Article Text

Abstract
Introduction The incidence of gestational diabetes mellitus (GDM) is increasing in Australia, influenced by changed diagnostic criteria. We aimed to identify whether the diagnostic change was associated with improved outcomes and/or increased obstetric interventions using state-wide data in New South Wales (NSW), Australia.
Research design and methods Perinatal and hospital data were linked for singleton births, 33–41 weeks’ gestation, 2006–2015, NSW. An adjusted Poisson model was used to split pregnancies from 2011 onwards into those that would have been diagnosed under the old criteria (‘previous GDM’) and newly diagnosed cases (‘additional GDM’). We compared actual rates of total and early (<39 weeks) planned births, cesareans, and maternal and neonatal adverse outcomes for GDM-diagnosed pregnancies using three predicted scenarios, where the ‘additional GDM’ group was assumed to have the same rates as: the ‘previous GDM’ group <2011 (scenario A); the ‘non-GDM’ group <2011 (scenario B); or the ‘non-GDM’ group ≥2011 (scenario C).
Results GDM incidence more than doubled over the study period, with an inflection point observed at 2011. For those diagnosed with GDM since 2011, the actual incidence of interventions (planned births and cesareans) and macrosomia was consistent with scenario A, which meant higher intervention rates, but lower rates of macrosomia, than those with no GDM. Incidence of neonatal hypoglycemia was lower than scenario A and closer to the other scenarios. There was a reduction in perinatal deaths among those with GDM, lower than that predicted by all scenarios, indicating an improvement for all with GDM, not only women newly diagnosed. Incidence of maternal and neonatal morbidity indicators was within the confidence bounds for all three predicted scenarios.
Conclusions Our study suggests that the widely adopted new diagnostic criteria for GDM are associated with increased obstetric intervention rates and lower rates of macrosomic babies, but with no clear impacts on maternal or neonatal morbidity.
- diabetes
- gestational
- diagnosis
- population health
- epidemiology
Data availability statement
Data may be obtained from a third party and are not publicly available. The data that support the findings of this study are available from the NSW Ministry of Health but restrictions apply to the availability of these data, which were used under license for the current study, and are not publicly available. The data sets were constructed with the permission of each of the source data custodians and with specific ethical approval from the NSW Population and Health Services Research Ethics Committee (reference number 2012/12/430). The data were linked by the Centre for Health Record Linkage (cherel.org.au).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
The incidence of gestational diabetes is increasing in Australia, with much of the increase due to a change in diagnostic criteria, but research on the outcomes and resource implications of the diagnostic change has shown varied findings and is generally limited to single-center studies.
What are the new findings?
Using a population-based cohort of all pregnancies over a 10-year period, we showed that the diagnostic criteria change has been associated with increased obstetric intervention in the form of total and early planned births and cesarean sections, but without a clear beneficial impact on maternal or neonatal outcomes.
Using prediction modeling, our results suggest that women newly diagnosed with gestational diabetes mellitus (GDM) since the change in diagnostic criteria (International Association of Diabetes and Pregnancy Study Groups) are receiving similar rates of obstetric interventions as those previously diagnosed despite their lower levels of hyperglycemia.
Women diagnosed with GDM are less likely to have a macrosomic baby than those without GDM, most likely due to the higher rates of births before the due date.
Perinatal deaths have decreased over the study period in all women diagnosed with GDM, and in women without diabetes, suggesting that this improvement cannot be attributed to the diagnostic change.
Significance of this study
How might these results change the focus of research or clinical practice?
Our results suggest that research must address the differing risk levels within the heterogenous group of women now diagnosed with GDM, so that clinical decisions can be more judicious, rather than applying a universal rule to the timing of delivery in women with ‘higher-risk’ pregnancies.
Introduction
Gestational diabetes mellitus (GDM) is defined as glucose intolerance first diagnosed in pregnancy, and currently occurs in approximately 15% of pregnancies in Australia.1 Women with GDM and their children have increased risks of short-term2 and longer term3 adverse outcomes. The incidence of GDM in Australia has tripled between 2000–2001 and 2016–2017, partly explained by increases in: overweight and obesity, age of mothers, and mothers from ethnic backgrounds with high susceptibility to diabetes.1 However, the rapid increase in incidence cannot be explained by changes in the risk profile of the pregnant population alone, and is most likely a result of altered diagnostic criteria (published in 2010),4–6 which identify a greater proportion of pregnant women with GDM.
In 2008, the Hyperglycemia and Adverse Pregnancy Outcomes (HAPO) study examined the relationship between impaired glucose tolerance and adverse outcomes such as rates of primary cesarean section, birth weight above the 90th percentile for gestational age, neonatal hypoglycemia, and cord-blood serum C-peptide above the 90th percentile.4 This study found evidence of a continuous relationship between maternal glucose levels and adverse outcomes. These results informed the new diagnostic criteria, endorsed by the International Association of Diabetes and Pregnancy Study Groups (IADPSG, 2010), the WHO, and Australasian Diabetes in Pregnancy Society (ADIPS, 2013), and recommended for adoption by the Royal Australian and New Zealand College of Obstetricians and Gynaecologists (2015).7 8
In Australia, adoption of the criteria has been incremental.7 A small number of single-center studies in Australia have examined outcomes before and after the change in diagnostic criteria, and found a significant increase in the numbers of women diagnosed with GDM under the new criteria, but concluded that there has been no reduction in adverse outcomes for the overall pregnant population.9 10
The diagnostic change, introduced without strong clinical trial evidence, has the potential to significantly increase resource use and costs of care by moving more women into ‘higher risk’ pregnancy care, consuming more antenatal resources10 and potentially increasing the number of women with negative experiences in their pregnancy, due to the burdensome nature of gestational diabetes management.11 It is important to determine that the diagnostic change has clear benefits for health outcomes. In our study, we aimed to identify whether the change in diagnostic criteria has been associated with increases in obstetric interventions and/or improvements in perinatal outcomes in the total birthing population of New South Wales (NSW), Australia, over 10 years using surveillance and routinely collected data.
Methods
This was an observational cohort of singleton pregnancies, 33–41 weeks’ gestation, from January 2006 to December 2015 in NSW, Australia. The healthcare system in Australia is a hybrid model of public and private health services, with free medical care provided in public hospitals (universal access), while consumers can choose to attend private hospitals where they choose to contribute to the cost of services.12 Data were linked from three population-level databases using probabilistic methods: the NSW Perinatal Data Collection, a surveillance system of all births in NSW in both public and private hospitals and a small number of homebirths (‘birth data’); the Admitted Patient Data Collection covering all admissions to both public and private hospitals in NSW (‘hospital data’); and the NSW Registry of Births, Deaths and Marriages death registrations, a legislated registry of all deaths certified by a registered medical practitioner or a coronial inquiry (‘deaths data’). The birth data contained pregnancy, labor and outcome data, including antenatal risk factor information, and the hospital data contained diagnoses and medical procedures for all hospital admissions for both mothers and their babies. The NSW Centre for Health Record Linkage conducted the linkage, with estimated false-positive and false-negative linkage rates less than 5 per 1000.13 There were 152 hospitals in NSW contributing birth data across the study period. In 2015, there were 30% of births in 11 level 6 tertiary hospitals, 20% of births in 11 level 5 hospitals, 20% of births in 16 level 4 hospitals, 23% of births from private hospitals, and the remaining 8% of births in lower level hospitals (see online supplemental table 1 for descriptions of obstetric levels).14 Researchers were given access to the deidentified source data sets, with unique identifiers for mothers and infants.
Supplemental material
Study variables
The detailed definitions and codes for all variables are found in online supplemental table 2. The exposure of interest was diagnosis with GDM, identified in the birth data or in hospital birth record or any antenatal hospital admissions.15 Routine screening for GDM is recommended in Australia between 24 and 28 weeks’ gestation, with earlier testing suggested for women with certain risk factors.16 In order to remove any cases incorrectly classified as GDM instead of type 1 or type 2 diabetes, we applied a 5-year lookback to the hospital data to identify any admissions for non-gestational diabetes before the current pregnancy, and removed these women from the analysis. The previous ADIPS criteria for the diagnosis of GDM involved a two-step approach: a non-fasted 50 g glucose challenge (cut-off 7.8 mmol/L at 1 hour), and then (if above the cut-off), a fasted 75 g oral glucose tolerance test (OGTT) with measurements at 0 and 2 hours; a diagnosis made if one or more glucose values (≥5.5 mmol/L at 0 hour, ≥8.0 mmol/L at 2 hours) were above the recommended cut-offs.14 The new IADPSG criteria were a one-step approach, with a single-fasted 75 g OGTT with measurements at 0, 1, and 2 hours, and diagnosis made if one or more glucose values (≥5.1 mmol/L at 0 hour, ≥10.0 mmol/L at 1 hour, ≥8.5 mmol/L at 2 hours) were above the recommended cut-offs.13 The change to the one-step approach impacts on the incidence of GDM in a number of ways: the less than perfect sensitivity of the glucose challenge cut-off in the two-step approach17 and the lower 1-hour cut-off in the one-step OGTT means an increase in the number of women who meet the one-step criteria for diagnosis; however, the 2-hour cut-off in the one-step criteria is higher, and therefore some women who would have been diagnosed by the ADIPS criteria are no longer diagnosed under the new criteria.6
The main outcomes of interest were rates of total planned births (planned cesareans and inductions), early planned births (planned births <39 weeks’ gestation), total cesarean sections, a composite maternal morbidity indicator of adverse outcomes such as transfusion, intubation, uterine rupture, cardiac arrest, and hysterectomy (see online supplemental table 2 for details),18 perinatal deaths (stillbirths and neonatal deaths within 28 days), a composite neonatal morbidity indicator of adverse outcomes such as birth trauma, respiratory distress, resuscitation/intubation, ventilation, and transfusion (see online supplemental table 2 for details),19 20 macrosomia (>4 kg birth weight), large for gestational age (>90th percentile weight for gestational age)21 and neonatal hypoglycemia. We also examined gestational age at birth.
Covariates in adjusted models included maternal age, country of birth, previous cesarean, assisted reproductive technology in the current pregnancy, smoking during the current pregnancy, any hypertension in the current pregnancy, prelabor rupture of membranes (PROM), and placental issues (including placenta previa and morbidly adherent placenta).
Exclusions
Women with no antenatal care visit before 30 weeks and those who birthed <33 weeks’ gestation were removed in order to ensure that all participants in the study had the opportunity to be screened and tested for GDM, and to start treatment if appropriate. We also limited the upper gestational age to 41 weeks, as there has been a decrease in the number of post-term births over the study period, unrelated to GDM, and our focus in this study was the changes from early birth to full term. Exclusions included: births with major congenital anomalies, women with type 1 and type 2 diabetes, records with missing data or possible linkage errors, and births to women who did not live in NSW.
Statistical analysis
We used predictive modeling and segmentation of the diagnosed group, to examine how we might expect the outcomes to change, versus the actual rate of the outcome; because it was not possible to simply examine outcome rates in the GDM-diagnosed group over time, as one would expect the outcomes to improve, simply due to ‘lower risk’ pregnancies being diagnosed and included progressively more with time due to incremental uptake of the diagnostic change.
We compared unadjusted characteristic profiles and outcomes in women diagnosed with GDM and those without GDM using absolute percentage differences and 95% CIs. We examined 10-year linear trends over time in both characteristics and outcomes within the GDM and non-GDM groups (and in the total cohort for outcomes only) by estimating risk differences and 95% CIs from a generalized linear regression using the identity link function and binomial error distribution. We ran an initial piecewise Poisson regression model on quarterly summary data to determine the data-driven inflection point in the incidence of GDM over time. We then ran a Poisson model with GDM diagnosis as the outcome, including a parameter for time (quarter) and an interaction between time and the inflection point. This is represented by the formula:
 (1)
(1)
where Yi is the outcome of GDM or not, β0 is the point estimate at time (T)=0, β1 is the change in rate with every 1-unit increase in time (the preinflection point trend), β2 is the slope after the inflection point (an interaction between time and the inflection point Xt) and Σβj Xij represents the covariates included in the model and ei is the error. We then generated two separate predictions for each person, one with the whole regression model, equivalent to an adjusted fit of the overall GDM incidence over time, and another excluding the time-by-inflection point interaction, predicting the incidence of GDM after 2011 assuming there was no inflection point. We summed these predictions by quarter and used the two incidence estimates to segment the GDM-diagnosed group after 2011 by quarter into those who would have been diagnosed under the previous criteria (‘previous GDM’) and those additionally diagnosed after 2011 with the revised criteria (‘additional GDM’).
We then ran adjusted Poisson models, with the same structure as above, for all outcomes, separately for GDM and non-GDM pregnancies. We used these adjusted Poisson models to run three different prediction models to yield:
Model 1: the predicted quarterly outcome rate among GDM-diagnosed women assuming no time-by-inflection point interaction (eg, adjusted rates continuing the trajectory before 2011).
Model 2: the predicted quarterly outcome rate among non-GDM-diagnosed women assuming no time-by-inflection point interaction (eg, adjusted rates continuing the trajectory before 2011).
Model 3: the predicted quarterly rate of the outcome among non-GDM-diagnosed women including the time-by-inflection point interaction (ie, the model fit to the actual non-GDM data across the entire time period).
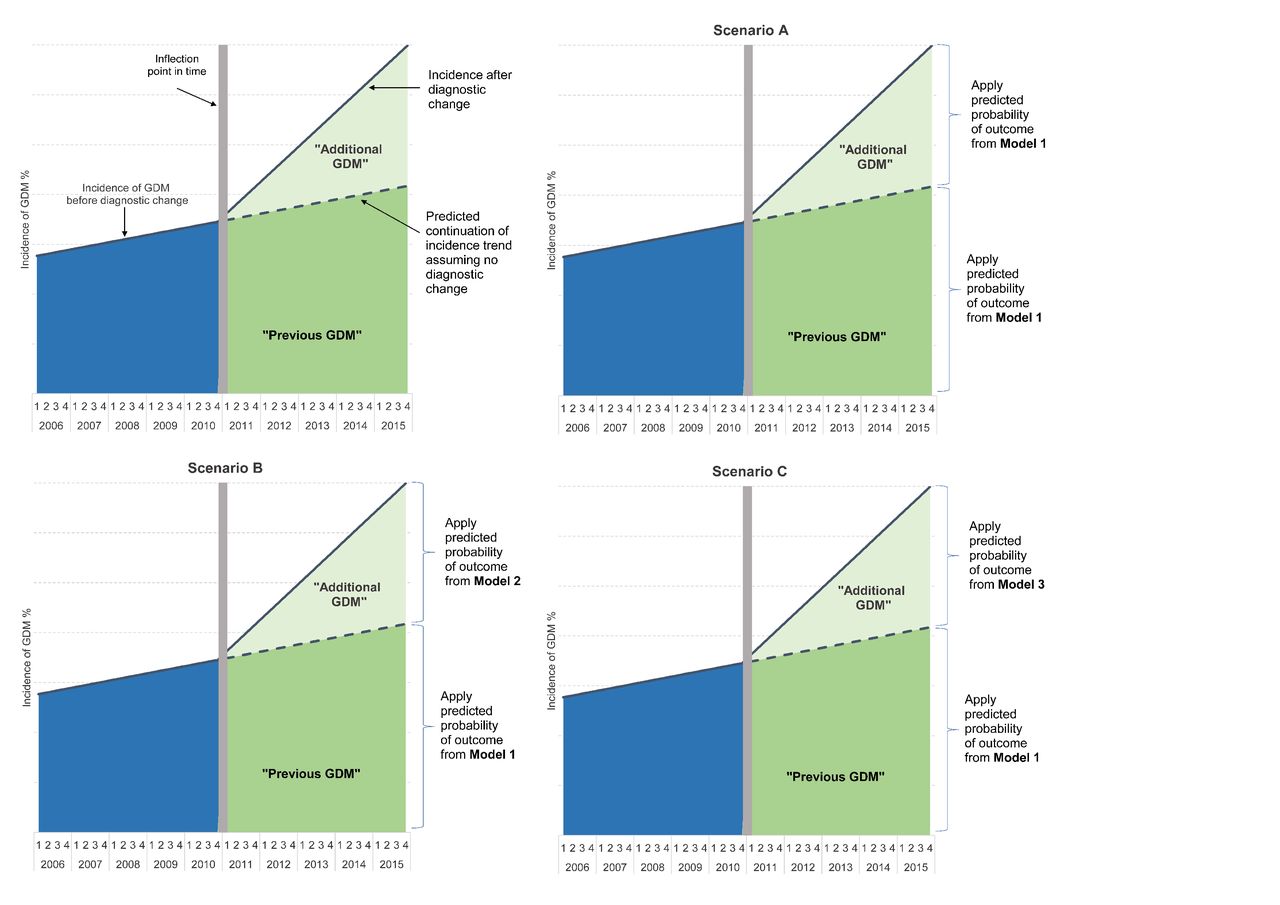
We then applied these prediction models to the segmented GDM population to form three predicted scenarios as shown in figure 1. We applied model 1 to the ‘previous GDM’ group in each scenario, and one of the three models to the ‘additional GDM’ group. The scenario descriptions were:
Scenario A: the ‘additional GDM’ group predicted to have similar intervention/outcome rates to those predicted for the ‘previous GDM’ group before the diagnostic change, that is, those diagnosed under the old criteria.
Scenario B: the ‘additional GDM’ group predicted to have similar intervention/outcome rates to those predicted for the non-GDM group before the diagnostic change, that is, those not diagnosed under the old criteria.
Scenario C: the ‘additional GDM’ group predicted to have similar intervention/outcome rates to those of the non-GDM group after the diagnostic change, that is, those not diagnosed under the new criteria, with contemporary intervention/outcome rates.
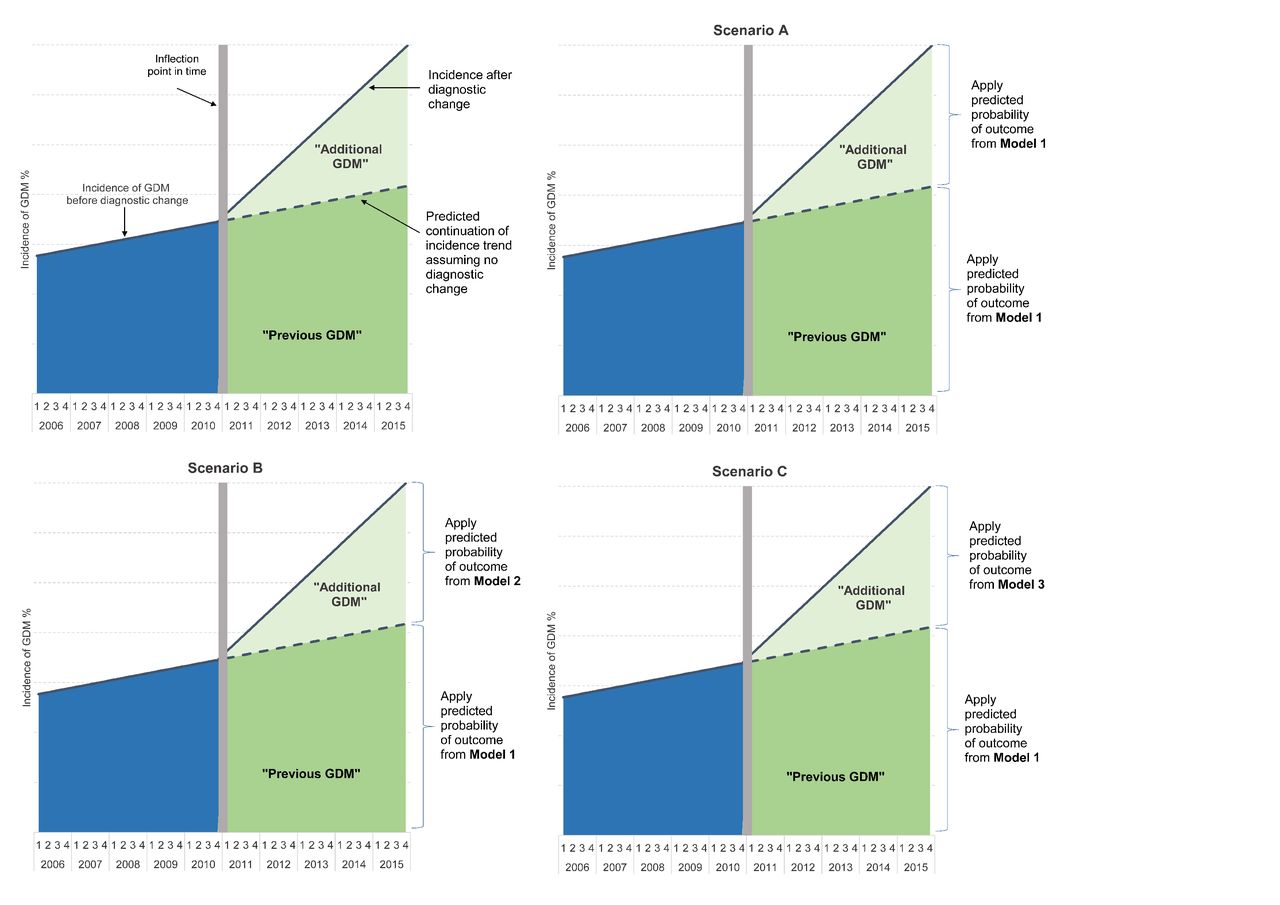
Scenarios applying prechange or postchange outcome rates to the ‘previous GDM’ and ‘additional GDM’ groups to get a total predicted outcome rate. GDM, gestational diabetes mellitus.
We summed the predicted probabilities of the outcomes by quarter and summed the totals from each segment (‘previous GDM’ and ‘additional GDM’) and divided by the total number of births in that year and quarter to calculate three predicted rates after the diagnostic change. We compared the predicted rates with the actual (observed) outcome rates for those diagnosed with GDM across the entire follow-up period as well as smoothed, modeled rates. We used bootstrapping to determine the uncertainty around the prediction estimates, resampling (with replacement) 500 data sets of n=500 000 from the main analysis data and rerunning the whole analysis including segmenting the GDM group and rerunning the prediction analyses and actual incidences. We created 95% CIs from the results of the 500 replications.
Results
There were 967 987 singleton births in NSW from January 2006 to December 2015. After exclusions, the final study population included 877 895 singleton births, 33–41 weeks’ gestation (71 740 with GDM and 806 155 with no diabetes; online supplemental figure 1). The percentage of pregnancies with a diagnosis of GDM increased from 5.8% in 2006 to 12.8% in 2015.
Table 1 shows the characteristics of the study population, comparing those diagnosed with GDM and those without GDM. Women with GDM differed significantly from those with no GDM on all the characteristics measured. Most notably, women diagnosed with GDM were more likely to be ≥35 years old, live in a major city and have a previous cesarean section, and less likely to be born in Australia or New Zealand or have smoked during pregnancy. In the GDM group, the proportion of women aged ≥35 decreased, while it increased very slightly in the non-GDM group. Smoking decreased in both groups, and the percentage of nulliparous women, women with a previous cesarean section, and those with a PROM increased in both groups. During the study period, there was a decrease in the percentage of women who were born in Australia or New Zealand in both the non-GDM and GDM groups, and there was a particular increase in the percentage of Southern Asian-born women among the GDM group.
Study population characteristics by GDM diagnosis and time, within the GDM diagnosed group
Table 2 shows the unadjusted outcomes by GDM status and year. Across the entire study period, women diagnosed with GDM were more likely than women without GDM to birth before 39 weeks, have a planned birth, have a cesarean section, and were more likely to have morbidity after the birth. The percentage of births at full term (39–41 weeks) decreased for all births, and within both GDM and non-GDM women, but the decrease was greater among the women diagnosed with GDM. Overall planned births increased in both groups, as did planned births <39 weeks and rates of total cesarean sections. Maternal morbidity increased very slightly over the study period, overall and for both GDM and non-GDM groups. Compared with babies of women with no diabetes, babies of women with GDM were more likely to die in the perinatal period (either stillbirth or in the first 4 weeks of life), and experience morbidity at birth. Babies of women with GDM were less likely to have macrosomia at birth (birth weight >4 kg), but more likely to be large for gestational age (birth weight >90th centile for gestational age) and were 8.5 times more likely to have hypoglycemia at birth. Perinatal mortality decreased significantly for the overall and non-GDM group, and also reached a low for the GDM group at the end of the study period, but the trend was not linear in the GDM group (perinatal mortality increased and then decreased) and therefore the test of the linear trend was not significant. Over the study period, there was a decrease in the percentage of babies born with macrosomia and large for gestational age, particularly among the GDM group.
Outcomes by gestational diabetes status, and by year, across the 10-year time period
We used a piecewise non-linear regression model on summarized quarterly data and identified the last quarter of 2010 as the inflection point in the incidence of GDM. We then ran an adjusted Poisson regression model, including a parameter for quarterly time, and the incrementing time after the breakpoint (quarter 1, 2011), with GDM as the outcome. With the assumption that there was no change in the diagnostic criteria, and that the same trend from 2006 to 2010 would have continued as is, the predicted incidence of GDM was 8.3% in the last quarter of 2015, considerably lower than the actual GDM incidence of 14.0% in the last quarter of 2015. We used the predicted and actual trends to split the GDM-diagnosed women into the proportion who would have been diagnosed with GDM using the previous criteria (‘previous GDM’) and the additional proportion diagnosed since the criteria change (‘additional GDM’; figure 2).
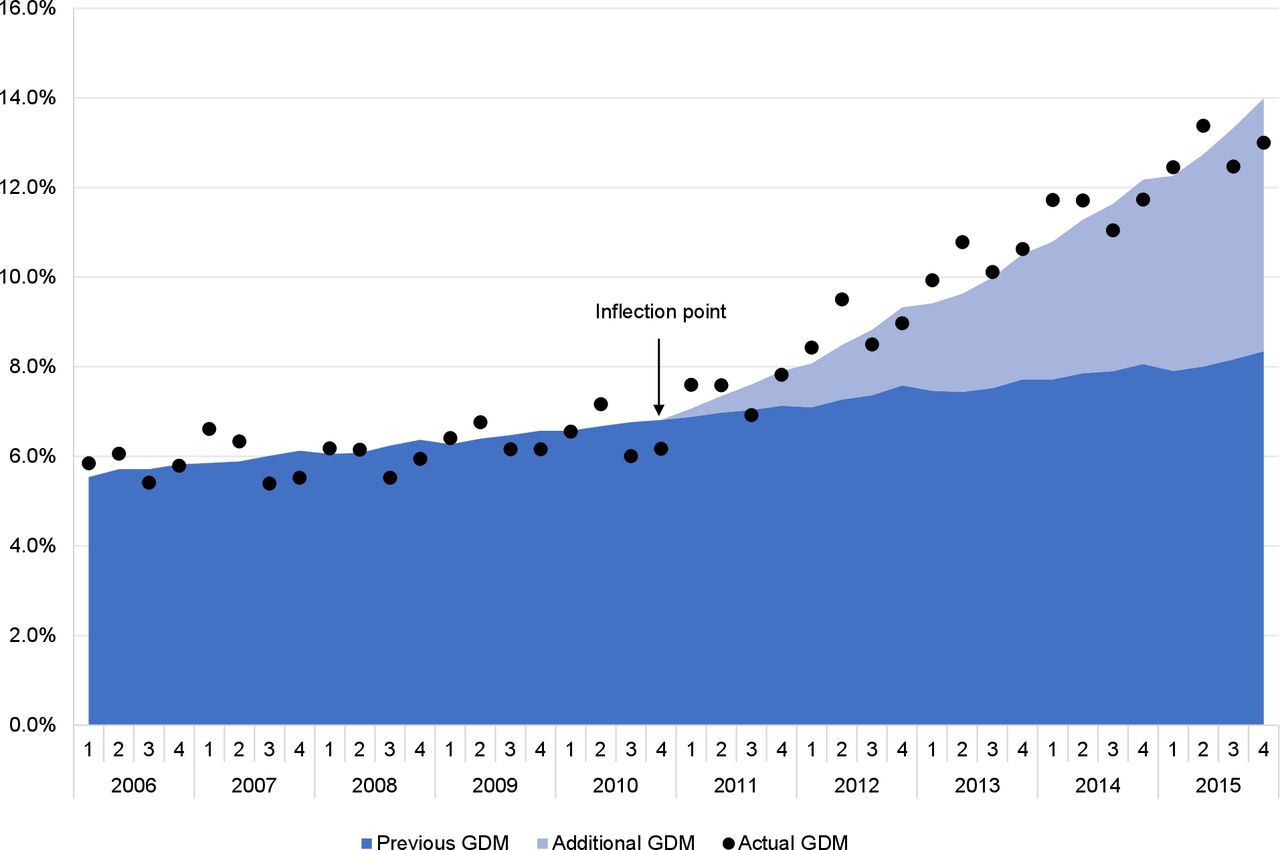
Predicted incidence of GDM by quarter assuming no change in diagnostic criteria (‘previous GDM’) and estimated additional GDM cases since the criteria change (‘additional GDM’). GDM, gestational diabetes mellitus.
Applying the adjusted models of outcome rates to the ‘previous GDM’ group and the ‘additional GDM’ as in figure 1, and summing the predicted probabilities by quarter, we plotted the predicted outcome rates against the actual outcome rates for women with GDM, with the denominator as all pregnancies/births with and without GDM (figure 3).

{kind=link}
{kind=link}
{kind=link}
The percentage of women with GDM and each outcome (actual and smoothed rates) out of all cohort pregnancies, compared with the three scenario predictions and bootstrapped 95% CIs for (A) planned births, (B) planned births <39 weeks, (C) cesarean sections, (D) maternal morbidity, (E) perinatal death, (F) neonatal morbidity, (G) macrosomia >4kg, (H) large for gestational age, and (I) neonatal hypoglycemia. GDM, gestational diabetes mellitus.
For planned births, early planned births and total cesarean sections, the scenario A prediction was the closest to the actual rate, indicating that both the ‘previous GDM’ and the ‘additional GDM’ groups were continuing on the same trajectory as the ‘previous GDM’ group before 2011. In contrast, the actual maternal morbidity incidence most closely fit scenario C though there was overlap in the CIs for all predictions. All the predicted perinatal death rate scenarios were higher than the actual rate, even when the non-GDM rates were applied to the ‘additional GDM’ group. The actual rate of neonatal morbidity was higher than all the predicted scenarios, although it was within the confidence limits for the predictions, and the predicted scenarios were very close to each other. Scenario A was the closest fit for the actual rate of macrosomia suggesting that the ‘additional GDM’ women were having similar rates of babies with macrosomia as the ‘previous GDM’ group, and these rates were lower than the non-GDM group. There was very little difference between the scenarios for the predicted incidence of large for gestational age babies, and all were similar to the actual rate. The actual rate of neonatal hypoglycemia was lower than that predicted by scenario A and was closer to scenarios B and C, indicating that the ‘additional GDM’ group had lower rates of neonatal hypoglycemia than the ‘previous GDM’ women, but slightly higher rates than the non-GDM women, although within the CI for the predictions.
Discussion
Our whole-of-population study found that the rates of GDM more than doubled from 2006 to 2015 (5.8% to 12.8% respectively). Overall, our results suggest that there has been an increase in obstetric interventions (ie, planned rather than spontaneous births) since the change in diagnostic criteria with the women meeting the new criteria but not the old, having the same intervention rates as those who met the old criteria. Total cesarean section rates were also close to the predictions assuming all the GDM-diagnosed women were like the previously diagnosed ones. Despite increased intervention, there were no clear improvements in the composite maternal morbidity indicator, and in fact, maternal morbidity increased slightly over the study period from 1.4% (2006) to 1.9% (2015). Neonatal morbidity also increased, and there was a doubling in the rate of neonatal hypoglycemia in the total cohort from 2.4% to 4.8%. There were lower rates of macrosomia and perinatal mortality, although the mortality did not appear to be related to the diagnostic change.
The increase in GDM incidence was more than expected from changing demographics and pregnancy risk factor profiles, and an inflection point at the end of 2010 was identified, when the incidence began to increase more steeply. This coincided with the publication of the IADPSG recommendations,5 but the take-up of these recommendations was gradual in NSW, as was the increase in incidence. The incidence increase in our study population was similar to published results from single-center Australian studies: 8.2% (2014) to 11.6% (2016; all births in a metropolitan hospital),22 5.9% (2014) to 10.3% (2016; all singleton births in a metropolitan hospital),10 and 9.8% (2014) to 19.6% (2015; births in a regional hospital).9 The advantage of our study was that we examined the entire cohort of women delivering babies between 2006 and 2015 in a large jurisdiction.
The actual incidence of planned and early planned births among those diagnosed with GDM suggested that the ‘additional GDM’ group was treated similarly in terms of obstetric intervention, such as induction of labor and planned cesarean section, to the group diagnosed with GDM under the old criteria. Interestingly, the incidence of macrosomia among those with GDM was also closest to scenario A, lower than the rate predicted by scenarios B and C, and indeed lower than the non-GDM group. The most likely explanation for this observation is that the diagnosis of GDM influenced obstetric decision-making about timing of birth, with greater rates of planned birth <39th week, and hence lower likelihood of birth weight >4 kg. Though macrosomia rates were reduced in the ‘additional GDM’ group, large for gestational age rates in the ‘additional GDM’ group were similarly predicted by all three scenarios suggesting the fetal overgrowth rate was not very different for the GDM and non-GDM groups, but earlier delivery for the GDM group was leading to lower rates of macrosomia.
Predicted rates of maternal morbidity and neonatal morbidity were very close for all scenarios, with confidence intervals of the predictions overlapping the smoothed actual rates, suggesting that the earlier intervention and lower rates of macrosomia were not impacting significantly on morbidity for the mother or baby. The actual incidence of perinatal mortality among those with GDM was lower than all scenarios. If this reduction was due to the changed diagnostic criteria, we would have expected to see a change in the rates for the additionally diagnosed women only, but we saw them for all those diagnosed with GDM from 2011 onwards. There was also a decrease in perinatal mortality in the women without GDM over the study time period. Neonatal hypoglycemia affected 17.9% of neonates born to women with GDM during the study period. The actual incidence of neonatal hypoglycemia was lower than that predicted by scenario A, and was closer to that predicted by scenarios B and C, suggesting that babies of the ‘additional GDM’ group had a lower risk of hypoglycemia than the ‘previous GDM’ group. Overall, though, the rate of hypoglycemia increased in the study period. Many guidelines for neonatal management in the setting of GDM pregnancy recommend serial heel prick blood glucose measurements of the neonate after birth. Therefore, ascertainment bias may account for this overall increase in neonatal hypoglycemia.
We know from the HAPO study that there was a continuous relationship between severity of hyperglycemia and adverse outcomes,4 but the HAPO study was not a randomized clinical trial, and it could not determine whether treating the higher risk pregnancies would have a significant impact on outcomes. A recent randomized controlled trial conducted in the USA compared outcomes after either the one-step or two-step GDM diagnostic approach, finding no significant differences in maternal or perinatal outcomes, even though twice as many women were diagnosed with GDM with the one-step approach. The authors concluded that the additional burden for women and increased healthcare costs of the one-step approach were not justified.23 Studies in Australia comparing outcomes before and after the change in diagnostic criteria have found no significant improvements in major outcomes,10 24 but one found increased costs due to the ‘high risk’ mode of care for the increasing percentage of women with GDM. Our study, likewise, found no clear advantage to the mother or neonate since the gradual adoption of the new diagnostic criteria in NSW.
The ‘high risk’ mode of care is not the only potential source of increased costs. The Australian Carbohydrate Intolerance Study in Pregnant Women trial, a treatment trial for women with GDM diagnosed after the two-step approach, did find that serious perinatal complications were lower in the intervention group (dietary advice, blood glucose monitoring, insulin as needed) than the group receiving routine care, but that more infants in the treatment group were admitted to neonatal care and the rate of induction was higher versus the routine care group.25 A recent study has shown that babies born following labor induction or prelabor cesarean spend more time in hospital and have higher hospital costs than those born following spontaneous labor, with cost increasing with each decreasing week of gestational age.26 There are also longer term developmental and educational outcomes that can be impacted by planned births before full term,27 and therefore the trade-off in risks versus benefits must be made carefully for each pregnancy.
Research is currently being undertaken to develop risk prediction models to understand the differing risk levels within the heterogenous group of women now diagnosed with GDM. A recent review of published prediction models noted the potential for such models to enable more personalized models of care for women with GDM, but found limitations in the current studies, highlighting the need for further work in this area.28 More personalized risk prediction is one important step, but we must also take steps to embed consumer voices in clinical decision-making. In a pilot study of a ‘community jury’, Thomas and colleagues explored the priorities and preferences of women potentially impacted by a diagnosis of GDM, and found that women prioritized the emotional consequences of a diagnosis, rather than the clinical ones, and their priorities were different from those of clinicians.29
Strengths and limitations
A major strength of our study was that we had a whole population of births in a high-quality linked data set and were able to examine trends over a 10-year time period, taking into account existing trajectories in outcomes. However, due to the use of population-level linked data, we had limited clinical detail in the data, with no access to the results of the glucose tolerance tests, nor an indicator of which women were diagnosed using the old or new criteria. This, and the gradual uptake of the new diagnostic criteria over the study period, meant we were not able to identify which women would have been diagnosed under the different criteria. This limitation was the prompt for our statistical methodology, using prediction models to account for the gradual adoption, with the ‘additional GDM’ group gradually increasing over time. There were other changes that occurred during the study time period, such as changes to the therapeutic targets for women diagnosed with GDM. The recommended therapeutic targets were lowered in many centers over the study period, meaning that women were being treated more aggressively over the same period when the diagnostic criteria were changed. As a result, it is difficult to disentangle the impacts of changed diagnostic versus therapeutic targets during this period that may impact women with GDM. However, a recent Australian study showed no difference in outcomes between tight and standard GDM treatment targets30 so the impact is likely small.
Conclusion
Our study found that the change in diagnostic criteria is associated with increasing obstetric intervention rates leading to more babies being born before full term, without a clear improvement in health outcomes, and the long-term health and resource implications must be considered, particularly since the incidence of GDM continues to rise. Further research must address the differing risk levels within the heterogenous group of women now diagnosed with GDM, so that clinical decisions can be more judicious than applying a universal rule to the timing of delivery in women with ‘higher-risk’ pregnancies.
Data availability statement
Data may be obtained from a third party and are not publicly available. The data that support the findings of this study are available from the NSW Ministry of Health but restrictions apply to the availability of these data, which were used under license for the current study, and are not publicly available. The data sets were constructed with the permission of each of the source data custodians and with specific ethical approval from the NSW Population and Health Services Research Ethics Committee (reference number 2012/12/430). The data were linked by the Centre for Health Record Linkage (cherel.org.au).
Ethics statements
Ethics approval
The study was approved by the NSW Population and Health Services Research Ethics Committee (reference number 2012/12/430).
Acknowledgments
We thank the NSW Ministry of Health for access to the population health data and the NSW Centre for Health Record Linkage for linking the data sets.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SJG, JMM and DAR conceived the study. All authors contributed to the design of the study. DAR conducted the analysis and drafted the manuscript. PK advised on the statistical analysis. SJG and JMM reviewed the manuscript critically. All authors approved the manuscript for submission.
Funding This study was supported by a 2018–2019 Ramsay Research and Teaching Fund grant.
Disclaimer The funder had no involvement in the design, analysis or reporting of the study.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.