Article Text

Abstract
Background Microbiome dysbiosis predisposes to colorectal cancer (CRC), but a population-based study of oral antibiotic exposure and risk patterns is lacking.
Objective To assess the association between oral antibiotic use and CRC risk.
Design A matched case–control study (incident CRC cases and up to five matched controls) was performed using the Clinical Practice Research Datalink from 1989 to 2012.
Results 28 980 CRC cases and 137 077 controls were identified. Oral antibiotic use was associated with CRC risk, but effects differed by anatomical location. Antibiotic use increased the risk of colon cancer in a dose-dependent fashion (ptrend <0.001). The risk was observed after minimal use, and was greatest in the proximal colon and with antibiotics with anti-anaerobic activity. In contrast, an inverse association was detected between antibiotic use and rectal cancers (ptrend=0.003), particularly with length of antibiotic exposure >60 days (adjusted OR (aOR), 0.85, 95% CI 0.79 to 0.93) as compared with no antibiotic exposure. Penicillins, particularly ampicillin/amoxicillin increased the risk of colon cancer (aOR=1.09 (1.05 to 1.13)), whereas tetracyclines reduced the risk of rectal cancer (aOR=0.90 (0.84 to 0.97)). Significant interactions were detected between antibiotic use and tumour location (colon vs rectum, pinteraction<0.001; proximal colon versus distal colon, pinteraction=0.019). The antibiotic–cancer association was found for antibiotic exposure occurring >10 years before diagnosis (aOR=1.17 (1.06 to 1.31)).
Conclusion Oral antibiotic use is associated with an increased risk of colon cancer but a reduced risk of rectal cancer. This effect heterogeneity may suggest differences in gut microbiota and carcinogenesis mechanisms along the lower intestinal tract.
- colorectal cancer
- antibiotics
- tumor location
- cancer risk
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Pathologic gut microbiota exerts differential influences on neoplastic and immune cells along the colorectal continuum.
Antibiotics allow for colonisation of pathogenic microbes, and exert strong, persistent effects on the structure and composition of the gut microbiota.
Previous epidemiological studies suggest an antibiotic–colorectal cancer (CRC) association; however, effect modification by anatomical location and non-linear association between antibiotics and cancer risk have not been studied.
What are the new findings?
Antibiotic use increased colon cancer risk, with the greatest effects observed in the proximal colon and with antibiotics with anti-anaerobic activity.
In contrast, use of antibiotics was associated with reduced cancer risk in the rectum at a high cumulative exposure.
These data suggest substantial heterogeneity exists in the magnitude and pattern of antibiotic effects along the colorectal continuum.
How might it impact on clinical practice in the foreseeable future?
The findings present a pattern of antibiotic-CRC risk by tumour location and type of antibiotics, and increase the importance for physicians to use antibiotics judiciously. This study will spur future studies of the microbes and mechanisms contributing to antibiotic–microbiome cancer risk, and development of approaches to intervene and mitigate the effects.
Introduction
In 2010, the estimated global consumption of antibiotics was 70 billion individual doses, which equates to 10 doses per person, and the annual rates continue to grow steadily.1 2 Given this widespread use of antibiotics, elucidating their effects on gut microbiota and links with health outcomes has substantial implications for public health. Use of antibiotics, even narrow-spectrum antibiotics, exerts strong, persistent effects on the structure of the gut microbiota and impairs the integrity of the intestinal barrier.3 4 Antibiotics allow for colonisation of pathogenic microbes,5 6 and thus, may enable colonisation with carcinogenic bacteria that induce local inflammation and tumour formation. Consistent with this hypothesis, recent data suggest differential pathogenic influences of the gut microbiota on neoplastic and immune cells along the colorectal continuum.7
Several epidemiological studies have suggested an antibiotic–cancer association. A Finnish cohort study reported increased cancer risk for several cancers, including prostate, breast, lung and colon.8 In a diabetic Asian population, a positive association between colorectal cancer (CRC) and use of anti-anaerobic agents, but not anti-aerobic agents, was observed.9 Yet, a study from the Netherlands found both anti-anaerobic and anti-aerobic agents contributed to increased CRC risk.10 The Harvard Nurses’ Health Study disclosed an association between long-term antibiotic use in early-to-middle adulthood (at age 20–39 and 40–59) and excess risk of subsequent colorectal adenomas, with a stronger association observed for proximal colon adenomas, and weaker or no association with distal colon or rectal tumours.11
However, there are several limitations to the current evidence: information about known CRC risk factors, such as body mass index (BMI), smoking and alcohol use, was not consistently measured or adjusted for across studies; a lack of sufficient power to test associations by tumour anatomical location, or results combined colon with rectal tumours; effect modification between known risk factors for CRC and antibiotics on cancer risk was not examined; studies with participant self-reported antibiotic use were susceptible to recall bias and limited in information about distinct antimicrobial classes and effects on anaerobes/aerobes; and finally, non-linear associations between antibiotics and cancer risk have not been studied.
Our aim was to investigate the associations between antibiotic use and site-specific colorectal cancer risk in the world’s largest primary care database. We hypothesised that antibiotic use, which targets the gut microbiota, was associated with colorectal cancer initiation and progression. We explored whether these effects differed by anatomical location.
Methods
Study design and setting
We conducted a matched case–control study using data obtained from the Clinical Practice Research Datalink (CPRD) in the United Kingdom. The CPRD is one of the world’s largest electronic medical record databases of anonymised clinical records with population-based data collected prospectively.12 At the time of this study, CPRD incorporated longitudinal medical records of 11.3 million patients from 674 practices in the UK, representing 6.9% of the UK population.12 The details of each drug prescription, including dosage, instructions and quantity, are automatically recorded in the computer and can be used to determine dose and duration of drug exposure. Large validation studies have suggested that data are of high quality for use in research.13 14
Participants, exposures and outcomes
The study population was drawn from all up-to-standard practices in the CPRD cohort from 1 January 1989 to 31 December 2012 with a minimum of 2 years of follow-up. Study entry was the start of observation, defined as patient registration date of the up-to-standard follow-up. The date of observation end was defined as event date (CRC diagnosis date) both for cases and controls.
CRC cases were identified from the clinical or referral record using a set of previously validated Read codes (online appendix table 1), which have a sensitivity of 92%, specificity of 99% and a positive predictive value of 98% for CRC.15 Controls were defined as patients without a diagnosis of CRC recorded at any time in CPRD. Up to five controls were randomly selected and matched to each case for year of birth (±3 years), gender, general practitioner practice site and year of registration in the CPRD (±1 year).
Supplementary Appendix 2
Our analysis was restricted to sporadic CRC. Thus, we excluded cases and controls with conditions that predispose to CRC (inflammatory bowel disease, Peutz-Jeghers syndrome, familial adenomatous polyposis and hereditary non-polyposis colorectal cancer). We also excluded patients with immunosuppressive states, including HIV infection, organ transplant and chemotherapy/immunosuppressive drug use because these factors may affect the risk of colon carcinogenesis. We excluded patients with anal cancers because they most commonly are of squamous cell origin rather than the epithelial cell origin of CRC. Age was restricted to 40–90 years. We included only oral antibiotic use since the impact of intravenous antibiotics on the gut microbiota is largely unknown. For those patients who had an identifiable tumour location, tumours originating from the caecum, ascending colon, hepatic flexure and transverse colon were classified as those of the proximal colon, whereas splenic flexure, descending or sigmoid colon tumours were classified as those of the distal colon. Tumours in the rectum or at the rectosigmoid junction were classified as rectal location (online appendix table 1).
We quantified antibiotic exposure by calculating the cumulative number of days prescribed, during research-standard CPRD follow-up (defined as time from registration date to 1 year before CRC diagnosis). Antibiotics were categorised based on their effects on aerobes/anaerobes, and by drug class (cephalosporins, macrolides, penicillins, quinolones, sulpha/trimethoprim, tetracyclines, and others, online appendix table 2). Timing preceding CRC was categorised as exposure occurring in the biologically plausible thresholds 1–10 years and >10 years.
Statistical analysis
Conditional logistic regression was used to estimate ORs and 95% CIs for the risk of incident CRC in relation to antibiotic use. In the main analysis, antibiotic exposure was evaluated by cumulative days prescribed and by known therapeutic anaerobic effect (yes/no), and class of antibiotics across anatomical site (colon vs rectum; proximal vs distal colon), controlling for BMI (categorical), smoking status (categorical), alcohol use (categorical), history of diabetes diagnosis (binary) and number of colonoscopies received (continuous). For time-varying covariates (BMI, smoking status and alcohol use), values were assigned using previously described methods16 (ie, use of the earliest records available during research-standard CPRD follow-up, or the most recent previous records if individuals lacked records at the beginning of research-standard follow-up; older values were dropped in a subsequent sensitivity analysis). We initially characterised antibiotic use in days as categorical terms (0 days, 1–15 days, 16–30 days, 31–60 days and >60 days) to quantify the average effect of each duration increase on CRC risk. To test for trend in the risk of CRC across different categories of length of prescription, we included the antibiotic categories as a continuous variable in the adjusted model. We then fitted fully adjusted models with a restricted cubic spline by taking the number of days of antibiotic use as a continuous term to assess possible non-linearity in any detected antibiotic cancer association overall and by tumour location. Effect modification was evaluated by introducing interaction terms (one at a time) between antibiotic use and location (colon vs rectum, and proximal colon vs distal colon), as well as known risk factors for CRC, including BMI, smoking status, alcohol use and diabetes history, to the full model. In order to examine the temporal relationship between CRC and antibiotic exposure, we analysed antibiotic use with time preceding diagnosis of 1–10 years and >10 years among patients with at least 15 years of follow-up. For missing data on BMI, smoking status and alcohol use, we employed multiple imputation to impute the missing data by using chained equations with 10 imputed datasets, assuming that BMI, alcohol and smoking were missing at random,17 as well as by including missing values as a category in each variable in the fully adjusted model.18
In sensitivity analyses, we excluded CRC cases occurring within 1 year after registration to deal with concerns of possible prevalent cases at study entry, included only lifestyle factors recorded during the follow-up period, included only antibiotic prescriptions more than 3 years before CRC diagnosis to guard against reverse causality (ie, antibiotic use being affected by undiagnosed CRC), assigned transverse colon cases to the distal colon instead of the proximal colon, and adjusted BMI as a continuous term in the final model. In addition, we assessed how different categorisation of antibiotic (anti-anaerobic and anti-aerobic; narrow and broad-spectrum) effects has an impact on CRC risk. The categorisations assessed were (online appendix table 3): (1) a restricted list of agents with predominant anti-anaerobic or anti-aerobic effects, (2) exclusion of vancomycin from the anaerobic antibiotic list, (3) categorisation of cephalosporins as anti-anaerobic antibiotics, (4) categorisation of ampicillin/amoxicillin as anti-aerobic antibiotics, (5) exclusion of cephalosporins from the anti-aerobic antibiotic list and (6) assessment of amoxicillin, the most commonly used oral antibiotic, as an anti-aerobic antibiotic agent, to test the impact of amoxicillin alone on the results. We additionally performed subgroup analysis on patients with single antibiotic class use versus no antibiotic use. Lastly, we assessed effect modification of age by stratifying patients into groups aged ≤70 years and >70 years, and applied the same final model in each age stratum.
This study was approved by the institutional review board of the Johns Hopkins University. Statistical analyses were performed using Stata/MP 15. 1 (StataCorp, College Station, Texas, USA). All tests of significance used two-sided p values at the p<0.05 level.
Role of the funder/sponsor
The funders of the study had no role in study design, data collection, data analysis, data interpretation or writing of the report.
Results
In the CPRD, 28 980 eligible CRC cases and 137 077 matched controls were identified using the selection algorithm (figure 1). Cases (median: 4, IQR: 0–11) and controls (median: 4, IQR: 0–12) were similar in medical visits. Participants with CRC were more likely to be overweight (35.2% vs 33.8%) and obese (18.6% vs 16.4%), to have a history of smoking (49.9% vs 46.9%), have moderate–heavy alcohol use (13.8% vs 11.4%), have a history of diabetes (8.8% vs 7.7%) and to undergo colonoscopy (3.5% vs 2.9%), and less likely to have chronic non-steroidal anti-inflammatory drug (NSAID) use (7.2% vs 9.0%) than the control group. As compared with participants with rectal cancer, those with colon cancer were more likely to be female (46.9% vs 39.2%), overweight-obese (44.9% vs 41.5%), smokers (49.3% vs 46.9%), alcohol users (74.0% vs 72.6%), have a diabetes history (9.1% vs 8.2%), and to undergo colonoscopy (3.9% vs 2.6%) than those with rectal cancer (table 1 and online appendix table 4).
Characteristics of cases and controls, overall and by tumour location
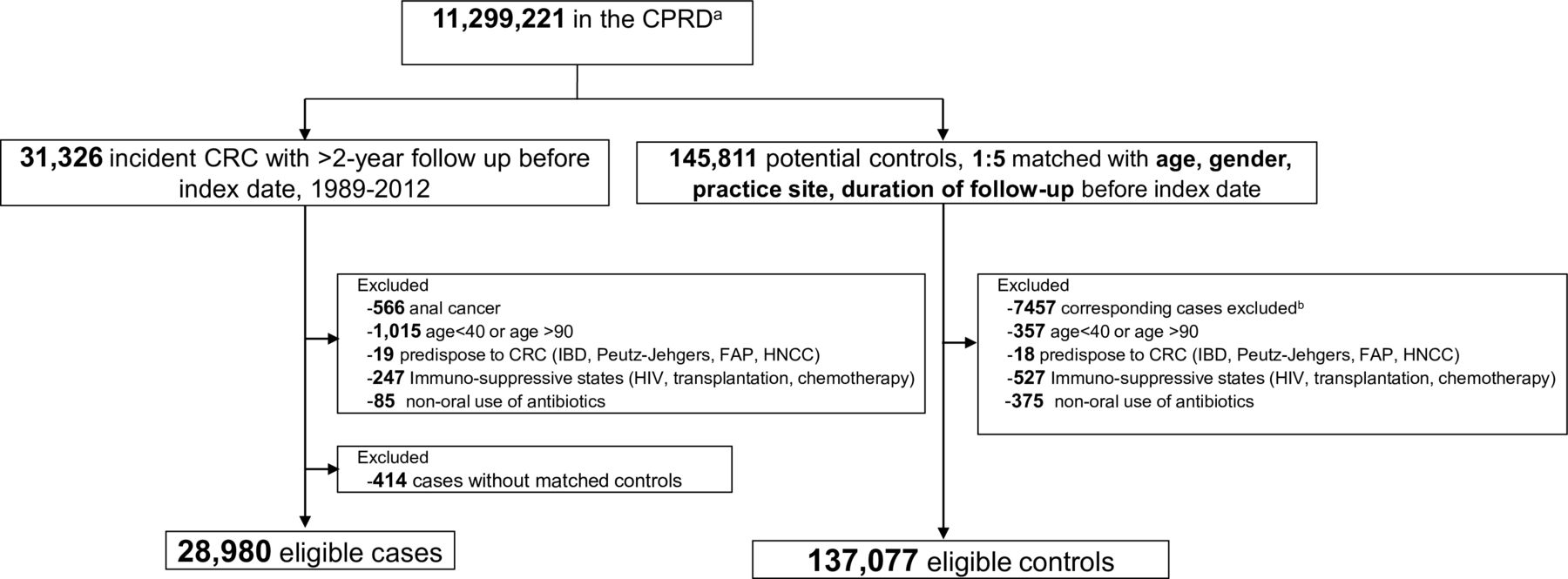
Data extraction flow chart. CPRD, Clinical Practice Research Datalink; CRC, colorectal cancer; FAP, familial adenomatous polyposis; HIV: human immunodeficiency virus; HNCC, hereditary non-polyposis colorectal cancer; IBD, inflammatory bowel disease. aCPRD GOLD data, January 2014 static version of CPRD GOLD. bTotal number of controls dropped due to matched cases excluded by the exclusion criteria: anal cancer (n=2659), age <40 or age >90 (n=3561), predisposed to CRC (n=90), immune-suppressive states (n=1147).
Participants had a median follow-up of 8.1 years (IQR 4.9–12.3 years). Antibiotics had been prescribed to 20 278 (70.0%) patients with CRC and 93 862 (68.5%) controls (p<0.001). Participants who subsequently developed colon cancers were more likely to be exposed to antibiotics as compared with controls (71.3% vs 69.1%, p<0.001), whereas participants with rectal cancers had comparable exposure to antibiotics (67.1% vs 67.2%, p=0.96). Both anti-anaerobic antibiotics and anti-aerobic antibiotics were more likely to be prescribed for patients who subsequently developed colon cancer than for controls, yet patients with rectal cancer had less anti-aerobic antibiotic exposure than controls (table 2). Of those with known CRC location, participants with proximal colon cancers were more likely to have antibiotic exposure, particularly those with anti-anaerobic effects, whereas participants with distal colon cancers had similar antibiotic exposure to controls, regardless of antibiotic spectrum (online appendix table 5). The most common prescriptions for antibiotics were penicillins (80.7%), macrolides (30.4%), sulfa and trimethoprim (28.9%), cephalosporins (25.1%), tetracyclines (20.3%) and quinolones (14.3%). Most participants (59.5%) were exposed to more than one antibiotic class. By antibiotic class (any vs none), participants with colon cancers had increased use of cephalosporins and quinolones, whereas those with rectal cancers received fewer prescriptions for tetracyclines and macrolides (table 2).
Use of antibiotics in cases and controls
The effect size and pattern of antibiotic exposure differed by tumour location (figure 2). In the colon, excess risk was observed with increased use of antibiotics in a dose-dependent fashion, with no use as the reference (1–15 days/16–30 days/31–60 days/>60 days vs no use, aORs=1.08 (95% CI 1.04 to 1.13)/1.14 (1.08 to 1.20)/1.15 (1.09 to 1.22)/1.17 (1.10 to 1.23]; ptrend <0. 001), adjusted for BMI, smoking, alcohol use, diabetes status, chronic NSAID/aspirin use, and number of colonoscopies. The effect of antibiotic use on cancer risk was more marked in the proximal colon (1–15 days/16–30 days/31–60 days/>60 days vs no use, aORs=1.14 (1.02 to 1.28)/1.15 (1.01 to 1.32)/1.32 (1.15 to 1.51)/1.09 (0.94 to 1.25]; ptrend=0.046), whereas no association was observed for each of the exposure categories on distal colon cancer risk (all p>0.10, ptrend=0.400). In the rectum, use of antibiotics showed an inverse association with CRC, with a maximum risk reduction of 15% for antibiotic use exceeding 60 days, as compared with no use (aOR=0.85, 95% CI 0.79 to 0.93, ptrend=0.003, figure 2).

Forest plot of adjusted odds ratios (aORs) for the effects of any antibiotic use, anti-anaerobic/aerobic antibiotics on colorectal cancer risk, stratified by anatomical location. ORs estimated using separate models for each site, with days of antibiotic use as categorical term, adjusted for body mass index (BMI), smoking, alcohol use, diabetes status, chronic non-steroidal anti-inflammatory drugs and aspirin use, and number of colonoscopies; N, number. Missing data were imputed for BMI, smoking and alcohol use in the above models.
Antibiotics with anti-anaerobic action properties were associated with an increased colon cancer risk (ptrend <0.001), particularly in the proximal colon (figure 2). An inverse association with antibiotic exposure was seen for rectal cancer, regardless of effects on anaerobes (agents with anti-anaerobic activity, ptrend=0.054, agents with anti-aerobic activity, ptrend=0.005). By antibiotic class, use of penicillins was associated with an increased colon cancer risk (aOR=1.09 (95% CI 1.05 to 1.13)), particularly in the proximal colon, but not cephalosporins, quinolones, macrolides, or sulfa/trimethoprim (online appendix figure 1). When restricting our analysis to patients receiving single-class antibiotic use versus no antibiotic use, penicillins consistently showed increased risk for colon cancer (online appendix figure 2). Further, we observed that penicillins (PCNs) affected colon cancer risk in a dose-dependent fashion (ptrend <0.001) but not rectal cancer (ptrend=0.92), online appendix figure 3). In contrast, tetracycline use decreased rectal cancer risk (aOR=0.90 (95% CI 0.84 to 0.97), online appendix figure 1). We noted that comparatively narrow-spectrum antibiotics (eg, macrolides, quinolones, sulfa class) did not affect cancer risk (online appendix figures 1,2).
Supplementary Appendix 1
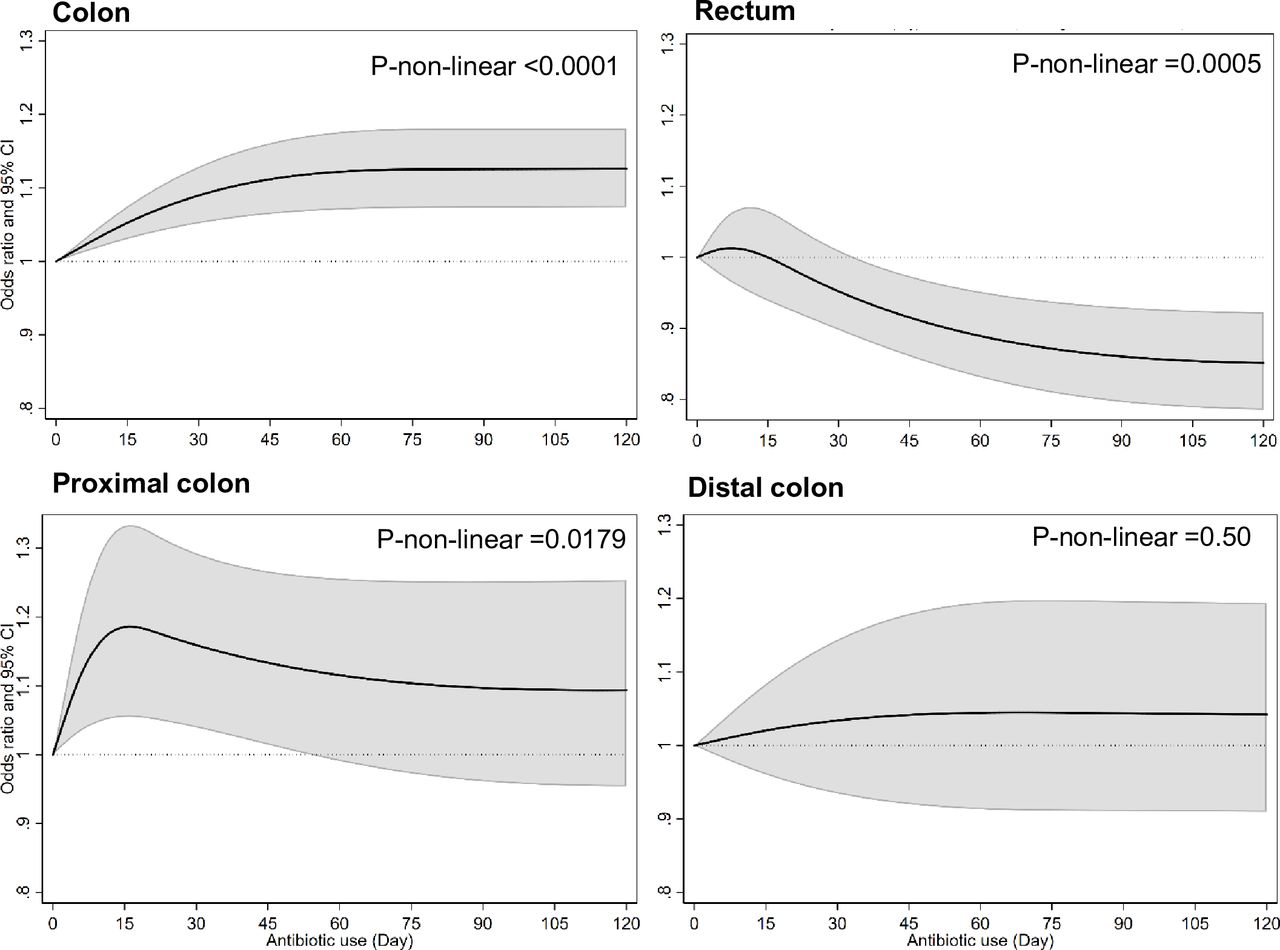
Figure 3 shows the adjusted non-linear pattern of antibiotic–cancer association by tumour location. For colon cancers, exposure to antibiotics was associated with substantially increased risk, with the effect increased after minimal antibiotic use and reaching a plateau after 60 days of cumulative exposure. Antibiotics were associated with an increased proximal colon cancer risk at minimum exposure levels, but antibiotics were not associated with a risk of distal colon cancer. For rectal cancer, there was a reduced risk of cancer associated with cumulative exposure to any antibiotic; however, this effect was not seen until after 30 days of cumulative exposure and reached a plateau after 90 days (figure 3). Significant interaction was found between antibiotic use and tumour location (colon vs rectum) (pinteraction <0.001), as well as between antibiotic use and location in the colon (proximal colon vs distal colon) (pinteraction=0.019). No interactions were observed between the use of antibiotics and known risk factors for CRC (BMI, smoking status, alcohol use, and diabetes history, all p>0.10) at each anatomical location.

{kind=link}
{kind=link}
{kind=link}
Association between any antibiotic use and colon, rectal, proximal colon and distal colon cancers, including detection of non-linearities. Curves were estimated from models with days of antibiotic exposure as a spline in each anatomical location, adjusted for body mass index (BMI), smoking, alcohol use, diabetes status, chronic non-steroidal anti-inflammatory drugs and aspirin use, as well as number of colonoscopies; non-users (day=0) were chosen as reference. Non-linearity was modelled by including a three-knot spline for colon cancers and distal colon cancers, and four-knot spline for rectal cancer and proximal cancers from best fitting models (with Akaike information criterion used to select optimal knots). Missing data were taken as categorical term for BMI (normal, overweight, obese, unknown), smoking (non-smoker, current smoker, ex-smoker, unknown) and alcohol use (non-drinker, current drinker, ex-drinker, unknown) in the above models.
Limiting the analysis to participants with at least 15 years of follow-up, use of antibiotics more than 10 years before the cancer diagnosis was associated with an increased colon cancer risk (aOR=1.17 (95% CI 1.06 to 1.31)) as compared with no antibiotic use, whereas antibiotic use 1–10 years before cancer diagnosis was not associated with colon cancer risk (aOR=1.00 (0.89 to 1.10)); no association was found between use of antibiotics and rectal cancer risk by time window (>10-year users vs non-users, aOR=0.98 (0.84 to 1.13); 1–10-year users vs non-users, aOR=0.93 (0.91 to 1.09)). Consistent results were observed with finer categories of antibiotic exposure (online appendix figure 4).
Our main findings were robust to a range of sensitivity analyses (online appendix tables 6-9, figure 5), and the known risk factors for CRC in the full model were consistent with previous literature (online appendix figure 6). When ampicillin/amoxicillin was considered as a primarily anti-aerobic antibiotic, the effects from anti-anaerobic and anti-aerobic agent exposure on colon cancer risk were reversed, (online appendix figures 7,8) suggesting that this class of antibiotics was the dominant contributor to the outcomes presented. In addition, we assessed the effect modification by age groups and results showed a consistent antibiotic–cancer risk pattern in both age ≤70 and age >70 groups (online appendix figure 9), regardless of tumour location.
Discussion
In this largest analysis of antibiotic–CRC association to date, we demonstrated that use of oral antibiotics was associated with CRC risk, but the effect size and pattern of risk varied by anatomical location in the colorectum. A dose-dependent increase in colon cancer risk was observed for any antibiotic use. This positive association was driven by anti-anaerobic antibiotics and was limited to the proximal colon, with risk increased after minimal antibiotic use. However, a reduced cancer risk from prolonged antibiotic exposure was shown in the rectum. Penicillin exposure was strongly associated with increased colon cancer risk, whereas an inverse association was found with rectal cancer for tetracyclines. The association between antibiotic exposure and colon cancer was seen in participants with antibiotic exposure more than 10 years before CRC detection.
Several studies suggest an increased risk for CRC or colorectal adenoma from antibiotic use.8 10 11 19 Our results add to this evidence by systematically investigating the exposure–risk relationships by tumour location, antibiotic action against anaerobes/aerobes and by antibiotic classes. These analyses, which examined linear and non-linear effects together with evaluation of effect modification by known risk factors for CRC, enhance the understanding of the antibiotic–cancer association.
We extended previously reported antibiotic–colon cancer associations (online appendix table 10) by observing that the exposure–risk pattern is non-linear and can increase with even a single antibiotic course but plateaus after 60 cumulative days. In addition, this study enhanced the understanding of how different antibiotic classes and anti-anaerobic/aerobic activity of antibiotic exposure affect the gut microbiome and pattern of cancer risk. Specifically, our study shows that penicillins were associated with a significantly increased colon cancer risk, a finding that is consistent with previous reports.10 19 We additionally demonstrated that the penicillin–cancer association was detected only in the proximal colon. This is intriguing as the proximal colon is the site first exposed to antibiotics not absorbed in the small intestine and before possible drug modification or degradation in the colon. Ampicillin/amoxicillin, the most commonly used penicillin, is likely to have driven the risk for colon cancer, given our observation that risk on colon cancer was reversed when assigning ampicillin/amoxicillin from the anti-anaerobic category to anti-aerobic category (online appendix figure 7, conditions S4, S6).
We uniquely showed that antibiotics, especially tetracyclines, have a protective role for rectal cancer. This contrasts with those reports of a null or positive association, which might have been due to limited sample size and combined analyses of rectal cancers with colon cancers.9 11 Several studies have reported the anti-inflammatory effects of tetracyclines and their potential antineoplastic role.20 21 Potential biological mechanisms contributing to diminished neoplastic risk from antibiotic exposure include inhibition of mitochondrial protein synthesis, matrix metalloproteinases and/or angiogenesis. In addition, antibiotics can eradicate pathogens (eg, such as those causing sexually transmitted diseases) that may contribute to malignant transformation.21 22 This association needs to be confirmed in other large cohorts and through mechanistic studies for additional validation.
In our study, the effect on CRC risk was most significant after oral exposure to anti-anaerobic agents, which markedly disrupt the microbiota organisation and structure in the colon since the gut microbiota is predominately composed of anaerobes. It is possible that the disrupted microbiota enables acquisition or development of a carcinogenic colon microbiota. Previous data have suggested that not only select bacteria but a select consortium may contribute to colon carcinogenesis.7 23–25 While the exact mechanism of differential antibiotic-cancer association by anatomical location is unknown, it is possible that putative carcinogenic bacteria, such as Fusobacterium, Porphyromonas, Enterococcaceae and Bacteroides–Prevotella, as well as toxin-producing species, including some B. fragilis and E. coli, may be differentially distributed along the colorectal tract or that colon epithelial cells display differing regional sensitivity to the microbiota. For example, Fusobacterium nucleatum, which is associated with a subset of CRC, was reported in one study to decrease in a gradient fashion from caecum to rectum, with proximal colon cancers harbouring the highest F. nucleatum levels.7 A recent meta-analysis using high-resolution bacterial 16S rRNA gene profiling did not confirm this pattern, but did identify an association between a small consortium of bacteria (a symbiont with capacity for tumorigenesis (Bacteroides fragilis), and oral pathogens including Fusobacterium nucleatum, Parvimonas micra, Gemella morbillorum) and CRC risk.25 CRC tissues are enriched for polymicrobial invasive biofilms, particularly on right-sided tumours.25 26 Thus, the greater antibiotic impact on the proximal colon may reflect disruption of biofilm formation, which has been linked with procarcinogenesis.24–27 Additionally, the emergence of data showing differential frequencies of tumour molecular characteristics, subsite-specific clinicopathological differences and response to treatment implies that the development of proximal colon, distal colon and rectal cancers differs mechanistically.28
A study of this breadth has several strengths. This is the first use of the CPRD to facilitate compiling the largest CRC cohort with matched cases and controls and available high-quality data on the use of antibiotics, lifestyle factors (BMI, smoking, alcohol use), comorbidity and other medications. We were able to investigate the relationships between antibiotics and CRC with greater precision and power than has been previously described, controlling for potential confounders. Second, in the UK, registration with a primary care GP is essentially universal (>98%), enabling prospective and unbiased collection of longitudinal clinical data in CPRD, with almost all (99.7%) prescriptions recorded.29 Data from CPRD are largely representative of the UK population and results are thought to be generalisable to this population and to comparable countries. Third, we systematically examined the possible non-linearity and effect modification of an antibiotic–cancer association and provided additional evidence for microbiota causality in CRC development. Further, availability of information about the cancer location, dose and classes of antibiotics provided insights into the heterogeneity of the antibiotic–cancer association and implied differences in microbiota mechanisms along the GI tract.
Our study has several limitations. First, missing data for lifestyle factors ranged from 10% to 20%. However, we employed two approaches to deal with this absence, and obtained consistent results. Second, data not captured in CPRD include prescriptions in secondary care, prescriptions filled and treatment adherence. Certain patient groups are missing from primary care records, such as prisoners, private patients, some residential homes and the homeless, and we excluded individuals with immunodeficient conditions; thus interpretation with respect to those populations is limited. Third, because we matched on date of birth, we were unable to examine the interaction of age and antibiotic exposure on cancer risk. However, categorisation of age (≤70 vs >70 years) supported our main outcomes. Fourth, CPRD does not have information on food intake, physical activity and family history, which may influence CRC risk. However, in a previous study with documented physical activity, food intake and family history of cancer, incorporating this information into the fully adjusted model did not significantly attenuate the increased risk from antibiotic use.11 Fifth, the number of patients with recorded Read codes specifying whether the colon cancer was located in the proximal versus distal colon was limited; thus, analyses in these anatomical groups may be underpowered and results should be interpreted with caution. In addition, cancer stage information in CPRD is lacking. Our dataset would not be able to examine the association between antibiotic use and cancer progression. As with most observational studies, potential residual confounding may exist. Lastly, misclassification of antibiotic effect on anaerobes and by antibiotic class may exist. To test these associations, we employed several sensitivity analyses comparing anti-anaerobic and anti-aerobic antibiotics and analysed how specific drugs may change/drive the effect size and pattern; the results showed consistency with our main analysis.
In conclusion, our results provide evidence supporting a potential causal relationship between antibiotic-induced microbiome dysbiosis, which may influence subclinical mucosal inflammation, and colon tumour formation. Substantial heterogeneity in the magnitude and pattern of antibiotic effects exists anatomically in the colon, consistent with different microbial-driven mechanisms of cancer pathogenesis occurring along the GI tract. More clinical and translational studies are warranted to test the interplay of antibiotics of different activities and class on the colonic anaerobic and aerobic microbiota and mechanisms of carcinogenesis. Nonetheless, whether antibiotic exposure is causal or contributory to colon cancer risk, our results highlight the importance of judicious antibiotic use by clinicians.
Acknowledgments
The authors thank Dr Krishnan Bhaskaran for his suggestions on characterisation of lifestyle factors in the Clinical Practice Research Datalink, and for generously sharing codes facilitating our non-linearity modeling analyses. The authors thank the members of the Sears laboratory for their valuable, thoughtful discussion and comments about this work. AW is supported by CRUK Pioneer Award Grant 22645.
References
Footnotes
JZ and CH contributed equally.
KAG and CLS contributed equally.
Contributors Study concept and design; acquisition, analysis or interpretation of data: all authors. Drafting of the manuscript: JZ, CH, CS. Critical revision of the manuscript for important intellectual content: all authors. Statistical analysis: JZ, CH. Obtained funding: CS. Administrative, technical or material support: CS. Study supervision: SC, KG, CS.
Funding This study was funded by the Johns Hopkins Fisher Center Discovery Program and Bloomberg~Kimmel Institute for Cancer Immunotherapy.
Competing interests DP reports grant and patent royalties through institution from Bristol Myers Squibb, grant from Compugen, stock from Trieza Therapeutics and Dracen Pharmaceuticals, and founder equity from Potenza; being consultant for Aduro Biotech, Amgen, Astra Zeneca (Medimmune/Amplimmune), Bayer, DNAtrix, Dynavax Technologies Corporation, Ervaxx, FLX Bio, Rock Springs Capital, Janssen, Merck, Tizona, and Immunomic-Therapeutics; being on the scientific advisory board of Five Prime Therapeutics, Camden Nexus II, WindMil; being on the board of director for Dracen Pharmaceuticals outside the submitted work. SC reports being consultant for Novartis and Theravance outside the submitted work. CS reports a grant from Bristol Myers Squibb for microbiome research outside the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.