Article Text

Abstract
Objective: Irritable bowel syndrome (IBS) is a chronic functional gastrointestinal disorder. Evidence for treatment of the condition with antidepressants and psychological therapies is conflicting.
Design: Systematic review and meta-analysis of randomised controlled trials (RCTs). MEDLINE, EMBASE and the Cochrane Controlled Trials Register were searched (up to May 2008).
Setting: RCTs based in primary, secondary and tertiary care.
Patients: Adults with IBS.
Interventions: Antidepressants versus placebo, and psychological therapies versus control therapy or “usual management”.
Main outcome measures: Dichotomous symptom data were pooled to obtain a relative risk (RR) of remaining symptomatic after therapy, with a 95% confidence interval (CI). The number needed to treat (NNT) was calculated from the reciprocal of the risk difference.
Results: The search strategy identified 571 citations. Thirty-two RCTs were eligible for inclusion: 19 compared psychological therapies with control therapy or “usual management”, 12 compared antidepressants with placebo, and one compared both psychological therapy and antidepressants with placebo. Study quality was generally good for antidepressant but poor for psychological therapy trials. The RR of IBS symptoms persisting with antidepressants versus placebo was 0.66 (95% CI, 0.57 to 0.78), with similar treatment effects for both tricyclic antidepressants and selective serotonin reuptake inhibitors. The RR of symptoms persisting with psychological therapies was 0.67 (95% CI, 0.57 to 0.79). The NNT was 4 for both interventions.
Conclusions: Antidepressants are effective in the treatment of IBS. There is less high-quality evidence for routine use of psychological therapies in IBS, but available data suggest these may be of comparable efficacy.
Statistics from Altmetric.com
Irritable bowel syndrome (IBS) is a functional gastrointestinal (GI) disorder for which there is no known structural or anatomical explanation. The prevalence of IBS in the general population is estimated to be between 5% and 20%,1–4 and its management accounts for up to 25% of a gastroenterologist’s workload in the outpatient clinic.5 The condition tends to follow a chronic relapsing and remitting course.6–9 Effective therapies for IBS are therefore required, in order to alleviate symptoms, and thereby reduce consultation behaviour and consumption of other valuable medical resources.
Patients with IBS are more likely to suffer from coexistent mood disorder, anxiety and neuroticism compared to healthy controls or individuals with organic pathology,10 and to report a low quality of life.11–13 A significant proportion of patients with IBS who consult in tertiary care have an underlying psychiatric illness,14 15 and even non-consulters have higher levels of depression when compared to the general population.16 17
The latest revision of the Rome criteria requires the presence of recurrent abdominal pain or discomfort, in association with a change in bowel habit, for the diagnosis of IBS to be reached.18 Patients with IBS often demonstrate increased sensitivity in response to balloon distension of the GI tract,19 and this visceral hypersensitivity is thought to contribute to the chronic pain experienced by those with the condition. Antidepressant drugs are often used in the treatment of chronic pain, owing to their potential modulation of pain perception, and have been shown to be effective in this setting.20
Box 1 Eligibility criteria
-
Randomised controlled trials
-
Adults (participants aged >16 years)
-
Diagnosis of irritable bowel syndrome (IBS) based on either a clinician’s opinion, or meeting specific diagnostic criteria (ie, Manning, Kruis score, Rome I, II, or III), supplemented by negative investigations where trials deemed this necessary
-
Compared antidepressants with placebo, or psychological therapies with either control therapy or a physician’s “usual management”
-
Minimum duration of therapy, 7 days
-
Minimum duration of follow-up, 7 days
-
Global assessment of IBS symptoms or abdominal pain following therapy (preferably patient-reported, but if this was not available then as assessed by a physician or questionnaire data)
For these reasons, it would be reasonable to assume a beneficial effect of antidepressant drugs, such as tricyclic antidepressants (TCAs) and selective serotonin reuptake inhibitors (SSRIs), or psychological therapies, such as cognitive behavioural therapy (CBT), on the symptoms of IBS. However, evidence for this is conflicting, and despite numerous systematic reviews examining this issue there is no clear consensus.21–28 This uncertainty is reflected in British Society of Gastroenterology (BSG) guidelines for the management of the condition,29 which state that evidence for any benefit of TCAs is conflicting, and may be limited to an improvement in pain, and therefore recommend their use as second-line treatment for this symptom. Similar recommendations are made for the role of psychological therapies, whilst the role of SSRIs in the management of IBS is not specified. The American Gastroenterological Association (AGA) technical review,30 and the American College of Gastroenterology (ACG) position statement,31 informed by a systematic review, are similarly guarded.
The role of both antidepressants and psychological therapies in the management of IBS is therefore unclear at the present time. In an attempt to address this uncertainty we have conducted a systematic review and meta-analysis of randomised controlled trials (RCTs) to estimate the effect of antidepressant therapy and psychological therapies on improvement or cure of IBS symptoms.
METHODS
Search strategy and study selection
A search of the medical literature was conducted using MEDLINE (1950 to May 2008), EMBASE (1980 to May 2008), and the Cochrane Controlled Trials Register (2007). Randomised controlled trials examining the effect of antidepressants and psychological therapies in adult patients (over the age of 16 years) with IBS were eligible for inclusion (box 1). The first period of cross-over RCTs were also eligible for inclusion. In the case of antidepressant trials the control arm was required to receive placebo, whilst for studies of psychological therapies the control arm could receive placebo, symptom monitoring (including waiting list control), or a physician’s “usual management”. Duration of therapy had to be at least 7 days. The diagnosis of IBS could be based on either a physician’s opinion or symptom-based diagnostic criteria, supplemented by the results of investigations to exclude organic disease, where studies deemed this necessary. Subjects were required to be followed up for at least 1 week, and studies had to report either a global assessment of IBS symptom cure or improvement, or abdominal pain cure or improvement, after completion of treatment, preferably as reported by the patient, but if this was not recorded then as documented by the investigator or via questionnaire data. Where studies included patients with other functional GI disorders, or did not report these types of dichotomous data, but were otherwise eligible for inclusion in the systematic review, we attempted to contact the original investigators in order to obtain further information.
Box 2 Methodology for data extraction
-
Outcome of interest: improvement in global symptoms of inflammatory bowel syndrome (IBS) preferable, if not reported then improvement in abdominal pain
-
Reporting of outcomes: patient-reported preferable; if not available, then investigator-reported
-
Time of assessment: upon completion of treatment
-
Denominator used: true intention-to-treat analysis; if not available, then all evaluable patients
-
Cut-off used for dichotomisation: any improvement in global symptoms of IBS or abdominal pain for Likert-type scales, investigator-defined improvement for continuous scales; if no investigator definition was available we used a ⩾1 standard deviation decrease in symptom score from baseline to completion of treatment (we assessed whether the use of any decrease in symptom score from baseline to completion of therapy altered our analysis)
Studies on IBS were identified with the terms irritable bowel syndrome and functional diseases, colon (both as a medical subject heading (MeSH) and free-text terms), and IBS, spastic colon, irritable colon, and functional adj5 bowel (as free-text terms). These were combined using the set operator AND with studies identified with the terms: psychotropic drugs, antidepressive agents, antidepressive agents (tricyclic), desipramine, imipramine, trimipramine, doxepin, dothiepin, nortriptyline, amitriptyline, selective serotonin reuptake inhibitors, paroxetine, sertraline, fluoxetine, citalopram, venlafaxine, cognitive therapy, psychotherapy, behaviour therapy, relaxation techniques, and hypnosis (both as MeSH terms and free-text terms), and the following free-text terms: behavioural therapy, relaxation therapy, and hypnotherapy.
There were no language restrictions and abstracts of the papers identified by the initial search were evaluated by the lead reviewer for appropriateness to the study question, and all potentially relevant papers were obtained and evaluated in detail. Foreign language papers were translated where necessary. Abstract books of conference proceedings between 2001 and 2007 were hand-searched to identify potentially eligible studies published only in abstract form. The bibliographies of all identified relevant studies were used to perform a recursive search of the literature. Articles were independently assessed by two reviewers using pre-designed eligibility forms, according to the prospectively defined eligibility criteria. Any disagreement between investigators was resolved by consensus.
Outcome assessment
The primary outcomes assessed were the effect of antidepressants compared to placebo, and the effect of psychological therapies compared to control treatment or a physician’s “usual management”, on global IBS symptoms or abdominal pain after cessation of treatment. Secondary outcomes included assessing efficacy according to specific type of antidepressant or psychological therapy, and adverse events occurring as a result of antidepressant therapy.
Data extraction
All data were extracted independently by two reviewers on to a Microsoft Excel spreadsheet (XP professional edition; Microsoft, Redmond, Washington, USA) as dichotomous outcomes (global IBS symptoms persistent or unimproved, or abdominal pain persistent or unimproved) (box 2). In addition, the following clinical data were extracted for each trial: setting (primary, secondary or tertiary care-based), number of centres, country of origin, dose of antidepressant or number of sessions of psychological therapy administered, duration of therapy, total number of adverse events reported, criteria used to define IBS, primary outcome measure used to define symptom improvement or cure following therapy, duration of follow-up, proportion of female patients, and proportion of patients according to predominant stool pattern. We also recorded the handling of the control arm for trials of psychological therapies. Data were extracted as intention-to-treat analyses, where all drop-outs are assumed to be treatment failures, wherever trial reporting allowed this.
Study quality
Assessment of study quality was performed independently by two reviewers according to the Jadad scale (table 1),32 which records whether a study is described as randomised and double-blind, the method of generation of the allocation schedule and method of double-blinding, and whether there is a description of drop-outs during the trial.
Data synthesis and statistical analysis
Data were pooled using a random effects model, to give a more conservative estimate of the effect of individual therapies, allowing for any heterogeneity between studies.33 The impacts of different interventions were expressed as a relative risk (RR) of global IBS symptoms or abdominal pain persisting with intervention compared to control with 95% confidence intervals (CIs). The number needed to treat (NNT) and 95% CIs were calculated from the reciprocal of the risk difference from the meta-analysis.
The results of individual studies can be diverse, and this inconsistency within a single meta-analysis can be quantified with a statistical test of heterogeneity, to assess whether the variation across trials is due to true heterogeneity or chance. This quantity is termed I2, and its value ranges from 0% to 100%, with 0% representing no observed heterogeneity, and larger values indicating increasing heterogeneity. A value below 25% is arbitrarily chosen to represent low levels of heterogeneity.34 Where the degree of statistical heterogeneity was greater than this between trial results in this meta-analysis, possible explanations were investigated using sensitivity analyses according to trial setting, criteria used to define IBS, whether method of randomisation or concealment of allocation were reported, level of blinding, study quality according to the Jadad scale and, for trials of psychological therapies, method of handling of the control arm. These are exploratory only, and may explain some of the observed variability, but the results should be interpreted with caution.
Review Manager version 4.2.8 and StatsDirect version 2.4.4 were used to generate Forest plots of pooled relative risks and risk differences for primary and secondary outcomes with 95% CIs, as well as funnel plots. The latter were assessed for evidence of asymmetry, and therefore possible publication bias, using the Egger test.35
RESULTS
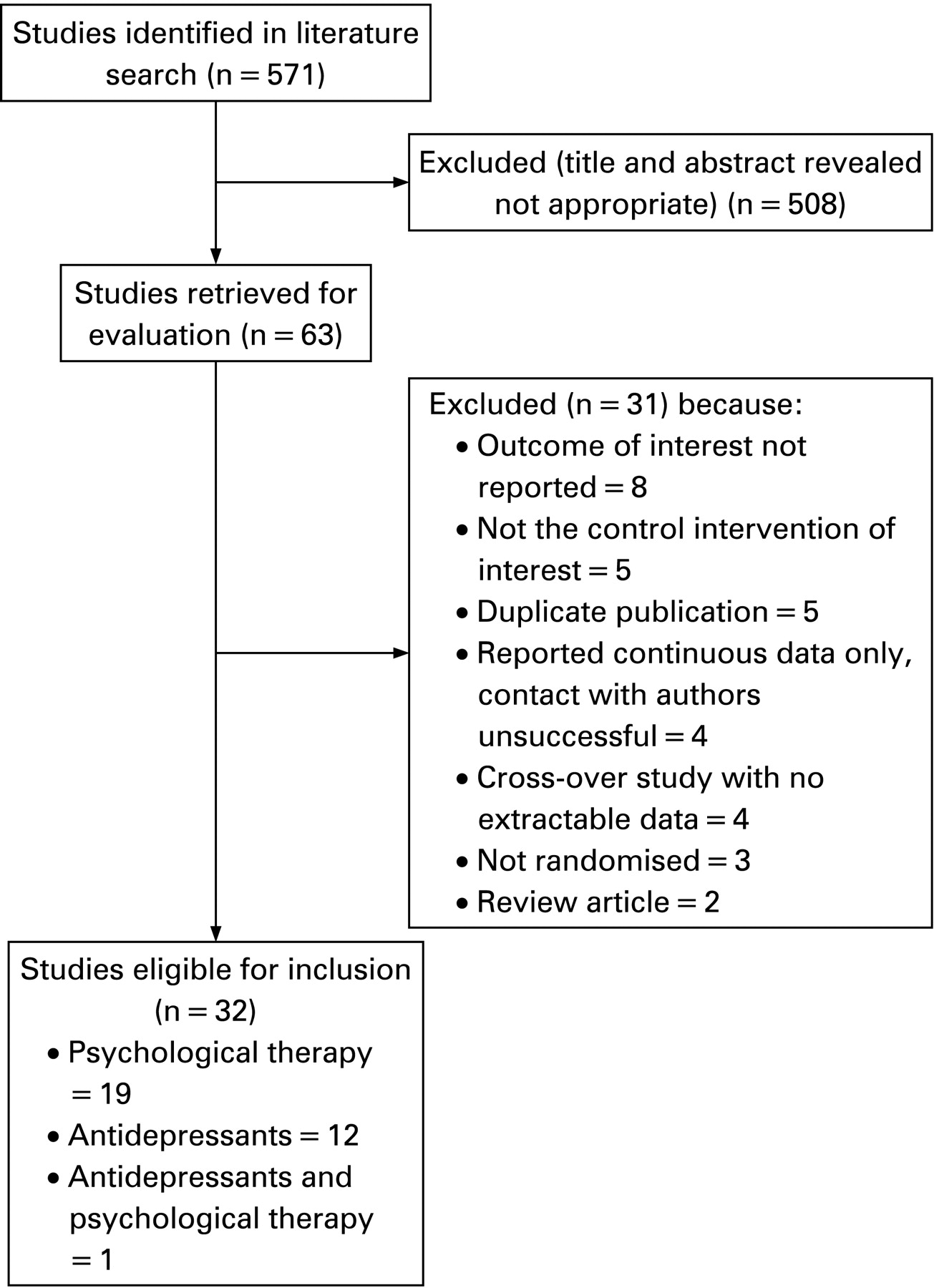
The search strategy generated 571 citations of which 63 appeared to be relevant to the systematic review and were retrieved for further assessment (fig 1). We successfully contacted six of the primary investigators of the 63 studies to clarify data, exclude patients with other functional GI disorders from the analysis, or obtain original data sets to conduct additional analyses ourselves in order to dichotomise data and thereby maximise trial eligibility for the current meta-analysis. Of these 63 RCTs, 31 were excluded for various reasons, leaving 32 eligible trials,36–67 19 of which compared psychological therapies to control therapy or a physician’s “usual management”,38–50 62–67 12 compared antidepressants to placebo,36 51–61 and one compared both psychological therapy and antidepressants to placebo.37 Agreement between reviewers for assessment of trial eligibility was good (kappa statistic = 0.90).
Efficacy of antidepressants in the treatment of IBS
There were 13 studies comparing antidepressants to placebo for the treatment of IBS,36 37 51–61 including a total of 789 patients, 432 of whom received active therapy and 357 placebo. Seven of the studies were conducted in secondary care,36 52 56 58–61 and six in tertiary care.37 51 53–55 57 Eight studies used TCAs,36 37 53 56 58–61 four studies SSRIs,52 54 55 57 and one study both.51 Ten of the studies scored 4 or more on the Jadad scale.37 51–58 60 The proportion of female patients recruited by trials ranged from 44% to 100%. Six studies reported sub-type of IBS according to predominant stool pattern.52 54 55 57 58 60 One recruited only constipation-predominant patients,52 one included only diarrhoea-predominant,60 and predominant stool pattern was mixed in the other four.54 55 57 58 Detailed characteristics of individual studies are provided in table 2.
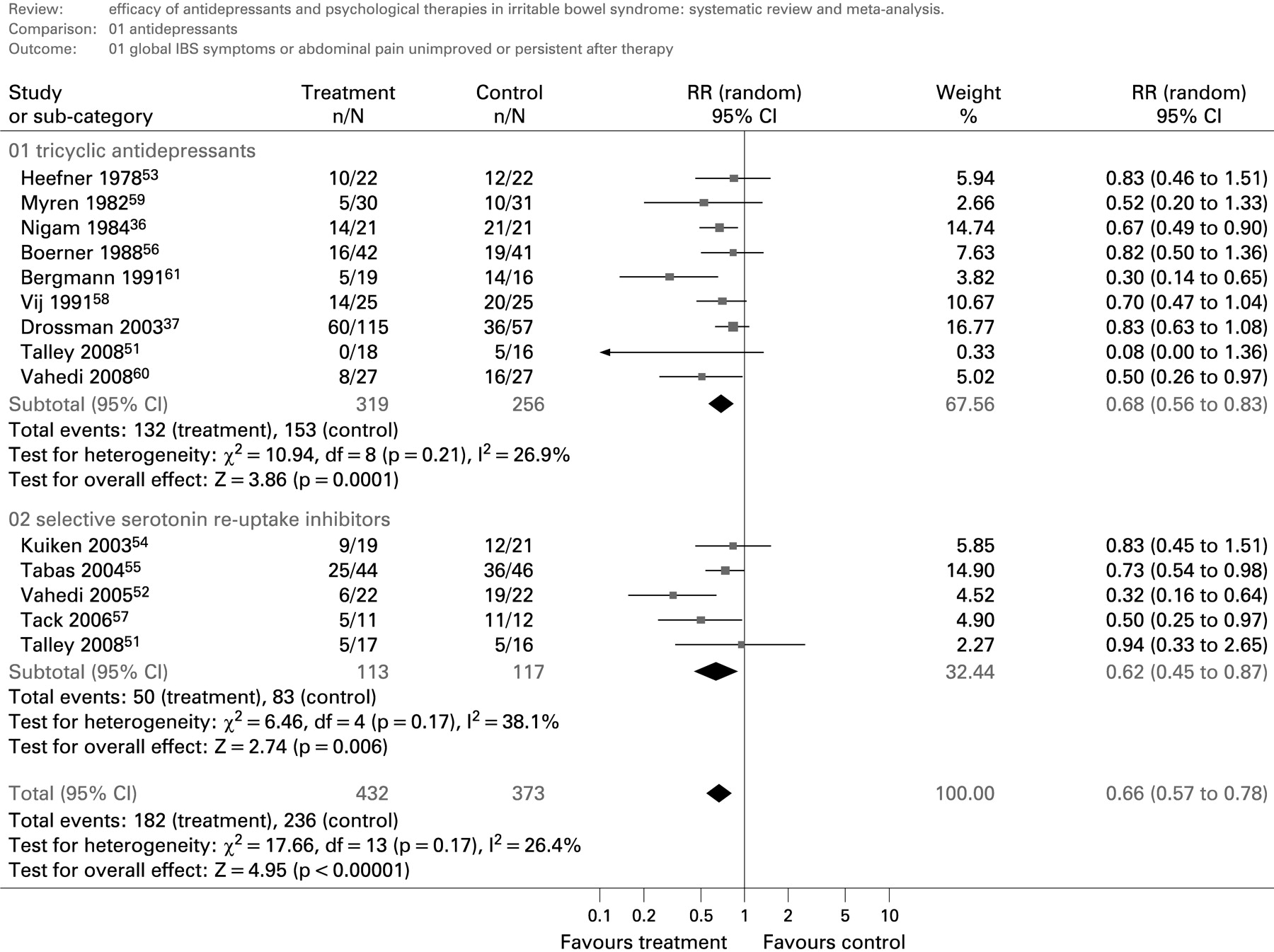
There were 182 of 432 (42.1%) patients assigned to antidepressant therapy with persistent or unimproved IBS symptoms following therapy, compared to 231 of 357 (64.7%) allocated to placebo. The relative risk of IBS symptoms persisting or remaining unimproved after treatment with antidepressant therapy versus placebo was 0.66 (95% CI, 0.57 to 0.78), with marginal statistically significant heterogeneity detected between studies (I2 = 26.4%, p = 0.17) (fig 2). The number needed to treat with antidepressant therapy to prevent IBS symptoms persisting in one patient was 4 (95% CI, 3 to 6). The Egger test demonstrated evidence of funnel plot asymmetry (p = 0.02), suggesting publication bias, with a lack of small studies showing no effect of antidepressant therapy on the symptoms of IBS (fig 3). However, this appeared to be driven by the TCA arm of one small study,51 and when this study arm was excluded from the meta-analysis the asymmetry was no longer statistically significant (Egger test, p = 0.07). Sensitivity analyses were conducted (table 3). Treatment effect appeared to be increased in secondary care-based studies, studies that did not state method of generation of the randomisation schedule or method of concealment of allocation, and studies scoring less than 4 on the Jadad scale. Heterogeneity between studies was no longer significant when studies were subgrouped according to whether or not the method of concealment of allocation was reported. A statistically significant difference in treatment effect was not detected in any of these subgroup analyses.

The effect of antidepressant therapy on abdominal pain was reported by five studies,52 53 55 58 60 with 63 of 127 (49.6%) patients receiving antidepressants having persistent abdominal pain following treatment, compared to 87 of 129 (67.4%) subjects allocated to placebo, giving a relative risk of abdominal pain persisting of 0.66 (95% CI, 0.41 to 1.06) with considerable heterogeneity between studies (I2 = 74.6%, p = 0.003).
Efficacy of TCAs in the treatment of IBS
Nine studies compared TCAs to placebo in a total of 575 patients.36 37 51 53 56 58–61 Of the 319 patients receiving active therapy, 132 (41.4%) had persistent symptoms after treatment, compared to 153 of 256 (59.8%) receiving placebo. The relative risk of IBS symptoms persisting with TCAs compared to placebo was 0.68 (95% CI, 0.56 to 0.83), with marginal statistically significant heterogeneity detected between studies (I2 = 26.9%, p = 0.21) (fig 2), and evidence of funnel plot asymmetry (Egger test, p = 0.03). Again, this was driven by one study,51 and when this was removed from the analysis there was no longer statistically significant publication bias (Egger test, p = 0.09). The number needed to treat with TCAs to prevent IBS symptoms persisting in one patient was 4 (95% CI, 3 to 8).
Efficacy of SSRIs in the treatment of IBS
Five studies compared SSRIs with placebo in a total of 230 patients.51 52 54 55 57 There were 50 of 113 (44.2%) patients allocated to SSRIs with persistent symptoms following therapy, compared to 83 of 117 (70.9%) placebo patients. The relative risk of IBS symptoms persisting with SSRIs compared to placebo was 0.62 (95% CI, 0.45 to 0.87), with statistically significant heterogeneity between studies (I2 = 38.1%, p = 0.17) (fig 2), but no evidence of funnel plot asymmetry (Egger test, p = 0.60). The number needed to treat with SSRIs to prevent IBS symptoms persisting in one patient was 3.5 (95% CI, 2 to 14).
Adverse events with antidepressant therapy
Eleven of the studies reported adverse events data,36 37 51–54 56–60 but only six provided the total number of patients experiencing adverse events with antidepressants compared to placebo in a total of 301 patients.53 54 56–59 There were 27 of 149 (18.1%) patients assigned to antidepressants reporting adverse events compared to 14 of 152 (9.2%) allocated to placebo. The relative risk of experiencing adverse events with antidepressants compared to placebo was 1.63 (95% CI, 0.94 to 2.80), with no heterogeneity detected between studies (I2 = 0%, p = 0.67). There were no serious adverse events, the commonest reported by patients allocated to antidepressant therapy were drowsiness and dizziness.
Efficacy of psychological therapies in the treatment of IBS
We identified 20 studies comparing various psychological therapies to control therapy or a physician’s “usual management” for the treatment of IBS in a total of 1278 patients.37–50 62–67 One study was conducted in primary care,49 and the remainder in tertiary care. Six studies used CBT,37 40 43 45 47 49 four studies used relaxation training or therapy,38 41 46 48 three studies used multi-component psychological therapy,39 42 65 two studies used hypnotherapy,62 66 two studies used dynamic psychotherapy,50 64 one study used self-administered CBT,67 one study used stress management,44 and one study used both CBT and relaxation therapy.63 The control arm received symptom monitoring in 11 studies,38–43 45 47 48 62 67 usual care in seven studies,44 46 49 50 63–65 supportive therapy in one study,66 and placebo in one study.37 Thirteen of the studies scored only 1 or 2 on the Jadad scale,38–45 47 48 50 62 65 and none scored 4 or more. The proportion of female patients recruited by trials ranged from 57% to 100%. Ten studies reported sub-type of IBS according to predominant stool pattern.38 39 41–43 47 64–67 No study recruited constipation or diarrhoea-predominant patients exclusively. Detailed characteristics of individual studies are provided in table 4.
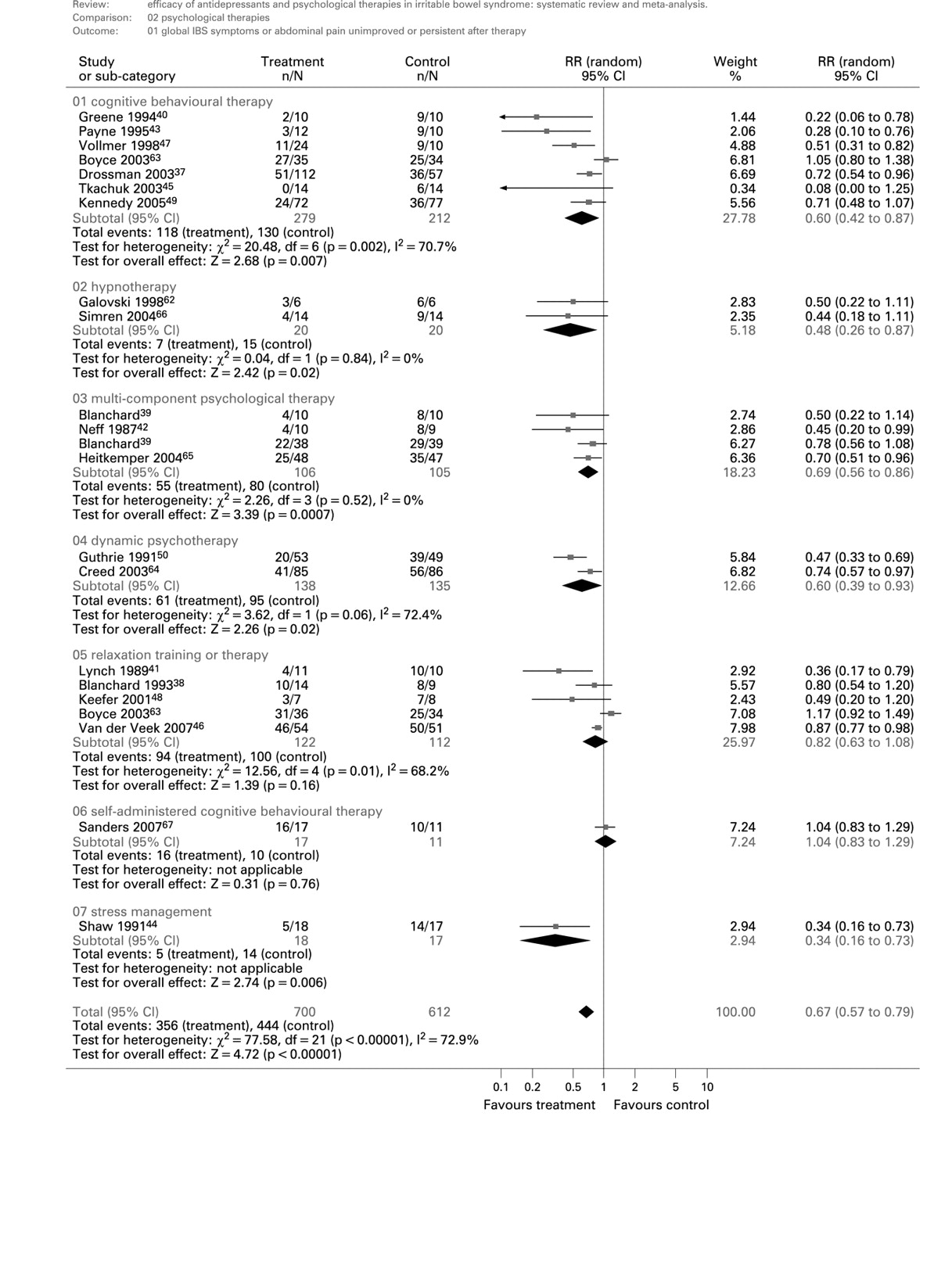
IBS symptoms persisted in 356 of 700 (50.9%) patients receiving psychological therapies compared to 419 of 578 (72.5%) receiving physician’s “usual management” or control therapy. The relative risk of IBS symptoms persisting with psychological therapies compared to physician’s “usual management” or control therapy was 0.67 (95% CI, 0.57 to 0.79) (fig 4), with considerable heterogeneity detected between studies (I2 = 72.9%, p<0.0001), and evidence of funnel plot asymmetry (Egger test, p<0.0001), with a lack of small studies showing no effect of psychological therapies on the symptoms of IBS (fig 5). The number needed to treat with psychological therapies to prevent IBS symptoms persisting in one patient was 4 (95% CI, 3 to 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
As nine of the studies of psychological therapies were conducted by the same group of investigators we performed a post hoc sensitivity analysis according to study centre. There were 270 patients with IBS in the nine studies published by Blanchard and colleagues,38–40 42 43 47 48 62 67 and 11 studies published by other groups of authors reporting on 1008 patients.37 41 44–46 49 50 63–66 The efficacy of psychological therapies in studies published by Blanchard and colleagues appeared to be greater (RR = 0.59; 95% CI, 0.42 to 0.82; I2 = 71.9%, p = 0.0002) than studies conducted in other centres (RR = 0.71; 95% CI, 0.58 to 0.87, I2 = 76.4%, p<0.0001), although a statistically significant difference was not detected (p = 0.35). We performed a further subgroup analysis according to handling of the control arm. The RR of symptoms persisting was lower in studies using symptom monitoring (0.54; 95% CI, 0.39 to 0.76) than in those where usual management, supportive therapy, or placebo were the control intervention (RR = 0.75; 95% CI, 0.62 to 0.91), though again this difference was not statistically significant (p = 0.09).
Efficacy of CBT in IBS
Seven studies compared CBT to control therapy or physician’s “usual management” in 491 patients.37 40 43 45 47 49 63 IBS symptoms persisted in 118 of 279 (42.3%) of those assigned to CBT compared to 130 of 212 (61.3%) of those allocated to control therapy or physician’s “usual management”, with a relative risk of symptoms persisting of 0.60 (95% CI, 0.42 to 0.87), and a number needed to treat of 3 (95% CI, 2 to 7). There was statistically significant heterogeneity between studies (I2 = 70.7%, p = 0.002), and evidence of funnel plot asymmetry (Egger test, p = 0.01), with a lack of small studies showing no effect of CBT on the symptoms of IBS. When the three studies conducted in the same centre were excluded from the analysis,40 43 47 the beneficial effect of CBT on symptoms of IBS disappeared (RR of symptoms persisting = 0.79; 95% CI, 0.56 to 1.13).
Efficacy of relaxation training or therapy in IBS
Five studies compared relaxation training or therapy to control therapy or physician’s “usual management” in 234 patients.38 41 46 48 63 IBS symptoms persisted in 94 of 122 (77.0%) of those assigned to relaxation training or therapy compared to 100 of 112 (89.3%) of those allocated to control therapy or physician’s “usual management”, with a relative risk of symptoms persisting of 0.82 (95% CI, 0.63 to 1.08), and statistically significant heterogeneity between studies (I2 = 68.2%, p = 0.01).
Efficacy of hypnotherapy in IBS
Two studies compared hypnotherapy to control therapy or physician’s “usual management” in 40 patients.62 66 IBS symptoms persisted in 7 of 20 (35%) of those assigned to hypnotherapy compared to 15 of 20 (75%) of those allocated to control therapy or physician’s “usual management”, with a relative risk of symptoms persisting of 0.48 (95% CI, 0.26 to 0.87), and a number needed to treat of 2 (95% CI, 1.5 to 7).
Efficacy of multi-component psychological therapy in IBS
Three studies compared multi-component psychological therapy to control therapy or physician’s “usual management” in 211 patients.39 42 65 IBS symptoms persisted in 55 of 106 (51.9%) of those assigned to multi-component psychological therapy compared to 80 of 105 (76.2%) of those allocated to control therapy or physician’s “usual management”, with a relative risk of symptoms persisting of 0.69 (95% CI, 0.56 to 0.86), and a number needed to treat of 4 (95% CI, 3 to 8).
Efficacy of dynamic psychotherapy in IBS
Two studies compared dynamic psychotherapy to control therapy or physician’s “usual management” in 273 patients.50 64 IBS symptoms persisted in 61 of 138 (44.2%) of those assigned to dynamic psychotherapy compared to 95 of 135 (70.4%) of those allocated to control therapy or physician’s “usual management”, with a relative risk of symptoms persisting of 0.60 (95% CI, 0.39 to 0.93), and a number needed to treat of 3.5 (95% CI, 2 to 25).
Efficacy of self-administered CBT and stress management in IBS
There was only one study using each of these treatment modalities.44 67 Self-administered CBT had little effect on symptoms over control therapy or physician’s “usual management”, whilst stress management appeared to reduce the risk of IBS symptoms persisting following therapy.
DISCUSSION
This systematic review and meta-analysis has demonstrated a significant benefit of antidepressants over placebo, and psychological therapies over control therapy or a physician’s “usual management”, for the treatment of IBS. The number needed to treat in both cases, to prevent one IBS patient’s symptoms persisting, was 4. Tricyclic antidepressants and SSRIs were equally effective, with no significant differences detected in either the relative risk of symptoms persisting or the number needed to treat between the two drug classes. Adverse events were more common in patients assigned to antidepressants than those allocated to placebo, but a statistically significant difference was not detected. The overall treatment effect was very similar for psychological therapies, but there was most evidence for CBT. Multi-component psychological therapy, dynamic psychotherapy, and hypnotherapy were also effective in IBS, though in smaller numbers of patients. Relaxation therapy did not have a statistically significant effect on IBS symptoms, though there were few eligible published studies, and this could therefore be due to a type II error. There was also insufficient evidence for stress management and self-administered CBT.
We are aware of six previous systematic reviews that have examined the efficacy of antidepressants in IBS.21–26 Unfortunately, all of these have methodological limitations. Four of these considered only English-language articles,21 22 24 25 three did not extract and combine data to give an overall treatment effect,21 23 25 three extracted data incorrectly from eligible studies,22 24 26 two included cross-over studies in the analysis,22 24 one only identified three of ten truly eligible studies published at the time of their review,26 one included trials of antidepressants in functional GI disorders and did not report IBS patients separately,22 and one only considered treatments available in the USA.23 It is therefore not surprising that these reviews have reached different conclusions about the role of antidepressants in IBS. In addition, there have been several RCTs published in the interim.
Two of these reviews also examined the role of psychological therapies in the treatment of IBS,23 25 and both stated that although the quality of the available evidence was poor these approaches may lead to an improvement in individual IBS symptoms. However, there was no data synthesis undertaken to provide an estimate of this effect. A review by Lackner et al published in 2004 identified 17 studies,27 but only ten of these provided extractable dichotomous data for analysis. The authors estimated a number needed to treat with psychological therapies to improve one case of IBS of 2. However, the total number of included patients was 185, and nine of the ten studies emanated from a single centre. A recent Cochrane Collaboration systematic review of the efficacy of hypnotherapy identified only four RCTs,28 though again data were not combined owing to concerns about differences in outcome measures and study design. A descriptive analysis was undertaken, and reported that hypnotherapy was superior to control therapy in terms of its effect on both abdominal pain and global IBS symptoms. Only one of these studies was eligible for the current systematic review and meta-analysis.62 The remaining three trials were ineligible as two did not provide extractable data and one used psychotherapy as the control intervention.
The current systematic review and meta-analysis is superior to these previous reviews for several reasons. First, we have used rigorous methodology including a report of our search strategy and inclusion criteria, exclusion of non-randomised studies, independent data extraction by two reviewers, and use of an intention-to-treat analysis, to ensure that the treatment effect has not been overestimated. Second, we included non-English RCTs in the analysis, and contacted investigators of potentially eligible studies to either obtain dichotomous data or to exclude patients with other functional GI disorders from the analysis. This inclusive approach has ensured that we have identified more relevant published articles than previous systematic reviews in this area, including trials eligible for inclusion at the time of other reviews but not successfully identified by the authors. This has provided us with access to data for almost 800 IBS patients treated with antidepressants versus placebo, and almost 1300 patients randomised to psychological therapies versus control therapy or a physician’s “usual management. Third, we have pooled data to give an overall treatment effect, and a number needed to treat. Whilst this approach could be criticised by some, owing to differences in the methodology of individual included studies, we performed sensitivity analyses to explore reasons for heterogeneity between studies, and to assess effect of study location, design and setting on overall treatment effect, which remained significant in all the subgroups we examined. Finally, we have extracted and pooled adverse events data. This has not been carried out by previous investigators, and provides further useful data for both the physician and the patient.
There are limitations of this systematic review and meta-analysis, which arise owing to characteristics of the published literature available for synthesis. Although eligible RCTs of antidepressant therapy were of good to moderate quality, there was evidence of heterogeneity between these studies and publication bias. However, the difference in favour of antidepressants remained statistically significant when only higher quality studies, according to the Jadad scale,32 were considered in the analysis. Heterogeneity was of borderline significance, and was reduced when the effect of reporting the method of concealment of allocation was examined, and publication bias was no longer statistically significant when one small outlying study was excluded from the analysis. Subgroup analyses demonstrated that treatment effect was less in trials based in tertiary-care settings, and RCTs that reported method of generation of the randomisation schedule and concealment of allocation. It is not surprising that antidepressant therapy was less effective in subjects recruited in tertiary care, as these are likely to be the patients whose symptoms are the most difficult to treat. Our observation that studies that did not report the method of generation of the randomisation schedule or concealment of allocation tended to report an exaggerated treatment effect is in line with reports from the systematic review literature.68 These issues may mean that the true treatment effect has been overestimated, but there is still evidence from our subgroup analyses that the use of antidepressants in IBS is beneficial. Furthermore, the RCT conducted by Creed et al also randomised a large number of IBS patients to antidepressant therapy with an SSRI,64 and compared their outcomes with those allocated to a physician’s usual management. As this study did not have a placebo arm it was not eligible for inclusion in the current meta-analysis, but again there was a statistically significant improvement in IBS symptoms in those receiving SSRI compared to usual management.
Psychological therapies for IBS also seem to be effective, but there are more serious issues regarding the validity of the findings. There was significant heterogeneity when all studies were combined, which raises concerns over the appropriateness of such an approach, although as all these treatment modalities address possible underlying psychological aspects of the condition we felt that this was useful and justified. When subgroup analyses were conducted according to the type of psychological intervention used this heterogeneity persisted, suggesting that it was not entirely due to differences in the intervention applied. There was also evidence of a large degree of publication bias, and this remained when only RCTs of CBT, the intervention with the most available published evidence, were considered. A further concern was that nine of the eligible studies originated from the same centre, and when a subgroup analysis was conducted examining this issue there appeared to be a greater treatment effect in these nine studies than in the 11 studies emanating from other centres, though a statistically significant difference was not detected.
Another concern common to eligible RCTs of antidepressants and psychological therapies is a lack of adherence to recommendations from the Rome committee for the design of treatment trials for functional GI disorders.69 Many of the studies did not use the Rome criteria to define the presence of IBS, did not provide evidence of a power calculation, did not use a validated outcome measure to define treatment success and, in the case of RCTs of psychological therapies, investigators were blinded to treatment allocation in only three studies,37 63 64 as in this situation double-blinding would be difficult to achieve. However, a significant proportion of the trials were designed and conducted before these recommendations were made, and many of the eligible studies do meet other methodological criteria specified by these recommendations, such as a minimum duration of therapy of 8–12 weeks, a parallel study design, patient follow-up after therapy to assess symptoms, and use of patient-reported improvement in symptoms. The fact that the majority of trials only followed up patients for between 8 and 12 weeks means that the effect of both these therapies on IBS symptoms in the longer term remains unknown. Finally, only one of these eligible RCTs was conducted in primary care,49 and seven in secondary care,36 52 56 58–61 meaning that the results may not be generalisable to patients encountered in these settings.
It would appear from these data that both TCAs and SSRIs are effective for the treatment of IBS. Only four patients need to be treated to improve or cure one patient’s symptoms. This is an important finding, as previous systematic reviews have given conflicting evidence of their efficacy, and therefore current national guidelines for the management of the condition from the BSG, AGA and ACG make either conflicting or vague recommendations for the role of antidepressant therapy in the treatment of IBS.29–31 SSRIs have a theoretical advantage in being potentially better tolerated than TCAs. Imipramine has been shown to prolong orocaecal and whole gut transit times, whereas paroxetine decreases orocaecal transit time,70 so it may be that TCAs will work better in diarrhoea-predominant IBS and SSRIs in constipation-predominant, although the studies included did not evaluate this issue. The mechanism of action of these drugs remains speculative, though it is plausible that they have a general effect in increasing pain thresholds in IBS sufferers, as they are beneficial in neuropathic pain.71 It is also possible that any improvement in symptoms following therapy in these trials arose from the successful treatment of co-existent depression. Data from the trials included in this review do not support this hypothesis however. Three studies reported that there was no significant relationship between depression scores and improvement in IBS symptoms,55 57 58 and one RCT reported that treatment effect with desipramine was better in those without evidence of co-existent depression.37 These findings are consistent with a systematic review of 61 trials evaluating antidepressants in neuropathic pain,71 where there was no correlation between symptom improvement and depression score.
Psychological therapies for the treatment of IBS appear to have a similar treatment effect, though often in groups of patients in specialist centres who have failed pharmacological treatment. As studies are small, and of poorer methodological quality, no definitive proposal can be made concerning their role, although when the nine studies of psychological therapies conducted in the same centre were excluded in a sensitivity analysis the remaining trials were larger, on average, than those of antidepressant treatments. There appears to be the most evidence for CBT, in terms of number of RCTs, but when the three small trials emanating from a single centre were excluded from the analysis there was no longer any beneficial effect of CBT on IBS symptoms. Psychological therapies may have a role for patients who do not respond to conventional medical treatment, but further data from large, well-designed, high quality RCTs are required before any firm recommendations for their place in the management of IBS can be made.
In summary, this systematic review has demonstrated that both antidepressants and psychological therapies, particularly CBT, are efficacious in the treatment of IBS in the short-term, with only four patients needing to be treated to improve or cure one patient’s symptoms. Current guidelines for the management of the condition should be updated to include this important and novel information.
Acknowledgments
This study was performed to inform the American College of Gastroenterology monograph on irritable bowel syndrome. We would like to thank Drs A Foxx-Orenstein, W Chey, L Brandt, L Schiller, B Spiegel and E Achkar for their contributions to the discussion concerning the role of antidepressants and psychological therapies in the treatment of irritable bowel syndrome. We are grateful to the following investigators for answering our data queries and, where applicable, providing us with their original data sets for analysis: Drs P Boyce, K Cain, F Creed, D Drossman, M Heitkemper, R Jones, K Sanders, P Seed, J Tack and B Tomenson. We would also like to thank Dr P Bercik for assisting us with the translation of foreign language articles.
REFERENCES
Supplementary materials
Web Only Data 58/3/367
Files in this Data Supplement:
Footnotes
-
Funding: This study was funded by the American College of Gastroenterology.
-
Competing interests: Declared (the declaration can be viewed on the Gut website at http://www.gut.bmj.com/supplemental).