Article Text

Abstract
Introduction With intense deficiency of medical resources during COVID-19 pandemic, risk stratification is of strategic importance. Blood glucose level is an important risk factor for the prognosis of infection and critically ill patients. We aimed to investigate the prognostic value of blood glucose level in patients with COVID-19.
Research design and methods We collected clinical and survival information of 2041 consecutive hospitalized patients with COVID-19 from two medical centers in Wuhan. Patients without available blood glucose level were excluded. We performed multivariable Cox regression to calculate HRs of blood glucose-associated indexes for the risk of progression to critical cases/mortality among non-critical cases, as well as in-hospital mortality in critical cases. Sensitivity analysis were conducted in patient without diabetes.
Results Elevation of admission blood glucose level was an independent risk factor for progression to critical cases/death among non-critical cases (HR=1.30, 95% CI 1.03 to 1.63, p=0.026). Elevation of initial blood glucose level of critical diagnosis was an independent risk factor for in-hospital mortality in critical cases (HR=1.84, 95% CI 1.14 to 2.98, p=0.013). Higher median glucose level during hospital stay or after critical diagnosis (≥6.1 mmol/L) was independently associated with increased risks of progression to critical cases/death among non-critical cases, as well as in-hospital mortality in critical cases. Above results were consistent in the sensitivity analysis in patients without diabetes.
Conclusions Elevation of blood glucose level predicted worse outcomes in hospitalized patients with COVID-19. Our findings may provide a simple and practical way to risk stratify COVID-19 inpatients for hierarchical management, particularly where medical resources are in severe shortage during the pandemic.
- blood glucose
- clinical study
- infections
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Previously published articles found that age, gender, comorbidities, lymphocyte counts, C reactive protein, procalcitonin, D-Dimer and other cytokines were associated with prognosis of patients with COVID-19. However, the effect of blood glucose level on prognosis was never reported.
What are the new findings?
Elevation of admission blood glucose level was an independent risk factor for progression to critical cases/death among non-critical cases (HR=1.30, 95% CI 1.03 to 1.63, p=0.026). Elevation of initial blood glucose level of critical diagnosis was an independent risk factor for in-hospital mortality in critical cases (HR=1.84, 95% CI 1.14 to 2.98, p=0.013). Higher median glucose level during hospital stay or after critical diagnosis (median glucose ≥6.1 mmol/L) was independently associated with increased risks of progression to critical cases/death among non-critical cases, as well as in-hospital mortality in critical cases.
How might these results change the focus of research or clinical practice?
Our findings may provide a simple and practical way to risk stratify COVID-19 inpatients for hierarchical management, particularly where medical resources are in severe shortage during the pandemic.
Background
The pandemic of COVID-19 is a global health crisis,1 with the number of confirmed cases worldwide reaching over 3 million and counting,2 as well as an overall case fatality rate of 2.3%–9.9% and mortality as high as 49% in critical cases.2–4 Faced with its rapid spread, medical resources, especially for intensive care units (ICUs), are being heavily taxed to the point of near depletion in many countries. Therefore, one of the pressing challenges in its management is the prompt and accurate prognostication of patients with COVID-19 based on their likelihood to progress into critical or life-threatening conditions. Risk stratification would be of immense help for clinicians as well as health administrative authorities worldwide to capitalize their limited resources in their response to the outbreak.5
However, there was still no universally feasible laboratory index to predict the prognosis of patients with COVID-19, particularly during such a large-scale infectious disease outbreak setting. Blood glucose level is a routine test that can be carried out in virtually all clinical settings. Among patients with COVID-19, 45.2% had anomalies in blood glucose levels.3 Previous studies showed that stress hyperglycemia was an independent risk factor associated with worse outcomes among critically ill patients.6 In addition, hypoglycemia may lead to cardiovascular events, also conferring a harmful effect on prognosis.7 We therefore speculated that blood glucose levels may have predictive value on COVID-19 prognosis.
In our current study, we reviewed 2041 patients with COVID-19 from two medical centers in Wuhan City and explored the effects of blood glucose levels on the outcomes of progression to critical cases and in-hospital mortality. We sought to identify an instant and simple approach for risk stratification and hierarchical management of COVID-19 in all clinical settings.
Research design and methods
Study population
Consecutive inpatients with COVID-19 from Wuhan Hankou Hospital and No. Six Hospital of Wuhan between 26 December 2019 and 15 March 2020 were collected in this study. The final follow-up date was 19 March 2020. Patients without available blood glucose test results were excluded from our study. The disease severity (critical or non-critical) was evaluated dynamically from the admission to the discharged. Critical patients were those who met any of the following conditions during the whole hospital stay: (1) respiratory failure requiring mechanical ventilation; (2) failures of other organs that required monitoring and treatment in ICU; and (3) shock.8 Informed consent was waived.
Data collection and definition
We collected the patients’ clinical data, including demographic information, medical history, laboratory findings, treatment and prognosis. Admission blood glucose level was measured from the first blood sample after admission. The initial blood glucose level of critical diagnosis was defined as the first blood glucose level after being diagnosed as critical case. We used occurrence of hypoglycemia, median blood glucose, glucose coefficient of variation, maximum blood glucose and minimum blood glucose to evaluate in-hospital blood glucose status. The level of median blood glucose during hospital stay or after critical diagnosis was categorized into <6.1 mmol/L and ≥6.1 mmol/L.9 Hyperglycemia was defined as blood glucose level ≥6.1 mmol/L after admission.10 Hypoglycemia was defined as blood glucose level below 4.0 mmol/L after admission.11
Study outcomes
For non-critical patients at admission, we used a composite outcome to analyze the association between glucose-relevant indexes and the risk of progression to critical cases/death. The composite outcome was reached when any of the following outcomes occurred, which included admission to ICU, mechanical ventilation, hemodynamic compromise or death. The time to the composite outcome was identified as the interval from admission to the first occurrence of the composite outcome during hospital stay. For critical patients, we evaluated the predictive performances of glucose-associated indexes in in-hospital mortality. The time from critical cases to death was defined as the time interval from the date diagnosed as critical cases to the date of death from any cause.
Statistical analysis
All continuous variables were tested for normality. Data were expressed as mean and SD if normally distributed or as median and IQR otherwise. The categorical variables were presented as frequencies and percentages. Cox proportional hazard regression models were applied to evaluate the association between the multiple blood glucose indexes and prognosis. This multivariable analysis was adjusted for all factors included in the univariable analysis. The HRs and 95% CIs of Cox regression models were reported. Because patients with diabetes generally had higher glucose levels and poor outcomes than that of patients without diabetes, which may result in bias in evaluating the relationship of glucose levels with the rate of progression to critical cases/death or in-hospital mortality. Therefore, in the present study, sensitivity analysis was conducted to evaluate the association of admission blood glucose level with the risk of critical cases/death among non-critical patient without diabetes at admission. Similar analyses were also performed to evaluate the association of initial blood glucose level of critical diagnosis with in-hospital mortality among critical patients without diabetes. We used Stata/MP V.14.0 and R software (V.3.6.1) to conduct data analyses, and two-sided p values less than 0.05 were considered significant.
Results
Baseline characteristics
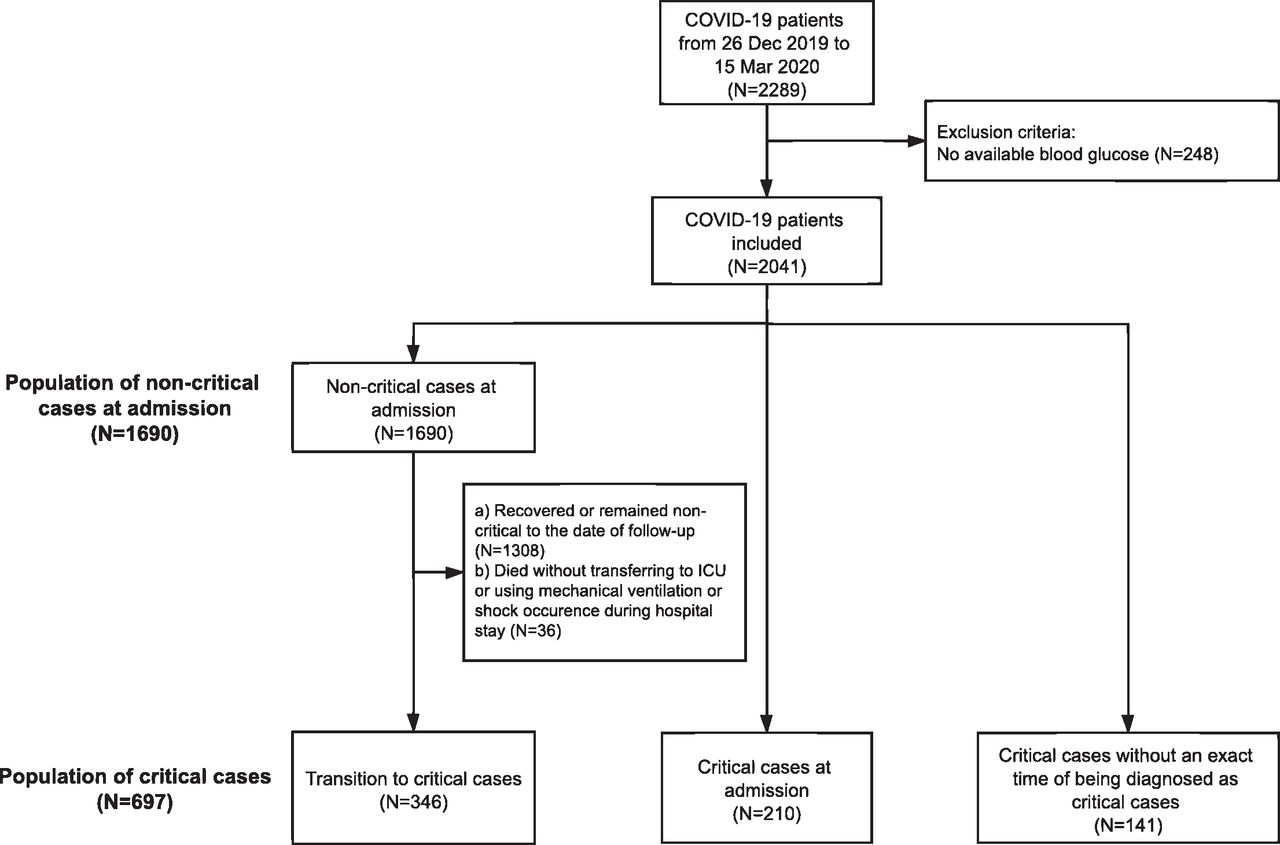
From 26 December 26 2019 to 15 March 2020, a total of 2289 cases of hospitalized patients with COVID-19 were consecutively collected from two medical centers in Wuhan, China. After exclusion of cases without available blood glucose data (n=248), a total of 2041 cases of hospitalized patients with COVID-19 were collected. The median glucose determination number was 2 (IQR 1–4) for all patients during the whole hospitalization with a median in-hospital stay of 13.5 days (IQR 7.8–20.9), and the determination number of fasting blood glucose for all patients was 2 (IQR 1–3). Among all cases, 697 patients were critical cases, 30.1% (210/697) patients were diagnosed as critical cases at admission, 49.6% (346/697) patients were developed among non-critical cases at admission and 20.2% (141/697) patients were diagnosed as critical cases but the exact time of being diagnosed as critical cases was missing. A total of 1690 patients were non-critical at admission. A detailed flow chart was shown in figure 1. Baseline characteristics of all 2041 cases were shown in online supplementary table S1. Table 1 showed the baseline characteristics of non-critical patients at admission and critical cases at the time of critical diagnosis. For non-critical patients at admission, the median age was 61.0 years (IQR 50.0–69.0) and 865 (51.2%) were female. The median admission blood glucose was 5.9 mmol/L (IQR 5.1–7.5). Median in-hospital stay was 13.3 days (IQR 7.7–20.9). For critical cases, the median age was 65.0 years (IQR 54.0–73.0), and 322 (46.2%) patients were women. Median initial blood glucose level of being diagnosed as critical cases was 6.9 mmol/L (IQR 5.7–8.7). Median in-hospital stay was 15.8 days (IQR 8.4–23.1). The 30-day in-hospital mortality was 14.6% for all patients.
Supplemental material
Demographics and baseline characteristics of non-critical patients with COVID-19 at admission and critical patients with COVID-19 at the time of critical diagnosis

Flow chart of the inclusion and exclusion of patients with COVID-19. ICU, intensive care unit.
Blood glucose level was an independent risk factor for progression to critical cases/death among non-critical cases
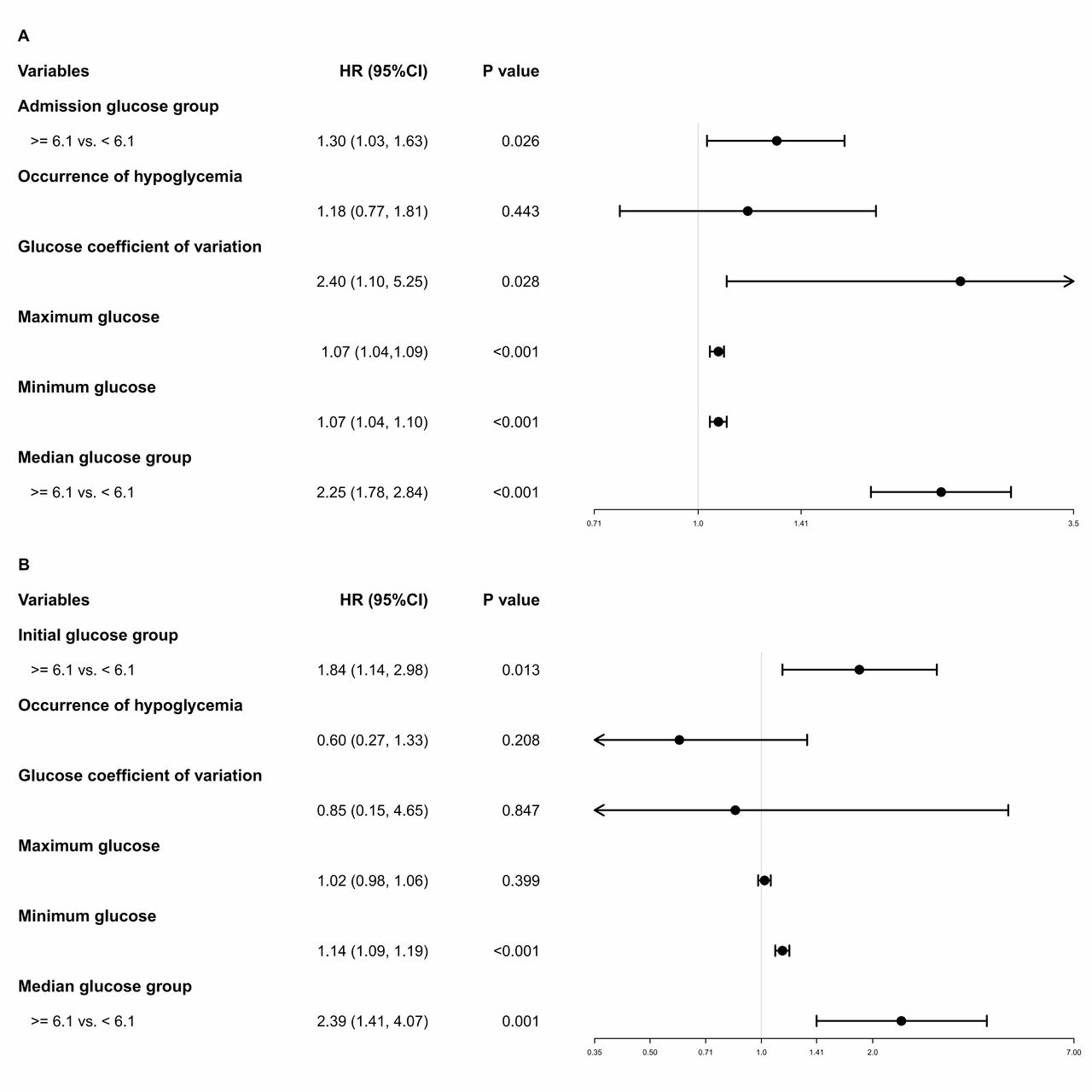
For 1690 non-critical cases at admission, 382 (22.6%) patients developed into critical cases/death. The 30-day rate of progression to critical cases/death among non-critical cases at admission is 28.9%. Results of univariable regression model showed that age, gender, hypertension, diabetes, chronic kidney disease, admission white cell counts, lymphocyte counts, D-Dimer, aspartate aminotransferase, alanine aminotransferase, insulin treatment, corticosteroid use, admission blood glucose, glucose coefficient of variation (CV), median blood glucose, median in-hospital glucose level, maximum blood glucose and minimum blood glucose were significantly associated with progression from non-critical cases to critical cases/death (p<0.05) (online supplementary table S2). In the multivariable Cox model, admission blood glucose level was an independent risk factor for progression to critical cases/death (HR=1.30, 95% CI 1.03 to 1.63, p=0.026) (table 2). For other glucose-associated indexes, multivariable Cox models showed that the median blood glucose (HR=1.09, 95% CI 1.06 to 1.12), glucose CV (HR=2.40, 95% CI 1.10 to 5.25, p=0.028), maximum blood glucose (HR=1.07, 95% CI 1.04 to 1.09) and minimum blood glucose (HR=1.07, 95% CI 1.04 to 1.10) were significant independent risk factors for progression to critical cases/death (figure 2A). We found that higher median in-hospital glucose level was independently associated with the higher rate of progression to critical cases/death among non-critical cases (HR=2.25, 95% CI 1.78 to 2.84, p<0.001). Sensitivity analysis were performed in patients without diabetes, and multivariable regression model showed that the independent risk factors were the same to the analysis in all cases. Details were shown in online supplementary figure S1A.
Association of blood glucose group with progression to critical cases/death from non-critical cases at admission in patients with COVID-19 and with in-hospital mortality in critical cases of COVID-19 in multivariable Cox regression model*
{kind=link}
{kind=link}
Forest plots of the association of multiple glucose indexes (A) with progression to critical cases/death among non-critical COVID-19 patients at admission and (B) with in-hospital mortality among critical patients with COVID-19 in multivariable Cox regression analysis.
Blood glucose level was an independent risk factor for in-hospital mortality in critical cases
As for the 697 critical cases, the time of critical diagnosis was available in 556 patients who were enrolled into the univariable and multivariable analysis. One hundred and fifty-one out of 556 patients died. The 30-day in-hospital mortality for critical cases is 30.9%. Univariable analysis revealed that age, gender, smoking history, admission white cell counts, lymphocyte counts, D-Dimer, creatinine, insulin treatment, corticosteroid use, initial blood glucose level of critical diagnosis, median blood glucose, median glucose level after critical diagnosis, maximum blood glucose and minimum blood glucose were significantly associated with in-hospital mortality (p<0.05) (online supplementary table S3). In multivariable analysis, initial blood glucose level of critical diagnosis was significantly associated with in-hospital mortality (HR=1.84, 95% CI 1.14 to 2.98, p=0.013) (table 2). Regarding the other blood glucose-associated indexes, multivariable analysis showed that median blood glucose (HR=1.09, 95% CI 1.04 to 1.14) and minimum blood glucose (HR=1.14, 95% CI 1.09 to 1.19) were significant independent risk factors for in-hospital mortality of critical cases (figure 2B). Higher median glucose level after critical diagnosis was independently associated with higher rate of in-hospital mortality in critical cases (HR=2.39, 95% CI 1.41 to 4.07, p=0.001). Sensitivity analysis in critical patients without diabetes were also performed. Multivariable regression model showed that the initial blood glucose of critical diagnosis, blood glucose control, median blood glucose and minimum blood glucose were independent risk factors for the in-hospital mortality of critical cases without diabetes. Details were shown in online supplementary figure S1B.
Discussion
Based on the data from 2041 consecutive patients with COVID-19, we found that admission blood glucose level was an independent risk factor for predicting the progression to critical cases/death from non-critical cases, and initial blood glucose level of critical diagnosis was an independent risk factor for in-hospital mortality in critical cases. In addition, patients with higher median glucose level during hospital stay or after critical diagnosis had significantly poorer clinical outcomes. The above results were also confirmed in COVID-19 patients without a history of diabetes.
The current pandemic of COVID-19 caused a global health crisis. It has been reported that progression into critical cases could happen within 3–10 days in 10%–20% of cases.12 13 Our data showed that critical cases consisted of 34.1% of the COVID-19 patient population, with a 30-day mortality of 30.7%. Therefore, predicting the likelihood of progression to critical cases in non-critical cases as well as predicting in-hospital mortality in critical cases became particularly important to the stratified management of patients with COVID-19 in a circumstance of severe shortage of medical resources during pandemic. As a convenient and easy-to-detect index, blood glucose level can be obtained and monitored in all clinical settings. Our data showed that 47.2% of patients with COVID-19 had elevated blood glucose levels at admission, and blood glucose level was an independent risk factor for progression to critical cases/death in non-critical cases. Furthermore, analysis of critical cases found that initial blood glucose level of critical diagnosis was an independent factor for in-hospital mortality in critical cases, indicating that blood glucose levels may serve as an instant and simple parameter for risk stratification and hierarchical management of COVID-19 in all clinical settings.
Interestingly, while 47.2% of the patients had admission hyperglycemia, only 13.4% of the patients had diabetes. Diabetes has been previously reported to affect the outcomes of COVID-19 cases.3 However, the predictive value of blood glucose level in patients without diabetes are more concerning in clinical practice. Elevation of the blood glucose level may represent relative hyperglycemia. Infection might trigger an inflammatory storm, which leads to insulin resistance. Infection could also induce stress and sympathetic stimulation. The SARS-CoV-2 virus might also directly attack the pancreas. All these factors may render infected COVID-19 patients more prone to hyperglycemia.14 15 Therefore, we performed analysis in patients without diabetes. Results are consistent with the overall findings. These results further illustrated that blood glucose could reliably predict the risk of hospitalized patients with COVID-19.
Our study showed that although the rate of hypoglycemia was higher (6.7%) in patients with normal median blood glucose level as compared with that in patients with high median blood glucose level (>6.1 mmol/L) (2.0%), the overall mortality was significantly reduced. This finding was different from prior study that median blood glucose level ≤6.1 mmol/L might increase the risk of both hypoglycemia and mortality in patients with diabetes.16 A possible explanation is that previous studies targeted patients with diabetes, and hypoglycemia is more likely to induce cardiovascular events, leading to increased mortality. However, for patients with COVID-19, the prevalence of cardiovascular comorbidities was actually lower than that of patients with diabetes. Thus, a slight increase in the risk of hypoglycemia did not offset the survival benefits of reducing blood glucose level. This result underlies the importance of close monitoring and control of blood glucose level during the treatment of COVID-19. Of note, in light of the potential risk of hypoglycemia, glucose control should be personalized, especially in patients with comorbidities such as cardiovascular diseases.
There are several limitations in the current study. First, the study was conducted during a large-scale infectious disease outbreak setting when the healthcare system was overwhelmed by large number of patients seeking medical care. It was a retrospective cohort study in nature, since conducting a large randomized trial was too challenging. Second, detailed data on non-insulin diabetes medications and fingerstick blood glucoses done in-between were lacking in this study. Third, the current study only included hospitalized patients, which were more severely ill cases. Hence, the generalizability of these findings to non-hospitalized patients with milder disease needs to be further verified.
In summary, our study found that blood glucose level was an independent risk factor to predict the progression to critical cases/death in non-critical cases and in-hospital mortality in critical cases, whereas patients with higher median glucose level during hospital stay or after critical diagnosis had significantly poorer clinical outcomes. Our results provided a simple and practical way to risk stratify COVID-19 inpatients for hierarchical management, particularly where medical resources are in severe shortage during the pandemic.
Acknowledgments
We would like to thank all the hospital staff members for their efforts in working in the frontline.
Footnotes
SP and HaiX are joint senior authors.
JW, JH, GZ, QW, QL and YH are joint first authors.
JW, JH, GZ, QW, QL, YH and SP contributed equally.
Contributors HaiX supervised the study. HaiX, JW, JH, GZ, QW, QL and YH designed the study. XG, CW and JS helped to organize the study. JW, JH, GZ, QW, QL, YH, YaL, YY, XS and HY collected the data. QZ did the data analysis. JW, SP, YiL, HaiX, XL and DY wrote the draft report. JS performed critical revision on the manuscript. All authors contributed to the analysis and interpretation of data. All authors approved the final version before submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study is approved by the ethics committees of Wuhan Hankou Hospital, No. Six Hospital of Wuhan and the First Affiliated Hospital of Sun Yat-sen University.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. Data used during the study are available from the corresponding author by request.