Article Text

Abstract
Objective To elucidate the association between antiviral therapy and extrahepatic outcomes in individuals infected with HCV.
Methods This nationwide cohort study screened 293 480 Taiwanese residents with HCV infection and excluded those with substantial comorbidity. A total of 12 384 eligible patients who had received pegylated interferon plus ribavirin between 1 October 2003 and 31 December 2010 were enrolled in the treated cohort; they were matched 1 : 2 with 24 768 untreated controls in the propensity score and post-diagnosis treatment-free period. The incidences of end-stage renal disease (ESRD), acute coronary syndrome (ACS), ischaemic stroke and catastrophic autoimmune diseases were calculated after adjustment for competing mortality.
Results The treated and untreated cohorts were followed up for a mean (±SD) duration of 3.3 (±2.5) and 3.2 (±2.4) years, respectively, until 31 December 2011. The calculated 8-year cumulative incidences of ESRD, ACS, ischaemic stroke and autoimmune catastrophes between treated and untreated patients were 0.15% vs 1.32% (p<0.001), 2.21% vs 2.96% (p=0.027), 1.31% vs 1.76% (p=0.001) and 0.57% vs 0.49% (p=0.816), respectively. Multivariate-adjusted Cox regression revealed that antiviral treatment was associated with lower risks of ESRD (HR 0.15; 95% CI 0.07 to 0.31; p<0.001), ACS (HR 0.77; 95% CI 0.62 to 0.97; p=0.026) and ischaemic stroke (HR 0.62; 95% CI 0.46 to 0.83; p=0.001), but unrelated to autoimmune catastrophes. These favourable associations were invalid in incompletely treated patients with duration <16 weeks.
Conclusions Antiviral treatment for HCV is associated with improved renal and circulatory outcomes, but unrelated to catastrophic autoimmune diseases.
- HEPATITIS C
- ANTIVIRAL THERAPY
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
-
Chronic HCV infection is a multi-faceted disease with various extrahepatic manifestations.
-
Infected individuals are exposed to increased risks of renal, circulatory and autoimmune complications.
-
Although interferon-free therapy is becoming the new paradigm of antiviral treatment, pegylated interferon plus ribavirin remains the first-line regimen that achieves a high eradication rate in many Asian countries.
What are the new findings?
-
Treating HCV with pegylated interferon plus ribavirin is associated with lower risks of end-stage renal disease, acute coronary syndrome and ischaemic stroke.
-
However, the risk is not attenuated in patients receiving incomplete treatment for less than 16 weeks.
-
Use of pegylated interferon plus ribavirin is unrelated to the occurrence of severe autoimmune diseases in patients with HCV infection.
How might it impact on clinical practice in the foreseeable future?
-
By uncovering the extrahepatic effectiveness in renal and circulatory outcomes, our findings are imperative in evaluating the cost-effectiveness of antiviral treatment for HCV and may have important implications in health policy making.
Introduction
HCV infection is a global public health problem, affecting approximately 170 million people around the world.1 It is not only a major aetiology of liver-related morbidity and mortality,2 but also causally associated with a number of extrahepatic manifestations that include cryoglobulinaemia, glomerulonephritis, endothelial dysfunction, insulin resistance and aberrant autoimmunity.3 ,4 A large body of evidence has shown that the risks of liver-unrelated death,5 chronic renal failure,6 ,7 atherosclerotic disease,8–10 cerebral vascular accident11 ,12 and autoimmune disorders13 are significantly higher in HCV-infected patients. Strategies that can effectively attenuate these excessive risks, however, have not been elucidated.
The past two decades have witnessed a tremendous advance in the antiviral therapy for HCV infection. Interferon-free regimens composed of direct acting antiviral agents are now becoming a new paradigm.14 Nevertheless, pegylated interferon (Peg-IFN) plus ribavirin has been widely used as the regimen of choice for a decade,15 and actually brings about excellent therapeutic responses in Asian countries where the favourable IL28B is prevalent.16 For instance, this regimen attains an eradication rate over 70% among treatment-naïve patients in Taiwan.17–19 Empirical data have been accumulating to show that antiviral therapy is associated with risk reduction of hepatic complications.20–22
Extrahepatic effectiveness of antiviral treatment for HCV infection has not been elucidated. Previous studies usually targeted a specific subpopulation of infected individuals. For example, Berenguer and colleagues reported that sustained viral response (SVR) to interferon plus ribavirin was associated with a lower risk of liver-unrelated mortality in patients with HIV co-infection.23 Our recent work demonstrated that antiviral therapy was associated with improved renal and cardiovascular outcomes in patients with diabetes mellitus (DM).24 A comprehensive evaluation from a general population remains unavailable. In order to fill this knowledge gap, this nationwide cohort study analysed healthcare data in the entire Taiwan population for the years 1997–2011 to clarify the association between treatment for HCV and extrahepatic outcomes.
Methods
This is an open cohort study based on the Taiwan National Health Insurance Research Database (NHIRD), which has been prospectively recording claim data of all forms of healthcare service in Taiwan since 1995. By reason of the single-player and compulsory policy, the national health insurance covers nearly the entire 23 million population of this country. In the NHIRD, disease is coded according to the International Classification of Diseases, Revision 9, Clinical Modification (ICD-9-CM). Previous studies have validated the coding accuracy for major diseases, including end-stage renal disease (ESRD), acute coronary syndrome (ACS) and ischaemic stroke.25–27 Diagnosis codes used in this study are listed in the online appendix (supplementary table S1). Furthermore, we used the Registry for Catastrophic Illness Patient Database (RCIPD), a subpart of NHIRD, to ascertain the diagnosis when appropriate. Fulfilment of specified criteria is mandatory and audited meticulously for certification in the RCIPD.28 The Research Ethics Committee of the Taiwan National Health Research Institute permitted data acquisition (EC1010303-E), and the Institutional Review Board of the E-Da Hospital approved the study protocol (EMRP-103–010).
Eligibility criteria for enrolment
First, all residents with a diagnosis of HCV infection from 1 January 1997 to the end of 2011 were screened. Because reimbursement for antiviral therapy necessitated not only documentation of HCV infection but also elevation of serum aminotransferases, we confined the study population to patients with abnormal liver enzymes. Therefore, inclusion required all of the following three criteria: measurement of serum antibody against HCV; diagnosis with a specific ICD-9-CM code (070.41, 070.44, 070.51, 070.54, 070.70, 070.71, V02.62); and prescription of ‘hepatoprotective’ agents (eg, silimarin, liver hydrolysate and choline bitartrate) which indicated elevation of aminotransferases.29 The inclusion criteria ensured all study participants should be entitled for antiviral therapy, and thereby minimised indication bias.
Patients with co-infection of HBV were ineligible. Moreover, enrolled individuals should be free of physical or psychiatric conditions that could contraindicate interferons or ribavirin. Patients were hence excluded if any of the following conditions was present at baseline: age >70 years, catastrophic illness certified in the RCIPD, any chronic renal disorder (ICD-9-CM codes, 580–587), ACS, ischaemic stroke, malignancy, oesophageal or gastric varices, hepatic encephalopathy, hepatorenal syndrome, ascites, and severe psychosis or mood disorder.
Identification of study cohorts according to antiviral treatment
The first measurement of anti-HCV antibody was assumed as the index date of diagnosis in all participants. We identified patients aged >20 years who had received combination therapy with Peg-IFN (α2a or 2b) plus ribavirin as the treated cohort. The insurance programme reimbursed HCV-infected patients for this regimen since 1 October 2003. The treatment duration principally ranged from 16 to 48 weeks but practically varied according to individual conditions. According to the response-guided protocol, premature termination with duration <16 weeks usually results from either intolerance to side effects or failure of early virological response, and indicates a dismal chance of viral clearance. Treated patients were consequently further grouped by whether or not their antiviral treatment was 16 weeks in minimum.
Propensity scores that estimated the probability of treatment were developed using the logistic regression to adjust for the baseline differences between treated and untreated patients. Each treated patient was matched in propensity scores with two controls who never received interferon or ribavirin throughout the study period. The baseline for treated patients was the day when therapy commenced, and that for untreated controls was set to match the period elapsing from diagnosis to treatment in their treated counterparts. The matching process was carried out using the greedy matching technique.30
Definition and ascertainment of outcomes
Enrolees were observed until occurrence of the study outcomes, death or 31 December 2011; whichever came first. They were followed up for four extrahepatic outcomes: ESRD, ACS, ischaemic stroke, and catastrophic autoimmune diseases. The occurrences of ESRD and autoimmune diseases were defined by RCIPD (HV type 4 and 5, respectively). ACS and ischaemic stroke were defined by hospitalisations with the specific disease codes as the primary diagnosis (ICD-9-CM codes: 410–414 for ACS and 433–434 for ischaemic stroke, respectively). Censoring from mortality was regarded as informative, because occurrence of death could compete for the risk of extrahepatic events.
Adjustment for confounding factors
The multivariate-adjusted analyses took into account probable confounding factors that included demographic characteristics, comorbidity, hepatic dysfunction, medication and hospital level. The definition of DM, hyperlipidaemia and hypertension required both their specific ICD-9-CM codes and prescription of disease-defining medications for 90 days or more. The Charlson index represented severity of underlying comorbidity.31 The effect of aspirin and non-steroidal anti-inflammatory drugs was also considered; average consumption of more than one tablet per month defined a user. Furthermore, the hospital level was recognised as a potential confounding source, insomuch as using interferon entailed expertise, and where patients were managed could influence the therapeutic decision and response.
Statistical analysis
The propensity score for antiviral therapy was generated by the logistic regression that was built on baseline features (see online supplementary table S2). Cumulative incidences of outcomes were estimated by the modified Kaplan–Meier method that accounted for death as a competing risk event. Between-group differences of the incidences were analysed by the Gray method.32 After the graph of the log (−log(survival)) versus the log of survival time verified the assumption of proportional hazards, the association was explored in modified Cox proportional hazard models adjusted for multiple covariates in the presence of competing mortality.33 We used the Akaike information criterion to determine the final models. In order to examine potential interaction between treatment effect and confounding factors, multivariable stratified analyses were carried out to elucidate whether there was heterogeneity in the associations among subgroups defined by confounders. SAS V.9.2 was used to manage the dataset, and R software with the “cmprsk_2.1-4” package was used to calculate the cumulative incidence and HR in the competing risk analyses. Calculated results were expressed with the point estimates along with their 95% CIs. All tests were two-sided, with p<0.05 regarded as statistically significant.
Results
Baseline characteristics of the study population
We screened 293 480 individuals diagnosed with HCV infection between 1 January 1997 and 31 December 2011, and excluded 98 974 patients who were either serologically unchecked or co-infected with HBV. The remaining 194 506 patients with HCV mono-infection were evaluated for eligibility, and 46 415 patients were considered eligible. Finally, 12 384 patients were grouped into the treated cohort (figure 1), 11 094 of whom (89.6%) received treatment for 16 weeks or longer. The untreated cohort accordingly comprised 24 768 controls (see online supplementary figure S1). The two study cohorts did not differ at baseline (table 1).
Baseline characteristics of the study cohorts

Flowchart of identification and enrolment of the study subjects. *A patient may fulfil more than one exclusion criteria.
Outcomes between patients with and those without antiviral treatment
The treated and untreated cohorts were followed up for a mean (±SD) duration of 3.3 (±2.5) and 3.2 (±2.4) years, respectively, until death or 31 December 2011 (table 2). The chance of survival was significantly higher in the treated than in the untreated cohort, with 93.28% (95% CI 94.29% to 92.26%) and 84.43% (85.41% to 83.46%) at 8 years (p<0.001), respectively (figure 2). With regard to the extrahepatic outcomes (figure 3), the 8-year cumulative incidences of ESRD (figure 3A), ACS (figure 3B) and ischaemic stroke (figure 3C) were all significantly lower in the treated as compared with the untreated cohort: 0.15% (95% CI 0.04% to 0.26%) vs 1.32% (95% CI 1.01% to 1.64%) for ESRD (p<0.001), 2.21% (95% CI 1.7% to 2.71%) vs 2.96% (95% CI 2.46% to 3.45%) for ACS (p=0.027), and 1.31% (95% CI 0.85% to 1.77%) vs 1.76% (95% CI 1.44% to 2.08%) for ischaemic stroke (p=0.001), respectively. On the other hand, the incidence of autoimmune diseases did not differ between the two cohorts (figure 3D), occurring in 0.57% (95% CI 0.31% to 0.83%) of the treated and 0.49% (95% CI 0.35% to 0.63%) of the untreated patients, respectively (p=0.816).
Event numbers and incidences of the outcomes between the study cohorts
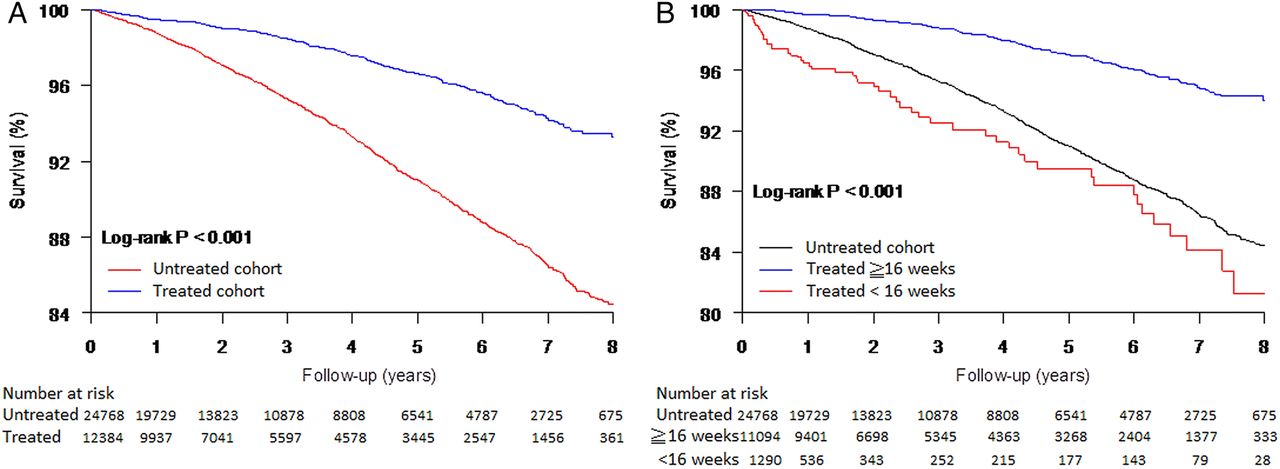
Survival curves of overall mortality in the treated and untreated cohorts (A); the treated cohort was further grouped by therapeutic duration (B).
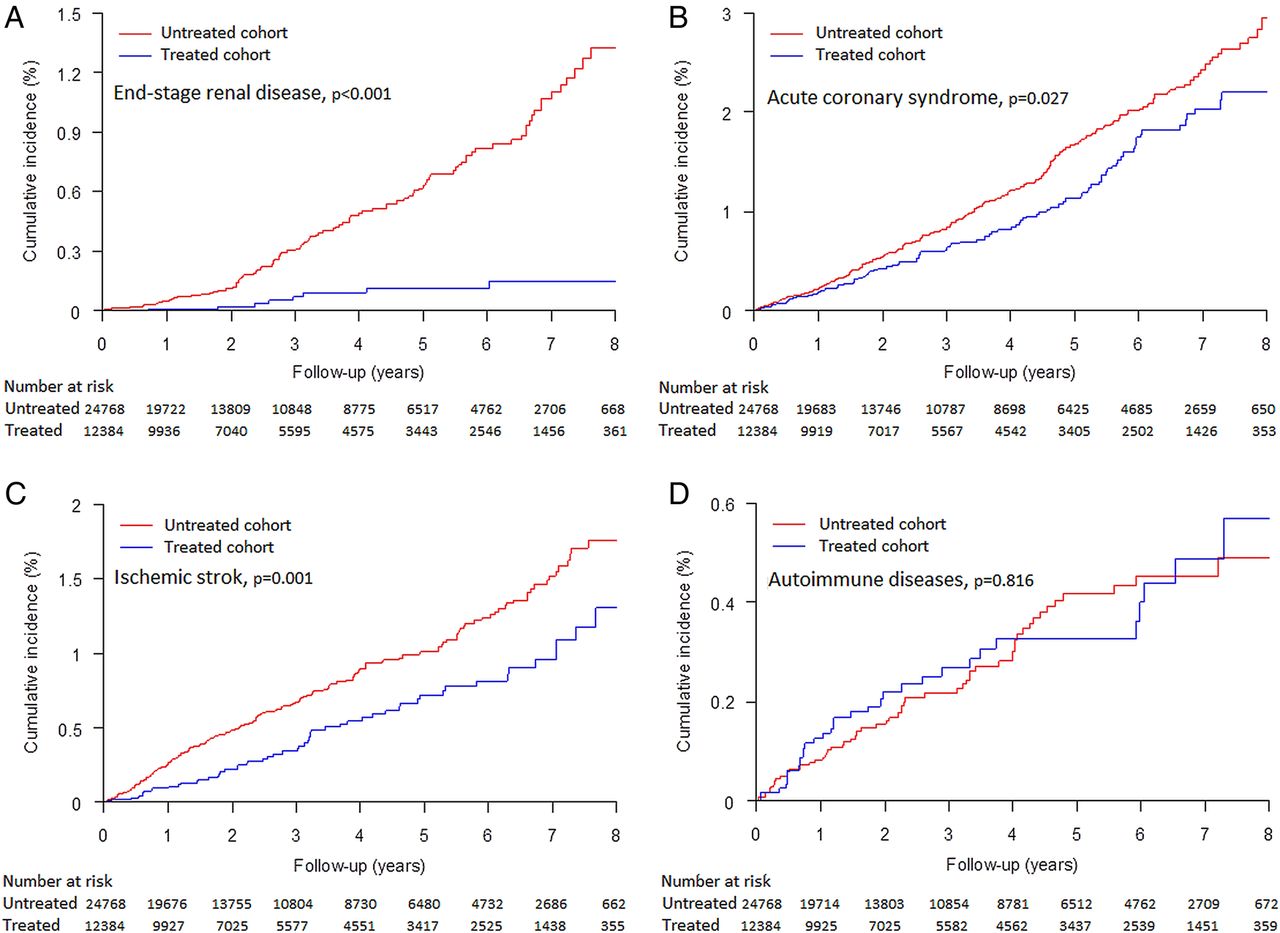
Cumulative incidence of extrahepatic outcomes between the treated and untreated cohorts: end-stage renal disease (A), acute coronary syndrome (B), ischaemic stroke (C), and autoimmune diseases (D); death was managed as a competing cause of risk.
Multivariate-adjusted association of antiviral therapy with extrahepatic outcomes
The association between antiviral therapy and attenuated risks of ESRD, ACS and ischaemic stroke remained significant in the Cox proportional hazard models that were adjusted for multiple covariates (table 3). Treatment with Peg-IFN plus ribavirin was associated with an adjusted HR of 0.15 (95% CI 0.07 to 0.31; p<0.001) for ESRD, 0.77 (95% CI 0.62 to 0.97; p=0.026) for ACS, and 0.62 (95% CI 0.46 to 0.83; p=0.001) for ischaemic stroke, respectively. In contrast, it was not an independent explanatory variable in the model of catastrophic autoimmune disorders.
Multivariate-adjusted Cox proportional hazard models for the outcomes
Stratified analyses according to patient subgroups
The associations between treatment and risk reduction of ESRD, ACS and ischaemic stroke were generally consistent across strata according to age, gender, DM and cirrhosis (figure 4). Of note, ESRD occurred in none of the 10 662 treated patients without DM at baseline. On the other hand, risk reduction of ACS and stroke in non-diabetic patients was not so dramatic. In the analyses stratified by cirrhosis, the point estimates were similar with or without cirrhosis, although the range of 95% CI was wider in the non-cirrhotic subgroup, probably by reason of the sample size. Finally, treatment was unrelated to autoimmune diseases in any specified stratum. Details of the stratified analyses can be found in the online appendix (supplementary figure S2).

Multivariate-adjusted analyses stratified by age, gender, diabetes mellitus (DM), and cirrhosis: end-stage renal disease (A), acute coronary syndrome (B), ischaemic stroke (C), and autoimmune diseases (D). All subgroup analyses were adjusted for confounding factors and the competing mortality.
Influence of incomplete therapy on the association with outcomes
Treated patients who received incomplete therapy for <16 weeks were older, more likely to be female, and had a higher prevalence of hypertension and thyroid disorder (see online supplementary table S3). The incidences of extrahepatic complications in these incompletely treated patients were similar to those who did not receive therapy at all (figure 5). The multivariate-adjusted Cox regression analyses further confirmed that the risks of these extrahepatic events did not differ between incompletely treated patients and the untreated controls (see online supplementary table S4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cumulative incidence of extrahepatic outcomes according to antiviral treatment and therapeutic duration: end-stage renal disease (A), acute coronary syndrome (B), ischaemic stroke (C), and autoimmune diseases (D).
Discussion
The most important finding of this nationwide cohort study is the association between antiviral treatment and risk reduction of renal and circulatory complications in patients with HCV infection. The incidences of ESRD, ACS and ischaemic stroke were significantly lower in patients treated with Peg-IFN plus ribavirin, as compared with their matched untreated controls. These associations remained significant after adjustment for various sources of confounding that included death as a competing cause of risk. The magnitude of risk reduction was approximately 85% in ESRD, 23% in ACS and 38% in ischaemic stroke over the 8-year study period, respectively. We further demonstrated that the risk would not be attenuated if the therapy was incomplete with duration shorter than 16 weeks. On the other hand, administration of Peg-IFN and ribavirin was unrelated to the occurrence of catastrophic autoimmune diseases. Collectively, these findings suggest that effective treatment of HCV could reduce extrahepatic morbidity in terms of renal failure and circulatory events.
Viral eradication plausibly underlies the uncovered associations. In view of the compelling evidence indicating the pathogenic role of HCV in renal and circulatory morbidity,3–13 it stands to reason that removal of the inciting pathogen is able to improve end-organ outcomes. This study regrettably is limited in lacking laboratory results to directly determine virological response, but we are confident of a high SVR rate in the treated cohort based on prior robust data from Taiwan.17–19 Because premature termination with duration <16 weeks could serve as an indicator of therapeutic failure, the unreduced risks in the incompletely treated patients also corroborated our inference. Besides, there is no reason to believe pharmacological properties of the interferon–ribavirin combination could directly explain the findings. In fact, this regimen is notoriously linked to various adverse reactions that may affect every system,34 and ranked among the top in the drug lists that could adversely cause renal failure.35
Previous studies have shown that antiviral treatment could stabilise renal function in patients with HCV-associated cryoglobulinaemia and glomerulonephritis, particularly in those who cleared the virus.36 These studies, constrained by the scale or design, were unable to address ‘hard’ clinical outcomes as the endpoints but had to resort to laboratory measurement such as serum creatinine or urine protein. Berenguer and colleagues have reported that HCV eradication was associated with significant reduction in liver-unrelated mortality among patients co-infected with HIV.23 Of note, they noted 1 vs 6 cases of cardiovascular death in 626 treatment responders (0.16%) and 973 non-responders (0.62%), respectively, although event incidences were not specifically compared for this cause of death.
We have recently demonstrated in patients with DM that treating concomitant HCV infection was associated with improved renal and circulatory outcomes.24 The present study, which encompasses a general population with 86.1% being non-diabetic, is able to further untangle the interrelationship between DM and antiviral treatment in determining extrahepatic risks of HCV. Since DM is by far the most influential risk factor (HR 21.33; 95% CI 13.46 to 33.80) of ESRD, it is likely that most cases with HCV-related ESRD are predisposed by diabetic nephropathy. Therefore, the effect of viral eradication in alleviating insulin resistance and preventing DM, which has been repetitively shown in the literature,37 ,38 may contribute to the striking reduction in renal risk. In accordance with this inference, if the participants were not diabetic before antiviral therapy, their risk of ESRD within 8 years of treatment was negligible. With regard to the risks of ACS and ischaemic stroke, the impact of DM was not so paramount and the effect of antiviral therapy in the non-diabetic subgroup appeared less dramatic. Conceivably, a macrovascular complication is determined by various factors, many of which are not amenable to viral clearance.
Our finding did not support the effectiveness of Peg-IFN plus ribavirin in lowering the risk of autoimmune diseases. This might implicate that autoimmunity induced by HCV should take place early in the course of infection and persist despite elimination of the virus. Compatibly, Molleston and colleagues reported that Peg-IFN-based treatment did not affect serum auto-antibodies in a paediatric cohort with HCV infection.39 In that study, auto-antibodies neither changed during the treatment nor differed between patients with and without viral clearance. Then again, this can be viewed as a reassuring finding insomuch that interferon itself can precipitate autoimmune disorders.40 We could not rule out the possibility of type II error for this infrequent outcome, especially when taking the length of observation into account. Although participants were followed up for as long as 8 years, the mean duration was approximately 3.3 years in this open-cohort research. Whether a longer observation would change the insignificant association warrants further investigation.
The landscape of treatment for HCV has been changing rapidly.41 The all-oral regimen promises to virologically cure most infected individuals, but its effectiveness in clinical outcomes cannot be taken for granted and has to be examined by empirical data in the future. For instance, the interferon-free therapy appears to be safely tolerable in severely morbid patients who cannot receive interferon or ribavirin, but it is questionable if HCV still substantially drives progression of the diseases in this population, and SVR at this stage may be too late to alter their end-organ outcomes.
Theoretically, a randomised placebo-controlled trial is the most ideal design to appraise the effectiveness of an intervention. However, critical events usually take time to develop, occurring at a low incidence in an average-risk population. Conduct of a trial in this scenario requires a huge sample size and prolonged observation, and can be impractical in reality. It is very improbable that there will be such a trial to clarify how antiviral therapy modifies extrahepatic outcomes of HCV. Besides, randomisation to placebo can hardly be regarded as ethically acceptable for patients with HCV infection.
In addition to the virtually universal coverage of a nationwide population, this study has the following methodological strengths. First, eligibility criteria were explicitly set to ensure all enrolled individuals should be entitled to antiviral therapy, so that bias from indication or contraindication is minimised. To this end, we deliberately confined enrolment to patients presumably with elevated liver enzymes and without conditions that precluded use of interferon or ribavirin. As a means to further optimise comparability between cohorts, we not only matched them in propensity scores, but also set the baseline at the administration of antiviral therapy. We did not choose the time of diagnosis or any outset prior to treatment because the condition might change over time. Moreover, the meticulous matching in elapsed duration from diagnosis to therapy eliminated immortal time bias. Taking competing mortality into consideration is another crucial merit. This procedure avoided overestimating the incidences of extrahepatic events in the untreated cohort who had a higher overall mortality.42 All in all, despite its observational nature, the present research provides the most convincing data to date in assessing potential benefits of treating HCV in outcomes outside the liver.
There are several limitations that require attention. First, the strict eligibility criteria prevent extrapolation to patients with serious comorbidity or those without elevated liver enzymes. Patients could be ineligible simply because they never used ‘hepatoprotective’ agents. Exclusion of these patients may limit generalisability of our analysis, but it will not compromise its validity. Similarly, while outcomes are unequivocally defined to ensure internal validity, the definition cannot capture less severe complications. For example, mild autoimmune disorders not certified in the RCIPD would be missed. This limitation, nevertheless, should have biased the results towards null difference rather than causing a spurious association. Furthermore, the NHIRD regrettably does not contain information regarding the SVR status, viral genotype, viral load, serum creatinine, lifestyle and family history. It was possible that some patients who spontaneously cleared the virus were enrolled as untreated controls. Nonetheless, this should lead to underestimation of the adverse events in the untreated cohort. Finally, for the specific aim of unconfounding the association between treatment and outcomes, the analysis was adjusted for multiple covariates including hospital level. Intriguingly, the level of healthcare setting was linked with ESRD and stroke in the multivariate Cox model. However, it is beyond the scope of the present research to delineate if it reflects the institutions’ facility, physicians’ expertise, patients’ composition, a confounded result, or simply a chance finding.
In conclusion, this nationwide cohort study shows that Peg-IFN plus ribavirin is associated with improvement in the renal and circulatory outcomes among patients with HCV infection, with an estimated risk reduction of 85% in ESRD, 23% in ACS and 38% in ischaemic stroke. We also demonstrate that this regimen is unrelated to the risk of autoimmune diseases. These results support an aggressive antiviral strategy to improve extrahepatic outcomes in patients with HCV infection.
Acknowledgments
This study is based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health and managed by National Health Research Institutes. The interpretation and conclusions contained herein do not represent those of Bureau of National Health Insurance, Department of Health or National Health Research Institutes.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Part of this study was presented at the 22th United European Gastroenterology Week (UEGW 2014) on 20 October 2014, Vienna, Austria (OP045).
-
Contributors Y-CH and C-YW conceived and designed the study. HJH, J-TL and C-YW obtained and managed the database. HJH and Y-TH analysed the data. Y-CH, H-HW and C-YW interpreted the results. Y-CH drafted the manuscript. Y-TH, H-HW, M-SW, J-TL and C-YW contributed to editing and revising the paper. C-YW is the guarantor.
-
Funding This work was supported in part by the Taiwan National Science Council (NSC 102-2314-B-650-008), National Health Research Institute (PH-101-PP-23) and the E-Da Hospital (EDAHP102006).
-
Competing interests Y-CH reports has received lecture fees from Merck Sharp & Dohme (Taiwan) and Roche (Taiwan).
-
Ethics approval The Research Ethics Committee of the Taiwan National Health Research Institute and the Institutional Review Board of the E-Da Hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.