emergency admission) was consistent in 141 cases (98.6%).
Statistical analysis
Statistical analyses were carried out with IBM SPSS V.20.0 (SPSS, New York, USA). Analysis of variance and χ2 tests were used to compare differences in continuous and categorical variables between the three groups of practices. Univariate logistic regression was used to identify factors associated with emergency route of diagnosis, surgical resection rate and all-cause mortality at 1 year. Factors with a significance level of ≤0.1 on univariate analysis were included in the final multivariate regression model. The purpose of multivariate logistic regression analysis was to identify whether membership of the low, middle or high tertile group of practices (gastroscopy volume) was associated with cancer outcome after adjustment for the contribution of other patient variables (age, gender, comorbidity and socioeconomic deprivation).
Results
General practices included in the study, and their rates of diagnostic gastroscopy
Of 8338 English GP practices with available data for population demographics, 8232 practices had patients with coded elective gastroscopy procedures, of which 6513 practices had one or more cases of OG cancer diagnosed during the data period. The 6513 practices eligible for study served a total combined adult population of 39 773 433, and there were 332 867 elective gastroscopies recorded per year in this population. Overall, this gives a crude national per capita activity rate of 8.4 elective gastroscopy procedures per 1000 adults per year in England.
The practices were ranked nationally according to their age-adjusted and sex-adjusted annual gastroscopy rate, and then divided into tertiles (low, medium and high tertiles). Over the 2-year period for capturing total elective gastroscopy activity data, 88.2% of the procedures were unique (ie, ‘first-time’ for individual patient within the 2-year time window). The corresponding figures for each general practice tertile were within 1% of each other (low tertile: 89%; middle tertile: 89%; high tertile 88%). The mean adjusted gastroscopy rate for the high tertile group of practices (12.9 per 1000) was more than 2.5 times (250%) that of practices in the low tertile group (4.4 per 1000). Hence, tertiling of practices by total elective gastroscopy activity was not influenced by differing levels of repeat procedures between the groups. Further sensitivity analyses were undertaken using practice quintiles or absolute gastroscopy rate (see Results).
The characteristics of general practices, according to tertile of gastroscopy rate, are summarised in table 1. The populations served by the tertile groups of practices showed no significant differences with respect to age or gender profile. There was a significant difference in the distribution of practices with respect to the ‘average’ practice-level deprivation variable (quintile)—the low tertile group contained the lowest proportion of ‘most deprived’ practices, whereas the high tertile group contained the highest proportion. Nevertheless, all tertile groups contained practices from every deprivation quintile. Linear regression revealed that only 7.9% of variation in age-sex adjusted practice rates was associated with the practice-level deprivation (adjusted r-square: 0.079), suggesting that most variation in gastroscopy rates is not accounted for by the average deprivation score of the practice population.
Characteristics of 6513 general practices in England grouped into tertiles according to their age-sex standardised rate of diagnostic elective gastroscopy (analysis of Hospital Episode Statistics (HES) data for England 2006–2008)
Diagnostic profile of patients undergoing gastroscopy procedures
The diagnostic profile of individual patients from the 6513 study practices who underwent elective diagnostic gastroscopy during the 2-year period is summarised in table 2, based on first (index) procedures. Upper GI malignancy accounted for only 2.1% of all patients undergoing investigation. Other serious pathologies (eg, peptic ulcers) accounted for a further 11.6% of people undergoing the procedure. The remaining 86.3% of gastroscopies were coded mainly with minor pathologies or symptom codes only.
Characteristics of 587 256 patients undergoing elective gastroscopy procedures from the 6513 general practices included in the study
We postulated that practices with low rates of gastrosopy (low tertile) may be operating more selective referral practices, reserving gastroscopy for older patients or those with more severe symptoms (eg, alarm symptoms) associated with serious disease. Conversely, practitioners at high tertile practices may tend to have a lower threshold for gastroscopy referral. The trends in the data support this idea (table 2). Although there was no difference in the age-sex profile of the practice populations served by the three groups of practices, the mean age of patients undergoing gastroscopy was highest for practices in the low tertile (p<0.001, ANOVA). The proportion of patients with serious disease also increased in the same pattern, with low tertile practices having the highest proportion of serious disease (cancers and major acid-peptic lesions; p<0.001, χ2 test) among patients referred for gastroscopy procedures.
Variation in gastroscopy rates within PCT
During the study period, general practices in England were grouped administratively and geographically into PCT responsible for commissioning services from their local hospitals. For each individual PCT (n=152), we determined the absolute range of adjusted gastroscopy rate for the study practices (lowest to highest rate) and calculated the magnitude of variation across the local PCT range. Of the 152 PCTs in England, variation across the range of gastroscopy rates was less than fivefold in 9 PCTs (5.9%), 5–10-fold in 51 PCTs (33.5%), and more than 10-fold in 92 PCTs (60.5%). This confirms very wide interpractice variation in gastroscopy rates among practices served by the same local hospital endoscopy services.
Validation of the OG cancer patient population extracted from HES
Before exploring factors associated with OG cancer outcomes, we verified at national level that the total case numbers, demographic characteristics and measured outcome variables for the patient cohort were consistent with external, independent analyses of available data for OG cancer in England. In our 2-year data period, we identified 23 521 cancer cases, of which 22 488 belonged to eligible general practices. This equates to 11 761 new cases per year in England. This compares favourably (91%) to an annual figure of 12 957 reported by the NCIN for the whole of England.30 The median age of patients in our study was 73 years, the same figure reported for cases in the National Oesophagogastric Cancer Audit.5
With respect to our patient outcome variables, we found a national rate of major surgical resection of 16.5% for OG cancers overall (15.5% reported by NCIN),29 emergency admission during the diagnostic pathway of 28% (26% reported by the NCIN)28 and 1-year survival rate following index gastroscopy of 40.7% (41.14% reported by the NCIN).30 The close agreement of our data outputs with independent analyses of English cancer data suggests valid methodology.
Characteristics of cancer patients across the tertile groups of general practices
The characteristics of the cancer patients by tertile of general practice gastroscopy rate are summarised in table 3. At the time of index gastroscopy, the average age of cancer patients belonging to practices in the low tertile group was approximately 1 year older than those belonging to high tertile practices. There was no difference with respect to gender or frequency of comorbidities across the three groups of practices. The distribution of patient-level deprivation score for the cancer patients across the three practice tertile groups was in a similar pattern to that seen for the average practice-level deprivation score. Hence, the greatest proportion of socioeconomically disadvantaged cancer patients were in the high tertile group, whereas the greater proportion of least disadvantaged cases belonged to the low tertile group of general practices (table 3).
Characteristics of 22 488 oesophagogastric patients by tertile of general practice gastroscopy volume (analysis of Hospital Episode Statistics (HES) data for England, 2006–2008)
Comparison of crude cancer outcomes across the tertile groups of general practices
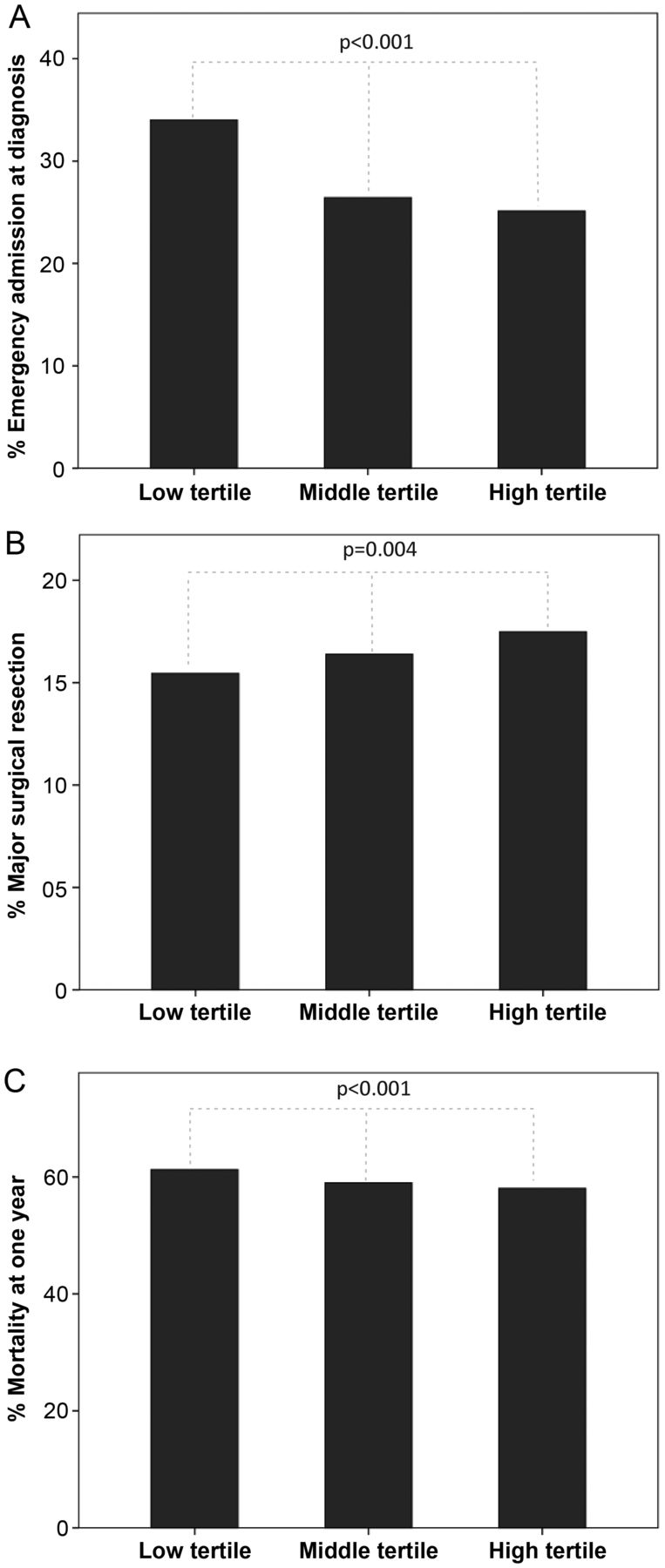
Comparison of crude (unadjusted) outcomes across the three tertiles of practices showed highly significant differences for all three outcome measures (emergency admission during diagnostic pathway, major surgical resection and mortality within 1 year of index gastroscopy) as shown in figure 1. Hence, when aggregated nationally, those patients belonging to the low tertile practices (lowest gastroscopy rates) had poorest cancer outcomes. This is despite the fact that, overall, this group of general practices tended to be serving areas with less social deprivation (table 1) and had a lower proportion of people living in the ‘most deprived’ areas (table 2).
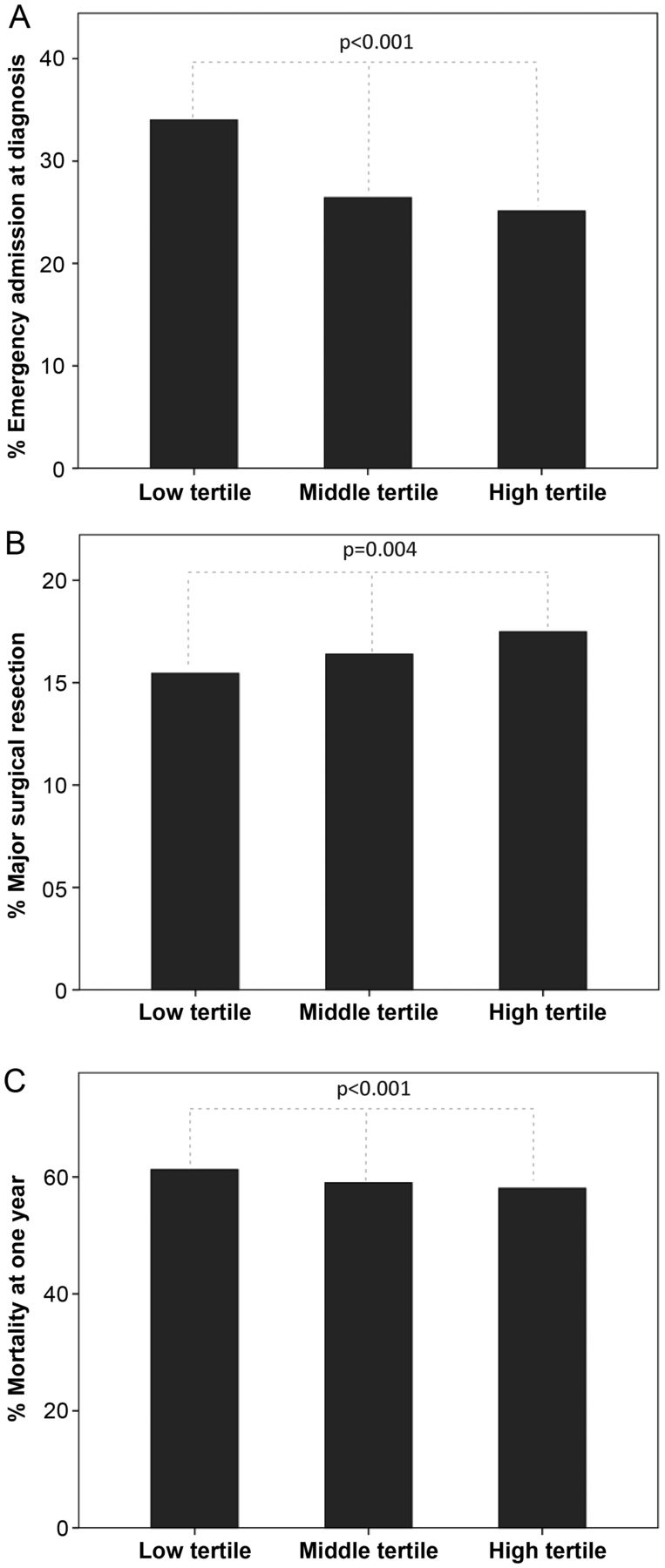
Comparison of crude outcomes for oesophagogastric cancer across the general practice tertile groups (low, middle or high gastroscopy rate per capita). (A) Emergency admission during the diagnostic pathway; (B) Major surgical resection; (C) Mortality at 1 year from index gastroscopy.
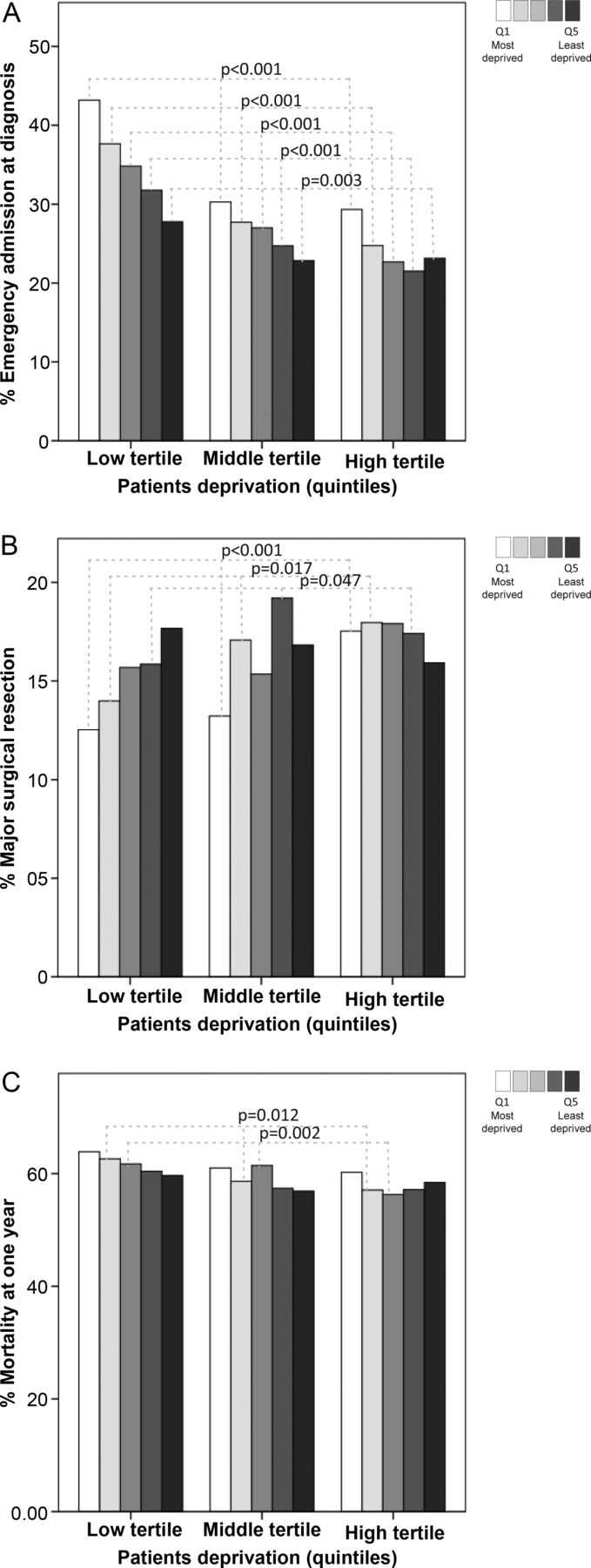
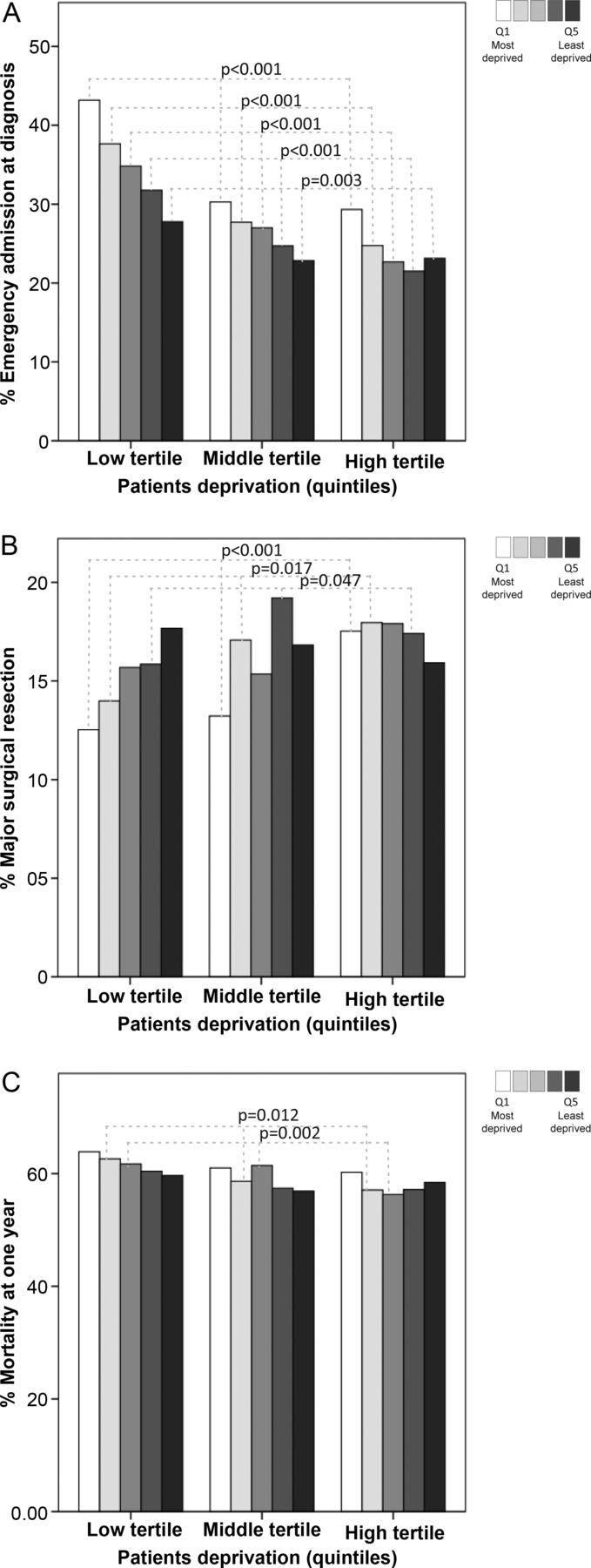
Stratified analysis of crude outcomes according to patient-level (figure 2) deprivation revealed that the imbalance in patient outcome across the three groups of practices was most marked among those who live in the most socioeconomically disadvantaged areas of England (quintile 1). Hence, within these socially disadvantaged areas, the rate of surgery was just 12.5% for those belonging to low tertile practices, 13.2% for those belonging to medium tertile practices and 17.5% for those registered with a high tertile practice (p<0.001; Pearson χ2; figure 2). Similar trends were apparent for the other outcomes.
{kind=link}
{kind=link}
Comparison of crude outcomes for oesophagogastric cancer across the general practice tertile groups: Stratified analysis for patient deprivation quintile. (A) Emergency admission during the diagnostic pathway; (B) Major surgical resection; (C) Mortality at 1 year from index gastroscopy. Quintile 1 refers to patients living in the most socioeconomically deprived areas of England.
Multivariate analysis of factors associated with cancer outcomes
Finally, we performed multiple logistic regression analysis to identify factors associated with each of the three cancer outcomes after adjustment for potentially confounding covariates. This confirmed independent associations between poorer cancer outcomes and advancing age, increased comorbidity and patient deprivation quintile (tables 4⇓–6). As expected, poorer patient deprivation status was associated with worse outcomes. General practice (average) deprivation quintile was an independent predictor only for emergency admission.
Factors associated with emergency admission during the diagnostic pathway in patients with oesophagogastric cancer in England (n=22 488)
Factors associated with chance for major surgical resection in patients with oesophagogastric cancer in England (n=22 488)
Factors associated with 12-month mortality in patients with oesophagogastric cancer in England (n=22 488)
Consistent with our hypothesis, we found that the exposure of interest (general practice gastroscopy rate tertile) was a significant and independent predictor for all three cancer outcome variables. Hence, after adjustment for age, comorbidity and deprivation, there were highly significant associations between cancer outcomes and the general practice rate of gastroscopy. Compared with patients belonging to practices in the highest tertile, those in the lowest gastroscopy rate tertile were 1.73 times as likely to be admitted as an emergency during the diagnostic pathway (table 4), 0.87 times as likely to undergo major surgical resection (table 5), and 1.14 times as likely to be dead within 12 months of gastroscopy (table 6).
Sensitivity analyses
To further confirm the association between the practice gastroscopy rate and cancer outcome, we undertook several additional multivariate analyses using an alternative ‘exposure’ variable to express the gastroscopy rate of the patients’ general practice. First, we substituted the elective gastroscopy rate tertiles for quintiles, reassigning each practice to one of five groups according to their rank order of age-sex-adjusted elective gastroscopy per capita. Second, we reassigned each practice to a quintile based on the gastroscopy rate for people over the age of 55 years. This age cut-off reflects the rate of gastroscopy performed in the ‘higher risk’ population for cancer as identified in guidelines.7 Third, we substituted the practice level categorical variable (tertile or quintile group) for a continuous scale variable reflecting the actual rate of gastroscopy at the practice (expressed as rate per 100 to simplify interpretation of ORs). In all cases, these analyses confirmed the independent association between gastroscopy rate of the general practice population, and all three of the cancer outcomes after adjustment for confounders (table 7).
Sensitivity analyses confirming association between general practice elective gastroscopy rates and emergency route of diagnosis, major surgical resection and death at 12 month for 22 488 cases of oesophagogastric cancer
Discussion
We developed and validated methods for analysing routinely collected NHS data in order to test a hypothesis that variation in rates of gastroscopy at the level of general practice populations is associated with outcome of oesophageal and gastric cancers. To our knowledge, this is the first study examining the association between primary care gastroscopy rates and cancer outcome, albeit the need for research in this area has been highlighted.31
As expected, we found wide variability in per capita rates of gastroscopy at the level of general practice populations. Although practices serving populations in more deprived areas were more likely to have higher rates of gastroscopy, there was no simple relationship between gastroscopy rates and socioeconomic status, and most variation appears unexplained by this factor. Most parts of England showed wide local variation in gastroscopy rates between practices belonging to the same PCT where services are provided by the same hospitals. This makes inequality in access to hospital-based diagnostic services an unlikely factor driving such small-area variations. The availability of direct access gastroscopy is long-established in England3 and the ‘two-week rule’ had mandated the nationwide availability of fast-track gastroscopy more than 5 years prior to the data period for this study.2 ,4
Further research is required to understand the causes for practice-level variation in gastroscopy rates across general practice. However, variation in thresholds for gastroscopy referral is an entirely expected phenomenon given the controversy that exists regarding the correct place for this investigation in the management of upper GI symptoms.4 ,10 ,11 Practices with high rates of gastroscopy had the lowest proportion of serious pathology which would suggest a tendency for lower threshold for investigation.
Consistent with our main hypothesis, we found that cancer outcomes were significantly different for patients belonging to practices with low, medium or high gastroscopy rates. After adjusting for confounding variables, we found that patients diagnosed from a practice within the lowest tertile of gastroscopy rate were significantly less likely to undergo major surgery than those from a practice in the highest tertile. Inequality in outcome was most divergent for cancer patients from the lowest deprivation category. Similar trends for inequality in the rate of emergency admission and all-cause mortality within a year of gastroscopy were apparent. These data provide strong evidence for an independent association between OG cancer outcomes and gastroscopy rates at the local practice level. It is interesting to note that across the tertiles of practices (low through medium to high), there is a very small but significant trend for lower mean age of cancer patients at the time of index gastroscopy—this would be consistent with a trend towards earlier diagnosis in areas exposed to higher rates of gastroscopy.
This does not imply that individual general practices with low or high rates of gastroscopy are exhibiting poor or good practice, nor that low rates are always associated with worse outcomes. It is not possible from routine data to judge whether the level of gastroscopy at an individual practice is ‘appropriately’ low or high. We have shown that practices with low rates of gastroscopy tended to have a higher ‘diagnostic yield’ of serious pathology which would be consistent with a more restrictive approach, and may even reflect closer adherence to referral guidelines.7 However, our study suggests that populations exposed to lower rates of investigation appear, on average, to experience worse cancer outcomes. It is particularly concerning that patients belonging to the most disadvantaged socioeconomic category have the greatest inequality in cancer outcomes with respect to practice gastroscopy rates.
As expected, socioeconomic deprivation was found to be an independent predictor of poor cancer outcomes for OG tumours—this phenomenon has been described for a range of cancers.32–34 In the present study, general practices belonging to the low tertile for gastroscopy rate were, on average, serving more affluent populations, and had the lowest proportion of cancer patients from the most disadvantaged areas. Hence, the inferior outcomes for this group of ‘low-referring’ practices, overall, cannot be explained by a confounding influence of deprivation. Our stratified analyses for deprivation illustrate a potential reason for this paradox—socially disadvantaged patients who are registered with a low referring practice have particularly poor outcomes—the worst in the country. This suggests that a ‘low’ gastroscopy rate is a potential indicator that might be used to identify practices where doctors may wish to review their referral policies, particularly in more deprived areas, where practice gastroscopy rates tend to be higher.
Strengths of our study include the application of clinically developed algorithms to extract and analyse the entire chronological sequence of coded care episodes for each cancer patient (thereby capturing key milestones in the patient's journey), our verification of the validity of the linkage techniques by direct comparison to local patient-level audit, and the successful validation of the patient population and outcome variables against independent external sources of national data for OG cancer in England. Hence, this was not simply a top-down analysis of HES data, and we took several validation steps to confirm the methodology, minimise the risk of data errors and check the clinical face validity of the outputs. This allowed us to test our hypothesis on national scale data with the benefit of large numbers. Furthermore, we undertook extensive sensitivity analyses using a range of approaches to quantifying the exposure of interest and found the findings to be robust.
Weaknesses of the research relate to the generic concern regarding the completeness, precision and depth of routine administrative coding.35–37 We applied transparent inclusion/exclusion criteria and validation steps to limit the impact of coding error and tested our hypothesis against three outcome variables. Data issues are inevitable, but are unlikely to have systematically biased the results in favour of the hypothesis. Our study is focussed on pooling data for both oesophageal and gastric cancers which share common symptoms and guidelines—separate analysis of different subgroups of OG cancers based on anatomical location (or histology) is not possible within routine coding, since many cases were coded with non-specific coding options. However, a distinction between tumour sites was not relevant to the primary study question.
We did not adjust for possible variation between hospitals in cancer treatment outcome, as this was not a likely confounder given our study design and the selected outcome measures. We aggregated practices into groups on the basis of referral rate for gastroscopy within the general practice population, and tested a range of gastroscopy measures in sensitivity analysis. By showing very wide variation in gastroscopy rates within each PCT, we confirm that practices sharing the same hospitals exhibit a wide spectrum of referral practice. Furthermore, rates of emergency admission or chance of surgical resection are surrogate markers of early diagnosis, and are most relevant to primary care diagnostic pathways rather than subsequent hospital treatment. We note recent data suggesting that postsurgical mortality for operable OG cancer cases varies between hospital institutions in the UK17 but we do not believe this is a credible source of bias in the present study.
Delay in seeking medical attention after symptom onset is a potential factor in late-stage cancer diagnosis.6 ,8 This relates partly to the inherent biology and anatomical location of these tumours—a factor common to all patients, and so not a confounding influence per se in the present study. A variety of socioeconomic characteristics has been associated with care-seeking behaviour (patient delay) in primary care,38 but our analysis adjusts for age, gender and socioeconomic status. We acknowledge a role for patient behavioural factors in determining consultation, and hence, gastroscopy referral. However, such individual factors are unlikely to operate systematically within one general practice population, but not within neighbouring populations, and produce the magnitude of variation we observe within individual PCTs. Evidence from the first English national audit of cancer diagnosis in primary care suggests that ‘primary care’ delay is important in OG cancer—between 20% and 25% of OG cancer cases had three or more consultations with their GP before referral, and only approximately 50% were referred through urgent (fast-track) pathways.39
There are over 13.6 million people served by low tertile practices. If this entire population experienced the same average gastroscopy rate as the middle tertile group (8.1 per 1000), we estimate this would require 49 301 additional procedures. Assuming a day-case gastroscopy cost of £43140 this amounts to £21 325 250. If this increase in diagnostic activity resulted in the same surgical resection rate as experienced by the middle tertile group, this implies a 0.95% absolute increase (15.44% to 16.39%) or an extra 59 surgical candidates from low tertile practices (0.95% of 6196 patients). This suggests a cost of over £360 000 per additional potential surgical cure.
Published median survival times for unresectable OG cancers are approximately 6–9 months,41 whereas typical survival figures reported after radical surgery are 27–38 months.42 ,43 Thus, we estimate that diagnosis at an operable stage may extend life by 18–32 months on average (around 2.5 years). This puts the crude cost per life-year saved for our hypothetical scenario at around £140 000. Alternatively, it is known that only about a fifth of surgical cases achieve 5-year survival and potential long-term cure5—this equates to just 12 lives saved of the 59 extra surgical cases at a cost of £21.3 million.
This crude calculation relies on simplistic assumptions, and a formal economic analysis would be required to model the full stream of potential costs and benefits arising from specific interventions to influence gastroscopy access. Nevertheless, our estimate suggests that a simple strategy to encourage a generalised increase in gastroscopy across all populations served by the ‘low tertile’ practices looks costly compared with alternative healthcare investments. Scarce resources might be deployed more cost-effectively within gastroenterology by increasing rates of other tests, such as colonoscopy. Economic models exploring the cost-effectiveness of a range of colonoscopy-based screening strategies for colorectal cancer have suggested a cost per life-year saved below a threshold of US$40 000 (£25 000).44
In practice, a range of alternative strategies might address current inequalities in OC cancer outcome, but at lower opportunity costs. We favour more targeted locally led intervention to enable GPs to identify whether their gastroscopy rates are low in relation to local norms (ie, ‘local outliers’), particularly in socioeconomically disadvantaged areas, with a focus on increasing access to gastroscopy for older subjects at risk of cancer. Costs could be offset by simultaneous efforts to encourage reductions in gastroscopy among younger dyspeptics where non-invasive strategies are appropriate,7 targeting practices at the high end of the referral volume continuum. The local generation and sharing of practice-level comparative data on gastroscopy could allow commissioners, endoscopy units and GPs to work together to reduce inequalities.
In a climate of cost containment in the UK healthcare system, there is an inevitable and legitimate focus on identifying and constraining ‘excessive’ use of expensive secondary care investigations. Local initiatives aimed at driving down gastroscopy activity may well avoid unnecessary investigations for younger patients with benign disease without compromising clinical outcome. However, we believe that there is a pressing need to focus on both ends of the referral volume spectrum. We have shown that practices with the lowest rates of gastroscopy tend to achieve poorest outcomes for OG cancer, particularly among those living in the most socially disadvantaged areas. Our findings should stimulate research to establish the costs and benefits of programmes designed to encourage targeted increases in gastroscopy rates in selected local populations. Despite national cancer guidelines and widespread provision of fast-track gastroscopy services in England, there are clearly persisting inequalities. If the situation is to improve, current referral guidelines and strategies to support compliance require urgent attention.
Acknowledgments
We thank the Information Centre for Health & Social Care for making the HES data available for analysis, providing the linkage to the death registry (Office of National Statistics) and providing advice and support during the project.
References
Footnotes
-
Contributors MS undertook the data extraction, linkages and data analysis, contributed to study design and assisted in drafting the manuscript. KB contributed the study conception and design, directed and supervised the analysis and drafted the manuscript. MGP contributed to study design, data analysis, supervision of the project and drafting the manuscript. ET was responsible for data management and advised on extraction and linkage methodologies. GP extracted hospital audit data for the local validation step, supervised by NS. NS, NK and RPS contributed to the clinical steering group for the study. MR advised on the statistical analyses and reviewed the manuscript. All authors read and approved the final manuscript.
-
Funding This work forms part of a project funded originally by the UK Information Centre for Health & Social Care (‘Engaging Clinicians in their NHS data’). MS was funded by a Libyan Educational Scholarship.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.