Article Text

Abstract
Background: Growing evidence suggests that patients with irritable bowel syndrome (IBS) have increased intestinal permeability. In addition, mucosal soluble mediators are involved in the pathophysiology of pain in IBS. We aimed to investigate (1) paracellular permeability in colonic biopsies of patients with IBS; and (2) the ability of soluble factors from colonic biopsies to reproduce these alterations in vitro.
Methods: Paracellular permeability in colonic biopsies of healthy subjects and patients with IBS was measured by mounting the biopsies in Ussing chambers. Cleared supernatant (SUP) of the culture from colonic biopsies was collected and applied to Caco-2 cells for 48 h. Paracellular permeability and transepithelial resistance (TER) were evaluated. mRNA expression of the tight junction proteins, zonula occludens (ZO)-1 and occludin, was assessed in colonic biopsies. Abdominal pain was assessed using a validated questionnaire.
Results: Permeability of colonic biopsies was significantly higher in patients with IBS compared to healthy subjects. These changes were associated with significantly lower expression of ZO-1 mRNA in biopsies of IBS as compared to healthy subjects. Compared to healthy subjects, SUP of IBS markedly reduced TER and significantly increased permeability in Caco-2 cells. SUP of IBS patients induced a significant decrease of ZO-1 mRNA in Caco-2 as compared to healthy subjects. SUP-induced increased paracellular permeability correlated with the severity of abdominal pain.
Conclusions: Our study shows that colonic soluble mediators are able to reproduce functional (permeability) and molecular (ZO-1 mRNA expression) alterations observed in IBS patients. These findings might pave the way both to identify novel biomarkers as well as new therapeutic targets in IBS.
Statistics from Altmetric.com
Irritable bowel syndrome (IBS) is characterised by abdominal discomfort or pain and changes in bowel habit in the absence of an identifiable disease process.1 Currently, the symptoms of IBS involve interactions among central nervous system components, peripheral dysfunction and low-grade inflammation and/or previous intestinal infection.2 In addition to this classical view, emerging evidence suggests that other factors, including altered intestinal permeability, can contribute to IBS and related symptoms.3 Intestinal permeability exerts a key role in the interplay between host and external environment. The paracellular permeability of the intestinal epithelial barrier (IEB) is regulated by a complex protein system that constitutes tight junctions (TJs). TJs are composed of the transmembrane proteins occludin and claudins that interact with the zonula occludens (ZO) proteins which bind to the actin cytoskeleton to control paracellular permeability.4 5
Recent studies have shown that an IBS subgroup presents with an increased intestinal permeability.6–8 However, conflicting results between post-infectious and unselected IBS patients have been reported.6 7 In one recent study, small intestinal permeability was increased in unselected diarrhoea-predominant and post-infectious IBS as compared to constipation-predominant IBS.8 Furthermore, a recent study has demonstrated that colonic soluble factors contained in faecal homogenates of patients with IBS with predominance of diarrhoea increased paracellular permeability in mice.9 However, whether paracellular permeability is altered in the colon of patients with IBS remains unknown.
Soluble mediators released by the intestinal mucosa of patients with IBS could also play a role in the generation of painful symptoms. Indeed, recent investigations have shown that soluble factors released from biopsies or from the colonic lumen of patients with IBS could induced visceral hyperalgesia in vivo.9–11 These effects were shown to be mediated via the release of various mediators such as histamine or tryptase.9–11 Furthermore, the effect of soluble factors upon visceral hypersensitivity could be the result of an increase in paracellular permeability induced by these factors.9 However, whether soluble factors can directly modify paracellular permeability of the IEB remains unknown.
Therefore, we aimed to investigate (1) the paracellular permeability in colonic biopsies of patients with IBS; and (2) the ability of soluble factors from colonic biopsies to reproduce alterations of IEB integrity in vitro.
MATERIAL AND METHODS
Subjects
Consecutive patients who met the Rome II criteria for IBS1 were seen in the Department of Internal Medicine and Gastroenterology of the University of Bologna and the Department of Gastroenterology of the Centre Hospitalier Universitaire de Nice. Healthy subjects were recruited by public advertisement after thorough exclusion of gastrointestinal symptoms. None were taking anti-inflammatory drugs (including mast cell stabilisers, histamine antagonists, anticholinergics, anti-diarrhoea medication, probiotics, immunosuppressants and steroids) or had any organic syndrome, including food allergy, coeliac disease, atopy and severe clinical depression or anxiety. Smoking habits of healthy subjects or patients with IBS were not recorded. All patients gave written informed consent.
Patients were asked to score frequency and severity of symptoms over the last 2 weeks before interview according to previously validated questionnaires.12 The severity of abdominal pain/discomfort was scored 0–4 according to its impact on patients’ daily activities: 0, absent; 1, mild (not influencing activities); 2, relevant (diverting from, but not urging modification of activities); 3, severe (influencing activities markedly enough to urge modifications); 4, extremely severe (precluding daily activities). The frequency of abdominal pain/discomfort was graded 0–4 according to the following scale: 0, absent; 1, up to 1 day/week; 2, 2 or 3 days/week; 3, 4–6 days per week; 4, daily. All clinical interviews were done within 2 weeks before the colonoscopy.
Collection and assay of mucosal mediators
A left colonoscopy without sedation was performed in participants after cleansing of distal colon with two 500-ml water enemas performed before the procedure. For all participants, two mucosal biopsies were obtained for routine haematoxylin & eosin histology to exclude the presence of microscopic colitis. One biopsy was placed in Eppendorf RNAse-free tubes, snap frozen in liquid nitrogen, and maintained at −70°C. Upon removal, two other biopsies were rapidly immersed in hard plastic tubes containing 1 ml of Hank’s buffer saline solution (HBSS; Invitrogen, Cergy-Pontoise, France), continuously oxygenated (95% O2/5% CO2) at 37°C. After 20 min incubation, the solution was removed and centrifuged at 200 g for 10 min before being filtered with centrifuge tube filters (0.22 μm, SPIN-X; Corning, New York, USA) to remove bacterial components. Aliquots of 200 μl of supernatant (SUP) were stored at −70°C until assays. Biopsies were blotted and weighed after collecting the SUP. In 13 patients with IBS and five healthy subjects, four biopsies were taken for the purpose of paracellular permeability as described below. None of these subjects were smokers.
Paracellular permeability of colonic biopsies in Ussing chambers
Paracellular permeability in colonic biopsies was measured as previously described.13 Four standard biopsies were mounted in adapted Ussing chambers (Transcellab; TBC, Paris, France) exposing a surface of 0.0314 cm2. Tissues were bathed on each side with 3 ml of Ham’s Nutrient Mixture (HAM’s F12; Invitrogen). The medium was continuously oxygenated and maintained at 37°C by a gas flow (95% O2/5% CO2). After a 15 min baseline period, 150 μl of apical medium was replaced by 150 μl of fluorescein–5.6 sulfonic acid (10 mg/ml) (400 D; Invitrogen). The fluorescence level of basolateral aliquots of 150 μl was measured at 30 min interval during 180 min using a fluorimeter (Tecan Infinite F500; Tecan SA, Lyon, France). Fluorescence values were converted in concentrations of fluorescein (ng/ml) using a standard curve. Values of permeability at 180 min were the mean of four biopsies with individual coefficient of variability less than 5.2%.
Caco-2 cells
Experiments were performed with the human intestinal epithelial cell line Caco-2 (EATCC, Port Down, UK). Cells were seeded onto porous filters (12-well Transwell Clear, 0.40 μm porosity, 1.1 cm of diameter; Corning, ATGC, Marne la Vallée, France), at a density of 200 000 cells/filter and cultured in Dulbecco’s modified Eagle’s medium (DMEM) (4.5 g/l glucose; Invitrogen) supplemented with 10% heat-inactivated fetal calf serum (FCS) (Abcys, Paris, France), 2 mmol/l glutamine (Invitrogen) and 50 IU/ml penicillin, and 50 μg/ml streptomycin (Invitrogen). After 14 days of culture, Caco-2 cells formed a differentiated and polarised monolayer. The culture medium was changed every 2 days.
Experimental protocol
Caco-2 cell monolayers were incubated for 48 h with SUP of healthy subjects or patients with IBS. The SUP was added to the apical and basolateral side of Caco-2 monolayers. The volume of SUP was normalised to the weight of biopsies (150 μl for 5 mg) in order to add similar concentrations of soluble mediators (eg, SUP was diluted once the biopsy weight was known). Control solutions were also performed by adding similar volumes of HBSS instead of SUP.
Resistances and paracellular permeability of Caco-2 cells
Caco-2 monolayer transepithelial resistances (TERs) were measured with an epithelial volt–ohm meter (WPI, Stevenage, UK) before and after 24 and 48 h incubation with SUP. Results (in ohms) are presented as differences compared to basal values.
Paracellular permeability studies were performed using the flux of dextran–fluorescein isothiocyanate (FITC) through Caco-2 monolayer as previously described.14 At the end of the 48 h incubation period, 150 μl of FITC-conjugated dextran (4 kDa, 10 mg/ml; Sigma, Saint Quentin Fallavier, France) were added to the apical compartment. Basolateral aliquots were taken after 8 h and the fluorescence level was measured in a 96-well fluorescent plate reader using a fluorimeter at 496 nm (PerkinElmer, Courtaboeuf, France). Values were converted in concentrations of FITC–dextran (ng/ml) using a standard curve.
ZO-1 and occludin mRNA expression by real-time quantitative polymerase chain reaction
Total RNA was extracted from cells using RLT (Qiagen, Courtaboeuf, France) according to the manufacturer’s instructions. Total RNA (5 μg), pd(N)6 random hexamers (1 μl, 265 ng/μl) (GE Healthcare, Orsay, France) dNTPs (1 μl, 10 mmol/l) (Invitrogen), first strand buffer 5× (5 μl) (Invitrogen), DDT (1 μl, 0.1 mol/l) (Invitrogen), and RNasin (0.5 μl, 40 U/μl) (Promega, Charbonnieres, France) were used to synthesise single-stranded cDNA using the Superscript II Reverse Transcriptase (0.5 μl, 200 U/μl; Invitrogen) in a total volume of 25 μl. Incubation was performed at 42°C for 60 min. Amplification conditions for S6 (housekeeping gene), ZO-1 and occludin were optimised for the RotorGene 2000 instrument (Ozyme, Saint Quentin en Yvelines, France). PCRs were performed with 2 μl of cDNA, 0.1 μl of a solution of SYBR Green I diluted at 1:100 (Sigma), 1 μl (10 μmol/l) of each primer, 1 μl (10 mmol/l) dNTPs, and 0.4 μl of titanium Taq DNA polymerase kit (Ozyme). Cycling conditions were as follows: 5 min at 95°C; amplification for 40 cycles, with denaturation for 5 s at 95°C, annealing for 15 s (66°C for S6 and ZO-1), (68°C for occludin) and extension for 15 s at 72°C. The following primers were used.
S6 forward: 5′-CCAAGCTTATTCAGCGTCTTGTTACTCC-3′
S6 reverse: 5′-CCCTCGAGTCCTTCATTCTCTTGGC-3′ (PCR product 130 bp)
ZO-1 forward: 5′-GAATGATGGTTGGTATGGTGCG-3′
ZO-1 reverse: 5′-TCAGAAGTGTGTCTACTGTCCG-3′ (PCR product 191 bp)
Occludin forward: 5′-ATGAGACAGACTACACAACTGG-3′
Occludin reverse: 5′-TTGTATTCATCAGCAGCAGC-3′ (PCR product 252 bp).
All PCR products were sequenced to validate the specificity of the amplification.
An external standard curve was generated with serial dilutions of control cDNA, by plotting the relative amounts of these dilutions against the corresponding Ct (threshold cycle) values. The amount of ZO-1, occludin and S6 was calculated from these standard curves using the RotorGene software V5.0 (Ozyme). Samples were tested in triplicate and the average values were used for quantification using the 2−ΔΔCT method as previously described.15
Pharmacological tools
Histamine (Sigma) was added to the apical and basolateral compartment of Caco-2 monolayer at a final concentration of 10 μmol/l. Chlorpheniramine (histamine-1 receptor antagonist; Sigma), cimetidine (histamine-2 receptor antagonis;, Sigma) and thioperamide (histamine-3/4 receptor antagonist; Sigma) were used at the following final concentrations dissolved in sterile water: 10−5 mol/l, 10−4 mol/l and 10−6 mol/l, respectively. Differentiated Caco-2 monolayers were first treated during 30 min with a cocktail of histamine receptor antagonists, prior to the addition of SUP of both healthy subjects and patients with IBS for 48 h.
Statistical analysis
Data were expressed as mean with the SD or median and interquartile ranges and were compared using non-parametric Mann–Whitney U test or ANOVA with post-tests when appropriate. Relationships between permeability and TER, abdominal pain severity and TJs expression were assessed by linear regression. A p value <0.05 was considered significant.
RESULTS
Fifty-one patients with IBS and 14 healthy subjects were included in the study. The clinical characteristics of the patients with IBS are described in table 1 according to IBS subtype.
Paracellular permeability of colonic biopsies
Paracellular permeability of colonic biopsies at 180 min of culture was significantly higher in IBS patients (107 (SD 30) ng/ml, n = 12) compared with healthy subjects (66 (SD 5) ng/ml, n = 5, p = 0.01). There was no difference among IBS subtypes (fig 1). In IBS patients, a statistical trend was observed between the severity of abdominal symptoms and paracellular permeability of colonic biopsies (r = 0.55, p = 0.06). However, no correlation was found between the frequency of abdominal pain and paracellular permeability.

ZO-1 and occludin expression in colonic biopsies
ZO-1 mRNA expression was significantly lower in biopsies of IBS patients compared to healthy subjects (1.2 (SD 2.0) vs 14.0 (SD 28.8), p = 0.04) (fig 2A). Occludin mRNA expression was similar between IBS patients and healthy subjects (17.5 (SD 36) vs 14 (SD 25), p = 0.7) (fig 2B). There was an inverse correlation between the expression of ZO-1 mRNA expression in colonic biopsies and the paracellular permeability induced in Caco-2 by SUP of the corresponding IBS patient (r = −0.56, p = 0.01).

Effect of SUP on TER and paracellular permeability of Caco-2 cells
After 48 h, SUP of IBS induced a significant fall in TER of Caco-2 monolayer (−100 (SD 66) Ω, n = 39) compared to that of healthy subjects (−9 (SD 32) Ω, n = 14, p<0.0001) and control solutions (−13 (SD 37), n = 12, p<0.0001) (fig 3). Interestingly, changes in TER were similar among IBS subtypes at any time-points (data not shown). SUP of patients with IBS applied to Caco-2 cells induced a significant increase of paracellular permeability (1218 (SD 265) ng/ml, n = 39) compared to SUP of healthy subjects (989 (SD 117) ng/ml, n = 14, p = 0.001) and control solutions (1042 (SD 121) ng/ml, n = 12, p = 0.01) (fig 4). In patients with IBS, there was a significant inverse correlation between paracellular permeability and changes in TER (r = −0.63, p<0.0001). Paracellular permeability was similar among IBS subtypes (fig 4).


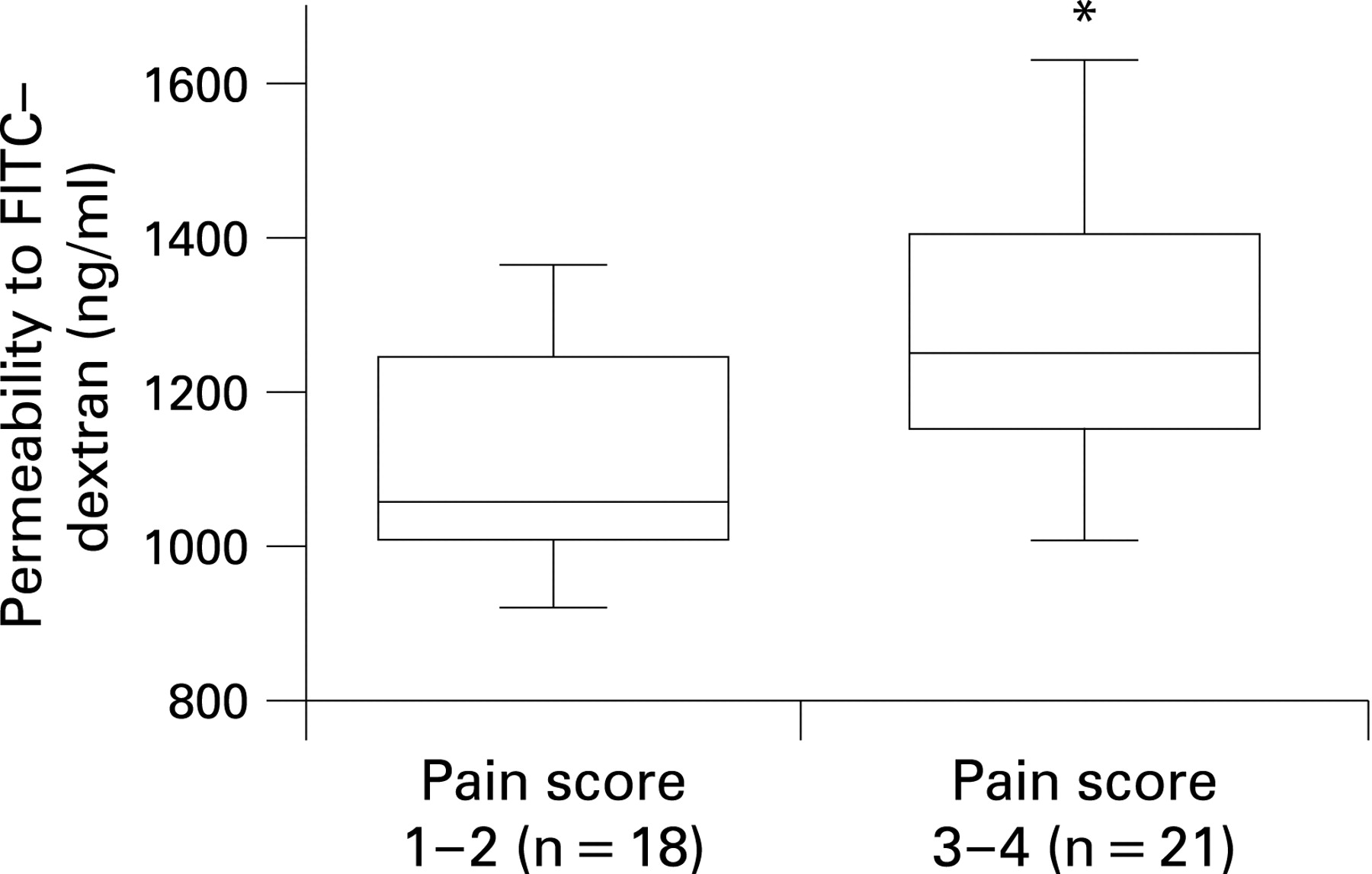
In patients with IBS, the severity of abdominal pain was significantly associated with paracellular permeability (fig 5). This correlation was more stringent in IBS patients with predominance of diarrhoea (r = 0.65, p = 0.01) than in patients with predominance of constipation (r = 0.56, p = 0.02). However, no correlation was found in IBS patients with alternating symptoms. In addition, the frequency of abdominal pain was not correlated with paracellular permeability in IBS patients. Paracellular permeability and the severity of abdominal pain were not associated with age or gender of patients.

Effect of SUP on ZO-1 and occludin expression on Caco-2 cells
ZO-1 mRNA expression was significantly lower in Caco-2 incubated with SUP of IBS patients than with SUP of healthy subjects (1.6 (SD 2.4) vs 10.3 (SD 16.0), p = 0.01) (fig 6A). In contrast, the expression of occludin mRNA was similar between IBS patients and healthy subjects (fig 6B). There was no difference between IBS subtypes. A trend to an inverse correlation was observed between the expression of ZO-1 mRNA in Caco-2 cells and paracellular permeability in IBS patients (r = −0.35, p = 0.09). In addition, no change was observed in the pericellular distribution of ZO-1 in Caco-2 monolayers incubated with SUP of IBS or healthy subjects (data not shown).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect of histamine and receptor antagonists on TER and paracellular permeability of Caco-2 cells
Compared to the control solution, changes in TER were not modified after addition of histamine (10 μmol/l) to Caco-2 cells for 16 h as compared to control (57.6 (SD 23.7) vs 40.0 (SD 52.6) Ω, n = 6, p = 0.4). In addition, histamine did not significantly alter paracellular permeability of Caco-2 cells compared to control solution (1113 (SD 221) vs 1337 (376) ng/ml, p = 0.3, respectively). Changes in TER and paracellular permeability of Caco-2 monolayers incubated with SUP of patients with IBS (n = 6) or healthy subjects (n = 4) were not significantly modified by a pre-treatment with a cocktail of histamine receptor antagonists (data not shown).
DISCUSSION
The current study showed that paracellular permeability of colonic biopsies of patients with IBS is increased irrespective of IBS subtype. Moreover, soluble mediators released from colonic biopsies of IBS patients induced a significant increase in the paracellular permeability of Caco-2 cell monolayers as compared to healthy subjects. Of interest, the magnitude of increase in permeability was positively correlated with abdominal pain severity of IBS patients. In addition, SUP of IBS patients induced a concomitant decrease in ZO-1 but not occludin mRNA expression in Caco-2 as compared to healthy subjects. A similar significant decrease in ZO-1, but not occludin, mRNA expression was also observed in colonic biopsies of IBS patients as compared to healthy subjects. In our experiments, the role of histamine as a candidate mediator is unlikely.
A growing body of evidence suggests that disturbances of IEB functions, in particular enhanced gut permeability, may play a contributory role in the sequence leading to gut dysfunction and generation of IBS symptoms. Indeed, using the lactulose/mannitol test, elevated intestinal permeability has been documented in 12–50% of IBS patients, depending on the infective nature of IBS, inclusion of patients with adverse reaction to food or various IBS criteria.7 16–19 More recently, Dunlop et al8 found highest small bowel permeability in non-post-infectious compared to post-infectious IBS or healthy subjects, and in IBS with predominance of diarrhoea compared to IBS with predominance of constipation and healthy subjects. Our study extends previous findings of increased permeability detected in the small intestine of IBS patients to the colon by showing that (1) paracellular permeability is also increased in the human colon of IBS patients; and (2) in contrast to the small intestine, this increase (observed in colonic biopsies and also induced by soluble factors from biopsies) is independent of IBS subtype. Interestingly, this latter finding is in contrast with the data by Gecse et al9 who showed that only SUP of IBS patients with predominance of diarrhoea bowel habit could increase paracellular permeability. These differences could result from the fact that alterations of paracellular permeability described by Gecse et al9 were observed following acute administration of SUP (1 h), whereas we performed a more prolonged administration of SUP (48 h). This point also further justified the use of transformed intestinal epithelial cell lines as they can survive for a long time in contrast to mucosal biopsies which showed functional alterations as early as 4–6 h.20 Another important finding was that changes of paracellular permeability were related to a direct effect of SUP upon intestinal epithelial cells. Indeed, integrated studies performed in vivo/ex vivo cannot exclude the possibility that effects of SUP upon permeability were mediated via the activation of other cells from the mucosa such as nerves or immune cells which are known to control IEB functions (for a review, see Neunlist et al21). This is of particular interest in an attempt to identify new biomarkers for therapeutic intervention in IBS. Indeed, alterations of ZO-1 expression which we observed in colonic biopsies or were induced by SUP in Caco-2 cells could be a direct marker of IEB dysfunction in IBS.
The causes underlying pain in IBS are still poorly understood. Enhanced permeability has been suggested as an aetiological factor in several inflammatory conditions associated with pain, including Crohn’s disease,22 coeliac disease23 and acute gastroenteritis.24 A cause–effect relationship between mucosal barrier alterations and visceral hypersensitivity has been described in a recent animal study in which the chemical blockade of enhanced colonic paracellular permeability induced by stress was accompanied by a decrease in sensitivity to colonic distension.25 Our present findings suggest that the correlation between paracellular permeability and pain scores of IBS patients could be related to the effect of soluble mediators released from biopsy specimens. Interestingly, similar findings were obtained using colonic biopsies of IBS patients. It has been recently demonstrated that patients with IBS had a marked increase in colonic mucosal area occupied by mast cells with increased release of histamine and tryptase compared to healthy subjects.12 Moreover, the severity of abdominal pain of IBS patients was directly related to the proximity between activated mast cells and mucosal nerves.12
Our study also suggests a molecular basis for the SUP-induced increase in permeability, involving the TJs complex. Indeed, SUP of IBS patients, but not of healthy subjects, induced a significant reduction in ZO-1 mRNA expression in Caco-2 cells. Interestingly, a significant decrease of ZO-1 mRNA expression was also observed in colonic biopsies of IBS patients but not of healthy subjects. Finally, there was a trend of inverse correlation between ZO-1 mRNA expression in Caco-2 monolayers and paracellular permeability and a strong significant inverse correlation between these parameters in colonic biopsies of IBS patients. All these findings indicate that mediators released from colonic biopsies of IBS patients could increase permeability by altering the expression of TJ proteins, in particular ZO-1. This observation is in agreement with the role of ZO-1 in the control of paracellular permeability. Indeed, various factors known to reduce permeability have been shown to increase ZO-1 expression both at the mRNA and protein level.13 14 Similarly, in diseases with increased permeability a reduction of ZO-1 expression and mRNA has also been observed.26 Whether the reduction of mRNA expression is associated with decreases of ZO-1 proteins remains unknown. Measurements of ZO-1 mRNA expression in biopsies of IBS patients could be used as a marker of the alteration in the IEB permeability. Indeed, we found an inverse correlation between ZO-1 mRNA expression in biopsies and permeability changes of Caco-2 induced by SUP coming from same patients.
Mediators released by biopsies responsible for the effects on IEB still remain to be identified. Previous studies10 11 have shown that candidates such as protease and histamine are involved in the effects of SUP of IBS upon the neuronal excitability. In our study, we chose first to explore the role of histamine because of its well-known involvement in the secretory response of the IEB in diseases such as allergy and inflammatory bowel diseases.27 28 Histamine also induces a secretory response in a human intestinal epithelial cell line and in mouse distal colon.29 However, the in vitro effects of histamine and/or various types of histamine receptor antagonists on paracellular permeability have led to controversial findings, depending on the type of cell line and designs of studies.30–33 Our data suggest that histamine has no effect upon the regulation of the IEB paracellular permeability in vitro. Taken together, these data suggest that histamine could be involved in the increased viscerosensitivity in IBS, but not in the increased paracellular permeability. Finally, a recent study has shown that SUP of IBS increases paracellular permeability via activation of protease-activated receptor 2 (PAR-2).9 Whether such pathways are involved in our observations is the focus of ongoing studies.
In conclusion, these data suggest that alterations of the integrity of IEB are present in colonic biopsies of patients with IBS. Soluble mediators from colonic biopsies are involved in these alterations by affecting TJ expression. These findings suggest that agents aimed at reinforcing IEB function could be a novel therapeutic target in IBS.
REFERENCES
Footnotes
See Commentary, p 161
Funding: This study was supported by a grant from Sanofi–Aventis and a “Programme Hospitalier de Recherche Clinique 2007–2008” of the CHU of Nice. The study was also supported by the Italian Ministry of Education, University and Research (No. 2002052573, to GB, VS and RDeG), and R.F.O. from the University of Bologna (to GB, RDeG and VS).
Competing interests: None.
Ethics approval: The study was approved by the two local ethics committees (Bologna and Nice) on 8 June 2005, and conducted in accordance with the Declaration of Helsinki.